Reno-colic fistula is very rare, representing 5.1% of uro-digestive fistulas[1]. Causes can include infection, stone disease, malignancy, or trauma to the kidney or the colon. Pyelo-colic fistulas are in most cases of renal origin (lithiasis)[2]. Traumatic causes are other major groups reported mainly related to renal interventional techniques (cryoablation, radiofrequency, percutaneous nephrolithotomy). Infectious causes are rarer (tuberculosis, refractory infection of renal cysts)[3,4].
The general, digestive, or urinary clinical manifestations are often variable and non-specific, making the diagnosis difficult[5]. The research of fecaluria and/or pneumaturia helps to direct toward the diagnosis of uro-digestive fistula.
Abdominal-pelvic CT scan with contrast, upper and lower digestive radiography, or ureteropyelography retrograde and/or percutaneous descending pyelography often confirms the diagnosis by showing the passage of urinary contrast medium to the digestive tract or vice versa, thus providing information on the cause, nature, and location of the uro-digestive fistula.
The choice of conservative or radical treatment essentially depends on the etiology and renal clearance. The radical treatment is nephrectomy with the closure of the privileged digestive fistula if the kidney is destroyed or a tumor etiology makes radical treatment unavoidable. Conservative treatment, if the fistula is post-traumatic with functional kidney, includes urinary drainage, antibiotic therapy, and rest of the digestive tract.xs
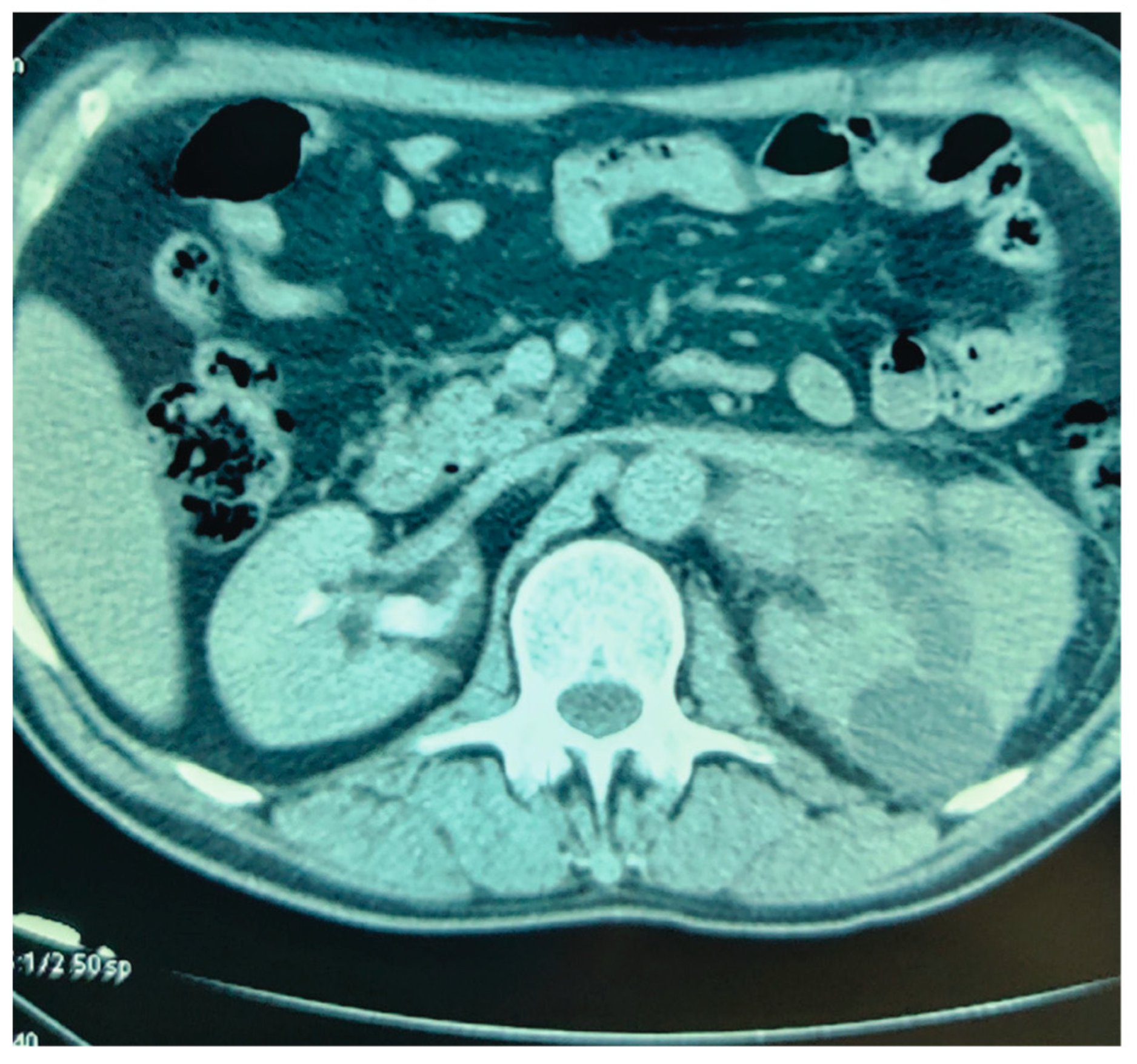
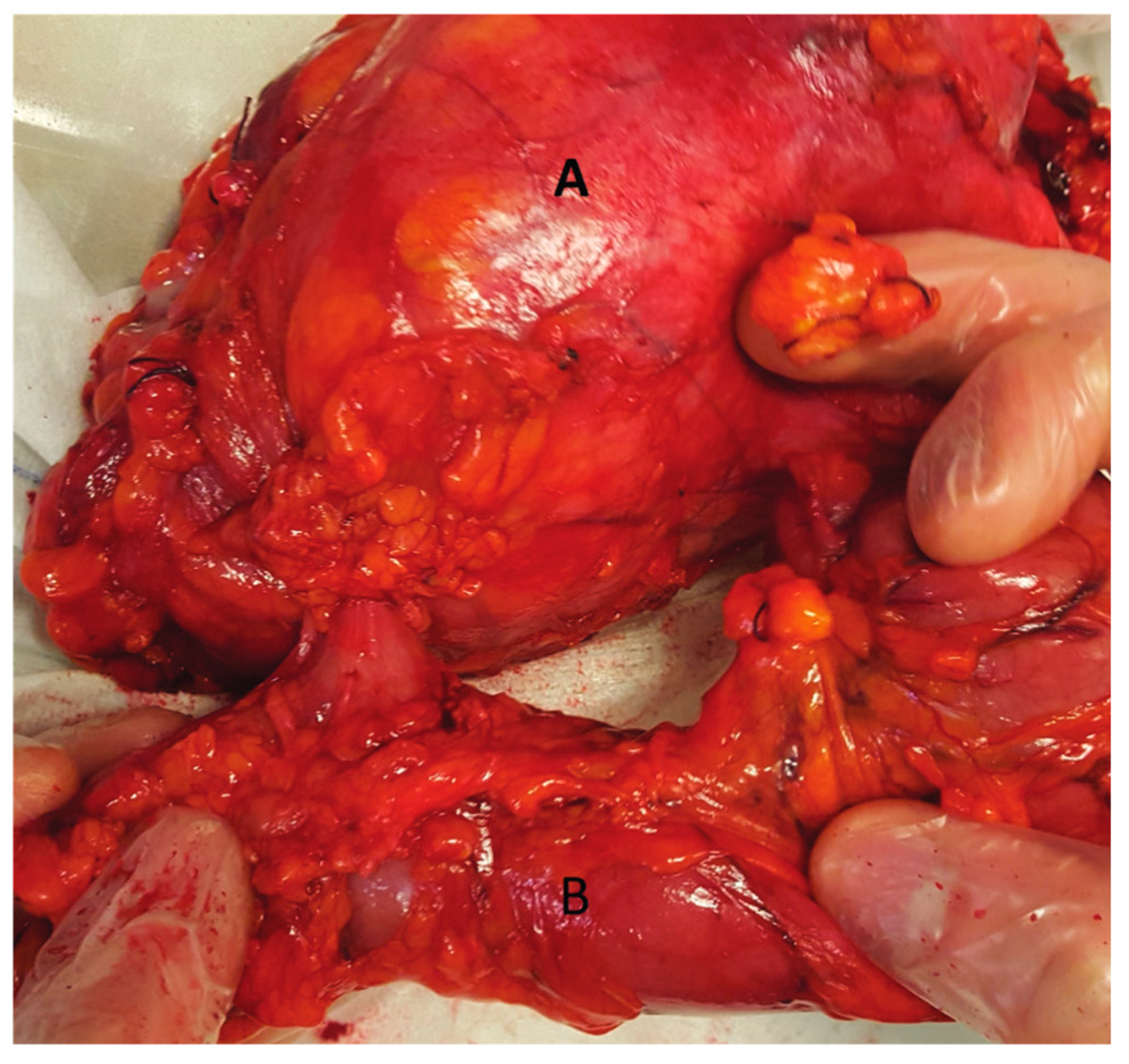
Our 65-year-old patient reported repeated renal colic, with air emission during urination, and presented with a pyelo-colic fistula (Figure 1 and Figure 2). Radical treatment was carried out. The anatomo-pathological analysis showed a chronic pyelonephretic kidney abscessed. with a destroyed kidney.
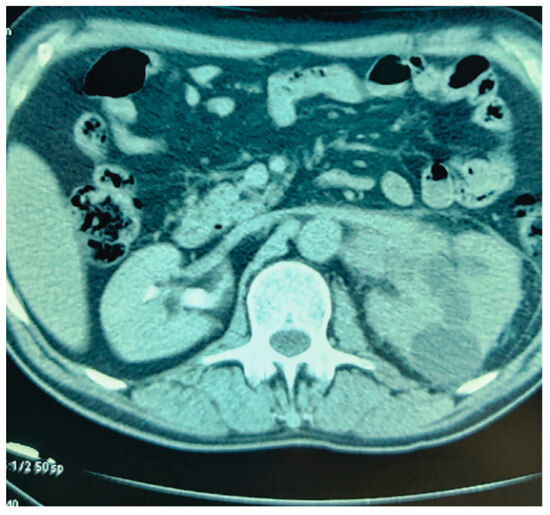
Figure 1.
Cross section of the left kidney Pyelocalycial dilation.
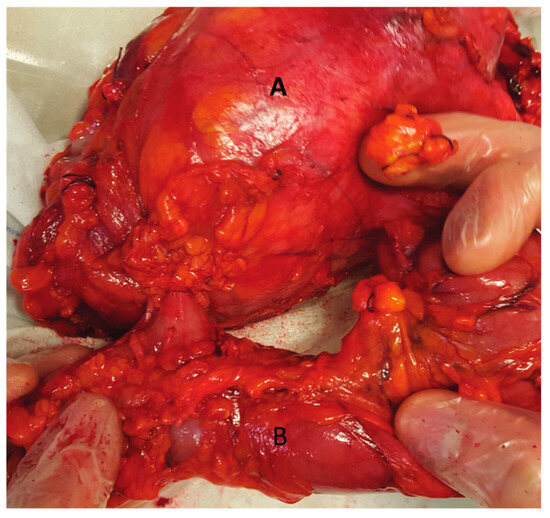
Figure 2.
One-piece resection: native left kidney (A) with fistula tract facing the left colon (B).
Conflicts of Interest
None declared. Patient Consent: Obtained..
References
- Vidal Sans, J.; Reig Ruiz, C. Fístulas urodigestivas: diagnóstico y tratamiento de 76 casos [Urodigestive fistulae: the diagnosis and treatment of 76 cases]. Arch. Esp. Urol. 1995, 48, 241–246. (In Spanish) [Google Scholar] [PubMed]
- Suhler, A.; Schimmel, F.; Viville, C. Fistules entéro-urinaires d'origine rénale et pyélique [Intestinal urinary fistulas of renal and pelvis origin]. Ann. Urol. 1995, 29, 8–10. (In French) [Google Scholar] [PubMed]
- El Otmany, A.; Hamada, H.; Hachi, H.; Benjelloun, S.; Oukhira, H.; Souadka, A. Fistule réno-sigmoïdienne sur un rein ectopique pelvien tuberculeux. Prog. Urol. 1999, 9, 122–124. [Google Scholar] [PubMed]
- Iwashita, Y.; Negi, S.; Iwashita, Y.; Higashiura, M.; Shigi, Y.; Yamanaka, S.; Ohya, M.; Mima, T.; Shigematsu, T. Severe refractory infection due to renocolic fistula in a patient with a giant kidney and ADPKD undergoing long-term hemodialysis. CEN Case Rep. 2018, 7, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Suhler, A.; Garbit, J.L.; Blitz, M. Fistules urétéro-intestinales [Uretero-intestinal fistulas]. Ann. Urol. 1995, 29, 15–17. (In French) [Google Scholar] [PubMed]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.