Abstract
The PLASMIC score for the prediction of a likelihood of a severe ADAMTS13 deficiency represents a valid pre-test diagnostic tool to identify patients with thrombotic thrombocytopenic purpura.
1. Introduction
The PLASMIC score was proposed to predict the likelihood of a severe ADAMTS13 deficiency in the context of Thrombotic MicroAngiopathies (TMAs), to promptly identify and properly treat acute patients with suspected Thrombotic Thrombocytopenic Purpura (TTP) [1]. We evaluated the diagnostic performance of the score in patients consecutively referred to our Unit.
2. Materials and Methods
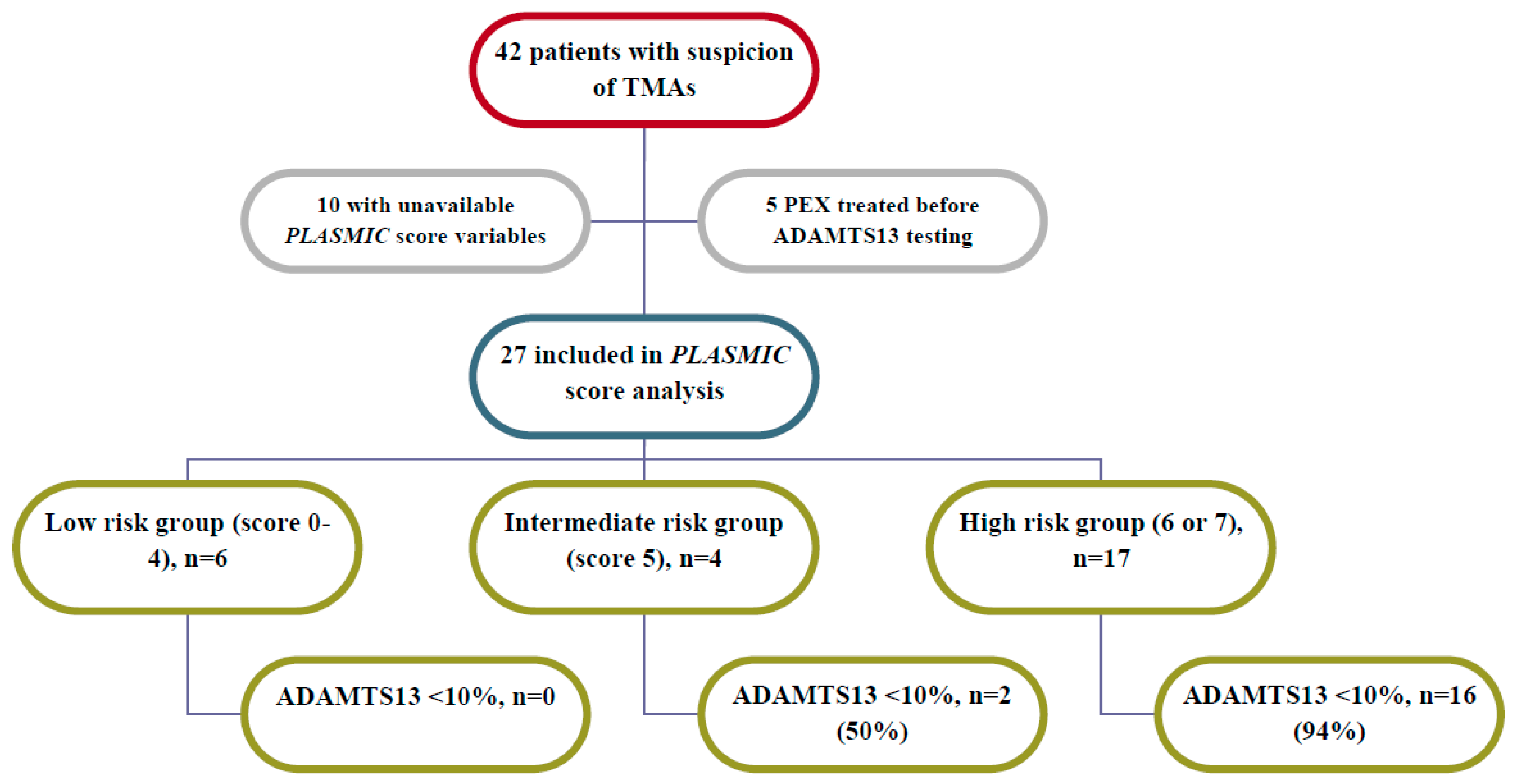
From 2012 to 2017, we tested ADAMTS13 in 42 patients diagnosed with TMA. From electronic records we extracted clinical and laboratory data referred to time of blood drawn for ADAMTS13 testing: full data were available for 25 of them (Figure.1). The score evaluates 7 parameters (1) point each): -platelet count <30 × 109/L, -hemolysis variables (reticulocyte count >2.5%, undetectable haptoglobin, or indirect bilirubin >2 mg/dL), -no active cancer, -no history of cell transplant, -mean corpuscular volume (MCV) <90 fL, -INR <1.5, and -creatinine level <2 mg/dL. Scoring system is defined low (0–4), intermediate (5), high (6–7) likelihood of ADAMTS13 <10%. Relevant clinical data, i.e., therapeutic procedures and immunosuppressive agents use, were collected. A ROC curve was generated and the Area Under Curve (AUC) was calculated to test the discrimination value.
3. Results
The PLASMIC score showed a good discrimination performance with a resulting AUC of 0.89 (95%CI 0.76–1.00; p = 0.008). According to the prediction model, we observed 6 patients in the low risk group, 4 and 15 in the intermediate and high-risk group, respectively. No severe deficiency was found in any case in the low-risk group, whereas a severe deficiency was found in 2 out of 4 intermediate-risk group patients and in 14 out of 15 high-risk group patients. In the low-intermediate risk group (0–5), we observed 2 short term (i.e.,: within 1 week after the disease onset) deaths, both in patients with severe sepsis. All 25 patients were treated by Plasma EXchange (PEX) and steroids. Nine patients [4 with a refractory TTP and 5 with relapsed TTP (2 of 3 patients having previous episodes of TTP)] were also treated by rituximab. We identified a TTP relapse in 3 (1 with score of 5) severely-deficient patients: in 2 of them (score = 6), who were diagnosed with cancer (pancreatic cancer and myeloproliferative neoplasm), a long-term death occurred.
4. Discussion
In our patients, PLASMIC score has a good predictive value of the pretest likelihood of a severe ADAMTS13 deficiency. Further research is needed to confirm present data.
Bullet points
- To discriminate patients with TMAs is challenging
- ADAMTS13 activity below 10% is specific for TTP
- PLASMIC score helps to identify TTP patients in absence of ADAMTS13 test
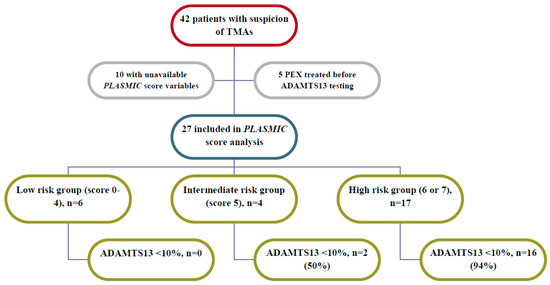
Figure 1.
Flow chart describing patients observed from January 2012–September 2017.
Figure 1.
Flow chart describing patients observed from January 2012–September 2017.
Conflicts of Interest
The authors declare no conflict of interest.
Reference
- Bendapudi, P.K.; Hurwitz, S.; Fry, A.; Marques, M.B.; Waldo, S.W.; Li, A.; Sun, L.; Upadhyay, V.; Hamdan, A.; Brunner, A.M.; et al. Derivation and external validation of the PLASMIC score for rapid assessment of adults with thrombotic microangiopathies: A cohort study. Lancet Haematol. 2017, 4, e157–e164. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).