
COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis
 ,
,  , , , , , , , , and
, , , , , , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Measures
2.2. Data Sources
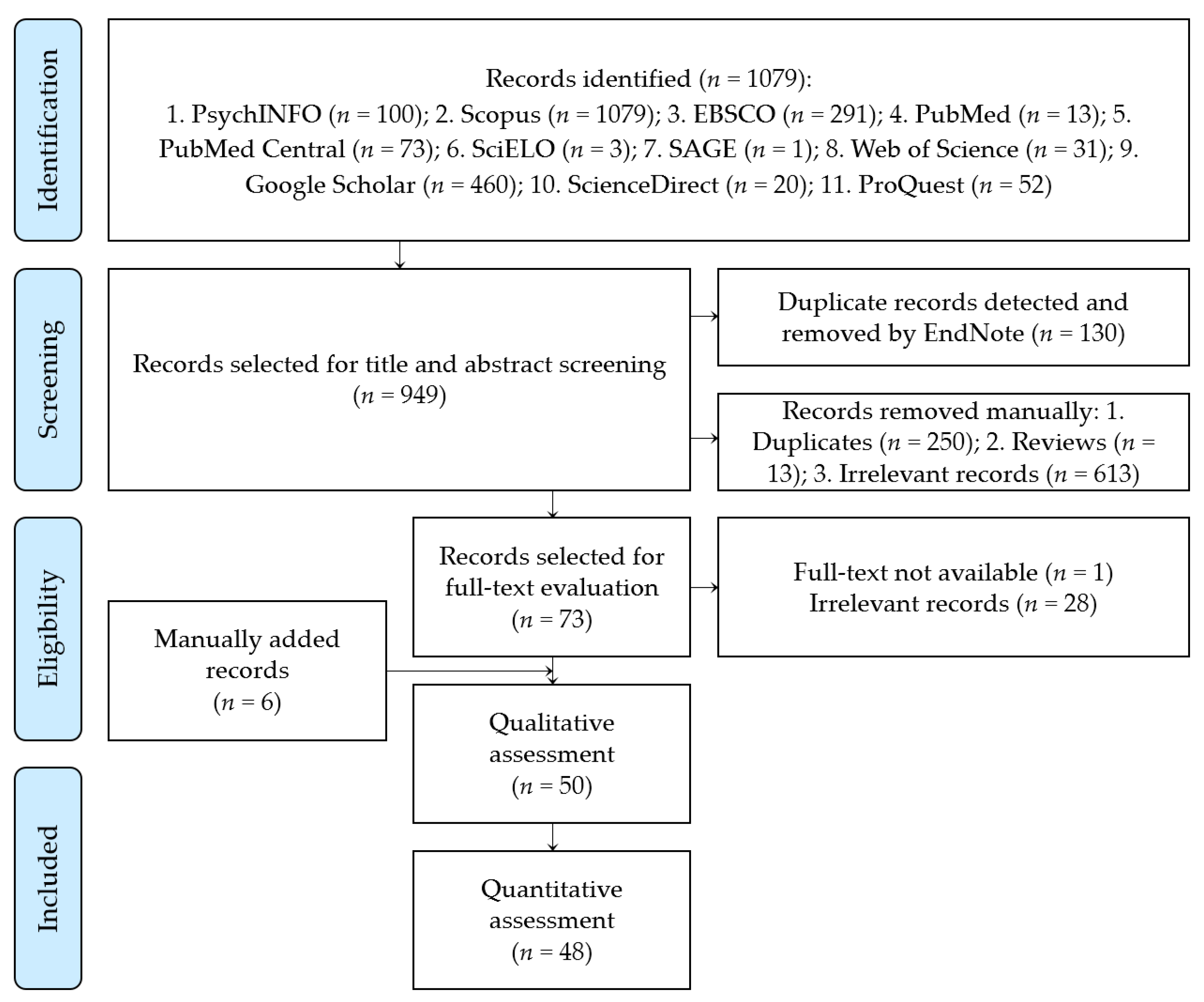
2.3. Data Extraction and Study Selection
2.4. Investigations of Heterogeneity
- 0% to 40%: might not be important;
- 30% to 60%: may represent moderate heterogeneity;
- 50% to 90%: may represent substantial heterogeneity;
- 75% to 100%: considerable heterogeneity.
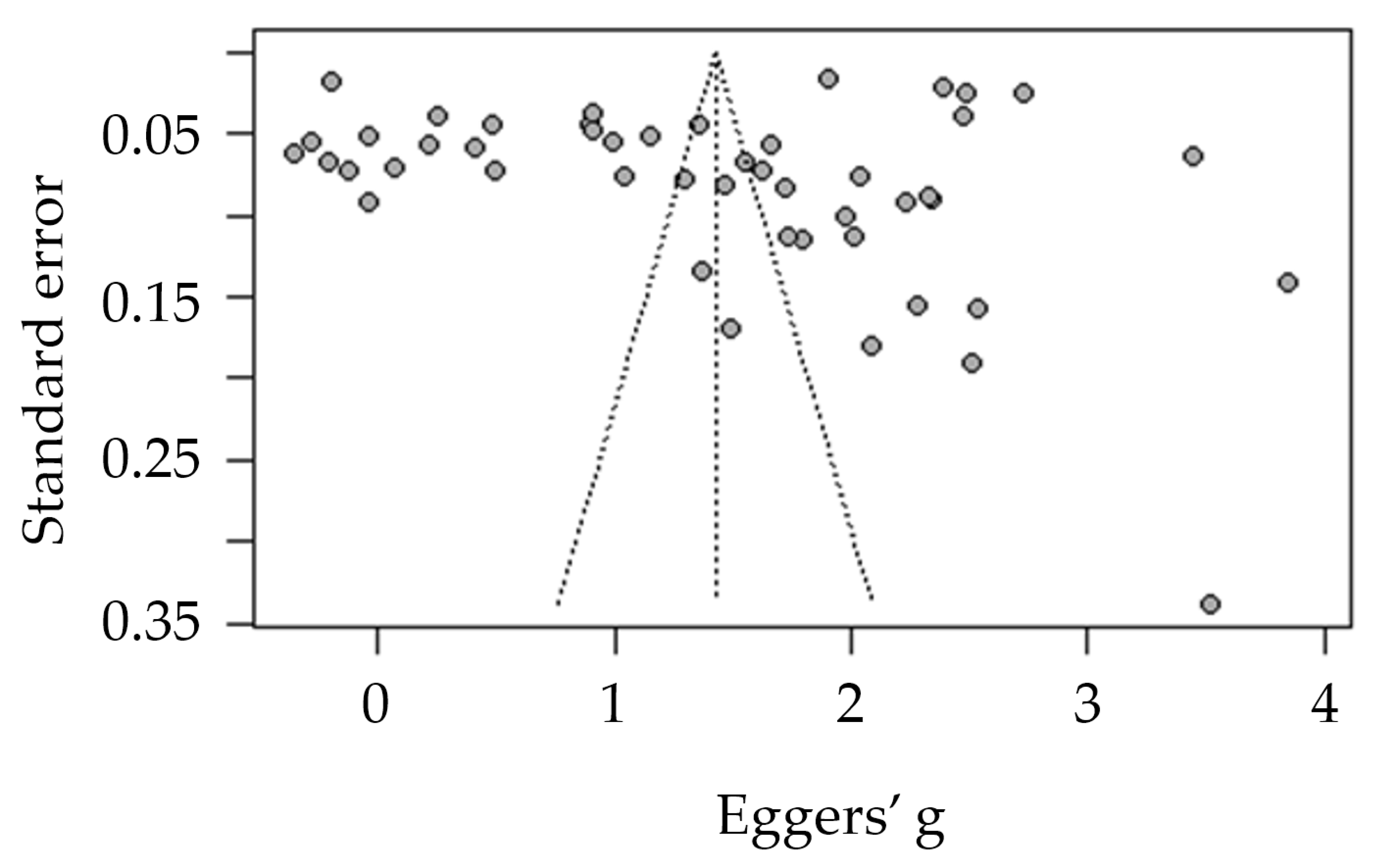
2.5. Publication Bias
2.6. Quality Assessment
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Risk of Publication Bias
3.3. Proportion of COVID-19 Acceptance
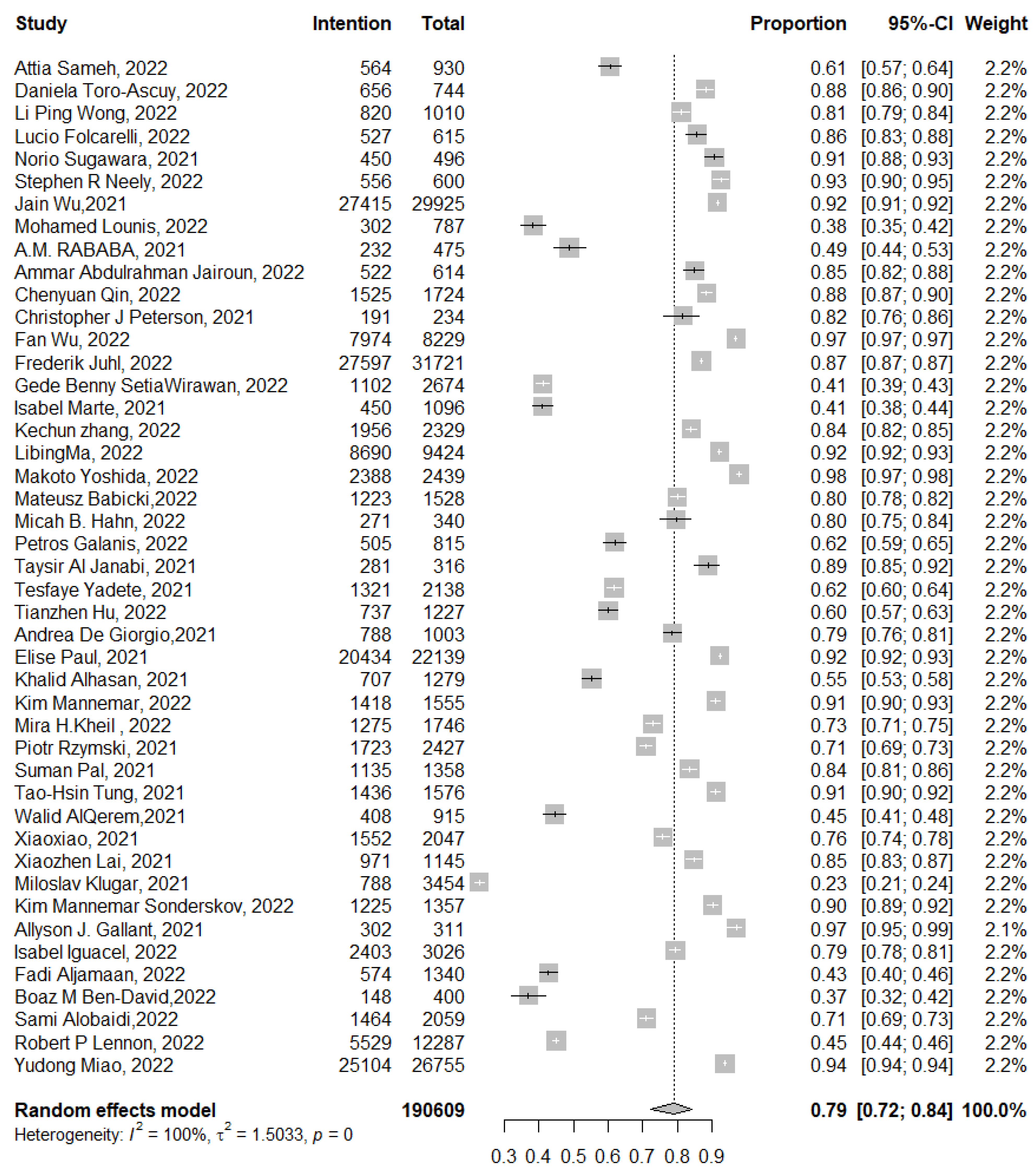
3.3.1. Actual and Intentional Acceptance of COVID-19 Booster Dose Vaccination
3.3.2. Actual Uptake of COVID-19 Vaccine Booster Dose
3.3.3. Intentional Acceptance of COVID-19 Vaccine Booster Dose
3.4. COVID-19 Booster Dose Vaccine Acceptance among HCWs
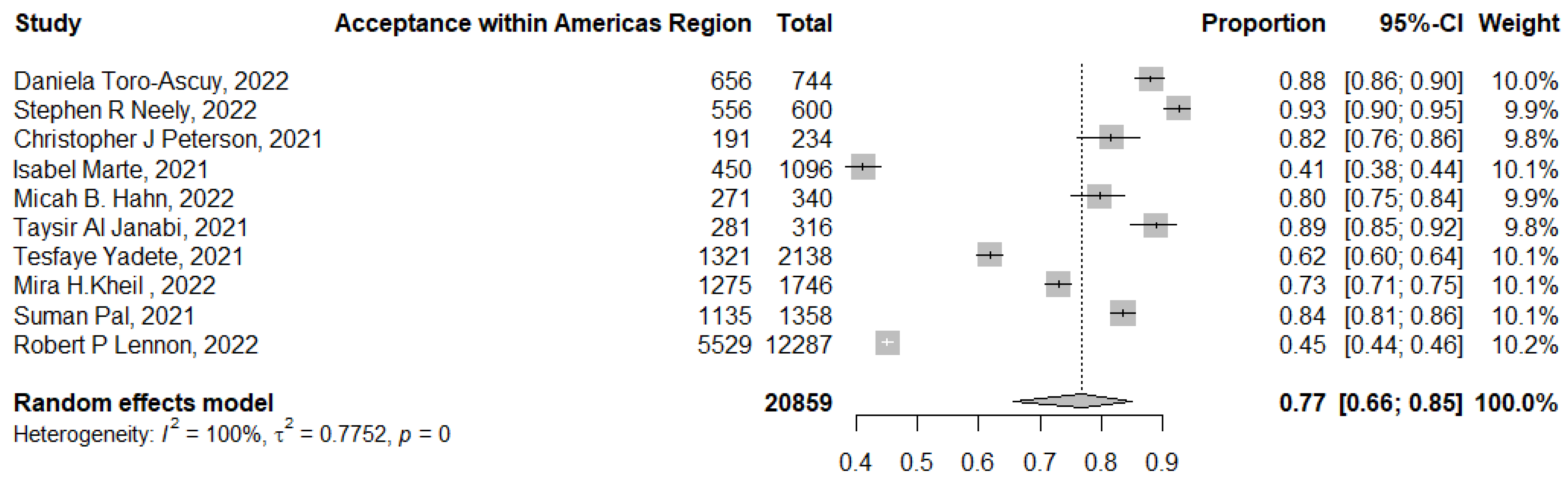
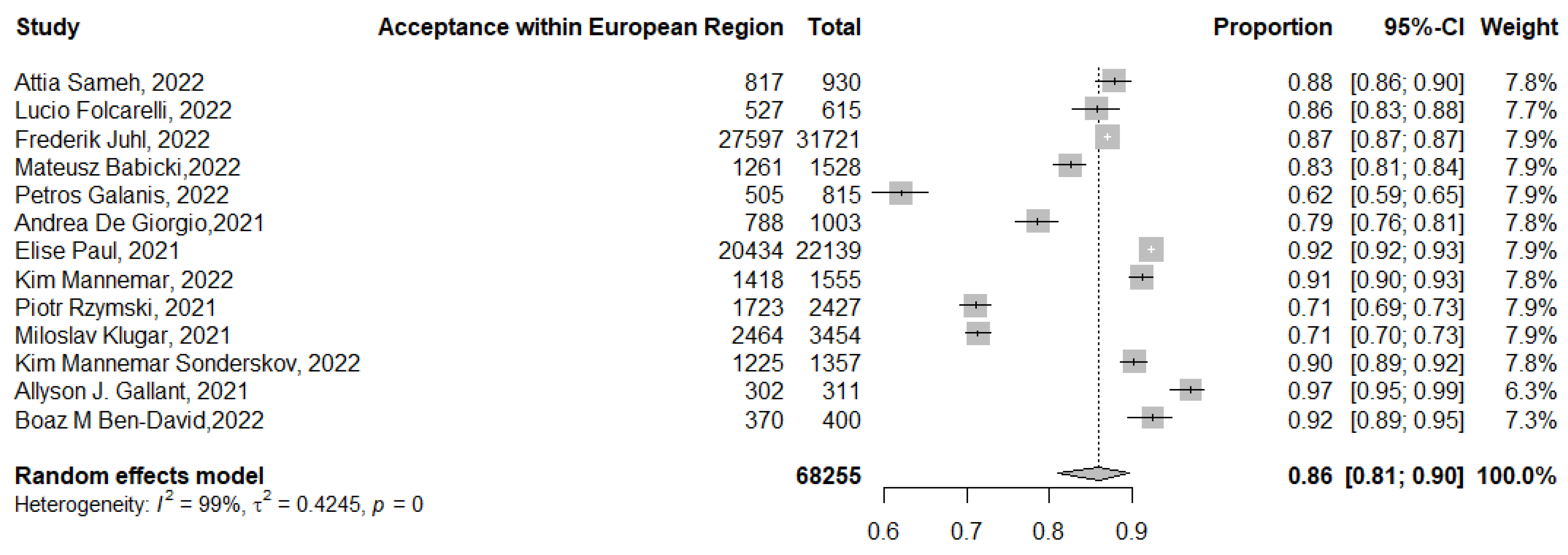
3.5. Acceptance of COVID-19 Booster Dose Vaccination across the WHO Regions
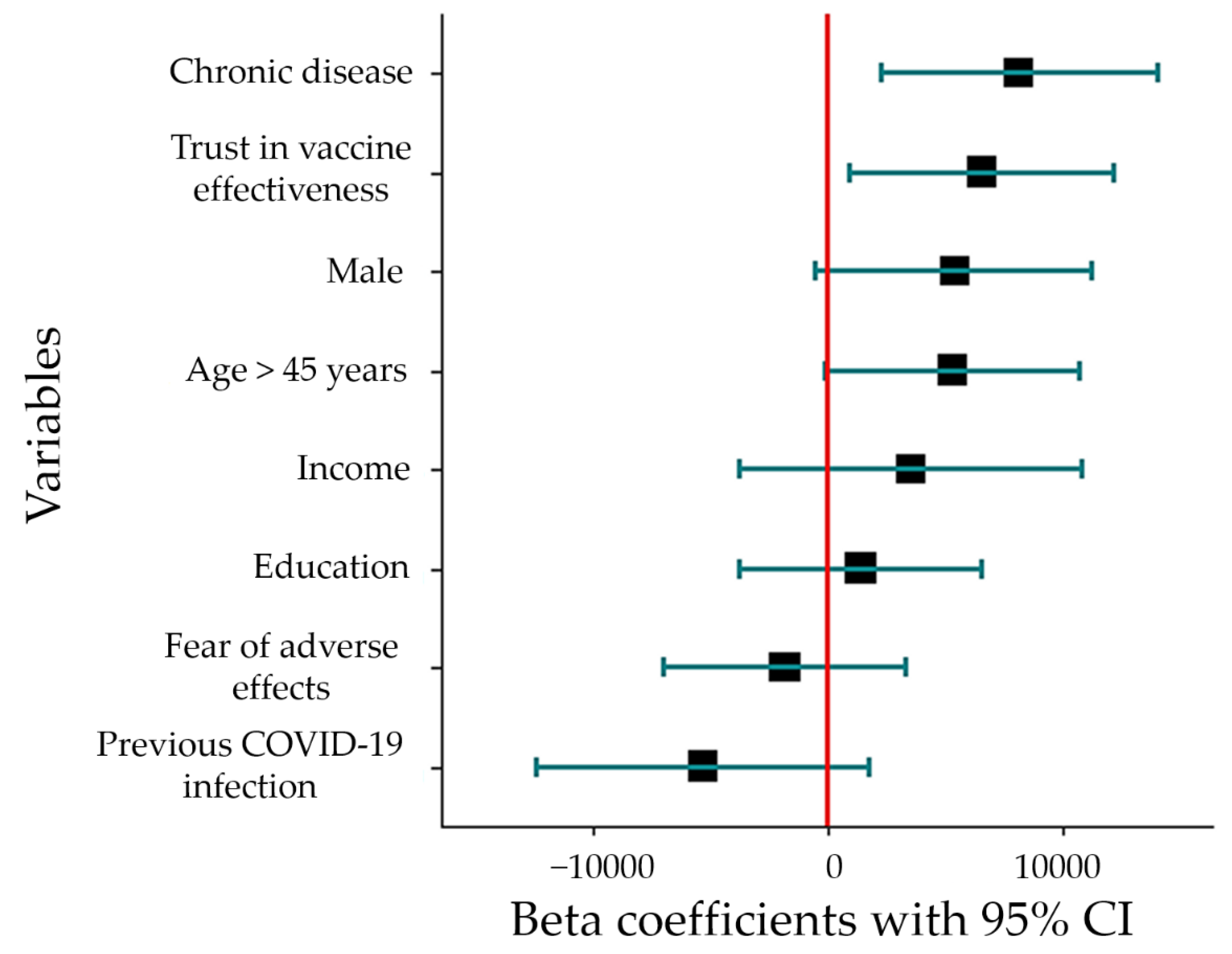
3.6. Predictors of COVID-19 Booster Dose Acceptance
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | confidence interval |
| COVID-19 | coronavirus disease 2019 |
| DOI | digital object identifier |
| EUL | emergency use listing |
| HCWs | healthcare workers |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| QA | quality assessment |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| VIF | variance inflation factor |
| WHO | World Health Organization |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Phillips, N. The coronavirus is here to stay—Here’s what that means. Nature 2021, 590, 382–384. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 September 2022).
- Asem, N.; Ramadan, A.; Hassany, M.; Ghazy, R.M.; Abdallah, M.; Ibrahim, M.; Gamal, E.M.; Hassan, S.; Kamal, N.; Zaid, H. Pattern and determinants of COVID-19 infection and mortality across countries: An ecological study. Heliyon 2021, 7, e07504. [Google Scholar] [CrossRef] [PubMed]
- Karmakar, M.; Lantz, P.M.; Tipirneni, R. Association of Social and Demographic Factors With COVID-19 Incidence and Death Rates in the US. JAMA Netw. Open 2021, 4, e2036462. [Google Scholar] [CrossRef]
- Nature News. COVID research: A year of scientific milestones. Nature, 2021; ahead of print. [Google Scholar] [CrossRef]
- World Health Organization. WHO COVID-19 Vaccine Tracker and Landscape. Available online: https://covid19.trackvaccines.org/ (accessed on 8 September 2022).
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A Global Map of COVID-19 Vaccine Acceptance Rates per Country: An Updated Concise Narrative Review. J. Multidiscip Health 2022, 15, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 Vaccine Hesitancy-A Scoping Review of Literature in High-Income Countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Saad-Roy, C.M.; Morris, S.E.; Metcalf, C.J.E.; Mina, M.J.; Baker, R.E.; Farrar, J.; Holmes, E.C.; Pybus, O.G.; Graham, A.L.; Levin, S.A.; et al. Epidemiological and evolutionary considerations of SARS-CoV-2 vaccine dosing regimes. Science 2021, 372, 363–370. [Google Scholar] [CrossRef]
- Andeweg, S.P.; de Gier, B.; Eggink, D.; van den Ende, C.; van Maarseveen, N.; Ali, L.; Vlaemynck, B.; Schepers, R.; Hahné, S.J.M.; Reusken, C.B.E.M.; et al. Protection of COVID-19 vaccination and previous infection against Omicron BA.1, BA.2 and Delta SARS-CoV-2 infections. Nat. Commun. 2022, 13, 4738. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Interim Statement on Booster Doses for COVID-19 Vaccination. Available online: https://www.who.int/news/item/04-10-2021-interim-statement-on-booster-doses-for-covid-19-vaccination (accessed on 8 September 2022).
- Tseng, H.F.; Ackerson, B.K.; Luo, Y.; Sy, L.S.; Talarico, C.A.; Tian, Y.; Bruxvoort, K.J.; Tubert, J.E.; Florea, A.; Ku, J.H.; et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat. Med. 2022, 28, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Choi, A.; Koch, M.; Wu, K.; Chu, L.; Ma, L.; Hill, A.; Nunna, N.; Huang, W.; Oestreicher, J.; Colpitts, T.; et al. Safety and immunogenicity of SARS-CoV-2 variant mRNA vaccine boosters in healthy adults: An interim analysis. Nat. Med. 2021, 27, 2025–2031. [Google Scholar] [CrossRef] [PubMed]
- Yue, L.; Xie, T.; Yang, T.; Zhou, J.; Chen, H.; Zhu, H.; Li, H.; Xiang, H.; Wang, J.; Yang, H.; et al. A third booster dose may be necessary to mitigate neutralizing antibody fading after inoculation with two doses of an inactivated SARS-CoV-2 vaccine. J. Med. Virol. 2022, 94, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef]
- World Health Organization. Interim Recommendations for Use of the Pfizer–BioNTech COVID-19 Vaccine, BNT162b2, under Emergency Use Listing. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-BNT162b2-2021.1 (accessed on 8 September 2022).
- World Health Organization. WHO Dashboard Officially Reporting COVID-19 Vaccination Data. Available online: https://app.powerbi.com/view?r=eyJrIjoiMWNjNzZkNjctZTNiNy00YmMzLTkxZjQtNmJiZDM2MTYxNzEwIiwidCI6ImY2MTBjMGI3LWJkMjQtNGIzOS04MTBiLTNkYzI4MGFmYjU5MCIsImMiOjh9 (accessed on 8 September 2022).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of Vaccination Readiness. Eur. J. Psychol. Assess. 2022, 38, 261–269. [Google Scholar] [CrossRef]
- Yadete, T.; Batra, K.; Netski, D.M.; Antonio, S.; Patros, M.J.; Bester, J.C. Assessing Acceptability of COVID-19 Vaccine Booster Dose among Adult Americans: A Cross-Sectional Study. Vaccines 2021, 9, 1424. [Google Scholar] [CrossRef] [PubMed]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Acceptance of a Third Dose of COVID-19 Vaccine and Associated Factors in China Based on Health Belief Model: A National Cross-Sectional Study. Vaccines 2022, 10, 89. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. Predictors of Willingness of the General Public to Receive a Second COVID-19 Booster Dose or a New COVID-19 Vaccine: A Cross-Sectional Study in Greece. Vaccines 2022, 10, 1061. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; John Wiley & Sons: Hoboken, NJ, USA, 2022. [Google Scholar]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Hafez, D.; Abdulmoneim, S.; Hamdy, N.; Nour El-Deen, A.; Ghazy, R.; Elrewany, E.; Osman, A.; Attia, M. COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis. PROSPERO 2022 CRD42022333758. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022333758 (accessed on 9 September 2022).
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp (accessed on 22 August 2022).
- Moskalewicz, A.; Oremus, M. No clear choice between Newcastle-Ottawa Scale and Appraisal Tool for Cross-Sectional Studies to assess methodological quality in cross-sectional studies of health-related quality of life and breast cancer. J. Clin. Epidemiol. 2020, 120, 94–103. [Google Scholar] [CrossRef]
- Mori, Y.; Miyatake, N.; Suzuki, H.; Mori, Y.; Okada, S.; Tanimoto, K. Pre-Impressions of the Third COVID-19 Vaccination among Medical Staff: A Text Mining-Based Survey. Vaccines 2022, 10, 856. [Google Scholar] [CrossRef]
- Al Janabi, T.; Pino, M. To Boost or Not to Boost: Acceptability of a COVID-19 Booster Dose among Osteopathic Medical Students: A Cross-Sectional Study from a Medical School in New York. Epidemiologia 2022, 3, 218–228. [Google Scholar] [CrossRef]
- Iguacel, I.; Álvarez-Najar, J.P.; Vásquez, P.D.C.; Alarcón, J.; Orte, M.; Samatán, E.; Martínez-Jarreta, B. Citizen Stance towards Mandatory COVID-19 Vaccination and Vaccine Booster Doses: A Study in Colombia, El Salvador and Spain. Vaccines 2022, 10, 781. [Google Scholar] [CrossRef]
- Gallant, A.J.; Nicholls, L.A.B.; Rasmussen, S.; Cogan, N.; Young, D.; Williams, L. Changes in attitudes to vaccination as a result of the COVID-19 pandemic: A longitudinal study of older adults in the UK. PLoS ONE 2021, 16, e0261844. [Google Scholar] [CrossRef]
- Sønderskov, K.M.; Vistisen, H.T.; Dinesen, P.T.; Østergaard, S.D. COVID-19 booster vaccine willingness. Dan. Med. J. 2021, 69, A10210765. [Google Scholar] [PubMed]
- Wu, J.; Li, Q.; Silver Tarimo, C.; Wang, M.; Gu, J.; Wei, W.; Ma, M.; Zhao, L.; Mu, Z.; Miao, Y. COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study. Front. Immunol. 2021, 12, 781161. [Google Scholar] [CrossRef] [PubMed]
- Hahn, M.B.; Fried, R.L.; Cochran, P.; Eichelberger, L.P. Evolving perceptions of COVID-19 vaccines among remote Alaskan communities. Int. J. Circumpolar. Health 2022, 81, 2021684. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Kobashi, Y.; Kawamura, T.; Shimazu, Y.; Nishikawa, Y.; Omata, F.; Zhao, T.; Yamamoto, C.; Kaneko, Y.; Nakayama, A.; et al. Factors Associated with COVID-19 Vaccine Booster Hesitancy: A Retrospective Cohort Study, Fukushima Vaccination Community Survey. Vaccines 2022, 10, 515. [Google Scholar] [CrossRef] [PubMed]
- Motta, M. The Prevalence and Correlates of Prospective Vaccine Hesitancy Among Individuals who Received COVID-19 Vaccine Boosters. SocArXiv 2022. [Google Scholar] [CrossRef]
- Peterson, C.J.; Abohelwa, M.; Payne, D.; Mohamed, A.A.; Nugent, K. 2019 Novel Coronavirus Vaccination Among Medical Students. J. Prim. Care Community Health 2021, 12, 21501327211058316. [Google Scholar] [CrossRef]
- Sønderskov, K.M.; Vistisen, H.T.; Dinesen, P.T.; Østergaard, S.D. A positive update on COVID-19 booster vaccine willingness among Danes. Dan. Med. J. 2022, 69, A01220047. [Google Scholar] [PubMed]
- Wu, F.; Yuan, Y.; Deng, Z.; Yin, D.; Shen, Q.; Zeng, J.; Xie, Y.; Xu, M.; Yang, M.; Jiang, S.; et al. Acceptance of COVID-19 booster vaccination based on the protection motivation theory: A cross-sectional study in China. J. Med. Virol. 2022, 94, 4115–4124. [Google Scholar] [CrossRef]
- Marte, M.I.; Pichardo, E.; Kandany, V.N.; Castillo, M.M. Acceptance towards COVID-19 vaccine: A cross-sectional study in the Dominican Republic. Princ. Pract. Clin. Res. 2021, 7, 58–64. [Google Scholar] [CrossRef]
- Al-Qerem, W.; Al Bawab, A.Q.; Hammad, A.; Ling, J.; Alasmari, F. Willingness of the Jordanian Population to Receive a COVID-19 Booster Dose: A Cross-Sectional Study. Vaccines 2022, 10, 410. [Google Scholar] [CrossRef]
- Hu, T.; Li, L.; Lin, C.; Yang, Z.; Chow, C.; Lu, Z.; You, C. An Analysis of the Willingness to the COVID-19 Vaccine Booster Shots among Urban Employees: Evidence from a Megacity H in Eastern China. Int. J. Environ. Res. Public Health 2022, 19, 2300. [Google Scholar] [CrossRef] [PubMed]
- Jairoun, A.A.; Al-Hemyari, S.S.; El-Dahiyat, F.; Jairoun, M.; Shahwan, M.; Al Ani, M.; Habeb, M.; Babar, Z.U. Assessing public knowledge, attitudes and determinants of third COVID-19 vaccine booster dose acceptance: Current scenario and future perspectives. J. Pharm. Policy Pract. 2022, 15, 26. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Wang, R.; Tao, L.; Liu, M.; Liu, J. Association Between Risk Perception and Acceptance for a Booster Dose of COVID-19 Vaccine to Children Among Child Caregivers in China. Front. Public Health 2022, 10, 834572. [Google Scholar] [CrossRef] [PubMed]
- Babicki, M.; Mastalerz-Migas, A. Attitudes of Poles towards the COVID-19 Vaccine Booster Dose: An Online Survey in Poland. Vaccines 2022, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Fang, Y.; Chan, P.S.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Behavioral Intention to Get a Booster Dose of COVID-19 Vaccine among Chinese Factory Workers. Int. J. Environ. Res. Public Health 2022, 19, 5245. [Google Scholar] [CrossRef] [PubMed]
- Alhasan, K.; Aljamaan, F.; Temsah, M.H.; Alshahrani, F.; Bassrawi, R.; Alhaboob, A.; Assiri, R.; Alenezi, S.; Alaraj, A.; Alhomoudi, R.I.; et al. COVID-19 Delta Variant: Perceptions, Worries, and Vaccine-Booster Acceptability among Healthcare Workers. Healthcare 2021, 9, 1566. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Bencherit, D.; Rais, M.A.; Riad, A. COVID-19 Vaccine Booster Hesitancy (VBH) and Its Drivers in Algeria: National Cross-Sectional Survey-Based Study. Vaccines 2022, 10, 621. [Google Scholar] [CrossRef]
- Klugar, M.; Riad, A.; Mohanan, L.; Pokorná, A. COVID-19 Vaccine Booster Hesitancy (VBH) of Healthcare Workers in Czechia: National Cross-Sectional Study. Vaccines 2021, 9, 1437. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.W.C.; Liow, Y.; Loh, V.W.K.; Liew, S.J.; Chan, Y.-H.; Young, D. COVID-19 vaccine acceptance and hesitancy among primary healthcare workers in Singapore. BMC Prim. Care 2022, 23, 81. [Google Scholar] [CrossRef]
- Kheil, M.H.; Jain, D.; Jomaa, J.; Askar, B.; Alcodray, Y.; Wahbi, S.; Brikho, S.; Kadouh, A.; Harajli, D.; Jawad, Z.N.; et al. COVID-19 Vaccine Hesitancy among Arab Americans. Vaccines 2022, 10, 610. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef]
- Toro-Ascuy, D.; Cifuentes-Muñoz, N.; Avaria, A.; Pereira-Montecinos, C.; Cruzat, G.; Peralta-Arancibia, K.; Zorondo-Rodríguez, F.; Fuenzalida, L.F. Factors Influencing the Acceptance of COVID-19 Vaccines in a Country with a High Vaccination Rate. Vaccines 2022, 10, 681. [Google Scholar] [CrossRef] [PubMed]
- Folcarelli, L.; Miraglia del Giudice, G.; Corea, F.; Angelillo, I.F. Intention to Receive the COVID-19 Vaccine Booster Dose in a University Community in Italy. Vaccines 2022, 10, 146. [Google Scholar] [CrossRef] [PubMed]
- Wirawan, G.B.S.; Harjana, N.P.A.; Nugrahani, N.W.; Januraga, P.P. Health Beliefs and Socioeconomic Determinants of COVID-19 Booster Vaccine Acceptance: An Indonesian Cross-Sectional Study. Vaccines 2022, 10, 724. [Google Scholar] [CrossRef] [PubMed]
- Aljamaan, F.; Alhaboob, A.; Saddik, B.; Bassrawi, R.; Assiri, R.; Saeed, E.; Alhasan, K.; Alenezi, S.; Alarabi, M.; Alrabiaah, A.; et al. In-Person Schooling Amidst Children’s COVID-19 Vaccination: Exploring Parental Perceptions Just after Omicron Variant Announcement. Vaccines 2022, 10, 768. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Siaw, Y.L.; Muslimin, M.; Lai, L.L.; Lin, Y.; Hu, Z. Intention to receive a COVID-19 vaccine booster dose and associated factors in Malaysia. Hum. Vaccin. Immunother. 2022, 18, 2078634. [Google Scholar] [CrossRef]
- Rababa’h, A.M.; Abedalqader, N.N.; Ababneh, M. Jordanians’ willingness to receive heterologous prime-boost COVID-19 vaccination and vaccine boosters. Eur. Rev. Med. Pharm. Sci. 2021, 25, 7516–7525. [Google Scholar] [CrossRef]
- Paul, E.; Fancourt, D. Predictors of uncertainty and unwillingness to receive the COVID-19 booster vaccine: An observational study of 22,139 fully vaccinated adults in the UK. Lancet Reg. Health Eur. 2022, 14, 100317. [Google Scholar] [CrossRef]
- Attia, S.; Mausbach, K.; Klugar, M.; Howaldt, H.P.; Riad, A. Prevalence and Drivers of COVID-19 Vaccine Booster Hesitancy Among German University Students and Employees. Front. Public Health 2022, 10, 846861. [Google Scholar] [CrossRef]
- Lai, X.; Zhu, H.; Wang, J.; Huang, Y.; Jing, R.; Lyu, Y.; Zhang, H.; Feng, H.; Guo, J.; Fang, H. Public Perceptions and Acceptance of COVID-19 Booster Vaccination in China: A Cross-Sectional Study. Vaccines 2021, 9, 1461. [Google Scholar] [CrossRef]
- Neely, S.R.; Scacco, J.M. Receptiveness of American adults to COVID-19 vaccine boosters: A survey analysis. PEC Innov. 2022, 1, 100019. [Google Scholar] [CrossRef]
- Miao, Y.; Li, Y.; Zhang, W.; Wu, J.; Gu, J.; Wang, M.; Wei, W.; Ye, B.; Miao, C.; Tarimo, C.S.; et al. The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5464. [Google Scholar] [CrossRef] [PubMed]
- Kunno, J.; Supawattanabodee, B.; Sumanasrethakul, C.; Kaewchandee, C.; Wanichnopparat, W.; Prasittichok, K. The Relationship between Attitudes and Satisfaction Concerning the COVID-19 Vaccine and Vaccine Boosters in Urban Bangkok, Thailand: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5086. [Google Scholar] [CrossRef] [PubMed]
- Al Janabi, T.; Pino, M. Predictors for Actual COVID-19 Vaccine Uptake and Intended Booster Dosage among Medical Students of an Osteopathic Medical School in New York. Epidemiologia 2021, 2, 553–563. [Google Scholar] [CrossRef]
- Lennon, R.P.; Block, R., Jr.; Schneider, E.C.; Zephrin, L.; Shah, A. Underserved population acceptance of combination influenza-COVID-19 booster vaccines. Vaccine 2022, 40, 562–567. [Google Scholar] [CrossRef]
- Ben-David, B.M.; Keisari, S.; Palgi, Y. Vaccine and Psychological Booster: Factors Associated With Older Adults’ Compliance to the Booster COVID-19 Vaccine in Israel. J. Appl. Gerontol. 2022, 41, 1636–1640. [Google Scholar] [CrossRef] [PubMed]
- Xiaoxiao, W.; Leyuan, L.; Minyue, P.; Xiaoguang, L.; Nan, L. Willingness of the General Public to Receive A COVID-19 Vaccine Booster—China, April–May 2021. China CDC Wkly. 2022, 4, 66–70. [Google Scholar] [CrossRef]
- Tung, T.H.; Lin, X.Q.; Chen, Y.; Zhang, M.X.; Zhu, J.S. Willingness to receive a booster dose of inactivated coronavirus disease 2019 vaccine in Taizhou, China. Expert Rev. Vaccines 2022, 21, 261–267. [Google Scholar] [CrossRef]
- De Giorgio, A.; Kuvačić, G.; Maleš, D.; Vecchio, I.; Tornali, C.; Ishac, W.; Ramaci, T.; Barattucci, M.; Milavić, B. Willingness to Receive COVID-19 Booster Vaccine: Associations between Green-Pass, Social Media Information, Anti-Vax Beliefs, and Emotional Balance. Vaccines 2022, 10, 481. [Google Scholar] [CrossRef]
- Rzymski, P.; Pazgan-Simon, M.; Kamerys, J.; Moniuszko-Malinowska, A.; Sikorska, K.; Wernik, J.; Zarębska-Michaluk, D.; Supronowicz, Ł.; Sobala-Szczygieł, B.; Skrzat-Klapaczyńska, A.; et al. Severe Breakthrough COVID-19 Cases during Six Months of Delta Variant (B.1.617.2) Domination in Poland. Vaccines 2022, 10, 557. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, F.J.; Nielsen, L.H.; Petersen, M.B. Willingness to Take the Booster Vaccine in a Nationally Representative Sample of Danes. Vaccines 2022, 10, 425. [Google Scholar] [CrossRef]
- Ma, L.; Yang, J.; Zhang, T.; Han, X.; Huang, Q.; Yang, Y.; Feng, L.; Yang, W.; Wang, C. Willingness toward COVID-19 vaccination, coadministration with other vaccines and receive a COVID-19 vaccine booster: A cross-sectional study on the guardians of children in China. Hum. Vaccin. Immunother. 2022, 18, 2049169. [Google Scholar] [CrossRef]
- Sugawara, N.; Yasui-Furukori, N.; Fukushima, A.; Shimoda, K. Attitudes of Medical Students toward COVID-19 Vaccination: Who Is Willing to Receive a Third Dose of the Vaccine? Vaccines 2021, 9, 1295. [Google Scholar] [CrossRef] [PubMed]
- Alobaidi, S.; Hashim, A. Predictors of the Third (Booster) Dose of COVID-19 Vaccine Intention among the Healthcare Workers in Saudi Arabia: An Online Cross-Sectional Survey. Vaccines 2022, 10, 987. [Google Scholar] [CrossRef] [PubMed]
- Britton, T.; Ball, F.; Trapman, P. A mathematical model reveals the influence of population heterogeneity on herd immunity to SARS-CoV-2. Science 2020, 369, 846–849. [Google Scholar] [CrossRef] [PubMed]
- Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Alqutub, S.T.; Esmail, O.F.; Abdou, M.S.M.; Reyad, O.A.; El-Ganainy, S.O.; Gad, B.K.; Nour El-Deen, A.E.; et al. A Meta-Analysis on the Safety and Immunogenicity of Covid-19 Vaccines. J. Prim. Care Community Health 2022, 13, 21501319221089255. [Google Scholar] [CrossRef] [PubMed]
- Ghazy, R.M.; Ashmawy, R.; Hamdy, N.A.; Elhadi, Y.A.M.; Reyad, O.A.; Elmalawany, D.; Almaghraby, A.; Shaaban, R.; Taha, S.H.N. Efficacy and Effectiveness of SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 350. [Google Scholar] [CrossRef]
- Fajar, J.K.; Sallam, M.; Soegiarto, G.; Sugiri, Y.J.; Anshory, M.; Wulandari, L.; Kosasih, S.A.P.; Ilmawan, M.; Kusnaeni, K.; Fikri, M.; et al. Global Prevalence and Potential Influencing Factors of COVID-19 Vaccination Hesitancy: A Meta-Analysis. Vaccines 2022, 10, 1356. [Google Scholar] [CrossRef] [PubMed]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Al-Sanafi, M.; Sallam, M. Psychological Determinants of COVID-19 Vaccine Acceptance among Healthcare Workers in Kuwait: A Cross-Sectional Study Using the 5C and Vaccine Conspiracy Beliefs Scales. Vaccines 2021, 9, 701. [Google Scholar] [CrossRef] [PubMed]
- Wald, A. Booster Vaccination to Reduce SARS-CoV-2 Transmission and Infection. JAMA 2022, 327, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Canaday, D.H.; Oyebanji, O.A.; White, E.; Keresztesy, D.; Payne, M.; Wilk, D.; Carias, L.; Aung, H.; St Denis, K.; Sheehan, M.L.; et al. COVID-19 vaccine booster dose needed to achieve Omicron-specific neutralisation in nursing home residents. eBioMedicine 2022, 80, 104066. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef]
- Pérez-Alós, L.; Armenteros, J.J.A.; Madsen, J.R.; Hansen, C.B.; Jarlhelt, I.; Hamm, S.R.; Heftdal, L.D.; Pries-Heje, M.M.; Møller, D.L.; Fogh, K.; et al. Modeling of waning immunity after SARS-CoV-2 vaccination and influencing factors. Nat. Commun. 2022, 13, 1614. [Google Scholar] [CrossRef]
- Norhayati, M.N.; Che Yusof, R.; Azman, Y.M. Systematic Review and Meta-Analysis of COVID-19 Vaccination Acceptance. Front. Med. 2022, 8, 783982. [Google Scholar] [CrossRef]
- Wang, Q.; Hu, S.; Du, F.; Zang, S.; Xing, Y.; Qu, Z.; Zhang, X.; Lin, L.; Hou, Z. Mapping global acceptance and uptake of COVID-19 vaccination: A systematic review and meta-analysis. Commun. Med. 2022, 2, 113. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, e2021726118. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of healthcare workers to accept COVID-19 vaccination and related factors: A systematic review and meta-analysis. Asian Pac. J. Trop. Med. 2021, 14, 543–554. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Yamey, G.; Garcia, P.; Hassan, F.; Mao, W.; McDade, K.K.; Pai, M.; Saha, S.; Schellekens, P.; Taylor, A.; Udayakumar, K. It is not too late to achieve global covid-19 vaccine equity. BMJ 2022, 376, e070650. [Google Scholar] [CrossRef]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Ye, Y.; Zhang, Q.; Wei, X.; Cao, Z.; Yuan, H.-Y.; Zeng, D.D. Equitable access to COVID-19 vaccines makes a life-saving difference to all countries. Nat. Hum. Behav. 2022, 6, 207–216. [Google Scholar] [CrossRef]
- Machado, B.A.S.; Hodel, K.V.S.; Fonseca, L.M.d.S.; Pires, V.C.; Mascarenhas, L.A.B.; da Silva Andrade, L.P.C.; Moret, M.A.; Badaró, R. The Importance of Vaccination in the Context of the COVID-19 Pandemic: A Brief Update Regarding the Use of Vaccines. Vaccines 2022, 10, 591. [Google Scholar] [CrossRef]
- Bongers, A.; Riggall, G.; Kokareva, L.; Chin, B. Managing the challenges associated with decreasing demand for COVID-19 vaccination in Central and West Asia. BMJ Glob. Health 2022, 7, e010066. [Google Scholar] [CrossRef]
- Obinna, D.N. Solidarity across borders: A pragmatic need for global COVID-19 vaccine equity. Int. J. Health Plann. Manag. 2022, 37, 21–29. [Google Scholar] [CrossRef]
- Chen, X.; Lee, W.; Lin, F. Infodemic, Institutional Trust, and COVID-19 Vaccine Hesitancy: A Cross-National Survey. Int. J. Environ. Res. Public Health 2022, 19, 8033. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Abdou, M.S.; Awaidy, S.; Sallam, M.; Elbarazi, I.; Youssef, N.; Fiidow, O.A.; Mehdad, S.; Hussein, M.F.; Adam, M.F.; et al. Acceptance of COVID-19 Vaccine Booster Doses Using the Health Belief Model: A Cross-Sectional Study in Low-Middle- and High-Income Countries of the East Mediterranean Region. Int. J. Environ. Res. Public Health 2022, 19, 12136. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. First COVID-19 Booster Dose in the General Population: A Systematic Review and Meta-Analysis of Willingness and Its Predictors. Vaccines 2022, 10, 1097. [Google Scholar] [CrossRef] [PubMed]
- Dziedzic, A.; Issa, J.; Hussain, S.; Tanasiewicz, M.; Wojtyczka, R.; Kubina, R.; Konwinska, M.D.; Riad, A. COVID-19 vaccine booster hesitancy (VBH) of healthcare professionals and students in Poland: Cross-sectional survey-based study. Front. Public Health 2022, 10, 938067. [Google Scholar] [CrossRef]
- Aw, J.; Seah, S.S.Y.; Seng, B.J.J.; Low, L.L. COVID-19-Related Vaccine Hesitancy among Community Hospitals’ Healthcare Workers in Singapore. Vaccines 2022, 10, 537. [Google Scholar] [CrossRef]
- Gu, M.; Taylor, B.; Pollack, H.A.; Schneider, J.A.; Zaller, N. A pilot study on COVID-19 vaccine hesitancy among healthcare workers in the US. PLoS ONE 2022, 17, e0269320. [Google Scholar] [CrossRef]
- Al-Jayyousi, G.F.; Sherbash, M.A.M.; Ali, L.A.M.; El-Heneidy, A.; Alhussaini, N.W.Z.; Elhassan, M.E.A.; Nazzal, M.A. Factors Influencing Public Attitudes towards COVID-19 Vaccination: A Scoping Review Informed by the Socio-Ecological Model. Vaccines 2021, 9, 548. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Al-Tammemi, A.a.B.; Alkurtas, M.; Mirzaei, F.; Kareem, N.; Al-Naimat, H.; Jardaneh, L.; Al-Majali, L.; AlHadidi, A.; et al. Assessing Healthcare Workers’ Knowledge and Their Confidence in the Diagnosis and Management of Human Monkeypox: A Cross-Sectional Study in a Middle Eastern Country. Healthcare 2022, 10, 1722. [Google Scholar] [CrossRef]
- Antonini, M.; Eid, M.A.; Falkenbach, M.; Rosenbluth, S.T.; Prieto, P.A.; Brammli-Greenberg, S.; McMeekin, P.; Paolucci, F. An analysis of the COVID-19 vaccination campaigns in France, Israel, Italy and Spain and their impact on health and economic outcomes. Health Policy Technol. 2022, 11, 100594. [Google Scholar] [CrossRef]
- Atkinson, C.L.; Atkinson, A.M. Vaccine Hesitancy and Administrative Burden in the Australian National Immunisation Program: An Analysis of Twitter Discourse. Knowledge 2021, 1, 25–39. [Google Scholar] [CrossRef]
- Motta, M.; Sylvester, S.; Callaghan, T.; Lunz-Trujillo, K. Encouraging COVID-19 Vaccine Uptake Through Effective Health Communication. Front. Polit. Sci. 2021, 3, 630133. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol 2022, 94, 2969–2976. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Country | Design, Inclusion/Exclusion Criteria | Sample Size (n), Female (%), Age | Study Period | Previous COVID-19 (n) | Education/Employment | COVID-19 Vaccine Coverage (%) | Vaccine Type |
|---|---|---|---|---|---|---|---|
| Petersonet et al., USA [43] | Cross-sectional, medical students | 234, 63%, NA | 13 July 2021–3 August 2021 | 31 | Medical students | Fully vaccinated (99.3) | Moderna and Pfizer |
| Sønderskov et al., Denmark [44] | Cross-sectional, those who received or were scheduled to receive vaccine and did not receive the booster dose were included; those who did not receive COVID-19 vaccine at all or received a booster dose were excluded | 1357, NA, NA | 10 December 2021–23 December 2021 | NA | NA | Fully vaccinated (95.0) | Moderna and Pfizer |
| Wu et al., China [45] | Cross-sectional, individuals who are at least 18 years old and were able to read and complete the self-administered questionnaire independently were included | 8229, 69%, 79% aged 26–45 years | 24 October 2021–28 October 2021 | 24 | Junior high school or below (33%), high school (29%), bachelor (36%), master, or above (2%). Employment as HCW (3%), other (98%) | Fully vaccinated (100) | NA |
| Marte et al., Dominican Republic [46] | Cross-sectional, all permanent residents over 18 years of age | 1096, 60%, mean age: 37 years | July 2021 | 276 | Bachelor (32%), master (28%), doctorate (21%), PhD (2%), technicians (7%), high school (11%), elementary school (0.3%); employment: public, private sector, or independently employed (85%), unemployed (15%) | Fully vaccinated (81.9) | Sinovac (68%), AstraZeneca (20%), Pfizer (4%), others (8%) |
| Al-Qerem et al., Jordan [47] | Cross-sectional, people aged 18 or above, living in Jordan, and fully vaccinated | 915, NA, 46% were 18–29 years | 1 October 2021–15 December 2021 | NA | High school or less (7%), diploma (5%), university student (18%), bachelor (64%), postgraduates (6%) | Fully vaccinated (100) | Pfizer (57%), AstraZeneca (5%), Sinopharm (38%) |
| Hu et al., China [48] | Cross-sectional, NA 2 | 1227, 49%, 75% were 18–39 years | 20 October 2021–10 December 2021 | NA | Bachelor’s degree (53%), postgraduate and above (32%); employment: civil servants (12%), staff in government-affiliated public institutions (14%), enterprise employees (56%), doctors (2%) | Fully vaccinated (100) | NA |
| Yadete et al., USA [25] | Cross-sectional, NA | 2138, 50%, NA | 14 July 2021–19 July 2021 | NA | NA | NA | NA |
| Jairoun et al., UAE [49] | Cross-sectional, students and faculty staff of Ajman University, aged 18 years and above | 614, 69%, 38% were 23–26 years | 25 August 2021–20 October 2021 | NA | Primary school/elementary (19%), secondary education (32%), diploma (26%), university degree (11%), postgraduates (12%). Employment in health sector workers (27%) | Fully vaccinated (77) | NA |
| Qin et al., China [50] | Cross-sectional, Chinese citizen, having child aged under 18 years old | 1724, 50%, 30 years or below 47% | 12 November 2021–19 November 2021 | NA | Bachelor’s degree (77%) | NA | NA |
| Babicki and Mastalerz-Migas. Poland [51] | Cross-sectional, over the age of 18, Poland resident, fully vaccinated, exclude no vaccination or incomplete vaccination | 1528, 83%, NA | 23 September 2021–3 October 2021 | NA | University degree (78%) | Fully vaccinated (100) | Comirnaty, Spikevax, AstraZeneca, Johnson & Johnson, Pfizer |
| Zhang et al., China [52] | Cross-sectional, 18 years or above, a full-time employee of a factory in Shenzhen. Those who did not complete the primary vaccination series and those who received a booster dose were excluded | 2329/ 51%, 46% were 30–39 years | 26 October 2021–31 October 2021 | NA | College/university or higher (46%), employment of a factory in Shenzhen | Fully vaccinated (93), partially vaccinated (7) | Sinopharm, Sinovac, CoronaVac, CanSino |
| Gallant et al., UK [37] | Longitudinal, adults aged 65 and older, living in the UK, independently in the community, were generally in good health | 311, 48%, mean age: 70 years | February 2021–March 2021 | NA | NA | Fully vaccinated (2), partially vaccinated (97) | NA |
| Iguacel et al., Colombia, El Salvador, and Spain [36] | Cross-sectional, 18 years or older, can read and complete the self-administered questionnaire independently | 3026, 67%, 40% were 18–25 years | August 2021–December 2021 | NA | High level (51%); employment: nurse (9%), medical doctor (7%), other health professionals (4%) | Fully vaccinated (78) | NA |
| Sønderskov et al., Denmark [38] | Longitudinal, adult population of Denmark | 1555, 49%, mean age: 53 years | 30 August 2021–15 September 2021 | NA | Primary and lower secondary school (14%), upper secondary education (7%), vocational education (41%), short-cycle higher education (8%), medium-cycle higher education (21%), long-cycle higher education (10%) | Fully vaccinated or planned (95) | Pfizer, Moderna, Johnson, AstraZeneca, an combination |
| Alhasan et al., KSA 1 [53] | Cross-sectional, HCW 3 | 1279, 62%, mean age: 39 years | 9–14 August 2021 | 297 | Low level (23%), medium level (26%), high level (51%); employment: consultant (25%), assistant consultant/fellow (7%), resident/registrar/physician in training (19%), nurse (42%) | Fully vaccinated (69) | Pfizer or AstraZeneca |
| Lounis et al., Algeria [54] | Cross-sectional, Algerian national, at least 18 years old, capacity to communicate in Arabic or French, and being previously vaccinated against SARS-CoV-2 | 787, 62%, NA | 28 January 2022–5 March 2022 | 514 | Bachelor’s degree (44%), masters’ degree or above (48%); employment: HCW (39%), non-HCW (61%) | Fully vaccinated (100) | Sinovac (66%), Sinopharm (5%), AstraZeneca (13%), Janssen (3%), Sputnik V (10%), Pfizer (0.5%) |
| Klugar et al., Czechia [55] | Cross-sectional, HCW | 3454, 81%, NA | 3 to 11 November 2021 | 1105 | Medical professionals (30%), allied health professionals (70%) | Received a third dose (49), fully vaccinated (50), received only one dose (2) | Pfizer (91%) |
| Koh et al., Singapore [56] | Cross-sectional, HCW, temporary staff, pharmacy and diagnostics staff were excluded | 891, 85%, NA | 1 January 2021–10 December 2021 | NA | Administrative staff (14%), allied health workers (5%), ancillary services staff (37%), medical staff (19%), nursing staff (26%) | Fully vaccinated (99) | Pfizer, Moderna, CoronaVac, Sinopharm |
| Kheil et al., USA [57] | Cross-sectional, adults aged 18 years or older | 1746, 55%, NA | 18 October 2021–29 November 2021 | NA | College (17%), bachelor’s degree (29%), master’s degree (15%), doctorate (25%) | Fully vaccinated or planned to receive the second dose (95) | Pfizer, Moderna, Johnson & Johnson |
| Wu et al., China [39] | Longitudinal study, Chinese adults, 18 years old or above | 29,925, 51%, 18–39 years (84%) | 6 to 9 August 2021 | NA | High school graduate (26%), university graduate (61%) | NA | NA |
| Pal et al., USA [58] | Cross-sectional, adults aged 18 years and working in a healthcare setting in the US were included | 1358, 79%, 31–60 years (71%) | 1 February 2021–31 March 2021 | 924 | Vocational (29%), bachelor’s degree (18%), master’s degree (12%), professional degree (28%); employment: DMP (40%), DPCP (38%), administration (10%) | Fully vaccinated or planning to receive both doses (92) | NA |
| Hahn et al., USA [40] | Longitudinal study, residents in remote Alaskan communities, aged 18 years or older; residents in Juneau were excluded | 340, 70%, mean age: 43 years | 9 November 2020–27 September 2021 | NA | NA | Fully vaccinated (100) | NA |
| Yoshida et al., Japan [41] | Retrospective cohort study | 2439, 58%, mean age: 53 years | December 2021 | NA | NA | Fully vaccinated (100) | NA |
| Toro-Ascuy et al., Chile [59] | Cross-sectional, Chilean adult population, 18 years or older | 744, 65%/ 18–59 years (95%) | May 2021–June 2021 | NA | High school (37%), undergraduate (42%), postgraduate (21%) | Not vaccinated (100) | NA |
| Folcarelli et al., Italy [60] | Cross-sectional, fully vaccinated individuals in Naples and did not receive the booster dose | 615, (57%), mean age: 32 years | November 2021–December 2021 | 102 | High school or less (69%), bachelor/graduate degree (31%); employment: student (71%) | Fully vaccinated (100) | Pfizer |
| Wirawan et al., Indonesia [61] | Cross-sectional, residents of Jakarta and Bali, aged 18 years old, and had received at least one dose of the vaccine | 2674, (58%), median age: 29 years | February 2022 | 62 | Completed high school (53%), completed college (39%); employment: unemployed (13%), housewife (25%), student (12%), part-time employment (18%), full-time employment (33%) | NA | NA |
| Aljamaan et al., KSA [62] | Cross-sectional, parents who were residents in KSA | 1340, 65%, 35–44 years (47%) | December 2021–January 2022 | NA | University degree (76%); employment: unemployed/retired (22%), HCW (23%), employee (47%) | Fully vaccinated (61), booster (35) | NA |
| Wong et al., Malaysia [63] | Cross-sectional, fully vaccinated Malaysian residents aged 18 years or older | 1010, 64%, mean age: 32 years | 22 November 2021–9 February 2022 | 145 | Professional and managerial (38%), general worker (14%), self-employed (6%), student (31%), housewife/retired/unemployed (11%) | Fully vaccinated (100) | NA |
| Rababa’h et al., Jordan [64] | Cross-sectional, Jordanian adults aged 18 and above | 475, 76%, 18–39 years (75%) | August 2021 | 237 | Bachelor (51%), graduate studies (34%); employed (58%), unemployed (38%) | NA | NA |
| Al Janabi and Pino. USA [35] | Cross-sectional, medical students | 319, 51%, age range 18–49 years | Spring 2021 | NA | NA | Full | NA |
| Paul and Fancourt. UK [65] | Cross-sectional | 22,139, NA, NA | 21 March 2020–6 December 2021 | NA | NA | NA | NA |
| Mori et al., Japan [34] | Cross-sectional, medical staff at Sakaide | 260, 74%, mean age: 40 years | 2 December to 8 December 2021 | NA | Medical doctors (13%), nurses (51%), administrative staff (24%) | NA | NA |
| Attia et al., Germany [66] | Cross-sectional, students and employees in German universities | 930, 73%, mean age: 29 years | 7 to 19 December 2021 | 55 | 322 were employees and 608 were students | NA | Pfizer was the most common |
| Lai et al., China [67] | Cross-sectional, Chinese adults | 1145, 50%, age range: 18–59 years | June 2021 | NA | College/associate/bachelor’s degree or above (73%), employed (87%) | Vaccinated (79%) | NA |
| Neely and Scacco. USA [68] | Cross-sectional | 600, 52%, NA | July 2021 | NA | NA | NA | NA |
| Motta. USA [42] | A retrospective observational study involving adults older than 18 years | 1551, 54%, mean age: 46 years | 22 to 27 April 2022 | NA | NA | Fully vaccinated (72–78%) | NA |
| Miao et al., China [69] | Cross-sectional, residents in China, 18 years of older vaccinated individuals | 26,755, 53%, NA | 6 to 9 August 2021 | NA | University graduate (63%) | Fully vaccinated | NA |
| Kunno et al., Thailand [70] | Cross-sectional, 18 years or older living in Bangkok and received the first dose of vaccination | 780, 76%, mean age: 42 years | September 2021–December 2021 | 362 | Bachelor’s (61%) | (97) | NA |
| Al Janabi and Pino. USA [71] | Cross-sectional, students at New York Institute of Technology College of Osteopathic Medicine (NYITCOM) | 316, 47%, NA | Spring of 2021 | NA | NA | Fully vaccinated (95) | Pfizer (61%), Moderna (34%), Janssen (5%) |
| Lennon et al., USA [72] | Cross-sectional | 12,287, 51%, age range: 35 to 59 years old | 7 May 2021–7 June 2021 | NA | Some college, not graduate (30%), college graduate/postgraduate degree (30%) | Full | NA |
| Ben-David et al., Israel [73] | Cross-sectional | 400/ 49%, mean age: 69 years | August 2021 | NA | Academic education (53%) | NA | NA |
| Wang et al., China [74] | Cross-sectional, vaccinated Chinese adults were included | 2047, NA, age range: 35–40 years | April to May 2021 | NA | NA | (100) | NA |
| Tung et al., China [75] | Cross-sectional | 1576, 77%, age: ≥40 years (53%) | August 2021 | NA | Senior secondary school and below (49%), university and above 798 (51%) | Fully vaccinated (96) | NA |
| De Giorgio et al., Croatia [76] | Cross-sectional | 1003, NA, NA | December 2021 | NA | NA | Fully vaccinated (33) | Pfizer, AstraZeneca, Johnson & Johnson, Moderna |
| Rzymski et al., Poland [77] | Cross-sectional, included Polish aged 18 years or older and fully vaccinated | 2427, 51%, age: <50 (62%) | September 2021 | 510 | Tertiary education (71%) | (100) | Pfizer, others |
| Jørgensen et al., Denmark [78] | Cross-sectional, Danish citizens aged 18 or older | 31,721, NA, NA | December 2021–13 February 2022 | NA | NA | NA | Pfizer and Moderna |
| Ma et al., China [79] | Cross-sectional, included guardians of children aged <6 years in China | 9424, NA, NA | 15 September 2021–8 October 2021 | NA | NA | NA | NA |
| Sugawara et al., Japan [80] | Cross-sectional, included medical students at Tokyo Medical University | 496, 41%, mean age: 21 years | July 2021 | NA | Medical students | (91) | NA |
| Alobaidi and Hashim. KSA [81] | Cross-sectional, HCWs in KSA aged >18 years | 2059, 50%, mean age: 33 years | 1 October 2021–30 November 2021 | NA | NA | NA | NA |
| Galanis et al., Greece [28] | Cross-sectional, included those aged 18 years or above, had to understand the Greek language and fully vaccinated | 815, 76%, mean age: 37 years | 23 May to 30 May 2022 | 450 | NA | (100) | NA |
| Study, Country | Survey Tool Used | Valid Study Outcome Predictors | Participants Accepting Booster Dose Total | Actual | Intention | Study Quality Score |
|---|---|---|---|---|---|---|
| Peterson et al., USA [43] | Online | NA 2 | 191 (82%) | 0 | 82% | Satisfactory |
| Sønderskov et al., Denmark [44] | Online | NA | 1225 (95) | 0 | 95% | Unsatisfactory |
| Wu et al., China [45] | Online | Gender, age, occupation, discomfort after vaccination, interval after last vaccination, active attention to news, PMT 3 scale (threat appraisal, response efficacy, self-efficacy, and response cost), VHS 4 scale (complacency, convenience, and confidence) | 7974 (97) | 0 | 97% | Satisfactory |
| Marte et al., Dominican Republic [46] | Online | NA | 450 (41) | 0 | 41% | Satisfactory |
| Al-Qerem et al., Jordan [47] | Online | Household average monthly income, severity of symptoms, deliberate receipt of COVID-19 vaccination status, risk level | 408 (45) | 0 | 45% | Satisfactory |
| Hu et al., China [48] | Online | NA | 737 (60) | 0 | 60% | Satisfactory |
| Yadete et al., USA [25] | Online | NA | 1321 (62) | 0 | 62% | Satisfactory |
| Jairoun et al., UAE [49] | Online | Employment, chronic disease status, having relatives infected with COVID-19, COVID-19 full vaccination status, admission to hospital due to COVID-19 | 522 (85) | 0 | 85% | Satisfactory |
| Qin et al., China [50] | Online | NA | 1525 (88) | 0 | 88% | Satisfactory |
| Babicki and Mastalerz-Migas. Poland [51] | Online | Confidence level, age, chronic disease status, adverse event occurrence | 1069 (69.9) | 2.5% | 67.4% | Satisfactory |
| Zhang et al., China [52] | Online | Social-media-related perceptions to booster dose, gender, educational level, monthly personal income, status as frontline workers or management staff | 1956 (84) | 0 | 84% | Satisfactory |
| Gallant et al., UK [37] | Online | NA | 302 (97.1) | 0 | 97.1% | Unsatisfactory |
| Iguacel et al., Colombia, El Salvador, and Spain [36] | Online | Age, gender, occupational status, and vaccination status | 2403 (79.4) | 0 | 79.4% | Unsatisfactory |
| Sønderskov et al., Denmark [38] | Online | Age | 1418 (91.2) | 0 | 91.2% | Satisfactory |
| Alhasan et al., KSA 1 [53] | Online | Nationality, full vaccination status, precaution implementation perception, awareness about the delta variant, and vaccination regimen effectiveness expectations | 707 (55.3) | 0 | 55.3% | Satisfactory |
| Lounis et al., Algeria [54] | Online | Age, sex, education, profession, COVID-19 infection status, postvaccination relief, postvaccination perceptions | 406 (51.6) | 0 | 51.6 | Good |
| Klugar et al., Czechia [55] | Online | NA | 2463 (71.3) | 48.5% | 22.8% | Very good |
| Koh et al., Singapore [56] | Record review | Sex, workplace, and profession as the key factor in affecting time to COVID-19 booster vaccination | 658 (73.8) | 73.8% | 0 | Very good |
| Kheil et al., USA [57] | Online | NA | 1275 (73) | 0 | 73% | Satisfactory |
| Wu et al., China [39] | Hybrid | Age, sex, educational level, marital status, chronic disease condition, smoking status | 26,340 (88.02) | 0 | 88.02% | Good |
| Pal et al., USA [58] | Online | NA | 1135 (83.6) | 0 | 83.6% | Satisfactory |
| Hahn et al., USA [40] | Online | NA | 271 (79.7) | 0 | 79.7 | Satisfactory |
| Yoshida et al., Japan [41] | Face-to-face | Age, sex, number of adverse reactions after the second vaccination, antibody titer, and place of residence | 2388 (97.9) | 97.9% | 0 | Satisfactory |
| Toro-Ascuy et al., Chile [59] | Online | Trust in vaccine status, trust in stakeholders’ status, trust in social media status, trust in press status | 656 (88.2) | 0 | 88.2% | Good |
| Folcarelli et al., Italy [60] | Online | Age, gender, marital status, having cohabitants, education, COVID-19 infection status for the participant or his/her relevant or friends, COVID-19 booster awareness | 527 (85.7) | 85.7% | 0 | Good |
| Wirawan et al., Indonesia [61] | Online | Health beliefs, media influence, trust in authoritative sources, age, sex, religion, education level, employment status, monthly income, health insurance, and COVID-19 history | 1505 (56.3) | 15.1 | 41.2 | Satisfactory |
| Aljamaan et al., KSA [62] | Online | NA | 574 (42.8) | 42.8% | 0 | Unsatisfactory |
| Wong et al., Malaysia [63] | Online | Age group, ethnicity, marital status, average monthly household income, region, past COVID-19 vaccination side effect status, severity of side effects after vaccination, pandemic fatigue status, practices of recommended measures against COVID-19 infection | 820 (81.2) | 0 | 81.2% | Good |
| Rababa’h et al., Jordan [64] | Online | Side effects status | 232 (49) | 0 | 49% | Satisfactory |
| Al Janabi and Pino. USA [35] | Online | Age, gender, marital status, race/ethnicity, household income, campus location, vaccine type | 281 (88.9) | 0 | 88.9% | Satisfactory |
| Paul and Fancourt. UK [65] | Online | Gender, age, ethnicity, education, smoking status, employment status, area of dwelling | - | 0 | 92% | Satisfactory |
| Mori et al., Japan [34] | Online | Age, pregnancy status for females, side effect status | 25 (93.1) | 0 | 93.1% | Unsatisfactory |
| Attia et al., Germany [66] | Online | Gender, age, employment status, pregnancy status (for females), ethical opinion of vaccine justice, vaccine safety opinion | 817 (87.8) | 27.2% | 60.6% | Good |
| Lai et al., China [67] | Online | Age, gender, maternal status, education level, employment status, household annual income, residence, and region | 971 (84.8) | 0 | 84.8% | Very good |
| Neely and Scacco. USA [68] | Online | Age, gender, political affiliation, ethnicity, residence, and region | 556 (92.6) | 0 | 92.6% | Good |
| Motta. USA [42] | Online | Age, gender, education level, employment status, respondents’ political ideology | 760 (49) | 49% | 0 | Good |
| Miao et al., China [69] | Online | Age, gender, educational status, ethnicity, religion, marital status, social level, chronic condition status, smoking status, washing hands status, wearing mask, gathering activities, COVID-19 conspiracy beliefs, risk of COVID-19 infection, curability of COVID-19, vaccine adverse reactions, channel of vaccine information, vaccine conspiracy beliefs, convenience, effectiveness, trust | 25,105 (93.83) | 0 | 93.83% | Satisfactory |
| Kunno et al., Thailand [70] | Online | Level of confidence in the effectiveness of the booster dose and the occurrence of adverse events in them or their loved ones, marital status, education level, occupation | 366 (46.9) | 46.9% | 0 | Satisfactory |
| Al Janabi and Pino. USA [71] | Online | Pharma mistrust, vaccine-induced immunity, vaccines adverse effects | 224 (70.2) | 70.2% | 0 | Unsatisfactory |
| Lennon et al., USA [72] | Mixed (phone and online) | Race, ethnicity, educational level, median income, party identification, geography/urbanity | 5530 (45) | 0 | 45% | Satisfactory |
| Ben-David et al., Israel [73] | Online | Academic education, contracting COVID-19, sense of control | 370 (92.3) | 60% | 32.3% | Unsatisfactory |
| Wang et al., China [74] | Online | Age, gender, healthcare workers, high education | 1552 (75.8) | 0 | 75.8% | Satisfactory |
| Tung et al., China [75] | Online | History of allergic reaction, concerns about vaccine effectiveness and safety | 1436 (91.1) | 0 | 91.1% | Satisfactory |
| De Giorgio et al., Croatia [76] | Online | Unrealistic optimism, age, educational level, employment, loss of a close person, sources of information regarding COVID-19 and vaccines | 789 (78.6) | 0 | 78.6% | Satisfactory |
| Rzymski et al., Poland [77] | Online | COVID-19 vaccine-related side effects status, vaccine trust status | 1724 (71) | 0 | 71% | Satisfactory |
| Jørgensen et al., Denmark [78] | Online | Age, sex, societal threat, response efficacy, self-efficacy, response cost | 27,598 (87) | 0 | 87% | Satisfactory |
| Ma et al., China [79] | Online | Guardians’ education level, children disease status, guardians’ vaccination status, vaccine safety and effectiveness concern status | 8690 (92.21) | 0 | 92.21% | Satisfactory |
| Sugawara et al., Japan [80] | Online | Development of COVID-19 vaccines parents’ opinion | 450 (90.7) | 0 | 90.7% | good |
| Alobaidi and Hashim. KSA [81] | Online | Gender, age, nationality, marital status, educational level, monthly income, comorbid medical illness status, health beliefs | 1464 (71.1) | 0 | 71.1% | Unsatisfactory |
| Galanis et al., Greece [28] | Online | Educational level, comorbidity status, influenza vaccination status, self, relatives COVID-19 infection status | 506 (62) | 0 | 62% | Satisfactory |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelmoneim, S.A.; Sallam, M.; Hafez, D.M.; Elrewany, E.; Mousli, H.M.; Hammad, E.M.; Elkhadry, S.W.; Adam, M.F.; Ghobashy, A.A.; Naguib, M.; et al. COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 298. https://doi.org/10.3390/tropicalmed7100298
Abdelmoneim SA, Sallam M, Hafez DM, Elrewany E, Mousli HM, Hammad EM, Elkhadry SW, Adam MF, Ghobashy AA, Naguib M, et al. COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(10):298. https://doi.org/10.3390/tropicalmed7100298
Chicago/Turabian StyleAbdelmoneim, Shaimaa Abdelaziz, Malik Sallam, Dina Mohamed Hafez, Ehab Elrewany, Hesham Metwalli Mousli, Elsayed Mohamed Hammad, Sally Waheed Elkhadry, Mohammed Fathelrahman Adam, Amr Abdelraouf Ghobashy, Manal Naguib, and et al. 2022. "COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 10: 298. https://doi.org/10.3390/tropicalmed7100298
APA StyleAbdelmoneim, S. A., Sallam, M., Hafez, D. M., Elrewany, E., Mousli, H. M., Hammad, E. M., Elkhadry, S. W., Adam, M. F., Ghobashy, A. A., Naguib, M., Nour El-Deen, A. E.-S., Aji, N., & Ghazy, R. M. (2022). COVID-19 Vaccine Booster Dose Acceptance: Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease, 7(10), 298. https://doi.org/10.3390/tropicalmed7100298