
Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases



Abstract
:1. Introduction
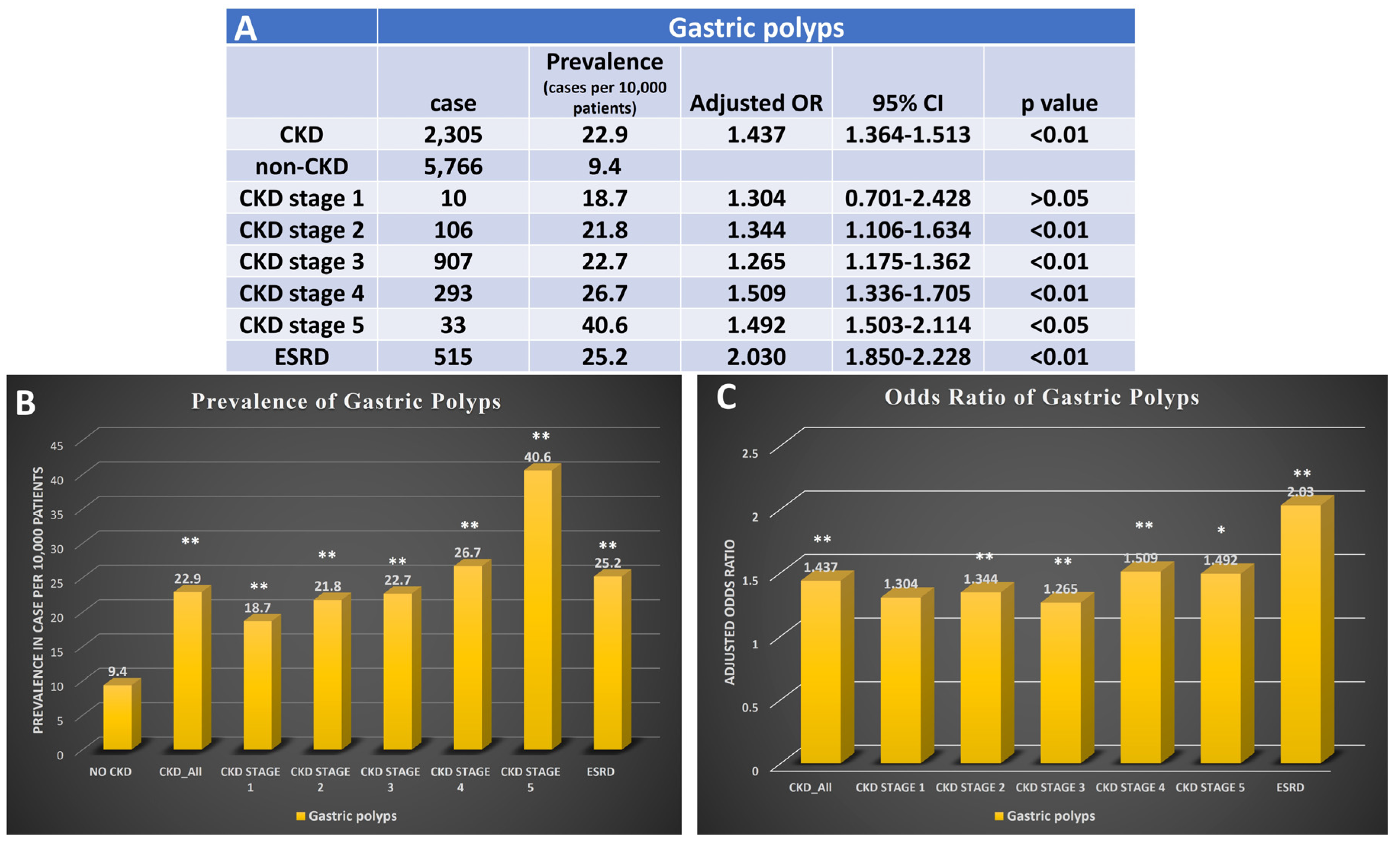
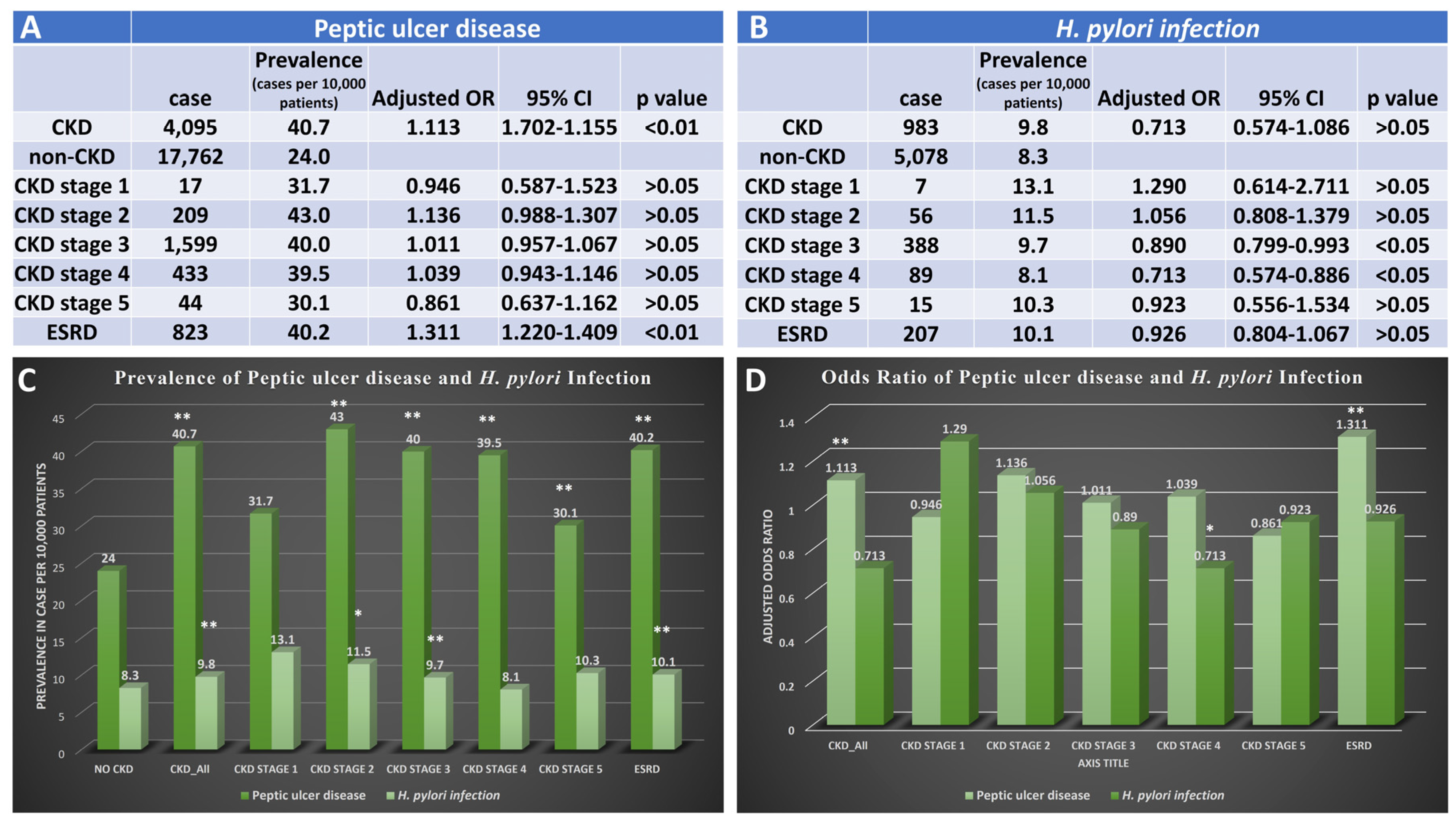
2. Results
3. Discussion
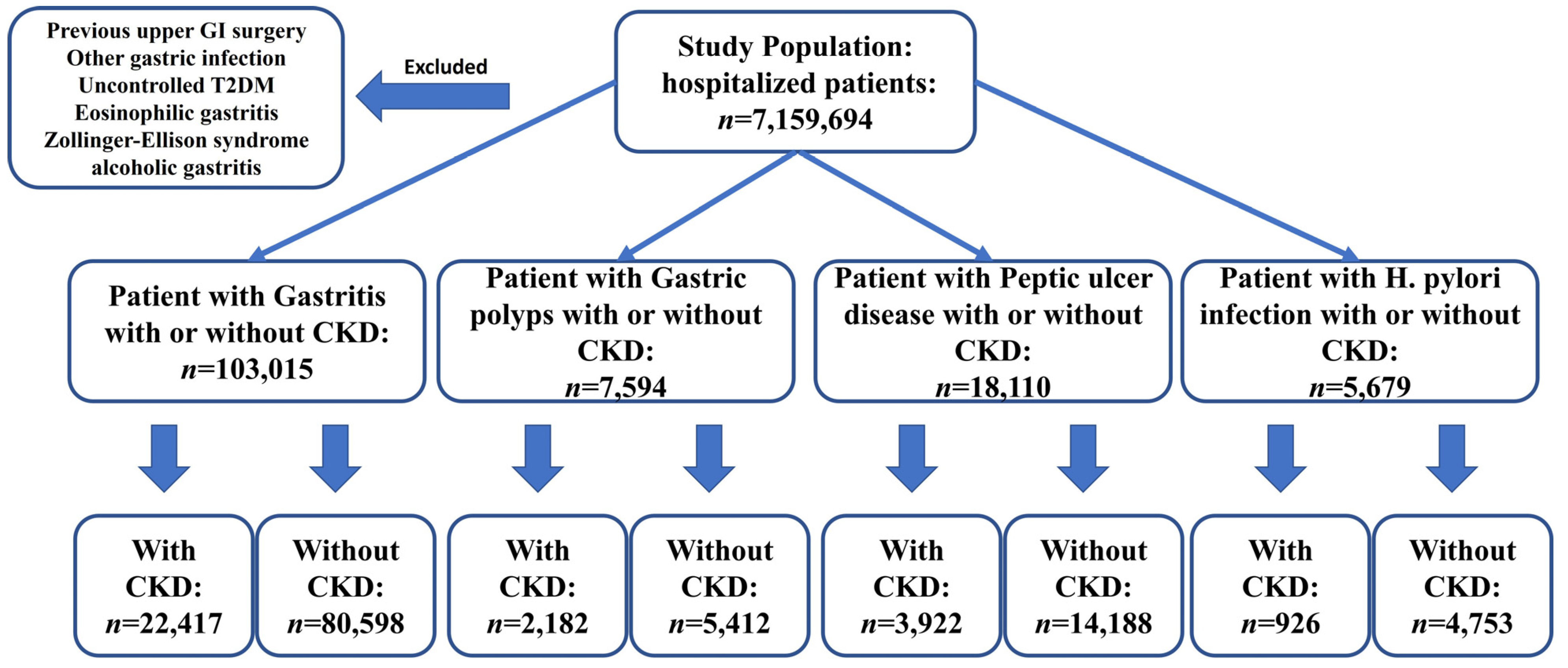
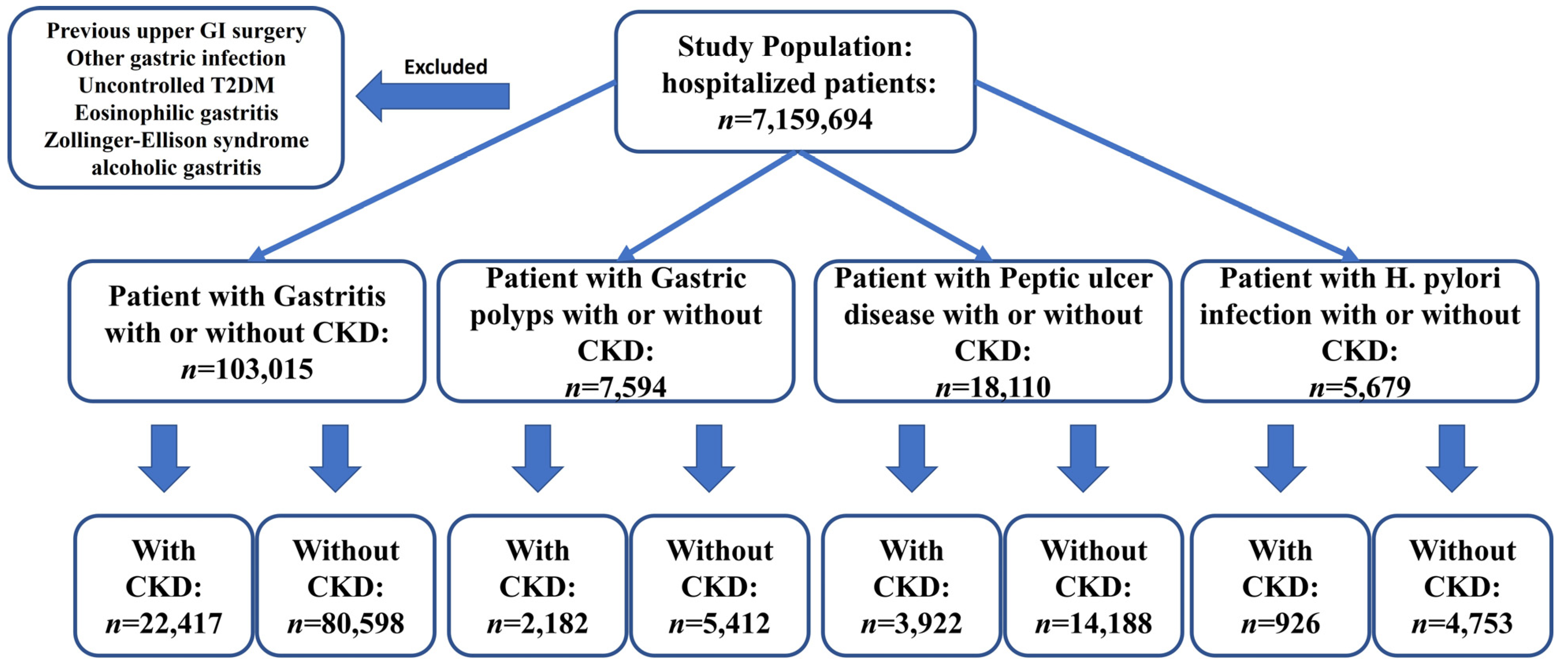
4. Materials and Methods
4.1. Database
4.2. Data Collection and Outcomes
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Vart, P.; Powe, N.R.; McCulloch, C.E.; Saran, R.; Gillespie, B.W.; Saydah, S.; Crews, D.C. National Trends in the Prevalence of Chronic Kidney Disease Among Racial/Ethnic and Socioeconomic Status Groups, 1988-2016. JAMA Netw. Open 2020, 3, e207932. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.K.; Knicely, D.H.; Grams, M.E. Chronic Kidney Disease Diagnosis and Management: A Review. JAMA 2019, 322, 1294–1304. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, P.; Remuzzi, G.; Glassock, R.; Levin, A.; Jager, K.J.; Tonelli, M.; Massy, Z.; Wanner, C.; Anders, H.-J. Chronic kidney disease. Nat. Rev. Dis. Primers 2017, 3, 17088. [Google Scholar] [CrossRef]
- Wang, X.; Shapiro, J.I. Evolving concepts in the pathogenesis of uraemic cardiomyopathy. Nat. Rev. Nephrol. 2019, 15, 159–175. [Google Scholar] [CrossRef]
- Bello, A.K.; Alrukhaimi, M.; Ashuntantang, G.E.; Basnet, S.; Rotter, R.C.; Douthat, W.G.; Kazancioglu, R.; Köttgen, A.; Nangaku, M.; Powe, N.R.; et al. Complications of chronic kidney disease: Current state, knowledge gaps, and strategy for action. Kidney Int. Suppl. 2017, 7, 122–129. [Google Scholar] [CrossRef]
- Zoccali, C.; Vanholder, R.; Massy, Z.A.; Ortiz, A.; Sarafidis, P.; Dekker, F.W.; Fliser, D.; Fouque, D.; Heine, G.H.; Jager, K.J.; et al. The systemic nature of CKD. Nat. Rev. Nephrol. 2017, 13, 344–358. [Google Scholar] [CrossRef]
- Karahan, D.; Şahin, İ. Comparison of gastrointestinal symptoms and findings in renal replacement therapy modalities. BMC Nephrol. 2022, 23, 261. [Google Scholar] [CrossRef]
- Cano, A.E.; Neil, A.K.; Kang, J.Y.; Barnabas, A.; Eastwood, J.B.; Nelson, S.R.; Hartley, I.; Maxwell, D. Gastrointestinal symptoms in patients with end-stage renal disease undergoing treatment by hemodialysis or peritoneal dialysis. Am. J. Gastroenterol. 2007, 102, 1990–1997. [Google Scholar] [CrossRef]
- Lew, S.Q.; Radhakrishnan, J. Chapter 33—Chronic Kidney Disease and Gastrointestinal Disorders. In Chronic Renal Disease, 2nd ed.; Kimmel, P.L., Rosenberg, M.E., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 521–539. [Google Scholar]
- Grant, C.J.; Harrison, L.E.; Hoad, C.L.; Marciani, L.; Gowland, P.A.; McIntyre, C.W. Patients with chronic kidney disease have abnormal upper gastro-intestinal tract digestive function: A study of uremic enteropathy. J. Gastroenterol. Hepatol. 2017, 32, 372–377. [Google Scholar] [CrossRef]
- Shah, V.; Lyford, G.; Gores, G.; Farrugia, G. Nitric oxide in gastrointestinal health and disease. Gastroenterology 2004, 126, 903–913. [Google Scholar] [CrossRef] [PubMed]
- Neumann, W.L.; Coss, E.; Rugge, M.; Genta, R.M. Autoimmune atrophic gastritis—Pathogenesis, pathology and management. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 529–541. [Google Scholar] [CrossRef]
- Shah, S.C.; Piazuelo, M.B.; Kuipers, E.J.; Li, D. AGA Clinical Practice Update on the Diagnosis and Management of Atrophic Gastritis: Expert Review. Gastroenterology 2021, 161, 1325–1332.e1327. [Google Scholar] [CrossRef] [PubMed]
- Waldum, H.; Fossmark, R. Gastritis, Gastric Polyps and Gastric Cancer. Int. J. Mol. Sci. 2021, 22, 6548. [Google Scholar] [CrossRef] [PubMed]
- Margolis, D.M.; Saylor, J.L.; Geisse, G.; DeSchryver-Kecskemeti, K.; Harter, H.R.; Zuckerman, G.R. Upper gastrointestinal disease in chronic renal failure. A prospective evaluation. Arch. Intern. Med. 1978, 138, 1214–1217. [Google Scholar] [CrossRef]
- Thomas, R.; Panackal, C.; John, M.; Joshi, H.; Mathai, S.; Kattickaran, J.; Iqbal, M. Gastrointestinal Complications in Patients with Chronic Kidney Disease—A 5-Year Retrospective Study from a Tertiary Referral Center. Ren. Fail. 2013, 35, 49–55. [Google Scholar] [CrossRef]
- Kővári, B.; Kim, B.H.; Lauwers, G.Y. The pathology of gastric and duodenal polyps: Current concepts. Histopathology 2021, 78, 106–124. [Google Scholar] [CrossRef]
- Markowski, A.R.; Markowska, A.; Guzinska-Ustymowicz, K. Pathophysiological and clinical aspects of gastric hyperplastic polyps. World J. Gastroenterol. 2016, 22, 8883–8891. [Google Scholar] [CrossRef]
- García Agudo, R.; Aoufi Rabih, S.; González Carro, P.; Pérez Roldán, F.; Proy Vega, B.; Arias Arias, Á.; Cazalla Cadenas, F.; Tenías Burillo, J.M.; Fernández Rodríguez, A. Gastrointestinal lesions in chronic kidney disease patients with anemia. Nefrol. (Engl. Ed.) 2019, 39, 50–57. [Google Scholar] [CrossRef]
- Kavitt, R.T.; Lipowska, A.M.; Anyane-Yeboa, A.; Gralnek, I.M. Diagnosis and Treatment of Peptic Ulcer Disease. Am. J. Med. 2019, 132, 447–456. [Google Scholar] [CrossRef]
- Abbasi-Kangevari, M.; Ahmadi, N.; Fattahi, N.; Rezaei, N.; Malekpour, M.R.; Ghamari, S.H.; Moghaddam, S.S.; Azadnajafabad, S.; Esfahani, Z.; Kolahi, A.A.; et al. Quality of care of peptic ulcer disease worldwide: A systematic analysis for the global burden of disease study 1990–2019. PLoS ONE 2022, 17, e0271284. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, M.; Reddy, K.M.; Marsicano, E. Peptic Ulcer Disease and Helicobacter pylori infection. Mo. Med. 2018, 115, 219–224. [Google Scholar]
- Lanas, A.; Chan, F.K.L. Peptic ulcer disease. Lancet 2017, 390, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.-M.; Hsu, C.-N.; Tai, W.-C.; Yang, S.-C.; Wu, C.-K.; Shih, C.-W.; Ku, M.-K.; Yuan, L.-T.; Wang, J.-W.; Tseng, K.-L.; et al. Risk factors influencing the outcome of peptic ulcer bleeding in chronic kidney disease after initial endoscopic hemostasis: A nationwide cohort study. Medicine 2016, 95, e4795. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.C.; Muo, C.H.; Wang, I.K.; Chang, C.T.; Chou, C.Y.; Liu, J.H.; Yen, T.H.; Huang, C.C.; Chung, C.J. Peptic ulcer disease risk in chronic kidney disease: Ten-year incidence, ulcer location, and ulcerogenic effect of medications. PLoS ONE 2014, 9, e87952. [Google Scholar] [CrossRef] [PubMed]
- Tseng, G.Y.; Lin, H.J.; Fang, C.T.; Yang, H.B.; Tseng, G.C.; Wang, P.C.; Hung, T.L.; Deng, Y.C.; Cheng, Y.T.; Huang, C.H. Recurrence of peptic ulcer in uraemic and non-uraemic patients after Helicobacter pylori eradication: A 2-year study. Aliment. Pharmacol. Ther. 2007, 26, 925–933. [Google Scholar] [CrossRef]
- Suzuki, H.; Mori, H. Helicobacter pylori gastritis—A novel distinct disease entity. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 556–557. [Google Scholar] [CrossRef]
- Quintero, E.; Kaunitz, J.; Nishizaki, Y.; De Giorgio, R.; Sternini, C.; Guth, P.H. Uremia increases gastric mucosal permeability and acid back-diffusion injury in the rat. Gastroenterology 1992, 103, 1762–1768. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Yuan, J.; Nazertehrani, S.; Ni, Z.; Liu, S. Chronic kidney disease causes disruption of gastric and small intestinal epithelial tight junction. Am. J. Nephrol. 2013, 38, 99–103. [Google Scholar] [CrossRef]
- Forssell, H. Gastric mucosal defence mechanisms: A brief review. Scand. J. Gastroenterol. 1988, 155, 23–28. [Google Scholar] [CrossRef]
- Falconi, C.A.; Junho, C.V.d.C.; Fogaça-Ruiz, F.; Vernier, I.C.S.; da Cunha, R.S.; Stinghen, A.E.M.; Carneiro-Ramos, M.S. Uremic Toxins: An Alarming Danger Concerning the Cardiovascular System. Front. Physiol. 2021, 12, 686249. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, R.H.; Laing, D.R. Changes of the digestive tract in uremia: A pathologic anatomic study. Arch. Intern. Med. 1934, 53, 851–864. [Google Scholar] [CrossRef]
- Paimela, H.; Tallgren, L.G.; Stenman, S.; von Numers, H.; Scheinin, T.M. Multiple duodenal polyps in uraemia: A little known clinical entity. Gut 1984, 25, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Beno, I.; Volkovová, K.; Bátovsky, M.; Staruchová, M. Increased mucosal antioxidant enzyme activities in chronic gastritis and benign gastric polyps. Eur. J. Cancer Prev. 1993, 2, 461–465. [Google Scholar] [CrossRef]
- Huang, T.; Zhou, F.; Yuan, X.; Yang, T.; Liang, X.; Wang, Y.; Tu, H.; Chang, J.; Nan, K.; Wei, Y. Reactive Oxygen Species Are Involved in the Development of Gastric Cancer and Gastric Cancer-Related Depression through ABL1-Mediated Inflammation Signaling Pathway. Oxidative Med. Cell. Longev. 2019, 2019, 5813985. [Google Scholar] [CrossRef]
- Kim, M.; Kim, C.S.; Bae, E.H.; Ma, S.K.; Kim, S.W. Risk factors for peptic ulcer disease in patients with end-stage renal disease receiving dialysis. Kidney Res. Clin. Pract. 2019, 38, 81–89. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Gastritis w CKD | Gastritis w/o CKD | p Value | Gastric Polyps w CKD | Gastric Polyps w/o CKD | p Value | |
|---|---|---|---|---|---|---|---|
| Age | 69.2 ± 0.1 | 58.9 ± 0.1 | <0.01 | 72.1 ± 0.3 | 66.9 ± 0.2 | <0.01 | |
| Sex | Female | 11,164 (49.8%) | 45,181 (56.1%) | <0.01 | 1048 (48.0%) | 3215 (58.4%) | <0.01 |
| Male | 11,253 (50.2%) | 35,417 (43.9%) | <0.01 | 1134 (52.0%) | 2287 (41.6%) | <0.01 | |
| Race | White | 12,022 (53.6%) | 48,983 (60.8%) | <0.01 | 1357 (62.2%) | 3916 (71.2%) | <0.01 |
| Black | 5602 (25.0%) | 13,016 (16.1%) | <0.01 | 476 (21.8%) | 634 (11.5%) | <0.01 | |
| Hispanic | 2811 (12.5%) | 11,151 (13.8%) | <0.01 | 187 (8.6%) | 504 (9.2%) | <0.01 | |
| Asian | 729 (3.3%) | 2125 (2.6%) | <0.01 | 57 (2.6%) | 134 (2.4%) | <0.01 | |
| Risk Factors | T2DM | 812 (3.6%) | 11,192 (13.9%) | <0.01 | 77 (3.5%) | 988 (18.0%) | <0.01 |
| Smoking | 2543 (11.3%) | 16,021 (19.9%) | <0.01 | 131 (6.0%) | 455 (8.3%) | <0.05 | |
| Obesity | 3584 (16.0%) | 11,525 (14.3%) | <0.01 | 417 (19.1%) | 997 (18.1%) | <0.05 | |
| Comorbidity | HTN | 12,244 (54.6%) | 39,239 (48.7%) | <0.01 | 1169 (53.6%) | 3039 (55.2%) | <0.05 |
| HLD | 10,252 (45.7%) | 23,370 (29.0%) | <0.01 | 1037 (47.5%) | 2086 (37.9%) | <0.05 | |
| Variable | PUD w CKD | PUD w/o CKD | p Value | H. pylori w CKD | H. pylori w/o CKD | p Value | |
|---|---|---|---|---|---|---|---|
| Age | 71.5 ± 0.2 | 62.7 ± 0.1 | <0.01 | 67.8 ± 0.5 | 56.2 ± 0.3 | <0.01 | |
| Sex | Female | 1968 (50.2%) | 7965 (56.1%) | <0.01 | 411 (44.4%) | 2238 (47.1%) | <0.01 |
| Male | 1954 (49.8%) | 6223 (43.9%) | <0.01 | 515 (55.6%) | 2515 (52.9%) | <0.01 | |
| Race | White | 2321 (59.2%) | 9744 (68.7%) | <0.01 | 363 (39.2%) | 1916 (40.3%) | <0.01 |
| Black | 824 (21.0%) | 1926 (13.6%) | <0.01 | 321 (34.7%) | 1236 (26.0%) | <0.01 | |
| Hispanic | 403 (10.3%) | 1298 (9.1%) | <0.01 | 136 (14.7%) | 887 (18.7%) | <0.01 | |
| Asian | 127 (3.2%) | 310 (2.2%) | <0.01 | 40 (4.3%) | 253 (5.3%) | <0.01 | |
| Risk Factors | T2DM | 190 (4.8%) | 1987 (14.0%) | <0.01 | 25 (2.7%) | 658 (13.8%) | <0.01 |
| Smoking | 449 (11.4%) | 3124 (22.0%) | <0.01 | 133 (14.4%) | 1052 (22.1%) | <0.01 | |
| Obesity | 641 (16.3%) | 2059 (14.5%) | <0.05 | 142 (15.3%) | 628 (13.2%) | <0.01 | |
| Comorbidity | HTN | 2106 (53.7%) | 7403 (52.2%) | <0.05 | 530 (57.2%) | 2036 (42.8%) | <0.01 |
| HLD | 1888 (48.1%) | 4757 (33.5%) | <0.01 | 410 (44.3%) | 1158 (24.4%) | <0.01 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Wright, Z.; Wang, J.; Frandah, W.M.; Song, G. Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases. Gastrointest. Disord. 2023, 5, 329-339. https://doi.org/10.3390/gidisord5030027
Wang X, Wright Z, Wang J, Frandah WM, Song G. Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases. Gastrointestinal Disorders. 2023; 5(3):329-339. https://doi.org/10.3390/gidisord5030027
Chicago/Turabian StyleWang, Xiaoliang, Zachary Wright, Jiayan Wang, Wesam M. Frandah, and Gengqing Song. 2023. "Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases" Gastrointestinal Disorders 5, no. 3: 329-339. https://doi.org/10.3390/gidisord5030027
APA StyleWang, X., Wright, Z., Wang, J., Frandah, W. M., & Song, G. (2023). Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases. Gastrointestinal Disorders, 5(3), 329-339. https://doi.org/10.3390/gidisord5030027