
Impact of Vascular Variations of Superior Mesenteric Artery During Complete Mesocolic Excision for Right Colon Cancer

 , ,
, ,  , , , ,
, , , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
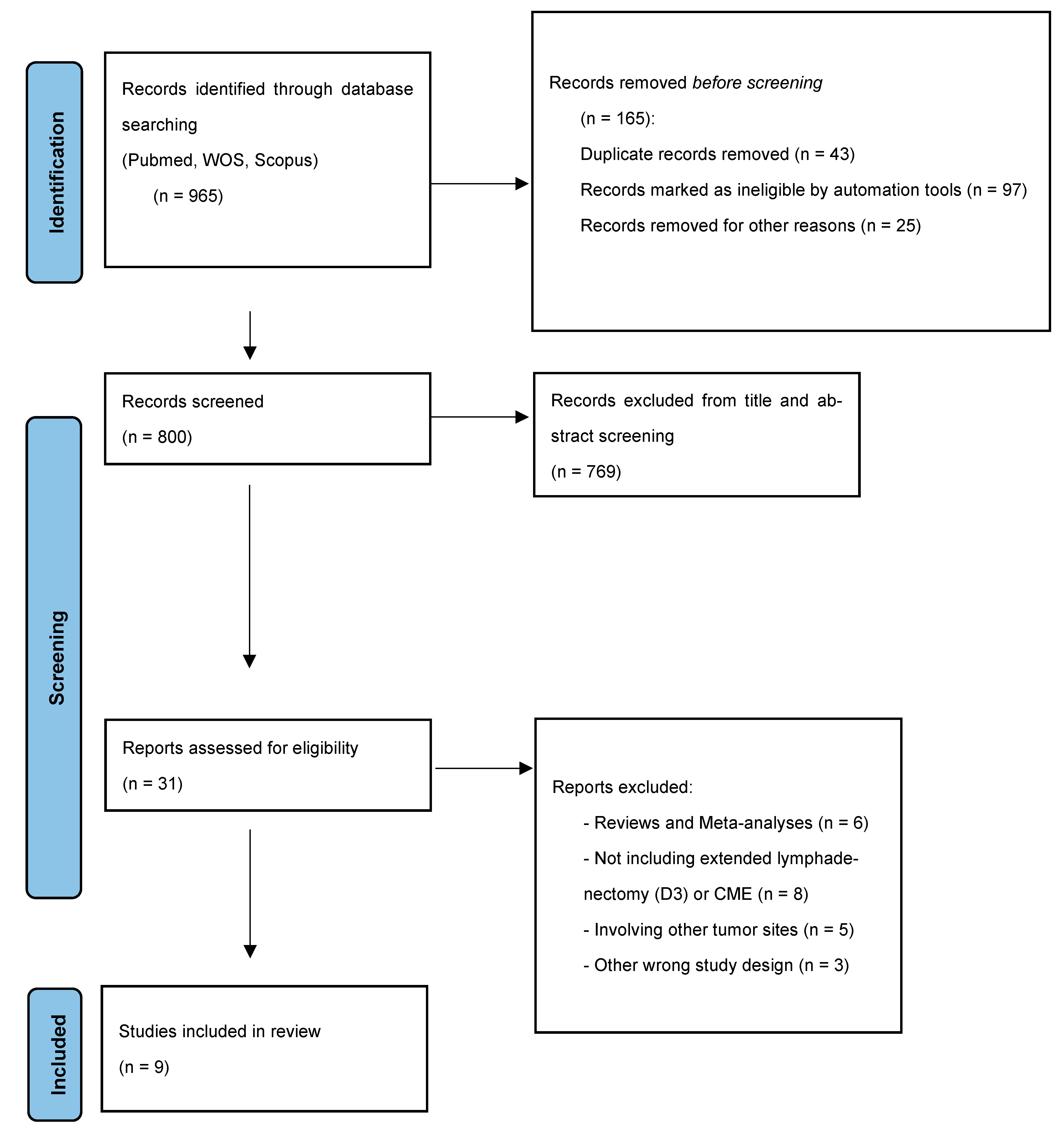
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Statistical Analysis
2.5. Quality Assessment
3. Results
3.1. Baseline Characteristics
3.2. Surgical Characteristics and Vascular Variations
3.3. Outcomes
4. Discussion
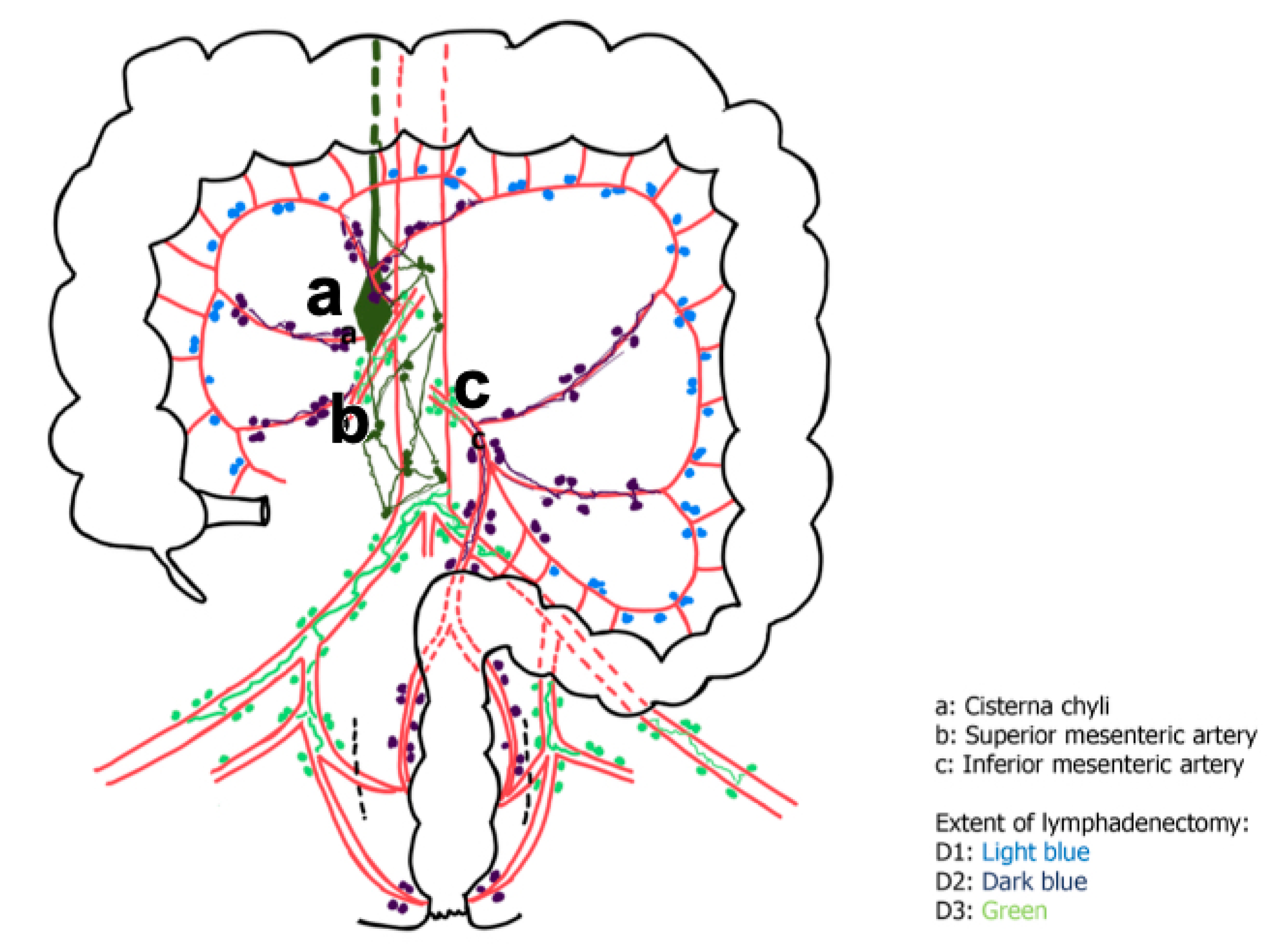
4.1. Anatomical Variability of the Mesenteric Arteries
4.2. Surgical Implications for CME and CVL
4.3. Preoperative Planning and Imaging
4.4. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hohenberger, W.; Weber, K.; Matzel, K.; Papadopoulos, T.; Merkel, S. Standardized surgery for colonic cancer: Complete meso- colic excision and central ligation–technical notes and outcome. Colorectal Dis. 2009, 11, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Muttillo, E.M.; Picardi, B.; Rossi, S.; Muttillo, I.A. Complete mesocolic excision and D3 lymphadenectomy with central vascular ligation in right-sided colon cancer: A systematic review of postoperative outcomes, tumor recurrence and overall survival. Surg. Endosc. 2021, 35, 4945–4955. [Google Scholar] [CrossRef]
- Sica, G.S.; Vinci, D.; Siragusa, L.; Sensi, B.; Guida, A.M.; Bellato, V.; García-Granero, Á.; Pellino, G. Definition and reporting of lymphadenectomy and complete mesocolic excision for radical right colectomy: A systematic review. Surg. Endosc. 2023, 37, 846–861. [Google Scholar] [CrossRef] [PubMed]
- Mazzarella, G.; Muttillo, E.M. Need to define right mesocolectomy and complete mesocolic excision concept: How, when and why? Colorectal Dis. 2021, 23, 3026. [Google Scholar] [CrossRef] [PubMed]
- Anania, G.; Davies, R.J.; Bagolini, F.; Vettoretto, N.; Randolph, J.; Cirocchi, R.; Donini, A. Right hemicolectomy with complete mesocolic excision is safe, leads to an increased lymph node yield and to increased survival: Results of a systematic review and meta-analysis. Tech. Coloproctol. 2021, 25, 1099–1113. [Google Scholar] [CrossRef]
- Tejedor, P.; Francis, N.; Jayne, D.; Hohenberger, W.; Khan, J.; on behalf the CME Project Working Group. Consensus statements on complete mesocolic excision for right-sided colon cancer-technical steps and training implications. Surg. Endosc. 2022, 36, 5595–5601. [Google Scholar] [CrossRef]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese society for cancer of the colon and rectum. Japanese society for cancer of the colon and rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2020, 25, 1–42. [Google Scholar] [CrossRef]
- West, N.P.; Kobayashi, H.; Takahashi, K.; Perrakis, A.; Weber, K.; Hohenberger, W.; Sugihara, K.; Quirke, P. Understanding optimal colonic cancer surgery: Comparison of Japanese D3 resection and European complete mesocolic excision with central vascular ligation. J. Clin. Oncol. 2012, 30, 1763–1769. [Google Scholar] [CrossRef]
- Turnbull, R.B., Jr. Current concepts in cancer. Cancer of the GI tract: Colon, rectum, anus. The no-touch isolation technique of resection. JAMA 1975, 231, 1181–1182. [Google Scholar] [CrossRef]
- Turnbull, R.B., Jr.; Kyle, K.; Watson, F.R.; Spratt, J. Cancer of the colon: The influence of the no-touch isolation technic on survival rates. Ann. Surg. 1967, 166, 420–427. [Google Scholar] [CrossRef]
- Cirocchi, R.; Randolph, J.; Davies, R.J.; Cheruiyot, I.; Gioia, S.; Henry, B.M.; Carlini, L.; Donini, A.; Anania, G. A systematic review and meta-analysis of variants of the branches of the superior mesenteric artery: The Achilles heel of right hemicolectomy with complete mesocolic excision? Colorectal Dis. 2021, 23, 2834–2845. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Prefferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. intern Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Goossen, K.; Tenckhoff, S.; Probst, P.; Grummich, K.; Mihaljevic, A.L.; Büchler, M.W.; Diener, M.K. Optimal literature search for systematic reviews in surgery. Langenbecks Arch. Surg. 2018, 403, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Alakkam, A.; Hill, R.V.; Saggio, G. Superior mesenteric origin of the proper hepatic artery: Embryological and clinical implications. Surg. Radiol. Anat. 2016, 38, 747–750. [Google Scholar] [CrossRef]
- Alsabilah, J.F.; Razvi, S.A.; Albandar, M.H.; Kim, N.K. Intraoperative Archive of Right Colonic Vascular Variability Aids Central Vascular Ligation and Redefines Gastrocolic Trunk of Henle Variants. Dis. Colon. Rectum. 2017, 60, 22–29. [Google Scholar] [CrossRef]
- Andersen, B.T.; Stimec, B.V.; Edwin, B.; Kazaryan, A.M.; Maziarz, P.J.; Ignjatovic, D. Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models: Positioning the middle colic artery bifurcation and its relevance to surgeons operating colon cancer. Surg. Endosc. 2022, 36, 100–108. [Google Scholar] [CrossRef]
- Pérez-Corbal, L.; Trujillo-Diaz, J.C.; Alarcón, I.; Licardie, E.; Senent, A.; Morales-Conde, S. Interactive 3D vascular reconstruction: A navigation tool to improve safety in laparoscopic D3 right colectomy—A video vignette. Colorectal Dis. 2021, 23, 3030–3032. [Google Scholar] [CrossRef]
- Haywood, M.; Molyneux, C.; Mahadevan, V.; Lloyd, J.; Srinivasaiah, N. The right colic artery: An anatomical demonstration and its relevance in the laparoscopic era. Ann. R. Coll. Surg. Engl. 2016, 98, 560–563. [Google Scholar] [CrossRef]
- Lee, S.J.; Park, S.C.; Kim, M.J.; Sohn, D.K.; Oh, J.H. Vascular Anatomy in Laparoscopic Colectomy for Right Colon Cancer. Dis. Colon. Rectum. 2016, 59, 718–724. [Google Scholar] [CrossRef]
- Omotehara, T.; Naito, M.; Hayashi, S.; Kawata, S.; Shimada, K.; Itoh, M. Common hepatic artery originating from superior mesenteric artery with replaced right hepatic artery. Anat. Sci. Int. 2021, 96, 568–571. [Google Scholar] [CrossRef]
- Stimec, B.V.; Andersen, B.T.; Benz, S.R.; Fasel, J.H.D.; Augestad, K.M.; Ignjatovic, D. Retromesenteric course of the middle colic artery-challenges and pitfalls in D3 right colectomy for cancer. Int. J. Colorectal Dis. 2018, 33, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Ye, K.; Wu, Y.; Chen, Q.; Xu, J.; Lin, J.; Kang, W. Variations in right colic vascular anatomy observed during laparoscopic right colectomy. World J. Surg. Oncol. 2019, 17, 16. [Google Scholar] [CrossRef]
- Michels, N.A. Newer anatomy of the liver and its variant blood supply and collateral circulation. Am. J. Surg. 1966, 112, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Yada, H.; Sawai, K.; Taniguchi, H.; Hoshima, M.; Katoh, M.; Takahashi, T. Analysis of vascular anatomy and lymph node metastases warrants radical segmental bowel resection for colon cancer. World J. Surg. 1997, 21, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Anania, G.; Campagnaro, A.; Chiozza, M.; Randolph, J.; Resta, G.; Marino, S.; Pedon, S.; Agrusa, A.; Cuccurullo, D.; Cirocchi, R.; et al. A SICE (Società Italiana di Chirurgia Endoscopica e Nuove Tecnologie) observational prospective multicenter study on anatomical variants of the superior mesenteric artery: Intraoperative analysis during laparoscopic right hemicolectomy-CoDIG 2 database (ColonDx Italian Group). Updates Surg. 2024, 76, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Cinelli, L.; Felli, E.; Muttillo, E.M.; Fiorentini, G.; Diana, M.; Pessaux, P.; Felli, E. Prepancreatic common hepatic artery arising from superior mesenteric artery: An exceptional but important finding during pancreaticoduodenectomy. Surg. Radiol. Anat. 2021, 43, 1413–1420. [Google Scholar] [CrossRef]
- Scarborough, J.E.; Schumacher, J.; Kent, K.C.; Heise, C.P.; Greenberg, C.C. Associations of specific postoperative complications with outcomes after elective colon resection: A procedure-targeted approach toward surgical quality improvement. JAMA Surg. 2017, 152, e164681. [Google Scholar] [CrossRef]
- Chapman, S.J. EuroSurg Collaborative Ileus management international (IMAGINE): Protocol for a multicentre, obser- vational study of ileus after colorectal surgery. Colorectal Dis. 2018, 20, O17–O25. [Google Scholar] [PubMed]
- Ng, Z.Q.; Han, M.; Beh, H.N.; Keelan, S. Chylous ascites in colorectal surgery: A systematic review. World J. Gastrointest. Surg. 2021, 13, 585–596. [Google Scholar] [CrossRef]
- Agustsdottir, E.E.S.; Stimec, B.V.; Stroemmen, T.T.; Sheikh, A.E.; Elaiyarajah, I.; Lindstroem, J.C.; Ignjatovic, D. Preventing chylous ascites after right hemicolectomy with D3 extended mesenterectomy. Langenbecks Arch. Surg. 2020, 405, 1017–1024. [Google Scholar] [CrossRef]
- Al-Busafi, S.A.; Ghali, P.; Deschênes, M.; Wong, P. Chylous Ascites: Evaluation and Management. ISRN Hepatol. 2014, 2014, 240473. [Google Scholar] [CrossRef] [PubMed]
- Cheng, D.; Zhang, Y.; Han, B.; Sun, P.; Wang, J.; Lin, Q.; Xu, M. Real-time indocyanine green lymphangiography in radical resection of right colon cancer allows the identification of chyle leakage. Contemp Oncol. 2021, 25, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Luzon, J.A.; Andersen, B.T.; Stimec, B.V.; Fasel, J.H.D.; Bakka, A.O.; Kazaryan, A.M.; Ignjatovic, D. Implementation of 3D printed superior mesenteric vascular models for surgical planning and/or navigation in right colectomy with extended D3 mesenterectomy: Comparison of virtual and physical models to the anatomy found at surgery. Surg. Endosc. 2019, 33, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Nesgaard, J.M.; Stimec, B.V.; Bakka, A.O.; Edwin, B.; Ignjatovic, D. Navigating the mesentery: A comparative pre- and perioperative visualization of the vascular anatomy. Colorectal Dis. 2015, 17, 810–819. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Selection | Comparability | Outcome | |||||
|---|---|---|---|---|---|---|---|
| Study | Representativeness of Exposed Cohort | Selection of Non-Exposed Cohort | Ascertain-ment of Exposure | Demonstration that Outcome of Interest Was Not Present at Start of Study | Comparability of Cohorts Based on the Design or Analysis | Assessment of Outcome | Adequacy of Follow-Up of Cohorts |
| Alakkam et al. [14], Surg Radiol Anat, 2015 |  | | | | | ||
| Alsabilah et al. [15], Dis Colon Rectum, 2017 | | | | | | ||
| Andersen et al. [16], Surg Endosc, 2021 | | | | | | ||
| Pérez-Corbal et al. [17], Colorectal Dis, 2021 | | | | | | ||
| Haywood et al. [18], Ann R Coll Surg Engl, 2016 | | | | | | ||
| Lee et al. [19], Dis Colon Rectum, 2016 | | | | | | ||
| Omotehara et al. [20], Anat Sci Int, 2021 | | | | | | ||
| Stimec et al. [21], Int J Colorectal Dis, 2018 | | | | | | ||
| Wu et al. [22], World J Surg Oncol, 2019 | | | | | | ||
counts as 1 point.| Author | Country | Type of Study | No. of Patients | Age | Gender M/F | BMI |
|---|---|---|---|---|---|---|
| Alakkam et al. [14], Surg Radiol Anat, 2015 | USA | Cadaver | 1 | 84 | 100/0 | NS |
| Alsabilah et al. [15], Dis Colon Rectum, 2017 | Korea | Intraoperative | 70 | 62.7 | 47.2/52.8 | 23.6 |
| Andersen et al. [16], Surg Endosc, 2021 | Norway | Radiology | 32 | 67.4 | 40.6/59.4 | NS |
| Pérez-Corbal et al. [17], Colorectal Dis, 2021 | Spain | Intraoperative | 1 | 79 | 0/100 | NS |
| Haywood et al. [18], Ann R Coll Surg Engl, 2016 | UK | Cadaver | 25 | NS | 56/44 | NS |
| Lee et al. [19], Dis Colon Rectum, 2016 | Korea | Intraoperative | 116 | 66.2 | 48.3/51.7 | 23.5 |
| Omotehara et al. [20], Anat Sci Int, 2021 | Japan | Cadaver | 1 | 80 | 100/0 | NS |
| Stimec et al. [21], Int J Colorectal Dis, 2018 | Switzerland | Radiology | 507 | NS | NS | NS |
| Wu et al. [22], World J Surg Oncol, 2019 | China | Intraoperative | 60 | 58.5 | 55/45 | 21.8 |
| Total (n = 9) | 813 pts | |||||
| Author | Type of Resection | Technique O/L/R | SMA Variations | ICA | RCA | MCA |
|---|---|---|---|---|---|---|
| Alakkam et al. [14], Surg Radiol Anat, 2015 | RH with CME/D3 lymphadenectomy | NS | 1 replaced PHA from SMA | NS | NS | NS |
| Alsabilah et al. [15], Dis Colon Rectum, 2017 | RH with CME/D3 lymphadenectomy | 29/71/0 | NS | 100 | 41.4 | 100 |
| Andersen et al. [16], Surg Endosc, 2021 | RH with CME/D3 lymphadenectomy | NS | 1 replaced MCA from IMA; 10 aMCA from the left-hand side of SMA | NS | NS | 100 |
| Pérez-Corbal et al. [17], Colorectal Dis, 2021 | RH with CME/D3 lymphadenectomy | 0/100/0 | Common trunk of the ICA and the RCA | 100 | 100 | 100 |
| Haywood et al. [18], Ann R Coll Surg Engl, 2016 | RH with CME/D3 lymphadenectomy | NS | 9 RCA replaced from right branch of MCA; 8 RCA replaced from SMA; 3 RCA replaced from ICA; 3 RCA replaced from the root of MCA | 100 | 92 | 100 |
| Lee et al. [19], Dis Colon Rectum, 2016 | RH with CME/D3 lymphadenectomy | 0/100/0 | ICA passed the SMV anteriorly or posteriorly (n = 58); RCA originated from the SMA (n = 38); RCA crossed the SMV anteriorly (n = 33) and posteriorly (n = 5) | 100 | NS | NS |
| Omotehara et al. [20], Anat Sci Int, 2021 | RH with CME/D3 lymphadenectomy | NS | CHA originated as the first branch of the SMA behind the SMV and the pancreas | NS | NS | NS |
| Stimec et al. [21], Int J Colorectal Dis, 2018 | RH with CME/D3 lymphadenectomy | NS | 4 retromesenteric MCA | NS | NS | NS |
| Wu et al. [22], World J Surg Oncol, 2019 | RH with CME/D3 lymphadenectomy | 0/100/0 | SMA was left (n = 57) and right (n = 3) of the SMV | 97.6 | 55 | 100 |
| Total (n = 9) |
| Author | Type of Study | Intraoperative Complications % | Conversion % | Postoperative Bleeding % |
|---|---|---|---|---|
| Alsabilah et al. [15], Dis Colon Rectum, 2017 | Intraoperative | 0 | NS | NS |
| Andersen et al. [16], Surg Endosc, 2021 | Radiology | NS | NS | NS |
| Pérez-Corbal et al. [17], Colorectal Dis, 2021 | Intraoperative | 0 | 0 | 0 |
| Lee et al. [19], Dis Colon Rectum, 2016 | Intraoperative | 0 | 0 | 2.6 |
| Stimec et al. [21], Int J Colorectal Dis, 2018 | Radiology | NS | NS | NS |
| Wu et al. [22], World J Surg Oncol, 2019 | Intraoperative | 0 | 0 | 16.7 |
| Anatomical Variation | Frequency | Surgical Implication | Clinical Gap | Recommendation |
|---|---|---|---|---|
| Replaced Proper Hepatic Artery (PHA) from SMA | Rare (≈1%) | Risk of hepatic ischemia if unrecognized and ligated | Often missed on standard preoperative imaging | Use of contrast-enhanced CT or 3D angiography preoperatively |
| Accessory/Double Middle Colic Artery (MCA) | Occasional (up to 19%) | Difficulty in achieving radical lymphadenectomy at the colonic flexure | Inconsistent classification, poor intra-op identification | Review pre-op 3D reconstructions; intra-op exploration recommended |
| Replaced MCA from IMA | Rare | Risk of non-oncological resection margins | Not routinely evaluated | Consider an anatomical variant in atypical SMA branching pattern |
| MCA bifurcation anterior/posterior to SMV | Frequent variation | Technical risk in vessel ligation and dissection | No standardized description of the bifurcation site | Careful intra-op identification; anticipate variants with 3D planning |
| RCA replaced from ICA, MCA, or absent | Common (RCA absent in ~28%) | Confusion during dissection; possible vascular injury | Poor pre-op detectability | Gentle dissection along SMV; avoid mass ligation |
| ICA passing anterior/posterior to SMV | ≈50/50 distribution | Risk of SMV injury during ICA dissection | Often not reported in imaging | Explore both anterior and posterior paths intraoperatively |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazzarella, G.; Coletta, D.; Muttillo, E.M.; Picardi, B.; Rossi, S.; Scorsi, A.; Meneghini, S.; Cirillo, B.; Brachini, G.; Assenza, M.; et al. Impact of Vascular Variations of Superior Mesenteric Artery During Complete Mesocolic Excision for Right Colon Cancer. Gastrointest. Disord. 2025, 7, 40. https://doi.org/10.3390/gidisord7020040
Mazzarella G, Coletta D, Muttillo EM, Picardi B, Rossi S, Scorsi A, Meneghini S, Cirillo B, Brachini G, Assenza M, et al. Impact of Vascular Variations of Superior Mesenteric Artery During Complete Mesocolic Excision for Right Colon Cancer. Gastrointestinal Disorders. 2025; 7(2):40. https://doi.org/10.3390/gidisord7020040
Chicago/Turabian StyleMazzarella, Gennaro, Diego Coletta, Edoardo Maria Muttillo, Biagio Picardi, Stefano Rossi, Alessandro Scorsi, Simona Meneghini, Bruno Cirillo, Gioia Brachini, Marco Assenza, and et al. 2025. "Impact of Vascular Variations of Superior Mesenteric Artery During Complete Mesocolic Excision for Right Colon Cancer" Gastrointestinal Disorders 7, no. 2: 40. https://doi.org/10.3390/gidisord7020040
APA StyleMazzarella, G., Coletta, D., Muttillo, E. M., Picardi, B., Rossi, S., Scorsi, A., Meneghini, S., Cirillo, B., Brachini, G., Assenza, M., Mingoli, A., & Muttillo, I. A. (2025). Impact of Vascular Variations of Superior Mesenteric Artery During Complete Mesocolic Excision for Right Colon Cancer. Gastrointestinal Disorders, 7(2), 40. https://doi.org/10.3390/gidisord7020040