We report a striking duplication of the entire urinary collecting system in an 18-year-old male with 2 renal pelves and 2 ureters on either side, along with a complete duplication of the bladder and urethra. The patient had previously undergone surgical interventions for lipomeningomyelocele, anorectal malformation, rectovesical fistula, and vesical calculus (right hemibladder). On videourodynamics, the hemibladders showed poor compliance, altered bladder morphology, gross secondary vesicoureteral reflux with acontractlity, and large post-void residual volumes. The patient’s profound urinary incontinence resolved with daily administration of solifenacin 5mg and (double) clean intermittent catheterization through both the urethrae. Serum creatinine was 1.1mg/dL, down from a peak of 1.45mg/dL, and the severe hydronephrosis has shown some improvement.
Figure 1 shows the first MRI image of complete urinary tract duplication demonstrating 2 renal pelves and 2 ureters on either side, 2 hemibladders (sagittal duplication) and 2 complete urethrae. Bilateral reflux into the lower moiety can be seen on dual urethrocystogram via both the urethrae. The glans showed 2 well-developed urethral meatuses with an intervening bridge of tissue consistent with Effman type III (complete) duplication [1].
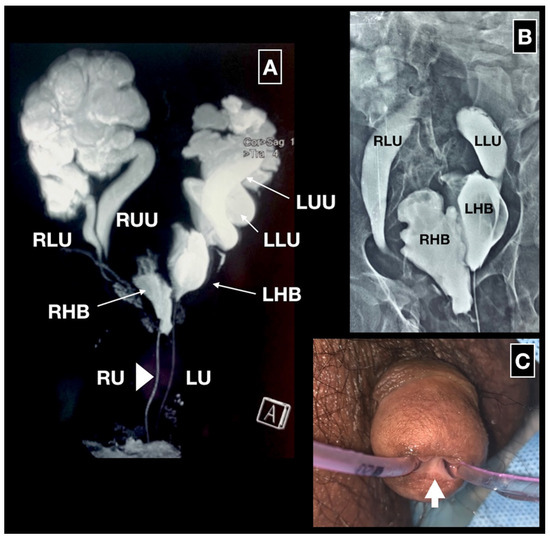
Figure 1.
MRI, dual urethrocystogram and clinical photograph of the glans. 1A. MRI shows 2 renal pelves and 2 ureters (RLU right lower moiety ureter, RUU right upper moiety ureter, LLU left lower moiety ureter, LUU left upper moiety ureter), the bladder split sagittally into 2 hemibladders (RHB right hemibladder, LHB left hemibladder) and complete duplication of the urethra (RU urethra draining the right hemibladder, LU urethra draining the left hemibladder). 1B. Retrograde urethrocystogram done via both the urethrae. The left hemibladder was placed somewhat cranial to the right one with reflux into bilateral lower ureters. 1C. Clinical photograph showing the 2 well-developed urethrae with an intervening bridge of tissue (arrow).
The extraordinary rarity of this condition can be attributed to different embryological origins of various parts of the urinary tract. The condition encountered would require coincidental splitting of the urethral plate, the urogenital sinus, and both ureteric buds, as well as compatibility with survival [2]. While double ureter is encountered in about 1% of the population, the other 2 conditions have been reported only in sporadic case reports [2]. To the best of our knowledge, there are no reports of all these abnormalities occurring in the same individual. This is also perhaps the first report of dual intermittent catheterization to empty 2 lower urinary tracts.
References
- Effmann, E.L.; Lebowitz, R.L.; Colodny, A.H. Duplication of the urethra. Radiology 1976, 119, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Baskin, L.S.; Cunha, G. Embryology of the human genitourinary tract. In Campbell-Walsh-Wein Urology, 12th ed.; Partin, A.W., Dmochowski, R.R., Kavoussi, L.R., Peters, C.A., Eds.; Elsevier: Philadelphia, PA, USA, 2020; pp. 305–340. [Google Scholar]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2021 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.