
Practical Models of Pharmaceutical Care for Improving Tuberculosis Patient Detection and Treatment Outcomes: A Systematic Scoping Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Search Strategy
2.2. Study Criteria
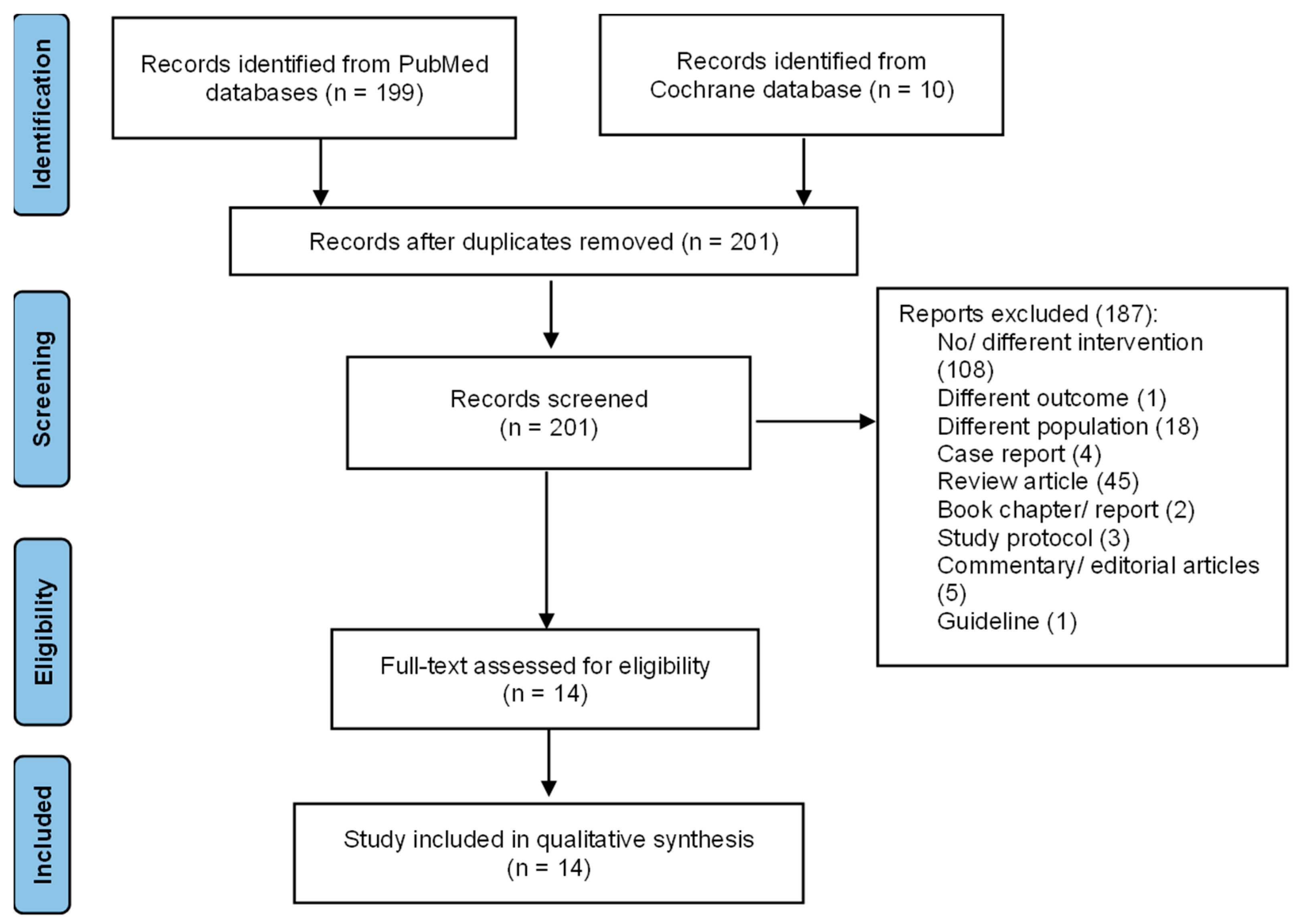
2.3. Article Selection, Data Extraction, and Analysis
3. Results
3.1. PC in Increasing TB Patient Detection
3.2. PC in Improving TB Treatment Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2022; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Pradipta, I.S.; Idrus, L.R.; Probandari, A.; Puspitasari, I.M.; Santoso, P.; Alffenaar, J.-W.C.; Hak, E. Barriers to Optimal Tuberculosis Treatment Services at Community Health Centers: A Qualitative Study From a High Prevalent Tuberculosis Country. Front. Pharmacol. 2022, 13, 936. [Google Scholar] [CrossRef] [PubMed]
- Pradipta, I.S.; Idrus, L.R.; Probandari, A.; Lestari, B.W.; Diantini, A.; Alffenaar, J.-W.C.; Hak, E. Barriers and Strategies to Successful Tuberculosis Treatment in a High-Burden Tuberculosis Setting: A Qualitative Study from the Patient’s Perspective. BMC Public Health 2021, 21, 1903. [Google Scholar] [CrossRef] [PubMed]
- Lestari, B.W.; McAllister, S.; Hadisoemarto, P.F.; Afifah, N.; Jani, I.D.; Murray, M.; van Crevel, R.; Hill, P.C.; Alisjahbana, B. Patient Pathways and Delays to Diagnosis and Treatment of Tuberculosis in an Urban Setting in Indonesia. Lancet Reg. Health West. Pac. 2020, 5, 59. [Google Scholar] [CrossRef] [PubMed]
- Surya, A.; Setyaningsih, B.; Suryani Nasution, H.; Gita Parwati, C.; Yuzwar, Y.E.; Osberg, M.; Hanson, C.L.; Hymoff, A.; Mingkwan, P.; Makayova, J.; et al. Quality Tuberculosis Care in Indonesia: Using Patient Pathway Analysis to Optimize Public-Private Collaboration. J. Infect. Dis. 2017, 216, S724–S732. [Google Scholar] [CrossRef] [PubMed]
- De Resende, N.H.; de Miranda, S.S.; Ceccato, M.D.G.B.; Haddad, J.P.A.; Reis, A.M.M.; da Silva, D.I.; Carvalho, W.D.S. Drug Therapy Problems for Patients with Tuberculosis and HIV/AIDS at a Reference Hospital. Einstein 2019, 17, eAO4696. [Google Scholar] [CrossRef]
- Nakatani, H.; Buchmann, M. Working Together: WHO and FIP; FIP: Hyderabad, India, 2011. [Google Scholar]
- Flottorp, S.A.; Oxman, A.D.; Krause, J.; Musila, N.R.; Wensing, M.; Godycki-Cwirko, M.; Baker, R.; Eccles, M.P. A Checklist for Identifying Determinants of Practice: A Systematic Review and Synthesis of Frameworks and Taxonomies of Factors That Prevent or Enable Improvements in Healthcare Professional Practice. Implement. Sci. 2013, 8, 35. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Ullah, W.; Almansour, H.; Fatima, R.; Saini, B.; Khan, G.M. Engaging Community Pharmacies in Early Detection of Missing Tuberculosis Patients through Public-Private Mix Intervention in Pakistan. Am. J. Trop. Med. Hyg. 2020, 103, 221–230. [Google Scholar] [CrossRef]
- Lonnroth, K.; Karlsson, M.; Lan, N.T.N.; Buu, T.N.; Dieu, T.T.N. Referring TB Suspects from Private Pharmacies to the National Tuberculosis Programme: Experiences from Two Districts in Ho Chi Minh City, Vietnam. Int. J. Tuberc. Lung Dis. 2003, 7, 1147–1153. [Google Scholar]
- Lambert, M.L.; Delgado, R.; Michaux, G.; Vols, A.; Speybroeck, N.; Van Der Stuyft, P. Collaboration between Private Pharmacies and National Tuberculosis Programme: An Intervention in Bolivia. Trop. Med. Int. Health 2005, 10, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Jakeman, B.; Logothetis, S.J.; Roberts, M.H.; Bachyrycz, A.; Fortune, D.; Borrego, M.E.; Ferreira, J.; Burgos, M. Addressing Latent Tuberculosis Infection Treatment through a Collaborative Care Model with Community Pharmacies and a Health Department. Prev. Chronic Dis. 2020, 17, E14. [Google Scholar] [CrossRef] [PubMed]
- Jakeman, B.; Gross, B.; Fortune, D.; Babb, S.; Tinker, D.; Bachyrycz, A. Evaluation of a Pharmacist-Performed Tuberculosis Testing Initiative in New Mexico. J. Am. Pharm. Assoc. 2015, 55, 307–312. [Google Scholar] [CrossRef]
- Carter, K.L.; Gabrellas, A.D.; Shah, S.; Garland, J.M. Improved Latent Tuberculosis Therapy Completion Rates in Refugee Patients through Use of a Clinical Pharmacist. Int. J. Tuberc. Lung Dis. 2017, 21, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Hecox, N. Tuberculin Skin Testing by Pharmacists in a Grocery Store Setting. J. Am. Pharm. Assoc. 2008, 48, 86–91. [Google Scholar] [CrossRef]
- Hess, K.; Goad, J.; Wu, J.; Johnson, K. Isoniazid Completion Rates for Latent Tuberculosis Infection among College Students Managed by a Community Pharmacist. J. Am. Coll. Health 2009, 57, 553–555. [Google Scholar] [CrossRef] [PubMed]
- Tanvejsilp, P.; Pullenayegum, E.; Loeb, M.; Dushoff, J.; Xie, F. Role of Pharmaceutical Care for Self-Administered Pulmonary Tuberculosis Treatment in Thailand. J. Clin. Pharm. Ther. 2017, 42, 337–344. [Google Scholar] [CrossRef]
- Juan, G.; Lloret, T.; Perez, C.; Lopez, P.; Navarro, R.; Ramón, M.; Cortijo, J.; Morcillo, E.J. Directly Observed Treatment for Tuberculosis in Pharmacies Compared with Self-Administered Therapy in Spain. Int. J. Tuberc. Lung Dis. 2006, 10, 215–221. [Google Scholar]
- Tang, Z.Q.; Jiang, R.H.; Xu, H. Bin Effectiveness of Pharmaceutical Care on Treatment Outcomes for Patients with First-Time Pulmonary Tuberculosis in China. J. Clin. Pharm. Ther. 2018, 43, 888–894. [Google Scholar] [CrossRef]
- Clark, P.M.; Karagoz, T.; Apikoglu-Rabus, S.; Izzettin, F.V. Effect of Pharmacist-Led Patient Education on Adherence to Tuberculosis Treatment. Am. J. Health-Syst. Pharm. 2007, 64, 497–506. [Google Scholar] [CrossRef]
- Karuniawati, H.; Putra, O.N.; Wikantyasning, E.R. Impact of Pharmacist Counseling and Leaflet on the Adherence of Pulmonary Tuberculosis Patients in Lungs Hospital in Indonesia. Indian J. Tuberc. 2019, 66, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.R.V.; De Miranda, S.S.; Ceccato, M.D.G.B.; Silveira, M.R.; de Resende, N.H.; Carvalho, W.S. Evaluation of the Impact of Pharmaceutical Care for Tuberculosis Patients in a Secondary Referral Outpatient Clinic, Minas Gerais, Brazil. An Acad. Bras. Cienc. 2017, 89, 2911–2919. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Sánchez Pozo, A.; Rekkas, D.; Volmer, D.; Hirvonen, J.; Bozic, B.; Skowron, A.; Mircioiu, C.; Sandulovici, R.; Marcincal, A.; et al. Hospital and Community Pharmacists’ Perceptions of Which Competences Are Important for Their Practice. Pharmacy 2016, 4, 21. [Google Scholar] [CrossRef]
- Toni, J.; Lipovec, N.C.; Sorli, P.S.; Kosnik, M. Pharmacist’s Role in the Treatment of Patients with Tuberculosis ñ Our Positive Experience. Eur. J. Hosp. Pharm. 2012, 19, 250. [Google Scholar] [CrossRef]
- Pradipta, I.S.; Khairunnisa, K.; Bahar, M.A.; Kausar, M.N.; Fitriana, E.; Ruslami, R.; Aarnoutse, R.E. Knowledge, Attitude and Practice of Community Pharmacy Personnel in Tuberculosis Patient Detection: A Sectional Study in a Burden Tuberculosis Setting. BMJ Open 2022, 12, e060078. [Google Scholar] [CrossRef]
- Bigio, J.; Aquilera Vasquez, N.; Huria, L.; Pande, T.; Creswell, J.; Ananthakrishnan, R.; Bimba, J.S.; Cuevas, L.E.; Vo, L.; Bakker, M.I.; et al. Engaging Pharmacies in Tuberculosis Control: Operational Lessons from 19 Case Detection Interventions in High-Burden Countries. BMJ Glob. Health 2022, 7, e008661. [Google Scholar] [CrossRef]
- Ridho, A.; Alfian, S.D.; van Boven, J.F.M.; Levita, J.; Yalcin, E.A.; Le, L.; Alffenaar, J.W.; Hak, E.; Abdulah, R.; Pradipta, I.S. Digital Health Technologies to Improve Medication Adherence and Treatment Outcomes in Patients With Tuberculosis: Systematic Review of Randomized Controlled Trials. J. Med. Internet Res. 2022, 24, e33062. [Google Scholar] [CrossRef]


{kind=link}
| No | Authors, Year | Objective | Design | Period | Location | Targeted Service | Outcome Orientation |
|---|---|---|---|---|---|---|---|
| 1 | Ullah et al., 2020 [11] | Assessing the effectiveness of TB case detection activities by pharmacy personnel. | Program implementation | January to December 2017 | Three areas in Pakistan | Presumptive TB patients | Increasing TB patient detection. |
| 2 | Lonnroth et al., 2003 [12] | Describing community pharmacist attitude in the program of TB referral system for presumptive TB patients and evaluating the program’s feasibility. | Mixed methods followed the implementation program | April 2001 to December 2002 | Ho Chi Minh, Vietnam | Presumptive TB patients | Increasing TB patient detection. |
| 3 | Lambert et al., 2005 [13] | Providing interventions to community pharmacists in decreasing anti-TB sales in pharmacies and increasing pharmacy personnel activities on the referral of presumptive TB patient activities to the health facility. | Intervention study | January to March 2002 | Cochabamba, Bolivia | Presumptive TB patients | Increasing TB patient detection. |
| 4 | Jakeman et al., 2015 [15] | Describing community pharmacy experiences in TST program. | Program implementation | March 2011 to August 2013. | New Mexico, USA | Risk population of LTBI patients | Increasing TB patient detection. |
| 5 | Jakeman et al., 2020 [14] | Evaluating collaborative TB care between the public health department and community pharmacy in managing newly LTBI patients. | Program implementation | February 2017 to April 2018 | New Mexico, USA | Newly diagnosed LTBI patients | Improving TB treatment outcomes. |
| 6 | Tanvejsil et al., 2016 [19] | Comparing TB treatment success among three services in TB patients, i.e., PC, home visit, and modified DOT. | Observational study | February 2017 | Songkhla, Thailand | Adult pulmonary TB patients. | Improving TB treatment outcomes. |
| 7 | Juan et al., 2006 [20] | Comparing DOT through pharmacies with SAT in high-risk patients of non-adherence. | Observational study | 1 January 1999 to 31 December 2002 | Valencia, Spain | High risk of non-adherent TB patients * | Improving TB treatment outcomes. |
| 8 | Carter et al., 2017 [16] | Assessing the effect of a clinical pharmacist-run clinic for LTBI on the treatment completion rates in refugee patients. | Observational study | August 2012 to April 2016 | Philadelphia and Pennsylvania, USA | Refugees with LTBI | Improving TB treatment outcomes. |
| 9 | Tang et al., 2018 [21] | Assessing the effect of PC on TB treatment outcomes compared with the UC. | A randomized case–control study | June 2018 | Shanghai, China | Pulmonary TB patients who have already received a TB regimen of less than one month | Improving TB treatment outcomes. |
| 10. | Clark et al., 2007 [22] | Assessing the effect of educational programs provided by pharmacists to improve medication adherence compared with a group without the educational program. | A randomized case–control study | August 2001 to February 2002 | Istanbul, Turkey | Newly diagnosed TB and MDR-TB patients | Improving TB treatment outcomes. |
| 11 | Karuniawati et al., 2019 [23] | Assessing the effect of pharmacist counselling using written information (leaflet). | Quasi experimental | July to December 2017 | Surakarta, Indonesia | Adult TB patients who have received TB medication for at least one month | Improving TB treatment outcomes. |
| 12 | Lopes et al., 2017 [24] | Describing and evaluating the effect of PC on TB patients. | Observational study | August 2009 to July 2012 | Belo horizinte, Brazil | Adult TB outpatient | Improving TB treatment outcomes. |
| 13 | Hess et al., 2009 [18] | Describing treatment completion rates for LTBI in a community pharmacy in a college campus. | Observational study | 2000–2006 | California, USA | University students diagnosed with LTBI | Improving TB treatment outcomes. |
| 14 | Hecox, 2008 [17] | To report experiences of pharmacist-provided TSTs. | Observational study | February to December 2006 | Washington, USA | Public who will have TSTs | Increasing TB case detection. |
| No. | PC Models | Authors | Setting Area | Outcomes |
|---|---|---|---|---|
| 1 | Pharmacy personnel screened TB signs and symptoms in their pharmacy to identify presumptive TB patients, then referred the patient to a health facility for further TB examination. | Ullah et al., 2020 [11] | Community |
|
| Lonnroth et al., 2003 [12] | Community |
| ||
| Lambert et al., 2005 [13] | Community |
| ||
| 2 | Pharmacists were granted the authority to prescribe, administer, and read TSTs. | Jakeman et al., 2015 [15] | Community |
|
| Hecox, 2008 [17] | Community |
|
| No. | PC Models | Authors | Setting Area | Outcomes |
|---|---|---|---|---|
| 1. | The community pharmacist provided weekly DOT services for newly diagnosed LTBI patients for 12 weeks. The PC included evaluating drug interaction and drug toxicity, dispensing LTBI regimen, monitoring medication adherence, and reporting the incidence of ADR to the relevant public health department. | Jakeman et al., 2020 [14] | Community |
|
| 2 | After the LTBI patients were diagnosed by a student health clinician and referred to the pharmacy, the pharmacist provided scheduled counseling with the patient on the importance of treating LTBI; medication adherence assessment by counting the pill or patient self-reported; assessment of ADR and risk factors of failed treatment. | Hess et al., 2009 [18] | Community |
|
| 3. | Pharmacists conducted a monthly visit to the refugee diagnosed with LTBI with several activities, i.e., assessing drug-related problems (e.g., drug interaction, ADR), following up on the DRPs occurred (lab examination and drug modification), and patient counseling for medication adherence. | Carter et al., 2017 [16] | Community |
|
| 4. | The community pharmacists included in the district-based DOT program comprised a hospital pulmonologist staff, the community pharmacist, and a part-time social worker. After the high-risk criteria of TB patients were diagnosed and discharged from the hospital, the patients were assigned to continue the medication at the nearest community pharmacist where they lived. The community pharmacist provided several services during each patient visit, such as reinforcing the importance of treatment adherence, making inquiries about the occurrence of any drug-related event, reminding the patient about forthcoming appointments at the pharmacy and hospital, and offering the required sociosanitary support. The pharmacist initiated contact by phone or home visits to identify the reasons for default and to ensure the continuation of treatment. | Juan et al., 2006 [20] | Community |
|
| 5. | In the PC service, the clinical pharmacist provides TB care when the patient visits the hospital, including educational intervention, assessment of drug-related problems, drug monitoring (ADR and medication adherence), and phone consultation for drug-related issues. | Tanvejsilp et al., 2016 [19] | Hospital | The percentage of treatment success in the PC intervention was the highest (94,90%; 95%CI 91.57–95.63). It was followed by the home visit (93.60%; 95%CI 91.57–95.63) and the modified DOT (90.10%; 95%CI 87.54–92.66). |
| 6. | Clinical pharmacists provided scheduled face-to-face or phone communication with TB patients regarding the educational program for medication adherence and successful treatment, identification DRPs, drug monitoring for ADR (e.g., lab check for ADR), and its follow-up. | Tang et al., 2018 [21] | Hospital |
|
| 7. | Pharmacists provided standard written and oral TB education for the TB inpatients and provided outpatient TB care with a routine schedule after they were discarded from the hospital. The PC also assessed the DRPs of TB patients. | Clark et al., 2007 [22] | Hospital |
|
| 8. | The hospital pharmacist provided oral and standardized written TB counseling to improve medication adherence. | Karuniawati et al., 2019 [23] | Hospital | The proportion of patients who received counseling and leaflets was the highest in improving medication adherence. It was followed by the group of patients who only received counseling and control (without counseling and leaflet) groups. |
| 9. | The hospital pharmacist provided routine consultation, performed pharmacology and non-pharmacology intervention, and assessed DRPs and ADR with the standardized instrument. | Lopes et al., 2017 [24] | Hospital |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradipta, I.S.; Yanuar, E.O.; Nurhijriah, C.Y.; Maharani, N.P.; Subra, L.; Destiani, D.P.; Diantini, A. Practical Models of Pharmaceutical Care for Improving Tuberculosis Patient Detection and Treatment Outcomes: A Systematic Scoping Review. Trop. Med. Infect. Dis. 2023, 8, 287. https://doi.org/10.3390/tropicalmed8050287
Pradipta IS, Yanuar EO, Nurhijriah CY, Maharani NP, Subra L, Destiani DP, Diantini A. Practical Models of Pharmaceutical Care for Improving Tuberculosis Patient Detection and Treatment Outcomes: A Systematic Scoping Review. Tropical Medicine and Infectious Disease. 2023; 8(5):287. https://doi.org/10.3390/tropicalmed8050287
Chicago/Turabian StylePradipta, Ivan Surya, Erya Oselva Yanuar, Chaca Yasinta Nurhijriah, Nadya Putri Maharani, Laila Subra, Dika Pramita Destiani, and Ajeng Diantini. 2023. "Practical Models of Pharmaceutical Care for Improving Tuberculosis Patient Detection and Treatment Outcomes: A Systematic Scoping Review" Tropical Medicine and Infectious Disease 8, no. 5: 287. https://doi.org/10.3390/tropicalmed8050287
APA StylePradipta, I. S., Yanuar, E. O., Nurhijriah, C. Y., Maharani, N. P., Subra, L., Destiani, D. P., & Diantini, A. (2023). Practical Models of Pharmaceutical Care for Improving Tuberculosis Patient Detection and Treatment Outcomes: A Systematic Scoping Review. Tropical Medicine and Infectious Disease, 8(5), 287. https://doi.org/10.3390/tropicalmed8050287