

Increasing the Awareness of Under-Diagnosed Tropical Cases of Dengue in Romania


 , , ,
, , , 
Abstract
:1. Introduction
2. Detailed Case Description
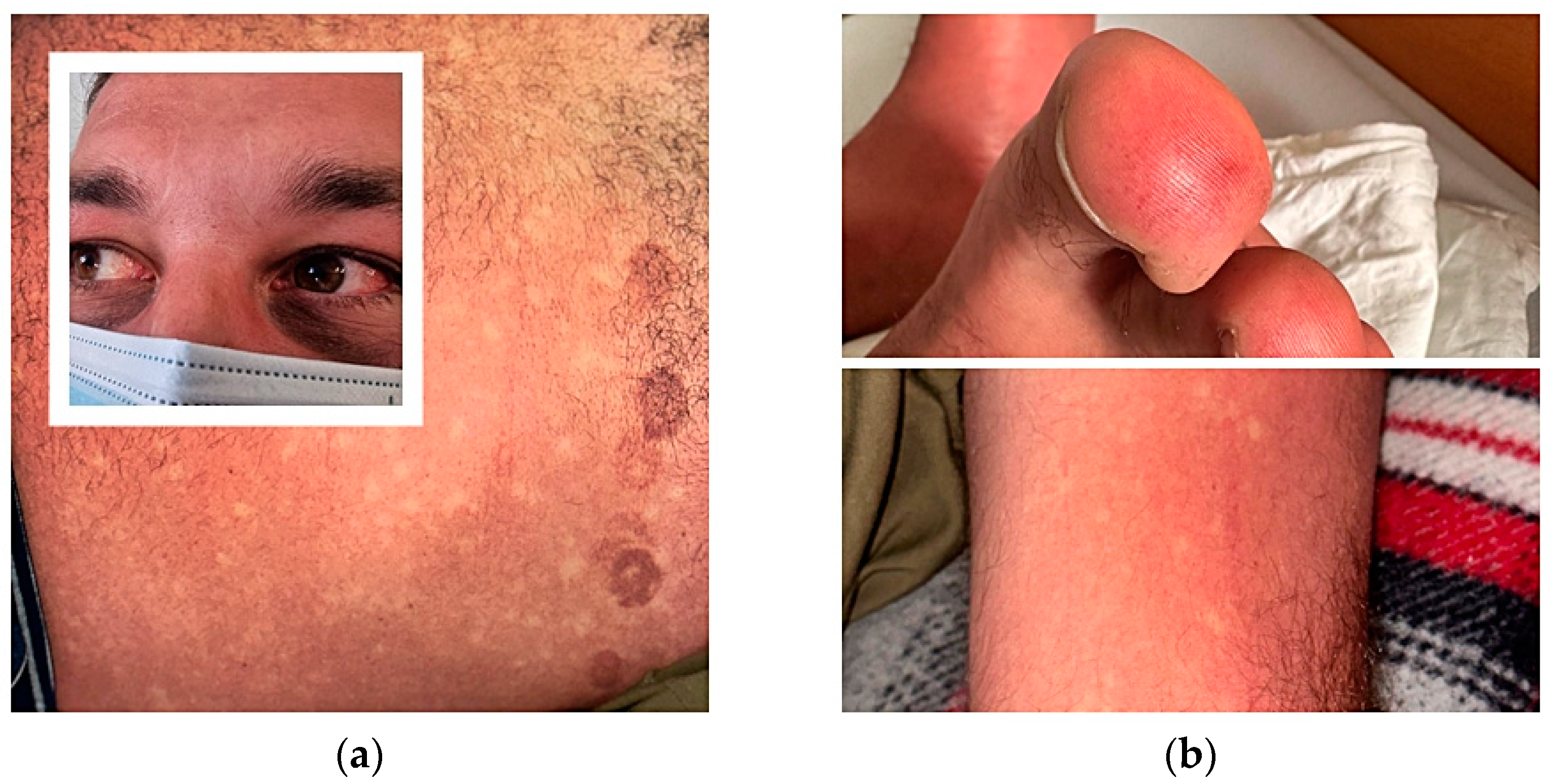
2.1. Case 1
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Impact-Assessment-of-the-COVID-19-Outbreak-on-International-Tourism. 2023. Available online: https://www.unwto.org/impact-assessment-of-the-covid-19-outbreak-on-international-tourism (accessed on 2 August 2023).
- Schaffner, F.; Mathis, A. Dengue and dengue vectors in the WHO European Region: Past, present, and scenarios for the future. Lancet Infect. Dis. 2014, 14, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Guzmán, M.G.; Kouri, G. Dengue: An update. Lancet Infect. Dis. 2022, 2, 33–42. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue and Severe Dengue Fact Sheet. April 2017. Available online: http://www.who.int/mediacentre/factsheets/fs117/en/ (accessed on 5 August 2023).
- Harapan, H.; Michie, A.; Sasmono, R.T.; Imrie, A. Dengue: A minireview. Viruses 2020, 12, 829. [Google Scholar] [CrossRef] [PubMed]
- Seixas, G.; Salgueiro, P.; Bronzato-Badial, A.; Gonçalves, Y.; Reyes-Lugo, M.; Gordicho, V.; Ribolla, P.; Viveiros, B.; Silva, A.C.; Pinto, J.; et al. Origin and expansion of the mosquito Aedes aegypti in Madeira Island (Portugal). Sci. Rep. 2019, 24, 2241. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.ecdc.europa.eu/en/dengue-monthly (accessed on 3 August 2023).
- European Centre for Disease Prevention and Control. Aedes Albopictus—Current Known Distribution. October 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/aedes-albop (accessed on 3 August 2023).
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2012, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization / World Health Organization. Epidemiological Update: Dengue in the Region of the Americas; PAHO/WHO: Washington, DC, USA, 5 July 2023. [Google Scholar]
- European Center for Disease Prevention and Control (ECDC). 2023. Available online: https://www.ecdc.europa.eu/en/publications-data/dengue-virus-disease-cases-june-2022-may-2023 (accessed on 30 July 2023).
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21(st) Century. 2011. Available online: https://pubmed.ncbi.nlm.nih.gov/22500131/ (accessed on 30 July 2023).
- Balmaseda, A.; Hammond, S.N.; Pérez, L.; Tellez, Y.; Indira, S.; Saborío, J.C.; Mercado, J.C.; Cuadra, R.; Rocha, J.; Pérez, M.A.; et al. Serotype-specific differences in clinical manifestations of dengue. Am. J. Trop. Med. Hyg. 2006, 74, 449–456. [Google Scholar] [CrossRef]
- Yacoub, S.; Wills, B. Dengue: An update for clinicians working in non-endemic areas. Clin. Med. 2015, 15, 82. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Comprehensive Guidelines for Prevention and Control of Dengue and Dengue Hemorrhagic Fever: Revised and Expanded Edition; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/204894 (accessed on 6 August 2023).
- Low, J.G.H.; Ong, A.; Tan, L.K.; Chaterji, S.; Chow, A.; Lim, W.Y.; Lee, K.W.; Chua, R.; Chua, C.R.; Tan, S.W.S.; et al. The Early Clinical Features of Dengue in Adults: Challenges for Early Clinical Diagnosis. PLoS Neglected Trop. Dis. 2011, 5, e1191. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Ooi, E.-E.; Vasudevan, S.G.; Gubler, D.J. Update on Dengue: Epidemiology, Virus Evolution, Antiviral Drugs, and Vaccine Development. March 2010. Available online: https://link.springer.com/article/10.1007/s11908-010-0102-7 (accessed on 5 August 2023).
- Waterman Stephen, H.; Gubler, D.J. Dengue fever. Clin. Dermatol. 1989, 7, 117. [Google Scholar] [CrossRef]
- Pincus Laura, B.; Grossman, M.E.; Fox, L.P. The exanthem of dengue fever: Clinical features of two US tourists traveling abroad. J. Am. Acad. Dermatol. 2008, 58, 308–316. [Google Scholar] [CrossRef]
- Tyring, S.; Moore, A.Y.; Lupi, O. Mucocutaneous Manifestations of Viral Diseases: An Illustrated Guide, Informa Health; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Andries, A.-C.; Duong, V.; Ly, S.; Cappelle, J.; Kim, K.S.; Try, P.L.; Ros, S.; Ong, S.; Huy, R.; Horwood, P.; et al. Value of Routine Dengue Diagnostic Tests in Urine and Saliva Specimens. PLoS Neglected Trop. Dis. 2015, 9, e0004100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Young, P.R.; Hilditch, P.A.; Bletchly, C.; Halloran, W. An antigen capture enzyme-linked immunosorbent assay reveals high levels of the dengue virus protein NS1 in the sera of infected patients. J. Clin. Microbiol. 2000, 28, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Alcon, S.; Talarmin, A.; Debruyne, M.; Falconar, A.; Deubel, V.; Flamand, M. Enzyme-linked immunosorbent assay specific to Dengue virus type 1 nonstructural protein NS1 reveals circulation of the antigen in the blood during the acute phase of disease in patients experiencing primary or secondary infections. J. Clin. Microbiol. 2002, 40, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Khosavanna, R.R.; Kareko, B.W.; Brady, A.C.; Booty, B.L.; Nix, C.D.; Lyski, Z.L.; Curlin, M.E.; Messer, W.B. Clinical Symptoms of Dengue Infection among Patients from a Non-Endemic Area and Potential for a Predictive Model: A Multiple Logistic Regression Analysis and Decision Tree. Am. J. Trop. Med. Hyg. 2021, 104, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Zhang, Y.; Wu, X.; Wu, J.; Gong, F.; Qiao, L.; Li, L.; Wang, C. A survey of clinical and laboratory characteristics of dengue fever epidemic from 2014 to 2018 in Guangzhou, China. Ann. Palliat. Med. 2020, 9, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.T.; Ho, T.N.; Nguyen, V.V.C.; Nguyen, T.H.; Ha, M.T.; Ta, V.T.; Da Ha Nguyen, L.; Phan, L.; Han, K.Q.; Duong, T.H.K.; et al. An evidence-based algorithm for early prognosis of severe dengue in the outpatient setting. Clinical Infectious Diseases. Clin. Infect. Dis. 2017, 64, 656–663. [Google Scholar] [PubMed]
- Verma, S.; Kanga, A.; Singh, D.; Verma, G.K.; Mokta, K.; Ganju, S.A.; Sharma, V. Emergence of travel: Associated dengue fever in a non-endemic, hilly state. Adv. Biomed. Res. 2014, 3, 239. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals: A Road Map for Neglected Tropical Diseases; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Ryan, S.J.; Carlson, C.J.; Mordecai, E.A.; Johnson, L.R. Global expansion and redistribution of Aedesborne virus transmission risk with climate change. PLoS Negl. Trop. Dis. 2019, 13, e0007213. [Google Scholar] [CrossRef]
- Oliveira, S.; Rocha, J.; Sousa, C.A.; Capinha, C. Wide and increasing suitability for Aedes albopictus in Europe is congruent across distribution models. Sci. Rep. 2021, 11, 9916. [Google Scholar] [CrossRef]
- Azarm, T.; Sohrabi, A.; Mohajer, H.; Azarm, A. Differential diagnosis of nontraumatic purpura in the elderly—Have you considered acquired hemophilia? J. Gerontol. Geriatr. 2019, 67, 168–180. [Google Scholar]
- Bennett, C.L.; Connors, J.M.; Carwile, J.M.; Moake, J.L.; Bell, W.R.; Tarantolo, S.R.; McCarthy, L.J.; Sarode, R.; Hatfield, A.J.; Feldman, M.D.; et al. Thrombotic Thrombocytopenic Purpura associated with Clopidogrel: A case report and review of the literature. J. Res. Med. Sci. 2011, 16, 353–357. [Google Scholar]
- Blacksell, S.D. Commercial dengue rapid diagnostic tests for point-of-care application: Recent evaluations and future needs? J. Biomed. Biotechnol. 2012, 2012, 151967. [Google Scholar] [CrossRef]
- Nisalak, A. Laboratory Diagnosis of Dengue Virus Infections. Southeast Asian J. Trop. Med. Public Health 2015, 46, 55–76. [Google Scholar]
- Zhang, H.; Li, W.; Wang, J.; Peng, H.; Che, X.; Chen, X.; Zhou, Y. NS1-based tests with diagnostic utility for confirming dengue infection: A meta-analysis. Int. J. Infect. Dis. 2014, 26, 57–66. [Google Scholar] [CrossRef]
- Dinu, S.; Pănculescu-Gătej, I.R.; Florescu, S.A.; Popescu, C.P.; Sîrbu, A.; Oprişan, G.; Bădescu, D.; Franco, L.; Ceianu, C.S. Molecular epidemiology of dengue fever cases imported into Romania between 2008 and 2013. Travel Med. Infect. Dis. 2015, 13, 69–73. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Clinical Presentation | Case 1 | Case 2 |
|---|---|---|
| Fever | +++ | + |
| Maculo-papular exanthema | +++ | ++ |
| Myalgia | ++ | + |
| Arthralgia | +++ | + |
| Oedema | + | - |
| Retro-orbital pain | ++ | - |
| Conjunctivitis | ++ | - |
| Lymphadenopathy | - | - |
| Hepatomegaly | - | - |
| Haemorrhage | + | - |
| Incubation period (define by days between return from the epidemiological area and onset of symptoms) | 12 | 3 |
| Laboratory Findings | Case 1 | Case 2 | Reference Values |
|---|---|---|---|
| Anaemia | 12.7 g/dL | 13 g/dL | (13–15) |
| Leukopenia | 2.9 × 103/μL | 3 × 103/μL | (4–10 × 103) |
| Neutropenia | 2.2 × 103/μL | 1.8 × 103/μL | (2.2–4.8 × 103) |
| Lymphocytopenia | 0.9 × 103/μL | 1 × 103/μL | (1.3–2.9 × 103) |
| Thrombocytopenia | 100 × 103/μL | 137 × 103/μL | (150–400 × 103) |
| Increased CRP | 32 mg/L | 12 mg/L | (0–5) |
| Increased ALT | 320 U/L | 280 U/L | (0–31) |
| Haematocrit | 40% | 43% | (35–47) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cismaru, I.M.; Radu, M.A.; Cotar, A.I.; Oancea, F.; Melinte, V.; Vacaroiu, C.; Ghemulet, I.; Gheorghita, V. Increasing the Awareness of Under-Diagnosed Tropical Cases of Dengue in Romania. Trop. Med. Infect. Dis. 2023, 8, 469. https://doi.org/10.3390/tropicalmed8100469
Cismaru IM, Radu MA, Cotar AI, Oancea F, Melinte V, Vacaroiu C, Ghemulet I, Gheorghita V. Increasing the Awareness of Under-Diagnosed Tropical Cases of Dengue in Romania. Tropical Medicine and Infectious Disease. 2023; 8(10):469. https://doi.org/10.3390/tropicalmed8100469
Chicago/Turabian StyleCismaru, Ioana Miriana, Maria Adelina Radu, Ani Ioana Cotar, Florin Oancea, Violeta Melinte, Cristina Vacaroiu, Isabela Ghemulet, and Valeriu Gheorghita. 2023. "Increasing the Awareness of Under-Diagnosed Tropical Cases of Dengue in Romania" Tropical Medicine and Infectious Disease 8, no. 10: 469. https://doi.org/10.3390/tropicalmed8100469
APA StyleCismaru, I. M., Radu, M. A., Cotar, A. I., Oancea, F., Melinte, V., Vacaroiu, C., Ghemulet, I., & Gheorghita, V. (2023). Increasing the Awareness of Under-Diagnosed Tropical Cases of Dengue in Romania. Tropical Medicine and Infectious Disease, 8(10), 469. https://doi.org/10.3390/tropicalmed8100469