
Biometric Vibration Signal Detection Devices for Swallowing Activity Monitoring


Abstract
1. Introduction
2. Materials and Methods
2.1. Physical Analysis of Differential Signals
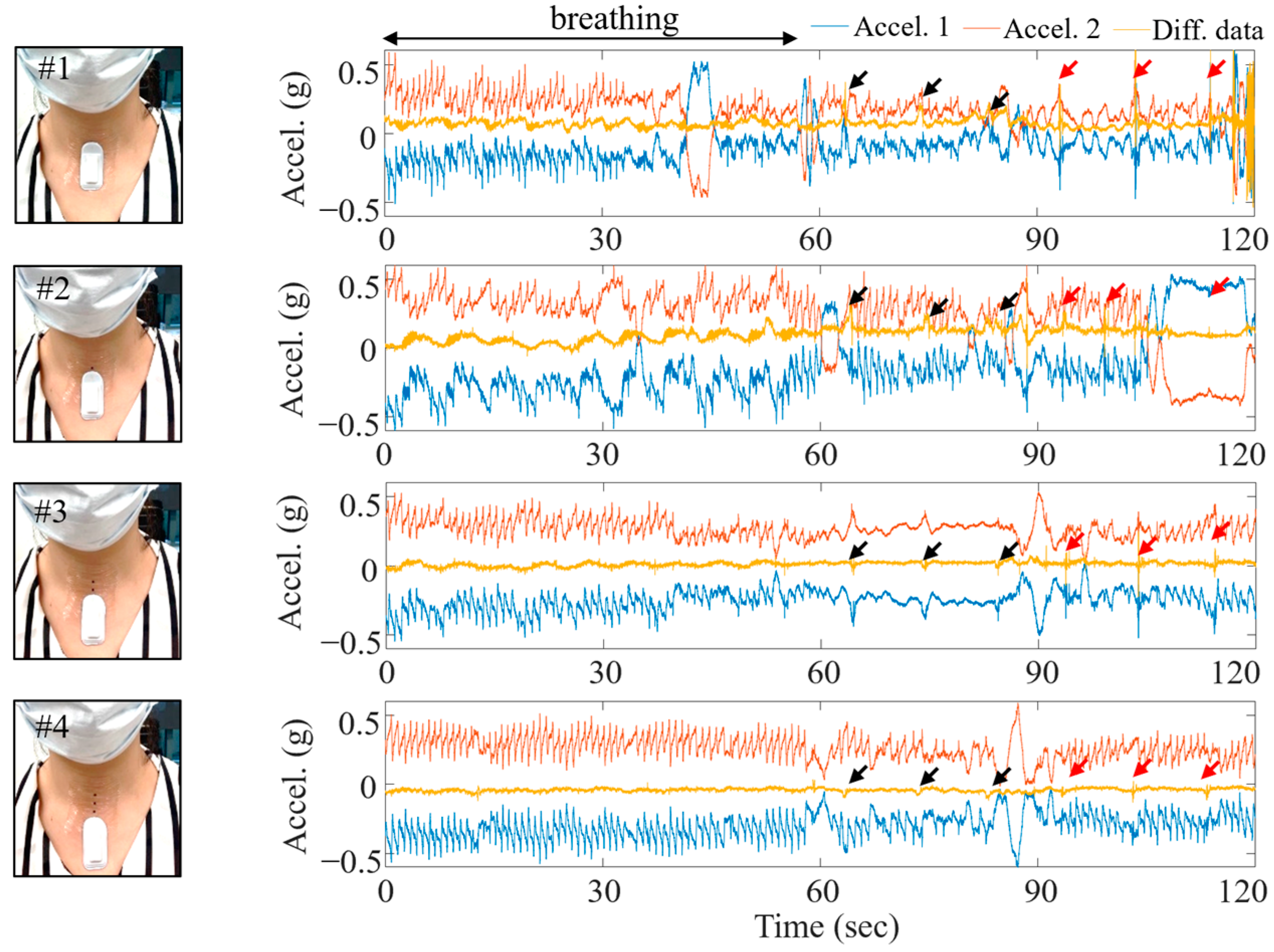
2.2. Location of Device Attachment to Acquire Biometric Vibration Signal
2.3. Data Collection
2.3.1. Protocol for Swallowing Test Scenario
2.3.2. Detection Algorithm
3. Results and Discussion
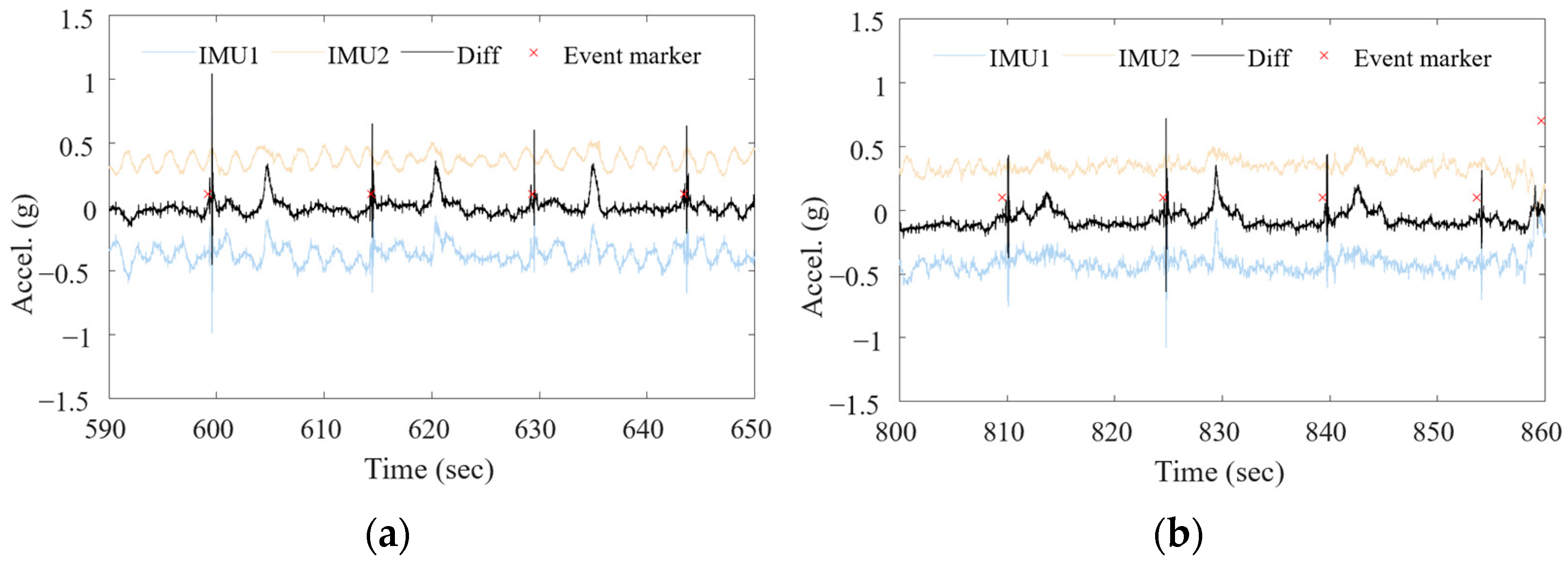
3.1. Differential Signal with Motion Removed
3.2. Experimental Results
4. Conclusions and Discussion
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Matsuo, K.; Palmer, J.B. Anatomy and physiology of feeding and swallowing: Normal and abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707. [Google Scholar] [CrossRef]
- Logemann, J.A. Swallowing disorders. Best Pract. Res. Clin. Gastroenterol. 2007, 21, 563–573. [Google Scholar] [CrossRef]
- Bhattacharyya, N. The prevalence of dysphagia among adults in the United States. Otolaryngol. Head Neck Surg. 2014, 151, 765–769. [Google Scholar] [CrossRef]
- Panebianco, M.; Marchese-Ragona, R.; Masiero, S.; Restivo, D.A. Dysphagia in neurological diseases: A literature review. Neurol. Sci. 2020, 41, 3067–3073. [Google Scholar] [CrossRef] [PubMed]
- Khedr, E.M.; Abbass, M.A.; Soliman, R.K.; Zaki, A.F.; Gamea, A. Post-stroke dysphagia: Frequency, risk factors, and topographic representation: Hospital-based study. Egypt. J. Neurol. Psychiatry Neurosurg. 2021, 57, 1–8. [Google Scholar] [CrossRef]
- Krebbers, I.; Simon, S.R.; Pilz, W.; Kremer, B.; Winkens, B.; Baijens, L.W. Patients with head-and-neck cancer: Dysphagia and affective symptoms. Folia Phoniatr. Et Logop. 2021, 73, 308–315. [Google Scholar] [CrossRef]
- Hsiang, C.-C.; Chen, A.W.-G.; Chen, C.-H.; Chen, M.-K. Early postoperative oral exercise improves swallowing function among patients with oral cavity cancer: A randomized controlled trial. Ear Nose Throat J. 2019, 98, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.J. Neurophysiological basis of swallowing. Dysphagia 1986, 1, 91–100. [Google Scholar] [CrossRef]
- Gallois, Y.; Neveu, F.; Gabas, M.; Cormary, X.; Gaillard, P.; Verin, E.; Speyer, R.; Woisard, V. Can swallowing cerebral neurophysiology be evaluated during ecological food intake conditions? A Systematic Literature Review. J. Clin. Med. 2022, 11, 5480. [Google Scholar] [CrossRef]
- Hao, N.; Sasa, A.; Kulvanich, S.; Nakajima, Y.; Nagoya, K.; Magara, J.; Tsujimura, T.; Inoue, M. Coordination of respiration, swallowing, and chewing in healthy young adults. Front. Physiol. 2021, 12, 696071. [Google Scholar] [CrossRef]
- Curtis, J.A.; Troche, M.S. Effects of verbal cueing on respiratory-swallow patterning, lung volume initiation, and swallow apnea duration in Parkinson’s disease. Dysphagia 2020, 35, 460–470. [Google Scholar] [CrossRef]
- Hopkins-Rossabi, T.; Curtis, P.; Temenak, M.; Miller, C.; Martin-Harris, B. Respiratory phase and lung volume patterns during swallowing in healthy adults: A systematic review and meta-analysis. J. Speech Lang. Hear. Res. 2019, 62, 868–882. [Google Scholar] [CrossRef]
- Hopkins-Rossabi, T.; Rowe, M.; McGrattan, K.; Rossabi, S.; Martin-Harris, B. Respiratory–swallow training methods: Accuracy of automated detection of swallow onset, respiratory phase, lung volume at swallow onset, and real-time performance feedback tested in healthy adults. Am. J. Speech Lang. Pathol. 2020, 29, 1012–1021. [Google Scholar] [CrossRef]
- Krishnan, G.; Goswami, S.P.; Rangarathnam, B. A systematic review of the influence of bolus characteristics on respiratory measures in healthy swallowing. Dysphagia 2020, 35, 883–897. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Pauloski, B.R.; Colangelo, L.; Lazarus, C.; Fujiu, M.; Kahrilas, P.J. Effects of a sour bolus on oropharyngeal swallowing measures in patients with neurogenic dysphagia. J. Speech Lang. Hear. Res. 1995, 38, 556–563. [Google Scholar] [CrossRef]
- Ghannouchi, I.; Speyer, R.; Doma, K.; Cordier, R.; Verin, E. Swallowing function and chronic respiratory diseases: Systematic review. Respir. Med. 2016, 117, 54–64. [Google Scholar] [CrossRef]
- Kang, Y.J.; Arafa, H.M.; Yoo, J.-Y.; Kantarcigil, C.; Kim, J.-T.; Jeong, H.; Yoo, S.; Oh, S.; Kim, J.; Wu, C.; et al. Soft skin-interfaced mechano-acoustic sensors for real-time monitoring and patient feedback on respiratory and swallowing biomechanics. NPJ Digit. Med. 2022, 5, 147. [Google Scholar] [CrossRef] [PubMed]
- Shune, S.E.; Namasivayam-MacDonald, A. Dysphagia-related caregiver burden: Moving beyond the physiological impairment. Perspect. ASHA Spec. Interest Groups 2020, 5, 1282–1289. [Google Scholar] [CrossRef]
- Pizzorni, N. Social and psychologic impact of dysphagia. In Dysphagia: Diagnosis and Treatment; Springer: Berlin/Heidelberg, Germany, 2019; pp. 873–886. [Google Scholar]
- Chun, K.S.; Kang, Y.J.; Lee, J.Y.; Nguyen, M.; Lee, B.; Lee, R.; Jo, H.H.; Allen, E.; Chen, H.; Kim, J.; et al. A skin-conformable wireless sensor to objectively quantify symptoms of pruritus. Sci. Adv. 2021, 7, eabf9405. [Google Scholar] [CrossRef]
- Liu, Y.; Norton, J.J.S.; Qazi, R.; Zou, Z.; Ammann, K.R.; Liu, H.; Yan, L.; Tran, P.L.; Jang, K.-I.; Lee, J.W.; et al. Epidermal mechano-acoustic sensing electronics for cardiovascular diagnostics and human-machine interfaces. Sci. Adv. 2016, 2, e1601185. [Google Scholar] [CrossRef]
- Lee, K.; Ni, X.; Lee, J.Y.; Arafa, H.; Pe, D.J.; Xu, S.; Avila, R.; Irie, M.; Lee, J.H.; Easterlin, R.L.; et al. Mechano-acoustic sensing of physiological processes and body motions via a soft wireless device placed at the suprasternal notch. Nat. Biomed. Eng. 2020, 4, 148–158. [Google Scholar] [CrossRef]
- Jeong, H.; Kwak, S.S.; Sohn, S.; Lee, J.Y.; Lee, Y.J.; O’brien, M.K.; Park, Y.; Avila, R.; Kim, J.-T.; Yoo, J.-Y.; et al. Miniaturized wireless, skin-integrated sensor networks for quantifying full-body movement behaviors and vital signs in infants. Proc. Natl. Acad. Sci. USA 2021, 118, e2104925118. [Google Scholar] [CrossRef]
- Atallah, L.; Lo, B.; King, R.; Yang, G.-Z. Sensor positioning for activity recognition using wearable accelerometers. IEEE Trans. Biomed. Circuits Syst. 2011, 5, 320–329. [Google Scholar] [CrossRef]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, Y.; Coyle, J.L.; Sejdić, E. Non-invasive identification of swallows via deep learning in high resolution cervical auscultation recordings. Sci. Rep. 2020, 10, 8704. [Google Scholar] [CrossRef]
- Chung, H.U.; Rwei, A.Y.; Hourlier-Fargette, A.; Xu, S.; Lee, K.; Dunne, E.C.; Xie, Z.; Liu, C.; Carlini, A.; Rogers, J.A.; et al. Skin-interfaced biosensors for advanced wireless physiological monitoring in neonatal and pediatric intensive-care units. Nat. Med. 2020, 26, 418–429. [Google Scholar] [CrossRef]
- Ni, X.; Ouyang, W.; Jeong, H.; Kim, J.-T.; Tzavelis, A.; Mirzazadeh, A.; Wu, C.; Lee, J.Y.; Keller, M.; Mummidisetty, C.K.; et al. Automated, multiparametric monitoring of respiratory biomarkers and vital signs in clinical and home settings for COVID-19 patients. Proc. Natl. Acad. Sci. USA 2021, 118, e2026610118. [Google Scholar] [CrossRef]
- Jeong, H.; Lee, J.Y.; Lee, K.; Kang, Y.J.; Kim, J.-T.; Avila, R.; Tzavelis, A.; Kim, J.; Ryu, H.; Kwak, S.S.; et al. Differential cardiopulmonary monitoring system for artifact-canceled physiological tracking of athletes, workers, and COVID-19 patients. Sci. Adv. 2021, 7, eabg3092. [Google Scholar] [CrossRef] [PubMed]
- Petropoulos, A.; Sikeridis, D.; Antonakopoulos, T. Wearable smart health advisors: An IMU-enabled posture monitor. IEEE Cons. Elec. Mag. 2020, 9, 20–27. [Google Scholar] [CrossRef]
- Monaco, V.; Giustinoni, C.; Ciapetti, T.; Maselli, A.; Stefanini, C. Assessing Respiratory Activity by Using IMUs: Modeling and Validation. Sensors 2022, 22, 2185. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Number of subjects | 8 |
| Age | 22–68 years |
| Gender ratio (M:F) | 1:1 |
| Avg. trials of swallows | 65 times |
| Type of swallow | 7 |
| Avg. non-swallow duration | 25 min |
| Specific Action | Time Interval between Swallowing (s) | Number of Swallowing |
|---|---|---|
| Swallowing saliva | 30 | 5 |
| Sitting + SW | 15 | 10 |
| Swaying body back and force + SW | 15 | 10 |
| Swaying body from side to side + SW | 15 | 10 |
| Walking + SW | 15 | 10 |
| Cycling + SW | 15 | 10 |
| Running + SW | 15 | 10 |
| Confounding action | - | - |
| Chewing gum 1 | - | - |
| Single | Saliva | Sitting | B and F | S2S | Walking | Cycling | Running |
|---|---|---|---|---|---|---|---|
| Accuracy | 86.4 | 87.1 | 84.4 | 86.7 | 84.8 | 80.4 | 78.2 |
| Precision | 48.9 | 70.6 | 66.7 | 71.3 | 67 | 60.6 | 63.2 |
| Sensitivity | 55 | 86.7 | 79 | 77.5 | 83.8 | 70.4 | 61.4 |
| Specificity | 91.2 | 87.3 | 86.3 | 89.7 | 85.2 | 84 | 85.2 |
| Dual | Saliva | Sitting | B and F | S2S | Walking | Cycling | Running |
|---|---|---|---|---|---|---|---|
| Accuracy | 88 | 98.3 | 88.3 | 87 | 88.4 | 82.3 | 81.2 |
| Precision | 53.8 | 74.3 | 73.9 | 70.0 | 72.3 | 63.8 | 67.6 |
| Sensitivity | 70 | 90.4 | 84 | 81.3 | 91.3 | 74.1 | 68.6 |
| Specificity | 90.8 | 89 | 89.7 | 88.9 | 87.4 | 85.2 | 86.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, Y.J. Biometric Vibration Signal Detection Devices for Swallowing Activity Monitoring. Signals 2024, 5, 516-525. https://doi.org/10.3390/signals5030028
Kang YJ. Biometric Vibration Signal Detection Devices for Swallowing Activity Monitoring. Signals. 2024; 5(3):516-525. https://doi.org/10.3390/signals5030028
Chicago/Turabian StyleKang, Youn J. 2024. "Biometric Vibration Signal Detection Devices for Swallowing Activity Monitoring" Signals 5, no. 3: 516-525. https://doi.org/10.3390/signals5030028
APA StyleKang, Y. J. (2024). Biometric Vibration Signal Detection Devices for Swallowing Activity Monitoring. Signals, 5(3), 516-525. https://doi.org/10.3390/signals5030028