
Copeptin and Stress

Abstract
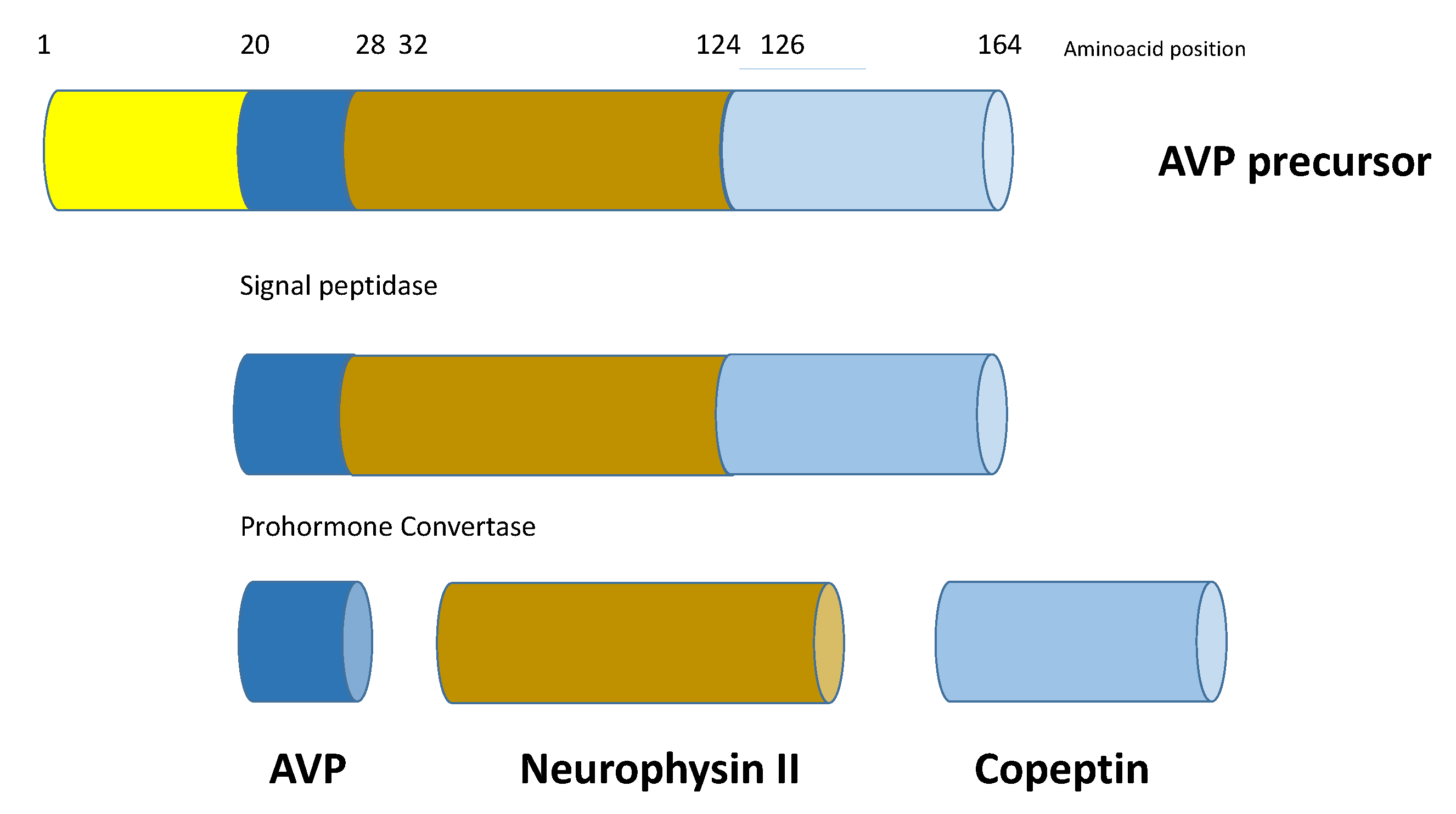
1. Introduction
2. Stress-Mediated Interaction between AVP System and Hypothalamus-Pituitary-Adrenal (HPA) Axis
3. Is Copeptin a Reliable Stress Biomarker
3.1. Sepsis and Septic Shock
3.2. Critical Illness and Intensive Care Setting
3.3. Pulmonary Diseases
3.4. Heart Failure and Acute Myocardial Infarction
3.5. Neurological Illnesses
3.6. Birth Stress
3.7. Psychological Stress
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Christ-Crain, M.; Fenske, W. Copeptin in the diagnosis of vasopressin-dependent disorders of fluid homeostasis. Nat. Rev. Endocrinol. 2016, 12, 168–176. [Google Scholar] [CrossRef]
- Morgenthaler, N.G. Copeptin: A biomarker of cardiovascular and renal function. Congest. Heart Fail. 2010, 16 (Suppl. 1), S37–S44. [Google Scholar] [CrossRef]
- Holwerda, D.A. A glycopeptide from the posterior lobe of pig pituitaries. I. Isolation and characterization. Eur. J. Biochem. 1972, 28, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Nagy, G.; Mulchahey, J.; Smyth, D.G.; Neill, J.D. The glycopeptide moiety of vasopressin-neurophysin precursor is neurohypophysial prolactin releasing factor. Biochem. Biophys. Res. Commun. 1988, 151, 524–529. [Google Scholar] [CrossRef]
- Hyde, J.F.; North, W.G.; Ben-Jonathan, N. The vasopressin-associated glycopeptide is not a prolactin-releasing factor: Studies with lactating Brattleboro rats. Endocrinology 1989, 125, 35–40. [Google Scholar] [CrossRef]
- Parodi, A.J. Protein glucosylation and its role in protein folding. Annu. Rev. Biochem. 2000, 69, 69–93. [Google Scholar] [CrossRef] [PubMed]
- Barat, C.; Simpson, L.; Breslow, E. Properties of human vasopressin precursor constructs: Inefficient monomer folding in the absence of copeptin as a potential contributor to diabetes insipidus. Biochemistry 2004, 43, 8191–8203. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, N.G. Copeptin–Biochemistry and Clinical Diagnostics. In UNI-MED, 1st ed.; UNI-MED Verlag AG: Bremen, Germany, 2014; ISBN 978-3-8374-2286-3. [Google Scholar]
- Fenske, W.K.; Schnyder, I.; Koch, G.; Walti, C.; Pfister, M.; Kopp, P.; Fassnacht, M.; Strauss, K.; Christ-Crain, M.J. Release and Decay Kinetics of Copeptin vs. AVP in Response to Osmotic Alterations in Healthy Volunteers. Clin. Endocrinol. Metab. 2018, 103, 505–513. [Google Scholar] [CrossRef]
- Szinnai, G.; Morgenthaler, N.G.; Berneis, K.; Struck, J.; Müller, B.; Keller, U.; Christ-Crain, M.J. Changes in plasma copeptin, the c-terminal portion of arginine vasopressin during water deprivation and excess in healthy subjects. Clin. Endocrinol. Metab. 2007, 92, 3973–3978. [Google Scholar] [CrossRef]
- Balanescu, S.; Kopp, P.; Gaskill, M.B.; Morgenthaler, N.G.; Schindler, C.; Rutishauser, J. Correlation of plasma copeptin and vasopressin concentrations in hypo-, iso-, and hyperosmolar States. J. Clin. Endocrinol. Metab. 2011, 96, 1046–1052. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Müller, B.; Struck, J.; Bergmann, A.; Redl, H.; Christ-Crain, M. Copeptin, a stable peptide of the arginine vasopressin precursor, is elevated in hemorrhagic and septic shock. Shock 2007, 28, 219–226. [Google Scholar] [CrossRef]
- Melmed, S. The Pituitary. In Blackwell Science, 1st ed.; Blackwell Science: Hoboken, NJ, USA, 1995; ISBN 0-86542-126-9. [Google Scholar]
- Melmed, S. The immuno-neuroendocrine interface. Series introduction. J. Clin. Investig. 2001, 108, 1563–1566. [Google Scholar] [CrossRef] [PubMed]
- René, P.; de Keyzer, Y. The vasopressin receptor of corticotroph pituitary cells. Prog Brain Res. 2002, 139, 345–357. [Google Scholar]
- Sivukhina, E.V.; Jirikowski, G.F. Magnocellular hypothalamic system and its interaction with the hypothalamo-pituitary-adrenal axis. Steroids 2016, 111, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Otubo, A.; Kawakami, N.; Maejima, S.; Ueda, Y.; Morris, J.F.; Sakamoto, T.; Sakamoto, H. Vasopressin gene products are colocalised with corticotropin-releasing factor within neurosecretory vesicles in the external zone of the median eminence of the Japanese macaque monkey (Macaca fuscata). J. Neuroendocrinol. 2020, 32, e12875. [Google Scholar] [CrossRef] [PubMed]
- Beglinger, S.; Drewe, J.; Christ-Crain, M. The Circadian Rhythm of Copeptin, the C-Terminal Portion of Arginine Vasopressin. J. Biomark. 2017, 2017, 4737082. [Google Scholar] [CrossRef] [PubMed]
- Darzy, K.H.; Dixit, K.C.; Shalet, S.M.; Morgenthaler, N.G.; Brabant, G. Circadian secretion pattern of copeptin, the C-terminal vasopressin precursor fragment. Clin. Chem. 2010, 56, 1190–1191. [Google Scholar] [CrossRef]
- Katan, M.; Morgenthaler, N.G.; Dixit, K.C.; Rutishauser, J.; Brabant, G.E.; Müller, B.; Christ-Crain, M. Anterior and posterior pituitary function testing with simultaneous insulin tolerance test and a novel copeptin assay. J. Clin. Endocrinol. Metab. 2007, 92, 2640–2643. [Google Scholar] [CrossRef]
- Drummond, J.B.; Soares, B.S.; Pedrosa, W.; Vieira, E.L.M.; Teixeira, A.L.; Christ-Crain, M.; Ribeiro-Oliveira, A., Jr. Copeptin response to hypoglycemic stress is linked to prolactin activation in children. Pituitary 2020, 23, 681–690. [Google Scholar] [CrossRef]
- Lewandowski, K.C.; Lewiński, A.; Skowrońska-Jóźwiak, E.; Stasiak, M.; Horzelski, W.; Brabant, G. Copeptin under glucagon stimulation. Endocrine 2016, 52, 344–351. [Google Scholar] [CrossRef]
- Kacheva, S.; Kolk, K.; Morgenthaler, N.G.; Brabant, G.; Karges, W. Gender-specific co-activation of arginine vasopressin and the hypothalamic-pituitary-adrenal axis during stress. Clin. Endocrinol. 2015, 82, 570–576. [Google Scholar] [CrossRef]
- Robertson, G.L.; Mahr, E.A.; Athar, S.; Sinha, T. Development and clinical application of a new method for the radioimmunoassay of arginine vasopressin in human plasma. J. Clin. Investig. 1973, 52, 2340–2352. [Google Scholar] [CrossRef]
- Kluge, M.; Riedl, S.; Erhart-Hofmann, B.; Hartmann, J.; Waldhauser, F. Improved extraction procedure and RIA for determination of arginine-vasopressin in plasma: Role of premeasurement sample treatment and reference values in children. Clin. Chem. 1999, 45, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, N.G.; Struck, J.; Alonso, C.; Bergmann, A. Assay for the measurement of copeptin, a stable peptide derived from the precursor of vasopressin. Clin. Chem. 2006, 52, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Walti, C.; Siegenthaler, J.; Christ-Crain, M. Copeptin levels are independent of ingested nutrient type after standardised meal administration–the CoMEAL study. Biomarkers 2014, 19, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Blum, C.A.; Mirza, U.; Christ-Crain, M.; Mueller, B.; Schindler, C.; Puder, J.J. Copeptin levels remain unchanged during the menstrual cycle. PLoS ONE 2014, 9, e98240. [Google Scholar] [CrossRef]
- Roussel, R.; Fezeu, L.; Marre, M.; Velho, G.; Fumeron, F.; Jungers, P.; Lantieri, O.; Balkau, B.; Bouby, N.; Bankir, L.; et al. Comparison between copeptin and vasopressin in a population from the community and in people with chronic kidney disease. J. Clin. Endocrinol. Metab. 2014, 99, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Christ-Crain, M. Vasopressin and Copeptin in health and disease. Rev. Endocr. Metab. Disord. 2019, 20, 283–294. [Google Scholar] [CrossRef]
- Morgenthaler, N.G.; Struck, J.; Jochberger, S.; Dünser, M.W. Copeptin: Clinical use of a new biomarker. Trends Endocrinol. Metab. 2008, 19, 43–49. [Google Scholar] [CrossRef]
- Katan, M.; Christ-Crain, M. The stress hormone copeptin: A new prognostic biomarker in acute illness. Swiss Med. Wkly. 2010, 140, w13101. [Google Scholar] [CrossRef]
- Struck, J.; Morgenthaler, N.G.; Bergmann, A. Copeptin, a stable peptide derived from the vasopressin precursor, is elevated in serum of sepsis patients. Peptides 2005, 26, 2500–2504. [Google Scholar] [CrossRef]
- Jochberger, S.; Morgenthaler, N.G.; Mayr, V.D.; Luckner, G.; Wenzel, V.; Ulmer, H.; Schwarz, S.; Hasibeder, W.R.; Friesenecker, B.E.; Dünser, M.W. Copeptin and arginine vasopressin concentrations in critically ill patients. J. Clin. Endocrinol. Metab. 2006, 91, 4381–4386. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Dong, G.; Zhao, X.; Wang, M.; Li, C.S. Prognostic significance of hypothalamic-pituitary-adrenal axis hormones in early sepsis: A study performed in the emergency department. Intensive Care Med. 2014, 40, 1499–1508. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, A.T.; Guaraldi, F.; Filippini, C.; Tesio, R.; Settanni, F.; Lucchiari, M.; Mengozzi, G.; Grottoli, S.; Ghigo, E.; Mascia, L. Activation of pituitary axis according to underlying critical illness and its effect on outcome. J. Crit. Care 2019, 54, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Zampino, R.; Iossa, D.; Ursi, M.P.; Bertolino, L.; Andini, R.; Molaro, R.; Fabrazzo, O.; Leonardi, S.; Atripaldi, L.; Durante-Mangoni, E. Prognostic value of pro-adrenomedullin and copeptin in acute infective endocarditis. BMC Infect. Dis. 2021, 21, 23. [Google Scholar] [CrossRef]
- Dong, X.Q.; Huang, M.; Yang, S.B.; Yu, W.H.; Zhang, Z.Y. Copeptin is associated with mortality in patients with traumatic brain injury. J. Trauma 2011, 71, 1194–1198. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, H.; Li, Y.; Zhang, H.; Liu, X.; Zhu, L.; Dong, L. The diagnosis and prognostic value of plasma copeptin in traumatic brain injury: A systematic review and meta-analysis. Neurol. Sci. 2021, 42, 539–551. [Google Scholar] [CrossRef]
- Zhu, X.D.; Chen, J.S.; Zhou, F.; Liu, Q.C.; Chen, G.; Zhang, J.M. Detection of copeptin in peripheral blood of patients with aneurysmal subarachnoid hemorrhage. Crit. Care 2011, 15, R288. [Google Scholar] [CrossRef]
- Fung, C.; De Marchis, G.M.; Katan, M.; Seiler, M.; Arnold, M.; Gralla, J.; Raabe, A.; Beck, J. Copeptin as a marker for severity and prognosis of aneurysmal subarachnoid hemorrhage. PLoS ONE 2013, 8, e53191. [Google Scholar] [CrossRef]
- Zuo, Z.; Ji, X. Prognostic value of copeptin in patients with aneurysmal subarachnoid hemorrhage. J. Neuroimmunol. 2019, 330, 116–122. [Google Scholar] [CrossRef]
- Jabbarli, R.; Pierscianek, D.; Darkwah Oppong, M.; Sato, T.; Dammann, P.; Wrede, K.H.; Kaier, K.; Köhrmann, M.; Forsting, M.; Kleinschnitz, C.; et al. Laboratory biomarkers of delayed cerebral ischemia after subarachnoid hemorrhage: A systematic review. Neurosurg. Rev. 2020, 43, 825–833. [Google Scholar] [CrossRef]
- Rhim, J.K.; Youn, D.H.; Kim, B.J.; Kim, Y.; Kim, S.; Kim, H.C.; Jeon, J.P. The Role of Consecutive Plasma Copeptin Levels in the Screening of Delayed Cerebral Ischemia in Poor-Grade Subarachnoid Hemorrhage. Life 2021, 11, 274. [Google Scholar] [CrossRef]
- Dong, X.; Huang, M.; Yu, W.; Zhang, Z.; Zhu, Q.; Che, Z.; Du, Q.; Wang, H. Change in plasma copeptin level after acute spontaneous basal ganglia hemorrhage. Peptides 2011, 32, 253–257. [Google Scholar] [CrossRef]
- Zhang, X.; Lu, X.; Huang, L.; Ye, H. Copeptin is associated with one-year mortality and functional outcome in patients with acute spontaneous basal ganglia hemorrhage. Peptides 2012, 33, 336–341. [Google Scholar] [CrossRef]
- Zhang, A.; Li, J.; Li, X.; Song, L.; Li, H. The prognostic value of copeptin for acute intracerebral hemorrhage patients. Exp. Ther. Med. 2013, 5, 467–470. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Colson, P.H.; Bernard, C.; Struck, J.; Morgenthaler, N.G.; Albat, B.; Guillon, G. Post cardiac surgery vasoplegia is associated with high preoperative copeptin plasma concentration. Crit. Care 2011, 15, R255. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.D.; Juhn, M.; Bergmann, S.; Katzke, S.; Weise, M.; Alakel, N.; Stölzel, F.; Kroschinsky, F.; Ehninger, G.; Höffken, G.; et al. Net reclassification improvement with serial biomarkers and bedsided spirometry to early predict the need of organ support during the early post-transplantation in-hospital stay in allogeneic HCT recipients. Bone Marrow Transpl. 2019, 54, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Pasero, D.; Berton, A.M.; Motta, G.; Raffaldi, R.; Fornaro, G.; Costamagna, A.; Toscano, A.; FIlippini, C.; Mengozzi, G.; Prencipe, N.; et al. Neuroendocrine predictors of vasoplegia after cardiopulmonary bypass. J. Endocrinol. Invest. 2020, 44, 1533–1541. [Google Scholar] [CrossRef] [PubMed]
- Ristagno, G.; Latini, R.; Plebani, M.; Zaninotto, M.; Vaahersalo, J.; Masson, S.; Tianinen, M.; Kurola, J.; Gaspari, F.; Milani, V.; et al. Copeptin levels are associated with organ dysfunction and death in the intensive care unit after out-of-hospital cardiac arrest. Crit. Care 2015, 19, 132. [Google Scholar] [CrossRef] [PubMed]
- Düring, J.; Annborn, M.; Cronberg, T.; Dankiewicz, J.; Devaux, Y.; Hassager, C.; Horn, J.; Kjaergaard, J.; Kuiper, M.; Nikoukhah, H.R.; et al. Copeptin as a marker of outcome after cardiac arrest: A sub-study of the TTM trial. Crit Care. 2020, 24, 185. [Google Scholar] [CrossRef]
- Paramanathan, S.; Grejs, A.M.; Jeppesen, A.N.; Søreide, E.; Kirkegaard, H.; Duez, C.H.V. Copeptin as a Prognostic Marker in Prolonged Targeted Temperature Management after Out-of-Hospital Cardiac Arrest. Ther. Hypothermia Temp. Manag. 2020. [Google Scholar] [CrossRef]
- Kalkan, A.K.; Ozturk, D.; Erturk, M.; Kalkan, M.E.; Cakmak, H.A.; Oner, E.; Uzun, F.; Tasbulak, O.; Yakisan, T.; Celik, A. The diagnostic value of serum copeptin levels in an acute pulmonary embolism. Cardiol. J. 2016, 23, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Wyzgał, A.; Koć, M.; Pacho, S.; Bielecki, M.; Wawrzyniak, R.; Kostrubiec, M.; Ciurzyński, M.; Kurnicka, K.; Goliszek, S.; Paczyńska, M.; et al. Plasma copeptin for short term risk stratification in acute pulmonary embolism. J. Thromb. Thrombolys. 2016, 41, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Hellenkamp, K.; Schwung, J.; Rossmann, H.; Kaeberich, A.; Wachter, R.; Hasenfuß, G.; Konstantinides, S.; Lankeit, M. Risk stratification of normotensive pulmonary embolism: Prognostic impact of copeptin. Eur. Respir. J. 2015, 46, 1701–1710. [Google Scholar] [CrossRef]
- Hellenkamp, K.; Pruszczyk, P.; Jiménez, D.; Wyzgał, A.; Barrios, D.; Ciurzyński, M.; Morillo, R.; Hobohm, L.; Keller, K.; Kurnicka, K.; et al. Prognostic impact of copeptin in pulmonary embolism: A multicentre validation study. Eur. Respir. J. 2018, 53. [Google Scholar] [CrossRef] [PubMed]
- Deveci, F.; Öner, Ö.; Telo, S.; Kırkıl, G.; Balin, M.; Kuluöztürk, M. Prognostic value of copeptin in patients with acute pulmonary thromboembolism. Clin. Respir. J. 2019, 13, 630–636. [Google Scholar] [CrossRef]
- Muller, B.; Morgenthaler, N.; Stolz, D.; Schuetz, P.; Müller, C.; Bingisser, R.; Bergmann, A.; Tamm, M.; Christ-Crain, M. Circulating levels of copeptin, a novel biomarker, in lower respiratory tract infections. Eur. J. Clin. Investig. 2007, 37, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Krüger, S.; Papassotiriou, J.; Marre, R.; Richter, K.; Schumann, C.; von Baum, H.; Morgenthaler, N.G.; Suttorp, R.; Welte, T.; CAPNETZ Study Group. Pro-atrial natriuretic peptide and pro-vasopressin to predict severity and prognosis in community-acquired pneumonia: Results from the German competence network CAPNETZ. Intensive Care Med. 2007, 33, 2069–2078. [Google Scholar] [CrossRef] [PubMed]
- Masiá, M.; Papassotiriou, J.; Morgenthalr, N.G.; Hernández, I.; Shum, C.; Gutiérrez, F. Midregional pro-A-type natriuretic peptide and carboxy-terminal provasopressin may predict prognosis in community-acquired pneumonia. Clin. Chem. 2007, 53, 2193–2201. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, P.; Wolbers, M.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; Widmer, I.; Neidert, S.; Fricker, T.; Blum, C.; Schild, U. Prohormones for prediction of adverse medical outcome in community-acquired pneumonia and lower respiratory tract infections. Crit. Care 2010, 14, R106. [Google Scholar] [CrossRef]
- Kruger, S.; Ewig, S.; Kunde, J.; Hartmann, O.; Suttorp, N.; Welte, T.; CAPNETZ Study Group. Pro-atrial natriuretic peptide and pro-vasopressin for predicting short-term and long-term survival in community-acquired pneumonia: Results from the German Competence Network CAPNETZ. Thorax 2010, 65, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Kolditz, M.; Ewig, S.; Hoffken, G. Management-based risk prediction in community-acquired pneumonia by scores and biomarkers. Eur. Respir. J. 2013, 41, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Stolz, D.; Christ-Crain, M.; Morgenthaler, N.G.; Leuppi, J.; Miedinger, D.; Bingisser, R.; Müller, C.; Struck, J.; Müller, B.; Tamm, M. Copeptin, C-reactive protein, and procalcitonin as prognostic biomarkers in acute exacerbation of COPD. Chest 2007, 131, 1058–1067. [Google Scholar] [CrossRef]
- Wojsyk-Banaszak, I.; Sobkowiak, P.; Jończyk-Potoczna, K.; Narożna, B.; Langwiński, W.; Szczepanik, M.; Kycler, Z.; Bręborowicz, A.; Szczepankiewicz, A. Evaluation of Copeptin during Pulmonary Exacerbation in Cystic Fibrosis. Mediat. Inflamm. 2019, 2019, 1939740. [Google Scholar] [CrossRef]
- Kuluöztürk, M.; İn, E.; Telo, S.; Karabulut, E.; Geçkil, A.A. Efficacy of copeptin in distinguishing COVID-19 pneumonia from community-acquired pneumonia. J. Med. Virol. 2021, 93, 3113–3121. [Google Scholar] [CrossRef] [PubMed]
- Karakioulaki, M.; Grendelmeier, P.; Strobel, W.; Schmid, T.; Jahn, K.; Grize, L.; Tamm, M.; Stolz, D. Copeptin, pro-atrial natriuretic peptide and pro-adrenomedullin as markers of hypoxic stress in patients with obstructive sleep apnea—A prospective intervention study. Respir. Res. 2021, 22, 114. [Google Scholar] [CrossRef]
- Cinarka, H.; Kayah, S.; Karatas, M.; Yavuz, A.; Gümüş, A.; Özyurt, S.; Cüre, M.C.; Şahin, Ü. Copeptin: A new predictor for severe obstructive sleep apnea. Ther. Clin. Risk Manag. 2015, 11, 589–594. [Google Scholar]
- Osma, Ü.; Selçuk, Ö.T.; Eyigör, M.; Renda, L.; Selçuk, N.T.; Eyigör, H.; Yılmaz, M.D.; İlden, O.; Işık, Ü.G.; Ünlü, H.K.; et al. Do serum copeptin levels change with positive airway pressure treatment in patients with severe obstructive sleep apnea? Tr-ENT 2020, 30, 52–57. [Google Scholar] [CrossRef]
- Selçuk, Ö.T.; Eyigör, M.; Renda, L.; Osma, U.; Eyigor, H.; Selcuk, N.T.; Yılmaz, M.D.; Demirkıran, C.; Unlu, H.; Gültekin, M. Can we use serum copeptin levels as a biomarker in obstructive sleep apnea syndrome? J. Craniomaxillofac. Surg. 2015, 43, 879–882. [Google Scholar] [CrossRef]
- Dobsa, L.; Cullen Edozien, K. Copeptin and its potential role in diagnosis and prognosis of various diseases. Biochem. Med. 2013, 23, 172–190. [Google Scholar] [CrossRef]
- Bolignano, D.; Cabassi, A.; Fiaccadori, E.; Ghigo, E.; Pasquali, R.; Peracino, A.; Peri, A.; Plebani, M.; Santoro, A.; Settanni, F.; et al. Copeptin (CTproAVP), a new tool for understanding the role of vasopressin in patophysiology. Clin. Chem. Lab. Med. 2014, 52, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Wang, R.; Yan, L.; Lin, M.; Liu, X.; You, T. Copeptin in heart failure: Review and meta-analysis. Clin. Chim. Acta 2017, 475, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Zabarovskaja, S.; Hage, C.; Gabrielsen, A.; Mellbin, L.; Lund, L.H. Copeptin in Heart Failure, Post-Left Ventricular Assist Device and Post-Heart Transplantation. Heart Lung Circ. 2017, 26, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, C.; Deveci, O.S.; Tepe, O.; Yesildas, C.; Ünal, I.; Yıldız, I.; Akıllı, R.E.; Deniz, A.; Demir, M.; Kanadaşı, M.; et al. Prognostic performance of copeptin among patients with acute decompensated heart failure. Acta Cardiol. 2020. [Google Scholar] [CrossRef]
- Gegenhuber, A.; Struck, J.; Dieplinger, B.; Poelz, W.; Pacher, R.; Morgenthaler, N.G.; Bergmann, A.; Haltmayer, M.; Mueller, T. Comparative evaluation of B-type natriuretic peptide, mid-regional pro-A-type natriuretic peptide, mid-regional pro-adrenomedullin, and Copeptin to predict 1-year mortality in patients with acute destabilized heart failure. J. Card. Fail. 2007, 13, 42–49. [Google Scholar] [CrossRef]
- Dungen, H.D.; Tscholl, V.; Obradovic, D.; Radenovic, S.; Matic, D.; Musial Bright, L.; Tahirovic, E.; Marx, A.; Inkrot, S.; Hashemi, D.; et al. Prognostic performance of serial in-hospital measurements of copeptin and multiple novel biomarkers among patients with worsening heart failure: Results from the MOLITOR study. ESC Heart Fail. 2018, 5, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Fu, F.; Chen, H.; Zhu, B. Copeptin in the assessment of acute lung injury and cardiogenic pulmonary edema. Respir. Med. 2012, 106, 1268–1277. [Google Scholar] [CrossRef]
- Stoiser, B.; Mörtl, D.; Hülsmann, M.; Berger, R.; Struck, J.; Morgenthaler, N.G.; Bergmann, A.; Pacher, R. Copeptin, a fragment of the vasopressin precursor, as a novel predictor of outcome in heart failure. Eur. J. Clin. Investig. 2006, 36, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Masson, S.; Latini, R.; Carbonieri, E.; Moretti, L.; Rossi, M.G.; Ciricugno, S.; Milani, V.; Marchioli, R.; Struck, J.; Bergmann, A.; et al. GISSI-HF Investigators. The predictive value of stable precursor fragments of vasoactive peptides in patients with chronic heart failure: Data from the GISSI-heart failure (GISSI-HF) trial. Eur. J. Heart Fail. 2010, 12, 338–347. [Google Scholar] [CrossRef]
- Maisel, A.; Xue, Y.; Shah, K.; Mueller, C.; Nowak, R.; Peacock, W.F.; Ponikowski, P.; Mockel, M.; Hogan, C.; Wu, A.H.; et al. Increased 90-day mortality in patients with acute heart failure with elevated copeptin: Secondary results from the Biomarkers in Acute Heart Failure (BACH) study. Circ. Heart Fail. 2011, 4, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Tentzeris, I.; Jarai, R.; Farhan, S.; Perkmann, T.; Schwarz, M.A.; Jakl, G.; Wojta, J.; Huber, K. Complementary role of copeptin and high-sensitivity troponin in predicting outcome in patients with stable chronic heart failure. Eur. J. Heart Fail. 2011, 13, 726–733. [Google Scholar] [CrossRef] [PubMed]
- Neuhold, S.; Huelsmann, M.; Strunk, G.; Stoiser, B.; Struck, J.; Morgenthaler, N.G.; Bergmann, A.; Moertl, D.; Berger, R.; Pacher, R. Comparison of copeptin, B-type natriuretic peptide, and amino-terminal pro-B-type natriuretic peptide in patients with chronic heart failure: Prediction of death at different stages of the disease. J. Am. Coll. Cardiol. 2008, 52, 266–272. [Google Scholar] [CrossRef]
- Yoshikawa, Y.; Shiomi, H.; Kuwahara, K.; Sowa, N.; Yaku, H.; Yamashita, Y.; Tazaki, J.; Imai, M.; Kato, T.; Saito, N.; et al. Utility of copeptin for predicting long-term clinical outcomes in patients with heart failure. J. Cardiol. 2019, 73, 379–385. [Google Scholar] [CrossRef]
- Miller, W.L.; Grill, D.E.; Struck, J.; Jaffe, A.S. Association of hyponatremia and elevated copeptin with death and need for transplantation in ambulatory patients with chronic heart failure. Am. J. Cardiol. 2013, 111, 880–885. [Google Scholar] [CrossRef]
- Khan, S.Q.; Dhillon, O.S.; O’Brien, R.J.; Struck, J.; Quinn, P.A.; Morgenthaler, N.G.; Squire, I.B.; Davies, J.E.; Bergmann, A.; Ng, L.L. C-terminal provasopressin (copeptin) as a novel and prognostic marker in acute myocardial infarction: Leicester Acute Myocardial Infarction Peptide (LAMP) study. Circulation 2007, 115, 2103–2110. [Google Scholar] [CrossRef]
- Voors, A.A.; von Haehling, S.; Anker, S.D.; Hillege, H.L.; Struck, J.; Hartmann, O.; Bergmann, A.; Squire, I.; Van Veldhuisen, D.J.; Dickstein, K. OPTIMAAL Investigators. C-terminal provasopressin (copeptin) is a strong prognostic marker in patients with heart failure after an acute myocardial infarction: Results from the OPTIMAAL study. Eur. Heart J. 2009, 30, 1187–1194. [Google Scholar] [PubMed]
- Kelly, D.; Squire, I.B.; Khan, S.Q.; Quinn, P.; Struck, J.; Morgenthaler, N.G.; Davies, J.E. C-terminal provasopressin (copeptin) is associated with left ventricular dysfunction, remodeling, and clinical heart failure in survivors of myocardial infarction. J. Card. Fail. 2008, 14, 739–745. [Google Scholar] [CrossRef]
- Möckel, M.; Searle, J. Copeptin-marker of acute myocardial infarction. Curr. Atheroscler. Rep. 2014, 16, 421. [Google Scholar] [CrossRef]
- Reichlin, T.; Hochholzer, W.; Stelzig, C.; Laule, K.; Freidank, H.; Morgenthaler, N.G.; Bergmann, A.; Potocki, M.; Noveanu, M.; Breidthardt, T.; et al. Incremental value of copeptin for rapid rule out of acute myocardial infarction. J. Am. Coll. Cardiol. 2009, 54, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Keller, T.; Tzikas, S.; Zeller, T.; Czyz, E.; Lillpopp, L.; Ojeda, F.M.; Roth, A.; Bickel, C.; Baldus, S.; Sinning, C.R.; et al. Copeptin improves early diagnosis of acutemyocardial infarction. J. Am. Coll. Cardiol. 2010, 55, 2096–2106. [Google Scholar] [CrossRef]
- Karakas, M.; Januzzi, J.L., Jr.; Meyer, J.; Lee, H.; Schlett, C.L.; Truong, Q.A.; Rottbauer, W.; Bamberg, F.; Dasdemir, S.; Hoffmann, U.; et al. Copeptin does not add diagnostic information to high-sensitivity troponin T in low-to intermediate-risk patients with acute chest pain: Results from the Rule Out Myocardial Infarction by Computed Tomography (ROMICAT) study. Clin. Chem. 2011, 57, 1137–1145. [Google Scholar] [CrossRef]
- Bahrmann, P.; Bahrmann, A.; Breithardt, O.A.; Daniel, W.G.; Christ, M.; Sieber, C.C.; Bertsch, T. Additional diagnostic and prognostic value of copeptin ultra-sensitive for diagnosis of non-ST-elevation myocardial infarction in older patients presenting to the emergency department. Clin. Chem. Lab. Med. 2013, 51, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Árnadóttir, Á.; Pedersen, S.; Bo Hasselbalch, R.; Goetze, J.P.; Friis-Hansen, L.J.; Bloch-Münster, A.M.; Skov Jensen, J.; Bundgaard, H.; Iversen, K. Temporal Release of High-Sensitivity Cardiac Troponin T and I and Copeptin After Brief Induced Coronary Artery Balloon Occlusion in Humans. Circulation 2021, 143, 1095–1104. [Google Scholar] [CrossRef] [PubMed]
- Bohyn, E.; Dubie, E.; Lebrun, C.; Jund, J.; Beaune, G.; Lesage, P.; Belle, L.; Savary, D. Expeditious exclusion of acute coronary syndrome diagnosis by combined measurements of copeptin, highsensitivity troponin, and GRACE score. Am. J. Emerg. Med. 2014, 32, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Möckel, M.; Searle, J.; Hamm, C.; Slagman, A.; Blankenberg, S.; Huber, K.; Katus, H.; Liebetrau, C.; Müller, C.; Muller, R.; et al. Early discharge using single cardiac troponin and copeptin testing in patients with suspected acute coronary syndrome (ACS): A randomized, controlled clinical process study. Eur. Heart J. 2014, 36, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Hennessen, M.; Lindahl, B.; Giannitsis, E.; Vafaie, M.; Biener, M.; Haushofer, A.C.; Seier, J.; Christ, M.; Alquézar-Arbé, A.; deFilippi, C.R.; et al. Combined testing of copeptin and high-sensitivity cardiac troponin T at presentation in comparison to other algorithms for rapid rule-out of acute myocardial infarction. Int. J. Cardiol. 2019, 276, 261–267. [Google Scholar] [CrossRef]
- Giannitsis, E.; Clifford, P.; Slagman, A.; Ruedelstein, R.; Liebetrau, C.; Hamm, C.; Honnart, D.; Huber, K.; Vollert, J.O.; Simonelli, C.; et al. Multicentre cross-sectional observational registry to monitor the safety of early discharge after rule-out of acute myocardial infarction by copeptin and troponin: The Pro-Core registry. BMJ Open 2019, 9, e028311. [Google Scholar] [CrossRef]
- Maisel, A.; Mueller, C.; Neath, S.X.; Christenson, R.H.; Morgenthaler, N.G.; McCord, J.; Nowak, R.M.; Vilke, G.; Daniels, L.B.; Hollander, J.E.; et al. Copeptin helps in the early detection of patients with acute myocardial infarction: Primary results of the CHOPIN trial (Copeptin Helps in the early detection Of Patients with acute myocardial INfarction). J. Am. Coll. Cardiol. 2013, 62, 150–160. [Google Scholar] [CrossRef]
- Chenevier-Gobeaux, C.; Freund, Y.; Claessens, Y.E.; Guerin, S.; Bonnet, P.; Doumenc, B.; Leumani, F.; Cosson, C.; Allo, J.C.; Riou, B.; et al. Copeptin for rapid rule out of acute myocardial infarction in emergency department. Int. J. Cardiol. 2013, 166, 198–204. [Google Scholar] [CrossRef]
- Wildi, K.; Boeddinghaus, J.; Nestelberger, T.; Twerenbold, R.; Badertscher, P.; Wussler, D.; Giménez, M.R.; Puelacher, C.; de Lavallaz, J.D.F.; Dietsche, S.; et al. Comparison of fourteen rule-out strategies for acute myocardial infarction. Int. J. Cardiol. 2019, 283, 41–47. [Google Scholar] [CrossRef]
- Giannitsis, E.; Huber, K.; Hamm, C.W.; Möckel, M. Instant rule-out of suspected non-ST-segment elevation myocardial infarction using high-sensitivity cardiac troponin T with Copeptin versus a single low high-sensitivity cardiac troponin T: Findings from a large pooled individual data analysis on 10,329 patients. Clin. Res. Cardiol. 2021, 110, 194–199. [Google Scholar] [PubMed]
- Lattuca, B.; Sy, V.; Nguyen, L.S.; Bernard, M.; Zeitouni, M.; Overtchouk, P.; Yan, Y.; Hammoudi, N.; Ceccaldi, A.; Collet, J.P.; et al. Copeptin as a prognostic biomarker in acute myocardial infarction. Int. J. Cardiol. 2019, 274, 337–341. [Google Scholar] [CrossRef]
- Frydland, M.; Møller, J.E.; Lindholm, M.G.; Hansen, R.; Wiberg, S.; Lerche Helgestad, O.K.; Thomsen, J.H.; Goetze, J.P.; Engstrøm, T.; Frikke-Schmidt, R.; et al. Biomarkers predictive of late cardiogenic shock development in patients with suspected ST-elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care. 2020, 9, 557–566. [Google Scholar] [CrossRef]
- Lu, J.; Wang, S.; He, G.; Wang, Y. Prognostic value of copeptin in patients with acute coronary syndrome: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0238288. [Google Scholar] [CrossRef]
- Johansson, A.; Olsson, T.; Carlberg, B.; Karlsson, K.; Fagerlund, M. Hypercortisolism after stroke–partly cytokine-mediated? J. Neurol. Sci. 1997, 147, 43–47. [Google Scholar] [CrossRef]
- Johansson, A.; Ahren, B.; Nasman, B.; Carlstrom, K.; Olsson, T. Cortisol axis abnormalities early after stroke–relationships to cytokines and leptin. J. Intern. Med. 2000, 247, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Slowik, A.; Turaj, W.; Pankiewicz, J.; Dziedzic, T.; Szermer, P.; Szczudlik, A. Hypercortisolemia in acute stroke is related to the inflammatory response. J. Neurol. Sci. 2002, 196, 27–32. [Google Scholar] [CrossRef]
- Fassbender, K.; Schmidt, R.; Mossner RDaffertshofer, M.; Hennerici, M. Pattern of activation of the hypothalamic-pituitaryadrenal axis in acute stroke. Relation to acute confusional state, extent of brain damage, and clinical outcome. Stroke 1994, 25, 1105–1108. [Google Scholar] [CrossRef]
- Spagnolello, O.; De Michele, M.; Lorenzano, S.; Cerulli Irelli, E.; Naitana, F.; Falcou, A.; Letteri, F.; Bachetoni, A.; Collepardo, D.; Bertazzoni, G.; et al. Copeptin Kinetics in Acute Ischemic Stroke May Differ According to Revascularization Strategies: Pilot Data. Stroke 2019, 50, 3632–3635. [Google Scholar] [CrossRef] [PubMed]
- Montellano, F.A.; Ungethüm, K.; Ramiro, L.; Nacu, A.; Hellwig, S.; Fluri, F.; Whiteley, W.N.; Bustamante, A.; Montaner, J.; Heuschmann, P.U. Role of Blood-Based Biomarkers in Ischemic Stroke Prognosis: A Systematic Review. Stroke 2021, 52, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Katan, M.; Fluri, F.; Morgenthaler, N.G.; Schuetz, P.; Zweifel, C.; Bingisser, R.; Müller, K.; Meckel, S.; Gass, A.; Kappos, L.; et al. Copeptin: A novel, independent prognostic marker in patients with ischemic stroke. Ann. Neurol. 2009, 66, 799–808. [Google Scholar] [CrossRef]
- De Marchis, G.M.; Dankowski, T.; König, I.R.; Fladt, J.; Fluri, F.; Gensicke, H.; Foerch, C.; Findling, O.; Kurmann, R.; Fischer, U.; et al. A novel biomarker-based prognostic score in acute ischemic stroke: The CoRisk score. Neurology 2019, 92, e1517–e1525. [Google Scholar] [CrossRef]
- Hotter, B.; Hoffmann, S.; Ulm, L.; Montaner, J.; Bustamante, A.; Meisel, C.; Meisel, A. Inflammatory and stress markers predicting pneumonia, outcome, and etiology in patients with stroke: Biomarkers for predicting pneumonia, functional outcome, and death after stroke. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e692. [Google Scholar] [CrossRef]
- Hotter, B.; Hoffmann, S.; Ulm, L.; Meisel, C.; Bustamante, A.; Montaner, J.; Katan, M.; Smith, C.J.; Meisel, A. External Validation of Five Scores to Predict Stroke-Associated Pneumonia and the Role of Selected Blood Biomarkers. Stroke 2021, 52, 325–330. [Google Scholar] [CrossRef]
- Purroy, F.; Suárez-Luis, I.; Cambray, S.; Farré, J.; Benabdelhak, I.; Mauri-Capdevila, G.; Sanahuja, J.; Quílez, A.; Begué, R.; Gil, M.I.; et al. The determination of copeptin levels helps management decisions among transient ischaemic attack patients. Acta Neurol. Scand. 2016, 134, 140–147. [Google Scholar] [CrossRef]
- Westermann, I.; Mw, D.; Haas, T.; Jochberger, S.; Luckner, G.; Mayr, V.; Wenzel, V.; Kh, S.; Innerhofer, P.; Morgenthaler, N.; et al. Endogenous vasopressin and copeptin response in multiple trauma patients. Shock 2007, 28, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Salvo, F.; Luppi, F.; Lucchesi, D.M.; Canovi, S.; Franchini, S.; Polese, A.; Santi, F.; Trabucco, L.; Fasano, T.; Ferrari, A.M. Serum Copeptin levels in the emergency department predict major clinical outcomes in adult trauma patients. BMC Emerg. Med. 2020, 20, 14. [Google Scholar] [CrossRef] [PubMed]
- Nass, R.D.; Motloch, L.J.; Paar, V.; Lichtenauer, M.; Baumann, J.; Zur, B.; Hoppe, U.C.; Holdenrieder, S.; Elger, C.E.; Surges, R. Blood markers of cardiac stress after generalized convulsive seizures. Epilepsia 2019, 60, 201–210. [Google Scholar] [CrossRef]
- Evers, K.S.; Hügli, M.; Fouzas, S.; Kasser, S.; Pohl, C.; Stoecklin, B.; Bernasconi, L.; Kuhle, J.; Wellmann, S. Serum Neurofilament Levels in Children With Febrile Seizures and in Controls. Front. Neurosci. 2020, 14, 579958. [Google Scholar] [CrossRef]
- Wellmann, S.; Benzing, J.; Cippà, G.; Admaty, D.; Creutzfeldt, R.; Mieth, R.A.; Beinder, E.; Lapaire, O.; Morgenthaler, N.G.; Haagen, U.; et al. High copeptin concentrations in umbilical cord blood after vaginal delivery and birth acidosis. J. Clin. Endocrinol. Metab. 2010, 95, 5091–5096. [Google Scholar] [CrossRef] [PubMed]
- Blohm, M.E.; Arndt, F.; Fröschle, G.M.; Langenbach, N.; Sandig, J.; Vettorazzi, E.; Mir, T.S.; Hecher, K.; Weil, J.; Kozlik-Feldmann, R.; et al. Cardiovascular Biomarkers in Amniotic Fluid, Umbilical Arterial Blood, Umbilical Venous Blood, and Maternal Blood at Delivery, and Their Reference Values for Full-Term, Singleton, Cesarean Deliveries. Front. Pediatr. 2019, 7, 271. [Google Scholar] [CrossRef]
- Schlapbach, L.J.; Frey, S.; Bigler, S.; Manh-Nhi, C.; Aebi, C.; Nelle, M.; Nuoffer, J.M. Copeptin concentration in cord blood in infants with early-onset sepsis, chorioamnionitis and perinatal asphyxia. BMC Pediatr. 2011, 11, 38. [Google Scholar] [CrossRef]
- Burkhardt, T.; Schwabe, S.; Morgenthaler, N.G.; Natalucci, G.; Zimmermann, R.; Wellmann, S. Copeptin: A marker for stress reaction in fetuses with intrauterine growth restriction. Am. J. Obstet. Gynecol. 2012, 207, 497.e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Rouatbi, H.; Zigabe, S.; Gkiougki, E.; Vranken, L.; Van Linthout, C.; Seghaye, M.C. Biomarkers of neonatal stress assessment: A prospective study. Early Hum. Dev. 2019, 137, 104826. [Google Scholar] [CrossRef]
- Vuohelainen, T.; Ojala, R.; Virtanen, A.; Holm, P.; Tammela, O. Predictors of delayed first voiding in newborn. Acta Paediatr. 2008, 97, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Kasser, S.; Hartley, C.; Rickenbacher, H.; Klarer, N.; Depoorter, A.; Datta, A.N.; Cobo, M.M.; Goksan, S.; Hoskin, A.; Magerl, W.; et al. Birth experience in newborn infants is associated with changes in nociceptive sensitivity. Sci. Rep. 2019, 9, 4117. [Google Scholar] [CrossRef] [PubMed]
- Hoffiz, Y.C.; Castillo-Ruiz, A.; Hall, M.A.L.; Hite, T.A.; Gray, J.M.; Cisternas, C.D.; Cortes, L.R.; Jacobs, A.J.; Forger, N.G. Birth elicits a conserved neuroendocrine response with implications for perinatal osmoregulation and neuronal cell death. Sci. Rep. 2021, 11, 2335. [Google Scholar] [CrossRef] [PubMed]
- Urwyler, S.A.; Schuetz, P.; Sailer, C.; Christ-Crain, M. Copeptin as a stress marker prior and after a written examination—The CoEXAM study. Stress 2015, 18, 134–137. [Google Scholar] [CrossRef]
- Siegenthaler, J.; Walti, C.; Urwyler, S.A.; Schuetz, P.; Christ-Crain, M. Copeptin concentrations during psychological stress: The PsyCo study. Eur. J. Endocrinol. 2014, 171, 737–742. [Google Scholar] [CrossRef][Green Version]
- Spanakis, E.K.; Wand, G.S.; Ji, N.; Golden, S.H. Association of HPA axis hormones with copeptin after psychological stress differs by sex. Psychoneuroendocrinology 2016, 63, 254–261. [Google Scholar] [CrossRef]
- Bae, Y.J.; Reinelt, J.; Netto, J.; Uhlig, M.; Willenberg, A.; Ceglarek, U.; Villringer, A.; Thiery, J.; Gaebler, M.; Kratzsch, J. Salivary cortisone, as a biomarker for psychosocial stress, is associated with state anxiety and heart rate. Psychoneuroendocrinology 2019, 101, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Goetze, J.P.; Støving, R.K. Copeptin in anorexia nervosa. Brain Behav. 2020, 10, e01551. [Google Scholar] [CrossRef] [PubMed]
- Tirabassi, G.; Boscaro, M.; Arnaldi, G. Harmful effects of functional hypercortisolism: A working hypothesis. Endocrine 2014, 46, 370–386. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Article; Year | Number of Patients | Aim | Conclusions | Prognostic Accuracy of Copeptin |
|---|---|---|---|---|
| Sepsis and septic shock | ||||
| Struck et al. [33]; 2005 | 50 healthy controls and 35 patients with septic shock | To quantify AVP release by means of a novel immunometric assay for copeptin in human serum and plasma | Plasma levels of copeptin were strongly elevated in septic shock patients as compared with healthy controls, but far more stable in serum and plasma than AVP. | |
| Morgenthaler et al. [12]; 2007 | 101 critically ill patients | To test the increase in copeptin levels in hemorrhagic and septic shock | Copeptin levels increased significantly with the severity of disease from infection without systemic inflammations to sepsis, severe sepsis and septic shock. Copeptin was higher in non-survivors than in survivors. | Outcome: in-hospital mortality Cut-off 96 pmol/L SE 61.5% SP 83.8% AUC 0.75 (95% CI 0.61–0.86) Multivariate logistic regression analyses:
|
| Jochberger et al. [34]; 2009 | 10 patients with infection, 22 with severe sepsis and 28 with septic shock | To compare the course of AVP and copeptin plasma concentrations between patients with infection, severe sepsis, and septic shock | Severe sepsis induced a stronger AVP response than infection without systemic inflammation. The lack of a difference in AVP plasma concentrations between patients with and without shock indicates that the AVP system does not function normally in severe sepsis. | |
| Zhang et al. [35]; 2014 | 461 patients referring to the emergency department with symptoms of systemic inflammatory response syndrome (SIRS) | To assess the predictive value of copeptin in determining sepsis progression and mortality in the emergency department | Increased copeptin at admission may provide crucial information for risk stratification in the different stages of sepsis. Copeptin is an independent prognostic biomarker for mortality in patients with severe sepsis or septic shock. | Outcome: septic shock Cut-off 96.5 pmol/L SE 78.9% SP 87.1% AUC 0.856 (95% CI 0.814–0.897) OR 1.034 (95% CI 1.023–1.044) p < 0.001 Outcome: 28-day mortality Cut-off 86.3 pmol/L SE 85.3% SP 59.8% AUC 0.826 (95% CI 0.780–0.871) OR 1.039 (95% CI 1.026–1.051) p < 0.001 |
| Mazzeo et al. [36]; 2019 | 11 critically ill patients admitted in ICU | To investigate the early activation of pituitary axes in response to stress. | Copeptin elevation was common and persistent in critical illnesses. Its magnitude changed according to the underlying condition (ARDS > TBI > SAH), but copeptin levels did not predict in-hospital mortality. | |
| Zampino et al. [37]; 2021 | 196 patients with infective endocarditis | To assess the prognostic role for copeptin and other biomarkers in infective endocarditis | Different biomarkers correlate with distinct outcomes in infective endocarditis. Copeptin may signal a worse prognosis and could be used to identify patients who need more aggressive treatment; it does not provide information on embolic risk or etiology. | Outcome: in-hospital mortality AUC 0.731 Outcome: 1-year mortality OR 2.55 (95% CI 1.18–5.54) p = 0.017. |
| Traumatic brain injury (TBI) | ||||
| Dong et al. [38]; 2011 | 94 patients with acute severe TBI and 50 healthy controls | To evaluate the relationship between copeptin levels and mortality after TBI | Copeptin levels were significantly higher in patients with TBI than in healthy controls. Among TBI patients, copeptin levels correlated inversely with GCS and were significantly higher in non-survivors after 1 month. | Outcome: 1-month mortality Cut-off 112 pmol/L SE 88.5% SP 75% AUC 0.874 (95% CI 0.789–0.933) OR 1.008 (95% CI 1.002–1.014) p = 0.010 |
| Zhang et al. [39]; 2021 | 2654 patients from 17 studies (meta-analysis) on TBI | To assess the diagnostic and prognostic value of plasma copeptin after TBI | Copeptin is a promising biomarker in the diagnosis and prognosis of TBI patients in terms of complications, mortality, poor functional outcome. | Outcome: brain concussion AUC 0.90 (95% CI 0.84–0.95) Outcome: progressive hemorrhagic injury AUC 0.83 (95% CI 0.80–0.87) Outcome: acute traumatic coagulopathy AUC 0.84 (95% CI 0.79–0.89) Outcome: mortality AUC 0.89 (0.87–0.92) Outcome: poor functional outcomes AUC 0.88 (95% CI 0.84–0.92) |
| Subarachnoid hemorrhage (SAH) | ||||
| Zhu et al. [40]; 2011 | 303 patients with an initial diagnosis of aneurysmal SAH | To investigate the ability of copeptin to predict disease outcome and brain vasospasm in patients with SAH. | Copeptin is a useful complementary tool for predicting functional outcome and mortality after SAH. | Outcome: in-hospital mortality Cut-off 28.7 pmol/L SE 78.1% SP 89.7% AUC 0.868 ± 0.042 Outcome: 1-year mortality Cut-off 20.5 pmol/L SE 92.8% SP 70.1% AUC 0.868 ± 0.036 OR 2.307 (95% CI 1.324–6.974) p = 0.004 Outcome: 1-year poor functional outcome Cut-off 23.8 pmol/L SE 82.2% SP 79.8% AUC 0.860 ± 0.026 Outcome: cerebrovasospasm Cut-off 23.4 pmol/L SE 69.2% SP 84.9% AUC 0.792 ± 0.027 |
| Fung et al. [41]; 2013 | 18 patients with aneurysmal SAH | To investigate the association between copeptin levels and the severity and prognosis of SAH. | Copeptin levels may indicate clinical severity of the initial bleeding, thus being helpful in guiding treatment decisions. | |
| Zuo et al. [42]; 2019 | 243 patients with aneurysmal SAH | To investigate the prognostic value of copeptin in patients with SAH | Copeptin is a promising biomarker in predicting short-term functional outcomes and mortality in SAH. | Outcome: 3-month poor functional outcome Cut-off 24 pmol/L SE 70.5% SP 69.6% AUC 0.74 (95% CI 0.67–0.81) OR 1.06 (95% CI 1.02–1.10) p < 0.001 Outcome: 3-month mortality AUC 0.81 (95% CI 0.74–0.87) OR 1.09 (95% CI 0.74–0.87) p < 0.001 Cut-off 31.2 pmol/L OR 4.13 (95% CI 1.75–7.12) |
| Jabbarli et al. [43]; 2020 | 16914 patients from 275 studies (systematic review) on SAH | To assess the predictive value of 257 biomarkers for delayed cerebral ischemia after SAH | Copeptin is one of the 15 non-genetic predictors of delayed cerebral ischemia after SAH with a level of evidence II. | |
| Rhim et al. [44]; 2021 | 86 patients with poor-grade SAH | To evaluate the prognostic power of copeptin in predicting delayed cerebral ischemia after SAH | If associated with transcranial doppler ultrasound, copeptin levels are of additive value in predicting the occurrence of delayed cerebral ischemia after SAH. | Outcome: delayed cerebral ischemia OR 1.022 (95% CI 1.008–1.037) p = 0.002 Performance of transcranial doppler: AUC 0.667 (95% CI 0.548–0.771) Performance of Copeptin with transcranial doppler: AUC 0.739 (95% CI 0.625–0.834) |
| Intracerebral hemorrhage (ICH) | ||||
| Dong et al. [45]; 2011 | 86 patients with acute ICH and 30 healthy controls | To investigate changes in plasma copeptin levels in patients during the initial 7-day period after ICH and also determine whether copeptin is an independent prognostic marker of mortality in ICH | Increased plasma copeptin is associated with hematoma volume and is an independent prognostic biomarker of mortality after ICH. | Outcome: 1-week mortality Cut-off 143.7 pmol/L SE 87.5% SP 72.2% AUC 0.873 (95% CI 0.784–0.935) OR 1.013 (95% CI 1.003–1.023) p = 0.009 |
| Zhang et al. [46]; 2012 | 89 patients with acute spontaneous basal ganglia hemorrhage and 50 healthy controls | To evaluate the relationship between plasma copeptin levels and both long-term outcome and early neurological deterioration after ICH | Increased plasma copeptin is an independent prognostic marker of 1-year mortality, 1-year unfavorable outcome and early neurological deterioration after ICH. | Outcome: 1-year mortality OR 1.138 (95% CI 1.063–1.345) p < 0.001 Outcome: 1-year poor functional outcome OR 1.191 (95% CI 1.102–1.323) p < 0.001 Outcome: early neurological deterioration OR 1.217 (95% CI 1.139–1.398) p < 0.001 |
| Zhang et al. [47]; 2013 | 120 patients with acute ICH | To examine the prognostic value of copeptin in acute ICH | Copeptin is correlated with clinical, biochemical and radiologic parameters of ICH severity. Copeptin levels are independent predictors of 90-day functional outcome in ICH patients. | Outcome: impaired nerve function OR 3.17 (95% CI 2.01–4.35) p = 0.003 Outcome: cerebral hemorrhage OR 1.28 (95% CI 1.05–1.48) p < 0.001 Outcome: 90-day mortality OR 5.29 (95% CI 3.68–8.03) p < 0.001 |
| Vasodilatory shock/post-surgical vasoplegia | ||||
| Colson et al. [48]; 2011 | 64 consecutive patients undergoing elective cardiopulmonary bypass surgery | To assess the prognostic value of preoperative copeptin levels for cardiovascular instability in the immediate post-surgical period | High preoperative copeptin levels are predictive of post cardiac surgery vasodilation and suggestive of the AVP system activation which predisposes patients to a relative AVP deficiency after surgical stress. | Outcome: post-cardiotomic vasoplegia Cut-off 9.43 pmol/L SE 90% SP 77% AUC 0.86 ± 0.04 (95% CI 0.78–0.94) |
| Braun et al. [49]; 2019 | To evaluate the prognostic value of copeptin levels for the early development of organ failure in patients undergoing allogeneic hematopoietic cell transplantation | Serial copeptin measurements improve the risk prediction for ICU admission for need for organ support as calculated by the continuous net reclassification improvement in allogeneic hematopoietic stem transplantation recipients. | Outcome: need for organ support Cut-off: 13.8 pmol/L SE 83% SP 71% AUC 0.820 | |
| Pasero et al. [50]; 2020 | 350 consecutive patients undergoing on-pump cardiac surgery | To assess the prognostic value of perioperative HPA axis parameters and copeptin levels for cardiovascular instability in the immediate post-surgical period | Higher preoperative copeptin levels, but not a reduced response to ACTH stimulation, are predictive for post-cardiotomic vasoplegia. | Outcome: post-cardiotomic vasoplegia Cut-off 16.9 pmol/L SE 89% SP 86% AUC 0.86 (95% CI 0.73–0.94) OR 1.17 (95% CI 1.04–1.32) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martino, M.; Arnaldi, G. Copeptin and Stress. Endocrines 2021, 2, 384-404. https://doi.org/10.3390/endocrines2040035
Martino M, Arnaldi G. Copeptin and Stress. Endocrines. 2021; 2(4):384-404. https://doi.org/10.3390/endocrines2040035
Chicago/Turabian StyleMartino, Marianna, and Giorgio Arnaldi. 2021. "Copeptin and Stress" Endocrines 2, no. 4: 384-404. https://doi.org/10.3390/endocrines2040035
APA StyleMartino, M., & Arnaldi, G. (2021). Copeptin and Stress. Endocrines, 2(4), 384-404. https://doi.org/10.3390/endocrines2040035