
Developing Usability Guidelines for mHealth Applications (UGmHA)


Abstract
1. Introduction
- Some of the guidelines are general, which means they are not specified for mHealth applications, such as Nielsen’s principles [11]. Since mHealth applications are intended to affect the health and the body of people, they need to have more rigorous and restricted guidelines.
- Some of the guidelines are specified for mHealth applications; however, they cover only a few features of mHealth applications, such as:
- (a)
- Xcertia [12], which covered access to personal health information and notification features, while other features, such as self-monitoring, were not covered.
- (b)
- HE4EH [6], which covered self-monitoring, health goals and tips and biometric measurement features, while other features, such as consultations, were not covered.
- (c)
- Telemedicine recommendations [13], which covered consultations and booking appointment features, while other features, such as self-monitoring, were not covered.
- Simple to follow and understandable by designers, developers and evaluators.
- Accessible to all people, including elderly people and people with special needs.
- Specialized in designing and evaluating mHealth applications that can cover different features. The following are examples of features gathered from different studies:
2. Literature Review
2.1. Electronic Health (eHealth) and Mobile Health (mHealth)
2.2. Usability and Guidelines
- Visibility of system status.
- Match between system and the real world.
- User control and freedom.
- Consistency and standards.
- Error prevention.
- Recognition rather than recall.
- Flexibility and efficiency of use.
- Aesthetic and minimalist design.
- Help users recognize, diagnose and recover from errors.
- Help and documentation.
- Visual design.
- Readability.
- App navigation.
- Onboarding.
- App feedback.
- Notifications, alerts and alarms.
- Help resources and troubleshooting.
- Historical data.
- Accessibility.
- Ongoing app evaluation.
- Visibility of system status.
- User control and freedom.
- Match between system and real world.
- Consistency and standards.
- Error prevention.
- Help users recognize, diagnose and recover from errors.
- Recognition rather than recall.
- Flexibility and efficiency of use.
- Aesthetic and minimalist design.
- Help and documentation.
- Privacy.
- Skills.
- Pleasurable interaction.
- Accessibility.
- Compatibility between different platforms.
- Minimized human–device interaction.
- Physical interaction and ergonomics.
- Readability and layout.
- Non-interrupting app information visualization.
- Content.
- Display.
- Navigation.
- Interactivity.
- Behavior change.
- Self-monitoring.
- Look and Feel
- Make elements on the page easy to read.
- Easy recognition and accessibility.
- Make clickable items easy to target and hit.
- Use language and culture appropriate for the elderly; minimize technical terms.
- Interaction
- Provide clear feedback on actions.
- Provide preferable gestures for the elderly.
- Provide the elderly with information on launcher/elderly status.
- Use conventional interaction items.
- Ergonomic design.
- Functionality
- Provide functions that reduce elderly memory load.
- Elderly does not feel lost or stuck (elderly control and freedom).
- Prevent errors from occurring.
- Provide necessary information and settings.
- Minimised distractions.
- Easy to operate.
- Readability and visualization.
- Consistency.
- Feedback.
- Navigability.
- Personalizing.
- Easy to understand and relevant.
- Learner-friendly.
2.3. Common Approaches for Developing New Usability Guidelines
- Exploratory stage: to collect existing studies related to the main topics of the research, such as general or related usability guidelines, principles, application features and attributes.
- Descriptive stage: to highlight the most important information of the previously collected studies to formalize the main concept of the research.
- Correlational stage: to determine the characteristics that the usability guidelines of the specific domain should have based on traditional guidelines.
- Selection stage: to keep, adapt or discard the existing sets of usability guidelines that were selected in the descriptive stage.
- Specification stage: to formally specify the set of proposed guidelines using a standard template.
- Validation (experimental) stage: to test the proposed guidelines against traditional ones through experiments.
- Refinement stage: to refine the proposed guidelines based on the validation-stage results.
2.4. Common Methods for Validating New Usability Guidelines
- Guideline evaluation: to check the proposed guidelines against traditional or specialized guidelines in terms of the number of discovered usability issues (The recommended method).
- Expert judgment: using a questionnaire that assesses expert and evaluator perceptions of the proposed usability guidelines (To receive additional feedback).
- User testing: to obtain users’ opinions about the proposed set of usability guidelines (To receive additional feedback).
- Between-subject: each participant is exposed to only one condition of testing.
- Within-subject: each participant is exposed to more than one of the conditions of testing.
- Number of the discovered usability issues.
- Number of discovered specific usability issues.
- Number of severe usability issues.
- Number of critical usability issues.
3. Materials and Methods
3.1. Developing UGmHA
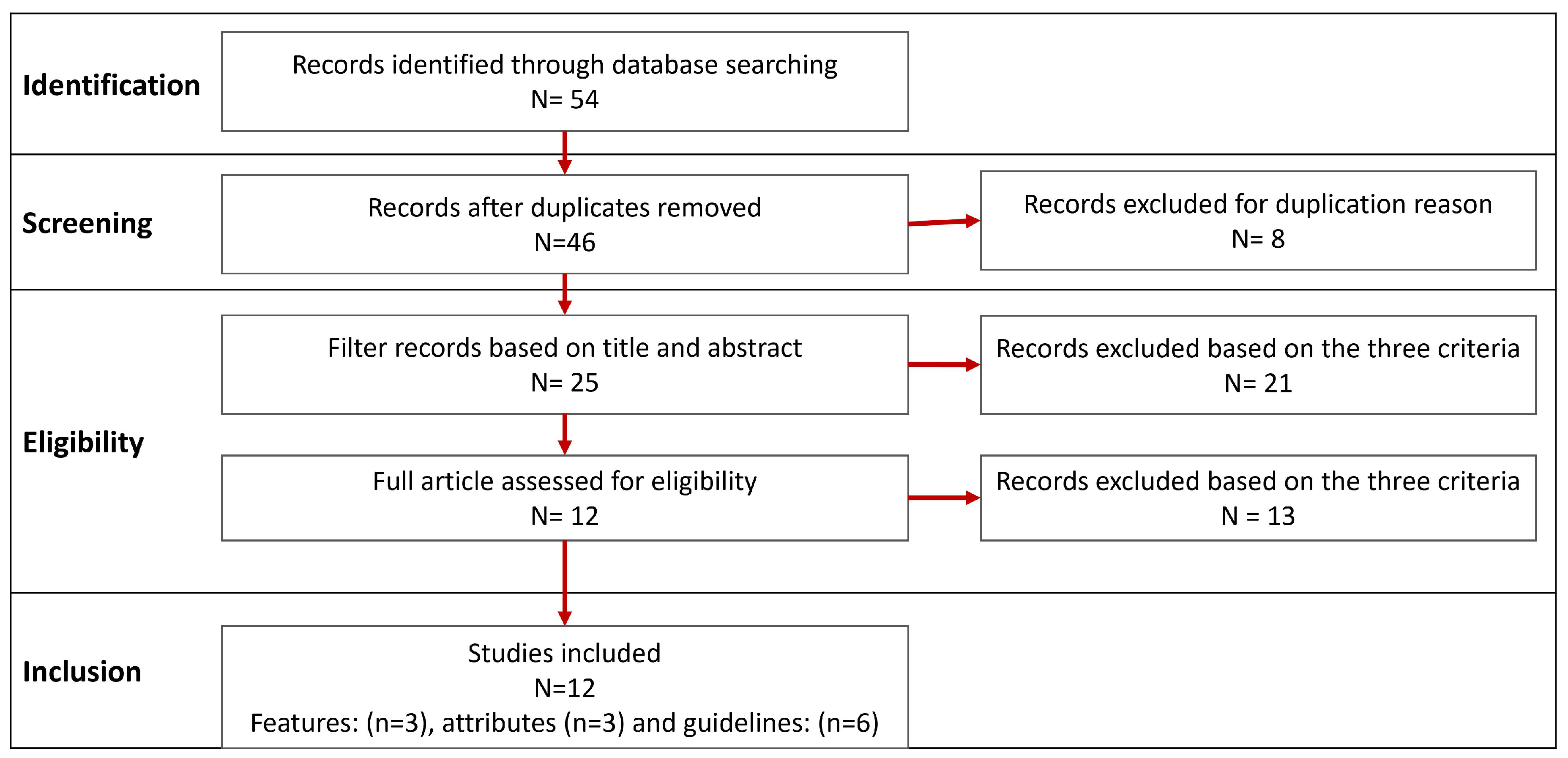
3.1.1. Stage 1: Exploratory Stage
- For features: (“mHealth applications” OR “mobile health applications”) AND “features”.
- For attributes: (“mHealth applications” OR “mobile health applications”) AND “attributes”.
- For guidelines and recommendations: (“mHealth applications” OR “mobile health applications”) AND (“usability guidelines” OR “usability principles” OR “usability heuristics” OR “design recommendations”).
- For accessibility guidelines: (“mHealth applications” OR “mobile health applications”) AND “accessibility guidelines”.
- Usability attributes, which include:
- –
- ISO attributes (effective, efficiency and satisfaction) [46].
- –
- Nielsen’s attributes (learnability, efficiency, memorability, errors and satisfaction) [47].
- –
- PACMAD attributes, which combine both attributes of ISO and Nielsen in addition to the cognitive load attribute (effective, efficiency, learnability, memorability, errors, satisfaction and cognitive load) [48].
- Usability guidelines and design recommendations, which include:
3.1.2. Stage 2: Descriptive Stage
- For features: we gathered all features from [14,15,16] and summarized them to obtain a list of integrated features. Additionally, we added two more features related to our research, which were accessibility to elderly people and accessibility to people with special needs. Below are the selected features:
- Booking appointments [16].
- Access to personal health information [15].
- Allowing uploading and viewing of biometric measurements [14].
- Graphic display of patient’s information [14].
- Track health progress [15].
- Reminders and notifications [14].
- Sharing health data with friends [15].
- Interactive prompts [14].
- Earn rewards [15].
- Bluetooth technology connection [14].
- Accessibility to elderly people.
- Accessibility to people with special needs.
- For usability attributes: we selected only the PACMAD [48] attributes since they combine attributes of both ISO [46] and Nielsen [47]. Below are the selected attributes and their definition based on PACMAD [48].
- –
- Effectiveness: the ability to produce the desired outputs.
- –
- Efficiency: the reduction of wasted materials, such as time, money and effort.
- –
- Satisfaction: the fulfillment of the user’s needs and desires.
- –
- Learnability: a user can learn how to use the application easily.
- –
- Memorability: a user can remember how to use the application after a while.
- –
- Errors: minimizing the user’s error rate while using the application.
- –
- Cognitive Load: the ability to use a mobile application while doing daily activities.
- For usability guidelines: we classified the studies into the main guidelines, which will be used as basic guidelines for the next stages, and checklist items, which help to make the main guidelines more specific to the mHealth applications:
- –
- Main guidelines: we selected all of Nielsen’s principles [11] as well as the “usability” workgroup of Xcertia guidelines [12]. The reason for selecting these two guidelines is that Nielsen’s principles are well-known guidelines that are used to evaluate most user interfaces. Moreover, Xcertia is specified to evaluate mHealth applications in general and developed by authorized organizations in the US.
- –
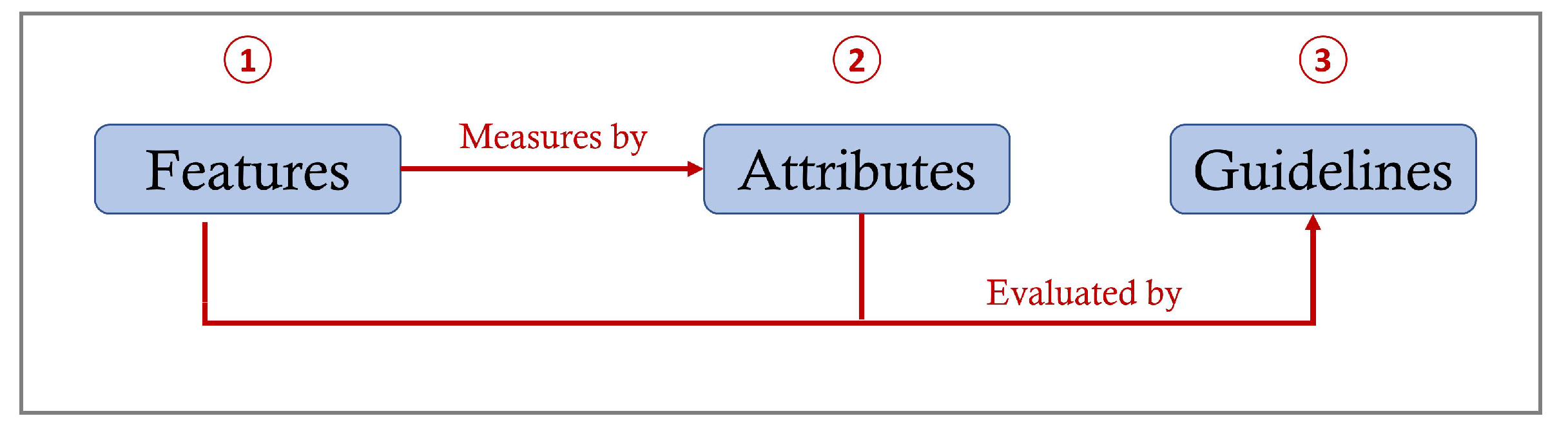
3.1.3. Stage 3: Correlational Stage
- Attributes:
- –
- Effectiveness: to measure if the appointment is booked at the right date and time selected by the user.
- –
- Efficiency: to measure if this feature saves users’ time and effort without the need to go to the clinic.
- Guidelines:
- –
- Visibility of system status in Nielsen and App feedback in Xcertia: to evaluate booking appointments with the effectiveness attribute if the application provides feedback to the user regarding the right date and time of the appointment.
- –
- Notifications and alarms in Xcertia: to evaluate booking appointments with the efficiency attribute if the application notifies a user after an appointment is booked. Thus, the users’ time and effort to remember the appointment are minimized.
- –
- Historical data in Xcertia: to evaluate booking appointments with the efficiency attribute if the application saves previous and upcoming appointments. Thus, the users’ time and effort to call the clinic to ask for their appointments are minimized.
3.1.4. Stage 4: Selection Stage
- Keep: without any change if the guideline is clear and correctly matched to the specific feature of mHealth applications.
- Adapt: if the guideline needs a change to be more related to the mHealth applications.
- Eliminate: if the guideline is redundant or not relevant to the features of mHealth applications.
- Create: if a new guideline is required to evaluate the specific feature of the mHealth applications that the main guidelines cannot evaluate.
3.1.5. Stage 5: Specification Stage
3.2. Validating UGmHA
3.2.1. Stage 6: Validation Stage
- Guideline evaluation phase: check the new set of UGmHA against Nielsen and Xcertia guidelines regarding the number of identified usability issues and severity.
- Expert judgment phase: evaluate the usefulness, efficiency and effectiveness of UGmHA guidelines by questionnaire or interview. Then, the results will be used in the seventh stage (refining stage) of Quinones et al.’s methodology [17].
- User testing phase: enhance the usability of an existing application using refined guidelines of UGmHA. Then, perform user testing for the enhanced application.
- Experiment Design:
- –
- Participants: The evaluators who participated in this experiment are two of the authors of this research. The first evaluator was Mrs. Eman Nasr, a master’s student in the Faculty of Computing and Information Technology (FCIT) at King Abdulaziz University with a medium knowledge of usability evaluation. The second evaluator was Dr. Duaa Sinnari, an assistant professor in FCIT at King Abdulaziz University with high experience in usability evaluation and human–computer interaction (HCI).
- –
- Guidelines: UGmHA was tested against Nielsen’s principles and the Xceria guidelines. The reason for selecting these two guidelines is that UGmHA is based mostly on Nielsen’s and Xcertia guidelines and because Nielsen’s principles are well-known guidelines and Xcertia is specified to evaluate mHealth applications.
- –
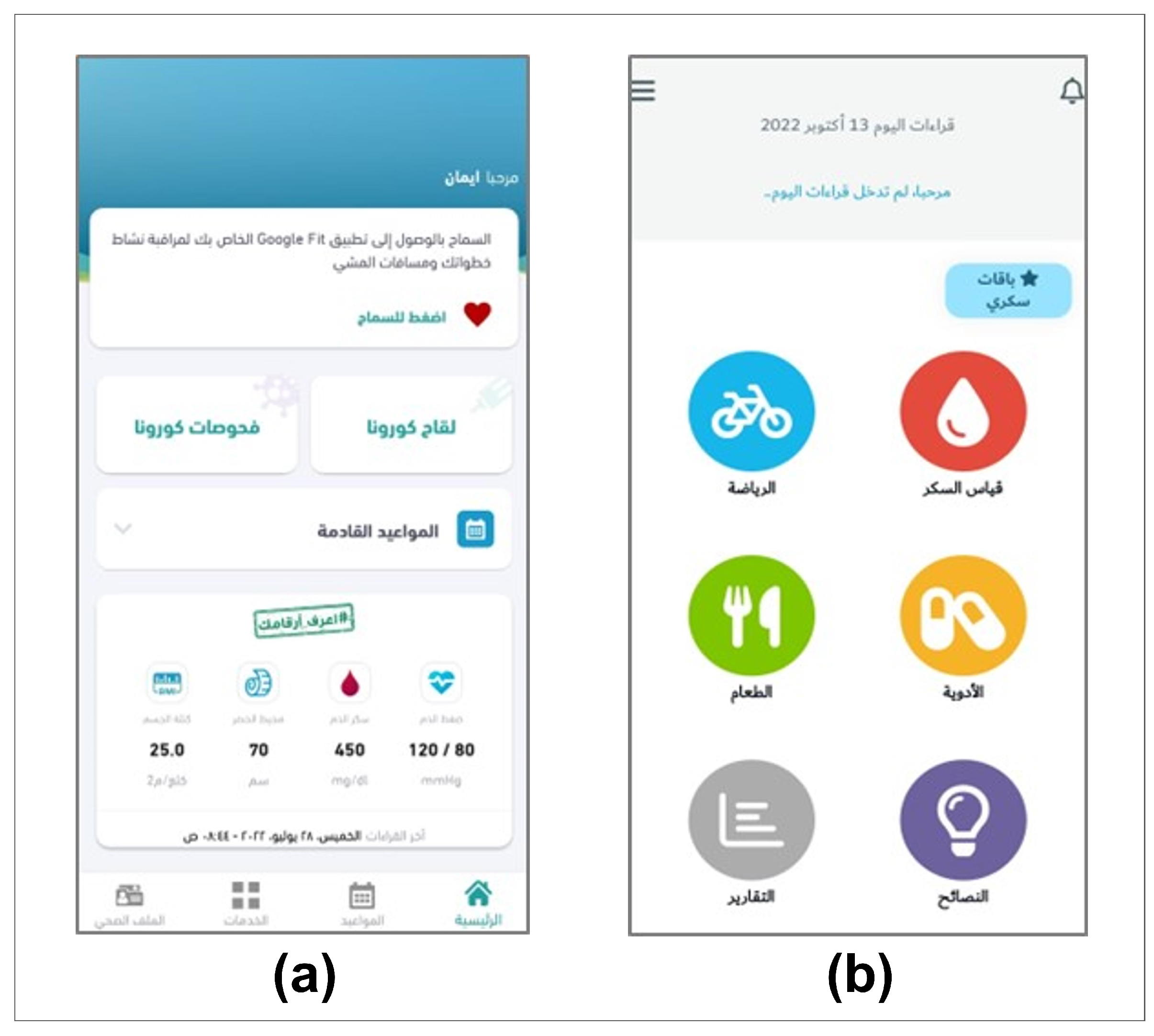
- Applications: We selected the “Sehhaty” and “Sokry” applications. Figure 4 shows the home screen of (a) the first application (Sehhaty) and (b) the second application (Sokry) on the Android operating system in the Arabic language. The reasons for selecting these two applications are because they are simple to use and to achieve diversity between the selected applications based on governmental/ private, functionality and popularity as shown in Table 8.
- Experiment Procedure: To assess the performance, each of the evaluators evaluated both applications individually in a within-subject study that compared the UGmHA, Xcertia and Nielsen guidelines. First, the evaluators evaluated the “Sehhaty” and “Sokry” applications individually using Nielsen’s guidelines and wrote down the discovered usability issues for each application. Second, the assessments of each evaluator using Nielsen’s guidelines were grouped together to generate a single list of usability issues for each application.Third, the evaluators worked together to rate each usability issue in the generated list based on the Severity Rating Scale (SRS). The SRS has five points (0–4) that can be used to prioritize and estimate which usability issues are important to be fixed as shown in Table 9 [51]. Then, the same aforementioned processes were repeated using Xcertia followed by the UGmHA guidelines. From this experiment, we produced six lists of usability issues, which are:
- Using Nielsen’s guidelines: list of usability issues of the “Sehhaty” application.
- Using Nielsen’s guidelines: list of usability issues of the “Sokry” application.
- Using Xcertia guidelines: list of usability issues of the “Sehhaty” application.
- Using Xcertia guidelines: list of usability issues of the “Sokry” application.
- Using UGmHA guidelines: list of usability issues of the “Sehhaty“ application.
- Using UGmHA guidelines: list of usability issues of the “Sokry” application.
3.2.2. Stage 7: Refining Stage
- Document the changes that should be made to the guidelines.
- Define the guidelines to be created, refined or deleted.
- Iterate and repeat some stages again, if necessary.
4. Results
4.1. Results of UGmHA Development
4.2. Results of the UGmHA Validation
4.2.1. Number of Usability Issues among the Three Guidelines
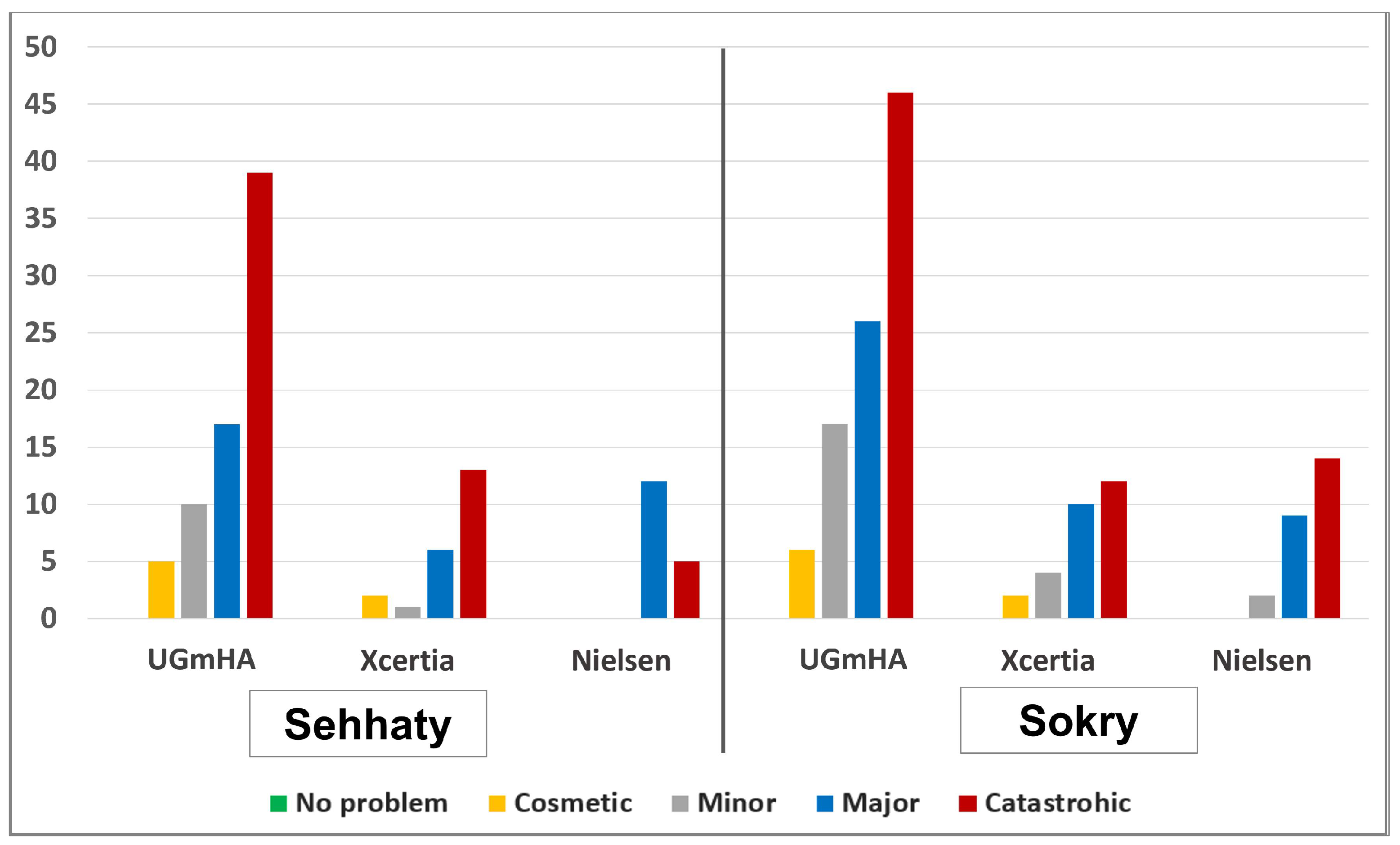
4.2.2. Severity of Usability Issues among the Three Guidelines
5. Discussion
5.1. UGmHA Development Discussion
- HE4EH [6], which covers self-monitoring, biometric measurements, etc.
- Telemedicine of mHealth applications [13], which covers consultation, booking appointments, etc.
- Elderly people [34], which covers the feature of accessibility for elderly people.
- People with special needs [35], which covers the feature of accessibility for people with special needs.
5.2. UGmHA Validation Discussion
6. Conclusions and Future Work
- Generating design recommendations based on the discovered usability issues for “Sehhaty” or “Sokry” and obtaining the application team’s opinion.
- Expert judgment by reviewing guidelines by user experience (UX) experts and acquiring their advice and comments to perform the Refining stage.
- User testing by enhancing the usability of an existing application using refined guidelines of UGmHA and, then, performing user testing for the enhanced application.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| eHealth | Electronic health |
| mHealth | Mobile health |
| UGmHA | Usability guidelines for mHealth applications |
| FDA | Food and Drug Administration |
| HIMSS | Healthcare Information and Management Systems Society |
| SRS | Severity rating scale |
| HCP | Healthcare provider |
Appendix A. Final Usability Guidelines for mHealth Applications (UGmHA)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | MHP1 |
|---|---|
| Priority | (3) Critical |
| Name | Visibility of system status (Application Feedback) |
| Definition | Ensure that the application keeps users aware of what is going on in the application by including appropriate feedback on user actions. |
| Features | Booking appointments, consultation with HCP via text, voice messages and video calls; sharing data with HCP; access to personal health information; self-monitoring of chronic diseases; allowing uploading and viewing of biometric measurements; set health goals and treatment plans; track health progress; Bluetooth technology; and accessibility by elderly people. |
| Checklists |
|
| ID | MHP2 |
|---|---|
| Priority | (2) Important. |
| Name | Match between the system and the real world (Metaphor). |
| Definition | Ensure that the application speaks the users’ language, employs terminology and concepts that the user is familiar with and arranges information in a natural and logical sequence. |
| Features | Accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP3 |
|---|---|
| Priority | (2) Important. |
| Name | User control and freedom (Navigation). |
| Definition | Ensure that the application has proper navigation and provides an “emergency exit” to smoothly leave an unwanted state. |
| Features | Booking appointments, consultation with HCP via text, voice messages and video calls; access to personal health information; self-monitoring of chronic diseases; allowing uploading and viewing of biometric measurements; and accessibility by elderly people. |
| Checklists |
|
| ID | MHP4 |
|---|---|
| Priority | (2) Important. |
| Name | Consistency and standards. |
| Definition | Ensure that the application’s elements are consistent and follow the standard design of the application. |
| Features | Accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP5 |
|---|---|
| Priority | (3) Critical. |
| Name | Error prevention. |
| Definition | Ensure that the application prevents problems from occurring by careful design. |
| Features | Booking appointments, self-monitoring of chronic diseases, allowing uploading and viewing of biometric measurements, accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP6 |
|---|---|
| Priority | (2) Important. |
| Name | Recognition rather than recall (Memory). |
| Definition | Ensure that the application minimizes the user’s memory load. |
| Features | Booking appointments, consultation with HCP via text, voice messages and video calls; access to personal health information; self-monitoring of chronic diseases; accessibility by elderly people; and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP7 |
|---|---|
| Priority | (1) Useful. |
| Name | Flexibility and efficiency of use (Efficiency). |
| Definition | Ensure that the application provides an accelerator that shortcuts some actions and allows users to customize the application based on their needs and preferences. |
| Features | Consultation with HCP via text, voice messages and video calls; sharing data with HCP; access to personal health information; self-monitoring of chronic diseases; accessibility by elderly people; and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP8 |
|---|---|
| Priority | (1) Useful. |
| Name | Aesthetic and minimalist design (Design). |
| Definition | Ensure that the application does not contain useless or irrelevant information. Ensure that the visual design adheres to the contrast, repetition, alignment and proximity rules. |
| Features | Access to personal health information, accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP9 |
|---|---|
| Priority | (3) Critical. |
| Name | Error diagnosis and recovery (Recovery). |
| Definition | Ensure that the application expresses the error messages in plain language (with no codes), accurately describes the issue and positively suggests a solution. |
| Features | Accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
| ID | MHP10 |
|---|---|
| Priority | (1) Useful. |
| Name | Help and documentation (Help). |
| Definition | Ensure that the application incorporates clear help and troubleshooting tools to assist users when necessary. |
| Features | Self-monitoring of chronic diseases, interactive prompts, accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP11 |
|---|---|
| Priority | (3) Critical. |
| Name | Notifications, alerts and alarms (Notifications). |
| Definition | Ensures that the application’s notifications, alerts and alarms take both safety and usability into account to notify users when their attention is required. Notifications (general reminders for users). Alerts (non-urgent signs meant to catch user attention). Alarms (urgent signs for safety-critical messages). |
| Features | Booking appointments, consultation with HCP via text, voice messages and video calls; self-monitoring of chronic diseases; allowing uploading and viewing of biometric measurements; reminders and notifications; and interactive prompts. |
| Checklists |
|
| ID | MHP12 |
|---|---|
| Priority | (2) Important. |
| Name | Onboarding. |
| Definition | Ensure that the application facilitates launching, registering and preparing for first time use. |
| Features | Access to personal health information. |
| Checklists |
|
| ID | MHP13 |
|---|---|
| Priority | (3) Critical. |
| Name | Historical data (History). |
| Definition | Ensure that the application stores historical data that allow users to access, read and understand these data easily. |
| Features | Booking appointments, consultation with HCP via text, voice messages and video calls; access to personal health information; self-monitoring of chronic diseases; allowing uploading and viewing of biometric measurements; graphic display of patient’s information; and track health progress. |
| Checklists |
|
| ID | MHP14 |
|---|---|
| Priority | (3) Critical. |
| Name | Accessibility. |
| Definition | Ensure that the application is usable by all users, including elderly people and people with special needs. |
| Features | accessibility by elderly people and accessibility by people with special needs. |
| Checklists |
|
| ID | MHP15 |
|---|---|
| Priority | (2) Important. |
| Name | Ongoing app evaluation (Evaluation). |
| Definition | Ensure that the application undergoes iterative evaluation and follows a user-centered design. |
| Features | Important to design and evaluate all features. |
| Checklists |
|
| ID | MHP16 |
|---|---|
| Priority | (1) Useful. |
| Name | Interactivity and motivations (Interactivity). |
| Definition | Ensure that the application motivates users and allows for communication between patients to share their experiences. |
| Features | Consultation with HCP via text, voice messages and video calls; sharing data with HCP; self-monitoring of chronic diseases; health tips and motivation; sharing health data with friends; interactive prompts; and earning rewards. |
| Checklists |
|
References
- Risling, T.; Martinez, J.; Young, J.; Thorp-Froslie, N. Evaluating patient empowerment in association with eHealth technology: Scoping review. J. Med. Internet Res. 2017, 19, e329. [Google Scholar] [CrossRef] [PubMed]
- Dicianno, B.E.; Parmanto, B.; Fairman, A.D.; Crytzer, T.M.; Yu, D.X.; Pramana, G.; Coughenour, D.; Petrazzi, A.A. Perspectives on the evolution of mobile (mHealth) technologies and application to rehabilitation. Phys. Ther. 2015, 95, 397–405. [Google Scholar] [CrossRef]
- Istepanian, R.S.; Jovanov, E.; Zhang, Y. Guest editorial introduction to the special section on m-health: Beyond seamless mobility and global wireless health-care connectivity. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 405–414. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New Horizons for Health Through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Barutçu, S. mHealth apps design using quality function deployment. Int. J. Health Care Qual. Assur. 2019, 32, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Khowaja, K.; Al-Thani, D. New checklist for the heuristic evaluation of mHealth apps (HE4EH): Development and usability study. JMIR mHealth uHealth 2020, 8, e20353. [Google Scholar] [CrossRef]
- Cook, V.E.; Ellis, A.K.; Hildebrand, K.J. Mobile health applications in clinical practice: Pearls, pitfalls, and key considerations. Ann. Allergy Asthma Immunol. 2016, 117, 143–149. [Google Scholar] [CrossRef]
- Larson, R.S. A path to better-quality mHealth apps. JMIR mHealth uHealth 2018, 6, e10414. [Google Scholar] [CrossRef]
- Andrade, F.; Nascimento, L.; Wood, G.; Calil, S. Applying heuristic evaluation on medical devices user manuals. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Toronto, ON, Canada, 7–12 June 2015; Springer: Cham, Switzerland, 2015; pp. 1515–1518. [Google Scholar]
- Rusu, C.; Roncagliolo, S.; Rusu, V.; Collazos, C. A Methodology to establish usability heuristics. In Proceedings of the ACHI 2011: The Fourth International Conference on Advances in Computer-Human Interactions, Guadeloupe, France, 23–28 February 2011; IARIA: Wilmington, NC, USA, 2011; pp. 59–62. [Google Scholar]
- Nielsen, J. Ten Usability Heuristics. 2005. Available online: http://www.nngroup.com/articles/ten-usability-heuristics (accessed on 5 November 2021).
- Xcertia mHealth App Guidelines. 2019. Available online: https://www.himss.org/sites/hde/files/media/file/2020/04/17/xcertia-guidelines-2019-final.pdf (accessed on 7 November 2020).
- Aldekhyyel, R.N.; Almulhem, J.A.; Binkheder, S. Usability of Telemedicine Mobile Applications during COVID-19 in Saudi Arabia: A Heuristic Evaluation of Patient User Interfaces. Healthcare 2021, 9, 1574. [Google Scholar] [CrossRef]
- Donevant, S.B.; Estrada, R.D.; Culley, J.M.; Habing, B.; Adams, S.A. Exploring app features with outcomes in mHealth studies involving chronic respiratory diseases, diabetes, and hypertension: A targeted exploration of the literature. J. Am. Med. Inform. Assoc. 2018, 25, 1407–1418. [Google Scholar] [CrossRef]
- Lazard, A.J.; Brennen, J.S.B.; Belina, S.P. App Designs and Interactive Features to Increase mHealth Adoption: User Expectation Survey and Experiment. JMIR mHealth uHealth 2021, 9, e29815. [Google Scholar] [CrossRef]
- Shati, A. Mhealth applications developed by the Ministry of Health for public users in KSA: A persuasive systems design evaluation. Health Inform. Int. J. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Quiñones, D.; Rusu, C.; Rusu, V. A methodology to develop usability/user experience heuristics. Comput. Stand. Interfaces 2018, 59, 109–129. [Google Scholar] [CrossRef]
- Mitchell, J. From Telehealth to e-Health: The Unstoppable Rise of e-Health; Department of Communications, Information Technology and the Arts: Canberra, Australia, 1999. [Google Scholar]
- Rooij, T.v.; Marsh, S. eHealth: Past and future perspectives. Pers. Med. 2016, 13, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Black, A.D.; Car, J.; Pagliari, C.; Anandan, C.; Cresswell, K.; Bokun, T.; McKinstry, B.; Procter, R.; Majeed, A.; Sheikh, A. The impact of eHealth on the quality and safety of health care: A systematic overview. PLoS Med. 2011, 8, e1000387. [Google Scholar] [CrossRef] [PubMed]
- Prado, L.; Carpentier, C.; Préau, M.; Schott, A.M.; Dima, A. mHealth Apps for Self-Management of Chronic Conditions in France: What Is Out There? In MEDINFO 2019: Health and Wellbeing e-Networks for All; IOS Press: Amsterdam, The Netherlands, 2019; pp. 1970–1971. [Google Scholar]
- Markus, M.L.; Keil, M. If we build it, they will come: Designing information systems that people want to use. MIT Sloan Manag. Rev. 1994, 35, 11. [Google Scholar]
- Tan, W.s.; Liu, D.; Bishu, R. Web evaluation: Heuristic evaluation vs. user testing. Int. J. Ind. Ergon. 2009, 39, 621–627. [Google Scholar] [CrossRef]
- International Organization for Standardization. Ergonomic Requirements for Office Work with Visual Display Terminals (VDTs); ISO: Geneva, Switzerland, 1992. [Google Scholar]
- Bevana, N.; Kirakowskib, J.; Maissela, J. What is usability. In Proceedings of the fourth International Conference on HCI, Stuttgart, Germany, 1–6 September 1991; pp. 1–6. [Google Scholar]
- Nielsen, J.; Molich, R. Heuristic evaluation of user interfaces. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Seattle, WA, USA, 1–5 April 1990; pp. 249–256. [Google Scholar]
- Quiñones, D.; Rusu, C. How to develop usability heuristics: A systematic literature review. Comput. Stand. Interfaces 2017, 53, 89–122. [Google Scholar] [CrossRef]
- Hermawati, S.; Lawson, G. Establishing usability heuristics for heuristics evaluation in a specific domain: Is there a consensus? Appl. Ergon. 2016, 56, 34–51. [Google Scholar] [CrossRef]
- Vieira, E.A.O.; Silveira, A.C.D.; Martins, R.X. Heuristic evaluation on usability of educational games: A systematic review. Inform. Educ. 2019, 18, 427–442. [Google Scholar] [CrossRef]
- Paz, F.; Paz, F.A.; Pow-Sang, J.A.; Collantes, L. Usability heuristics for transactional web sites. In Proceedings of the 2014 11th International Conference on Information Technology: New Generations, IEEE, Las Vegas, NV, USA, 7–9 April 2014; pp. 627–628. [Google Scholar]
- Leverenz, T. The Development and Validation of a Heuristic Checklist for Clinical Decision Support Mobile Applications. Ph.D. Thesis, Wichita State University, Wichita, KS, USA, 2019. [Google Scholar]
- Chattratichart, J.; Lindgaard, G. A comparative evaluation of heuristic-based usability inspection methods. In CHI’08 Extended Abstracts on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, 2008; pp. 2213–2220. [Google Scholar]
- Roy, B.; Call, M.; Abts, N. Development of usability guidelines for mobile health applications. In Proceedings of the International Conference on Human–Computer Interaction, Orlando, FL, USA, 26–31 July 2019; Springer: Cham, Switzerland, 2019; pp. 500–506. [Google Scholar]
- Al-Razgan, M.S.; Al-Khalifa, H.S.; Al-Shahrani, M.D. Heuristics for evaluating the usability of mobile launchers for elderly people. In Proceedings of the International Conference of Design, User Experience, and Usability, Heraklion, Crete, Greece, 22–27 June 2014; Springer: Cham, Switzerland, 2014; pp. 415–424. [Google Scholar]
- Arachchi, T.K.; Sitbon, L.; Zhang, J. Enhancing access to eLearning for people with intellectual disability: Integrating usability with learning. In Proceedings of the IFIP Conference on Human–Computer Interaction, Mumbai, India, 25–29 September 2017; Springer: Cham, Switzerland, 2017; pp. 13–32. [Google Scholar]
- Sanz, F.; Galvez, R.; Rusu, C.; Roncagliolo, S.; Rusu, V.; Collazos, C.A.; Cofré, J.P.; Campos, A.; Quiñones, D. A set of usability heuristics and design recommendations for u-learning applications. In Proceedings of the Information Technology: New Generations: 13th International Conference on Information Technology, Las Vegas, NV, USA, 11–13 April 2016; Springer: Cham, Switzerland, 2016; pp. 983–993. [Google Scholar]
- Campos, A.; Rusu, C.; Roncagliolo, S.; Sanz, F.; Gálvez, R.; Quiñones, D. Usability heuristics and design recommendations for driving simulators. In Proceedings of the Information Technology: New Generations: 13th International Conference on Information Technology, Las Vegas, NV, USA, 11–13 April 2016; Springer: Cham, Switzerland, 2016; pp. 1287–1290. [Google Scholar]
- Gale, N.; Mirza-Babaei, P.; Pedersen, I. Heuristic guidelines for playful wearable augmented reality applications. In Proceedings of the 2015 Annual Symposium on Computer-Human Interaction in Play, London, UK, 5–7 October 2015; pp. 529–534. [Google Scholar]
- da Hora Rodrigues, K.R.; Teixeira, C.A.C.; de Almeida Neris, V.P. Heuristics for assessing emotional response of viewers during the interaction with TV programs. In Proceedings of the Human–Computer Interaction. Theories, Methods, and Tools: 16th International Conference, HCI International 2014, Heraklion, Crete, Greece, 22–27 June 2014; Proceedings, Part I 16. Springer: Cham, Switzerland, 2014; pp. 577–588. [Google Scholar]
- Charness, G.; Gneezy, U.; Kuhn, M.A. Experimental methods: Between-subject and within-subject design. J. Econ. Behav. Organ. 2012, 81, 1–8. [Google Scholar] [CrossRef]
- Kuparinen, L.; Silvennoinen, J.; Isomäki, H. Introducing usability heuristics for mobile map applications. In Proceedings of the International Cartographic Conference, Dresden, Germany, 25–30 August 2013; International Cartographic Association: Bern, Switzerland, 2013. [Google Scholar]
- Munoz, R.; Chalegre, V. Defining virtual worlds usability heuristics. In Proceedings of the 2012 Ninth International Conference on Information Technology-New Generations, IEEE, Las Vegas, NV, USA, 16–18 April 2012; pp. 690–695. [Google Scholar]
- Moraes, M.C.; Silveira, M.S. How am I? Guidelines for animated interface agents evaluation. In Proceedings of the 2006 IEEE/WIC/ACM International Conference on Intelligent Agent Technology, IEEE, Hong Kong, China, 18–22 December 2006; pp. 200–203. [Google Scholar]
- Muhanna, M.; Masoud, A.; Qusef, A. Usability heuristics for evaluating Arabic mobile games. Int. J. Comput. Games Technol. 2022, 2022, 5641486. [Google Scholar] [CrossRef]
- Keele, S. Guidelines for Performing Systematic Literature Reviews in Software Engineering; Technical Report, Ver. 2.3; EBSE: Durham, UK, 2007. [Google Scholar]
- Iso, W. 9241-11. Ergonomic requirements for office work with visual display terminals (VDTs). Int. Organ. Stand. 1998, 45, 22. [Google Scholar]
- Usability 101: Introduction to Usability. 2012. Available online: https://www.nngroup.com/articles/usability-101-introduction-to-usability/ (accessed on 8 March 2021).
- Harrison, R.; Flood, D.; Duce, D. Usability of mobile applications: Literature review and rationale for a new usability model. J. Interact. Sci. 2013, 1, 1. [Google Scholar] [CrossRef]
- Sehhaty Application. 2022. Available online: https://play.google.com/store/apps/details?id=com.lean.sehhaty (accessed on 6 December 2022).
- Sokry Application. 2022. Available online: https://play.google.com/store/apps/details?id=com.sokry (accessed on 6 December 2022).
- Severity Ratings for Usability Problems. 1994. Available online: https://www.nngroup.com/articles/how-to-rate-the-severity-of-usability-problems/ (accessed on 5 September 2021).
- Quiñones, D.; Rusu, C. Applying a methodology to develop user eXperience heuristics. Comput. Stand. Interfaces 2019, 66, 103345. [Google Scholar] [CrossRef]






| Ref | Validation Process | Validation Result |
|---|---|---|
| [41] | Four evaluators evaluated an application by comparing Nielsen guidelines against the authors’ guidelines. | The authors’ guidelines were more effective than Nielsen’s since they discovered more usability issues (19 issues, 6 of them were severe) than Nielsen’s guidelines (15 issues, 5 of them were severe). |
| [42] | Six evaluators evaluated two applications by comparing Nielsen guidelines against the authors’ guidelines. | The author’s guidelines worked better than Nielsen’s since they discovered more usability issues (App1: 43, App2: 45) than Nielsen’s guidelines (App1: 28, App2: 24) |
| [43] | Two evaluators evaluated four animated agents through new guidelines. | The results showed which agent’s design was better. |
| [44] | Eighteen evaluators evaluated two Arabic applications by comparing the authors’ guidelines against Nielsen’s guidelines and game usability principles (two applications and three guidelines). | The author’s guidelines worked better than the others since they discovered more usability issues (Game1: 13, Game2: 12) than Nielsen (Game1: 6, Game2: 5) and the game usability principles (Game1: 10, Game2: 8). |
| Topic | Collected Information | Selected Information |
|---|---|---|
| Features | Features provided by [14] | Features of these studies are combined and |
| Features provided by [15] | summarized in Table 3. | |
| Features provided by [16] | ||
| Accessibility to elderly people | Selected. | |
| Accessibility by people with special needs | Selected. | |
| Attributes | Usability attributes proposed by ISO standard [46] (three attributes): effective, efficiency and satisfaction | Unselected. |
| Usability attributes proposed by Nielsen [47] (five attributes): learnability, efficiency, memorability, errors and satisfaction | Unselected. | |
| Usability attributes proposed by Harrison [48] (seven attributes): effective, efficiency, learnability, memorability, errors, satisfaction and cognitive load | Selected because it combines both attributes of ISO and Nielsen in addition to the cognitive load. | |
| Existing guidelines | Nielsen’s guidelines (10 guidelines) [11] | The set of Nielsen’s principles are selected. |
| Xcertia guidelines (five workgroups: privacy, security, content, usability and operability) [12] | The only selected workgroup is “usability” and discards all others since our focus is only on usability. | |
| HE4EH (25 guidelines) [6] | Select some checklists that cover the feature of self-monitoring in general and discard checklists that cannot be generalized to all chronic diseases. | |
| Telemedicine mobile application design recommendations [13] | All recommendations are selected. | |
| Elderly people guidelines (13 guidelines) [34] | Select the checklists that can be used for mHealth applications and discard the checklists that are specific to the mobile launchers. | |
| Intellectual disabilities guidelines (31 guidelines) [35] | Select the checklists that can be used for mHealth applications and discard the checklists that are specific to the eLearning systems. |
| No. | Features | Attributes | Nielsen | Xcertia |
|---|---|---|---|---|
| F1 | Booking appointment [16] | Efficiency and effectiveness | NH1 | XU5, XU6, UX8 |
| F2 | Consultation with HCP via text, voice messages and video calls [14,16] | Efficiency and effectiveness | NH1 | XU5 |
| F3 | Sharing data with HCP [14,15] | Memorability and efficiency | NH1, NH6 | XU5 |
| F4 | Access to personal health information [15] | Memorability, error, efficiency and effectiveness | NH1, NH5, NH6, NH9 | XU4, XU5, XU8 |
| F5 | Self-monitoring of chronic disease [14,15] | Learnability, cognitive load, efficiency and effectiveness | NH1, NH6 | XU6, XU8 |
| F6 | Allowing uploading and viewing of biometric measurements [14] | Memorability, error, efficiency and effectiveness | NH1, NH3, NH6 | XU3, XU6, XU8 |
| F7 | Graphic display of patient’s information [14] | Memorability, satisfaction, effectiveness and efficiency | NH2, NH4, NH6, NH8 | XU1, XU2, XU8 |
| F8 | Set health goals and treatment plan [14,15] | Satisfaction, learnability, cognitive load, effectiveness | NH1, NH2 | XU2 |
| F9 | Track health progress [15] | Memorability, efficiency and cognitive load | NH1 | XU5, XU6, XU8 |
| F10 | Reminders and notifications [14] | Memory and cognitive load | NH6 | XU6 |
| F11 | Health tips and motivation [14,15] | Satisfaction and effectiveness | NH2 | XU2 |
| F12 | Sharing health data with friends [15] | Satisfaction and learnability | - | - |
| F13 | Interactive prompts [14] | Learnability | NH10 | XU6, XU7 |
| F14 | Earn rewards [15] | Satisfaction | - | - |
| F15 | Bluetooth technology connection [14] | Efficiency and effectiveness | NH1 | XU5 |
| F16 | Accessibility to elderly people | Satisfaction, efficiency, effectiveness and memorability | - | XU9 |
| F17 | Accessibility by people with pecial needs | Satisfaction, efficiency, effectiveness and memorability | - | XU9 |
| ID | Guideline Name | Action | Covered Features | Applicability |
|---|---|---|---|---|
| NH1 | Visibility of system status | Adapt * | F1–F6, F8, F9, F15 | (3) Critical |
| NH2 | Match between system and the real world | Adapt * | F2, F7, F8, F11 | (2) Important |
| NH3 | User control and freedom | Adapt * | F1, F4, F5, F6 | (2) Important |
| NH4 | Consistency and standards | Adapt * | F7, F11 | (2) Important |
| NH5 | Error prevention | Adapt * | F5, F6 | (3) Critical |
| NH6 | Recognition rather than recall | Adapt * | F4, F5 | (2) Important |
| NH7 | Flexibility and efficiency of use | Adapt * | F3, F4, F5, F8 | (1) Useful |
| NH8 | Aesthetic and minimalist design | Adapt * | F4, F7 | (1) Useful |
| NH9 | Help users recognize, diagnose and recover from errors | Adapt * | F1, F4 | (3) Critical |
| NH10 | Help and documentation | Adapt * | F13 | (2) Important |
| ID | Guideline Name | Action | Covered Features | Applicability |
|---|---|---|---|---|
| XU1 | Visual design | Eliminate (the checklists were moved to Nielsen’s NH4, NH5 and NH6 guidelines) | F7 | - |
| XU2 | Readability | Eliminate (the checklists were moved to Nielsen’s NH8 guideline) | F7, F8, F11 | - |
| XU3 | App navigation | Eliminate (the checklists were moved to Nielsen’s NH3 guideline) | F6 | - |
| XU4 | Onboarding | Adapt * | F4 | (2) Important |
| XU5 | App feedback | Eliminate (the checklists were moved to Nielsen’s NH1 guideline) | F1–F4, F9, F15 | - |
| XU6 | Notifications, alerts and alarms | Adapt * | F1, F5, F6, F9, F10, F13 | (3) Critical |
| XU7 | Help resource and troubleshooting | Eliminate (the checklists were moved to Nielsen’s NH10 guideline) | F13 | - |
| XU8 | Historical data | Adapt * | F1, F2, F4–F7, F9 | (2) Important |
| XU9 | Accessibility | Adapt * | F16, F17 | (3) Critical |
| XU10 | Ongoing app evaluation | Keep (no change for this guideline) | F1–F17 | (2) Important |
| ID | Guideline Name | Action | Covered Features | Applicability |
|---|---|---|---|---|
| N1 | Interactivity and Motivations | Create (to cover F12 and F14 features since they are covered neither in Nielsen’s nor in the Xcertia guidelines.) | F12, F14 | (1) Useful |
| ID | Guideline Name |
|---|---|
| MHP1 | Visibility of system status |
| MHP2 | Match between system and the real world |
| MHP3 | User control and freedom |
| MHP4 | Consistency and standards |
| MHP5 | Error prevention |
| MHP6 | Recognition rather than recall |
| MHP7 | Flexibility and efficiency of use |
| MHP8 | Aesthetic and minimalist design |
| MHP9 | Error diagnosis and recovery |
| MHP10 | Help and documentation |
| MHP11 | Notifications, alerts and alarms |
| MHP12 | Onboarding |
| MHP13 | Historical data |
| MHP14 | Accessibility |
| MHP15 | Ongoing app evaluation |
| MHP16 | Interactivity and motivations |
| Sehhaty | Sokry | |
|---|---|---|
| Government/ Private | A government mHealth application that belongs to the Ministry of Health (MOH) in Saudi Arabia. | A private mHealth application. |
| Functionality | Provides different services, such as booking appointments, children’s vaccines, immediate consultations to make video and audio calls with doctors, COVID-19 services and reviewing health data, including insurance and registered information in MOH. | Helps users manage their diabetes by recording blood sugar readings, meals, exercises and medications. In addition, provides health advice related to diabetes. |
| Popularity | Popular with the people since it is connected with health records of MOH and considered an essential application for people in Saudi Arabia (+10 million downloads) [49]. | Less popular to the people (+50,000 downloads) [50]. |
| Rating | Description |
|---|---|
| 0 | I do not agree that this is a problem at all. |
| 1 | Cosmetic problem only. Need not be fixed unless extra time is available in the project. |
| 2 | Minor usability problem. Fixing this should be given low priority. |
| 3 | Major usability problem. Important to fix so it should be given high priority. |
| 4 | Usability catastrophes. Imperative to fix this before the product can be released. |
| ID | Guideline ID |
|---|---|
| Priority | (3) Critical, (2) Important or (1) Useful. |
| Name | Name of the guideline that resulted from the integration of Nielsen [11] and Xcertia [12]. |
| Definition | Identify the guideline and its purpose. |
| Features | The selected features covered by the guideline. |
| Checklists | The checklist items selected from [6,12,13,34,35] to add more details to the guideline and to make it more related to the features of mHealth applications and accessible to the elderly and people with special needs. |
| Sehhaty | Sokry | Total | |
|---|---|---|---|
| UGmHA | 73 | 95 | 168 |
| Xcertia | 22 | 28 | 50 |
| Nielsen | 17 | 25 | 42 |
| Sehhaty | Sokry | |||||
|---|---|---|---|---|---|---|
| Rating | UGmHA | Xcertia | Nielsen | UGmHA | Xcertia | Nielsen |
| No Problem | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Cosmetic | 7 (10%) | 2 (9%) | 0 (0%) | 6 (6%) | 2 (7%) | 0 (0%) |
| Minor | 10 (14%) | 1 (5%) | 0 (0%) | 17 (18%) | 4 (14%) | 2 (8%) |
| Major | 17 (23%) | 6 (27%) | 12 (71%) | 26 (27%) | 10 (36%) | 9 (36%) |
| Catastrophic | 39 (53%) | 13 (59%) | 5 (29%) | 46 (48%) | 12 (43%) | 14 (56%) |
| Total | 73 | 22 | 17 | 95 | 28 | 25 |
| ID | UGmHA | Corresponding Guideline (Nielsen) | Corresponding Guideline (Xcertia) |
|---|---|---|---|
| MHP1 | Visibility of system status | Visibility of system status | App feedback |
| MHP2 | Match between system and the real world | Match between system and the real world | - |
| MHP3 | User control and freedom | User control and freedom | App navigation |
| MHP4 | Consistency and standards | Consistency and standards | Visual design |
| MHP5 | Error prevention | Error prevention | Visual design |
| MHP6 | Recognition rather than recall | Recognition rather than recall | Visual design |
| MHP7 | Flexibility and efficiency of use | Flexibility and efficiency of use | - |
| MHP8 | Aesthetic and minimalist design | Aesthetic and minimalist design | Readability |
| MHP9 | Error diagnosis and recovery | Error diagnosis and recovery | - |
| MHP10 | Help and documentation | Help and documentation | Help resource and troubleshooting |
| MHP11 | Notifications, alerts and alarms | - | Notifications, alerts and alarms |
| MHP12 | Onboarding | - | Onboarding |
| MHP13 | Historical data | - | Historical data |
| MHP14 | Accessibility | - | Accessibility |
| MHP15 | Ongoing app evaluation | - | Ongoing app evaluation |
| MHP16 | Interactivity and Motivations | - | - |
| UGmHA | Xcertia | Nielsen | |
|---|---|---|---|
| Number of guidelines | 16 | 10 | 10 |
| Number of checklist items | 154 | 60 | 0 |
| Number of mHealth-specific checklist items | 44 | 6 | 0 |
| Number of accessibility checklist items | 18 | 7 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasr, E.; Alsaggaf, W.; Sinnari, D. Developing Usability Guidelines for mHealth Applications (UGmHA). Multimodal Technol. Interact. 2023, 7, 26. https://doi.org/10.3390/mti7030026
Nasr E, Alsaggaf W, Sinnari D. Developing Usability Guidelines for mHealth Applications (UGmHA). Multimodal Technologies and Interaction. 2023; 7(3):26. https://doi.org/10.3390/mti7030026
Chicago/Turabian StyleNasr, Eman, Wafaa Alsaggaf, and Doaa Sinnari. 2023. "Developing Usability Guidelines for mHealth Applications (UGmHA)" Multimodal Technologies and Interaction 7, no. 3: 26. https://doi.org/10.3390/mti7030026
APA StyleNasr, E., Alsaggaf, W., & Sinnari, D. (2023). Developing Usability Guidelines for mHealth Applications (UGmHA). Multimodal Technologies and Interaction, 7(3), 26. https://doi.org/10.3390/mti7030026