Enhancement of the Inner Foveal Response of Young Adults with Extended-Depth-of-Focus Contact Lens for Myopia Management

 ,
,  ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment
2.3. Protocol
2.4. Contact Lenses
2.5. Visual Acuity
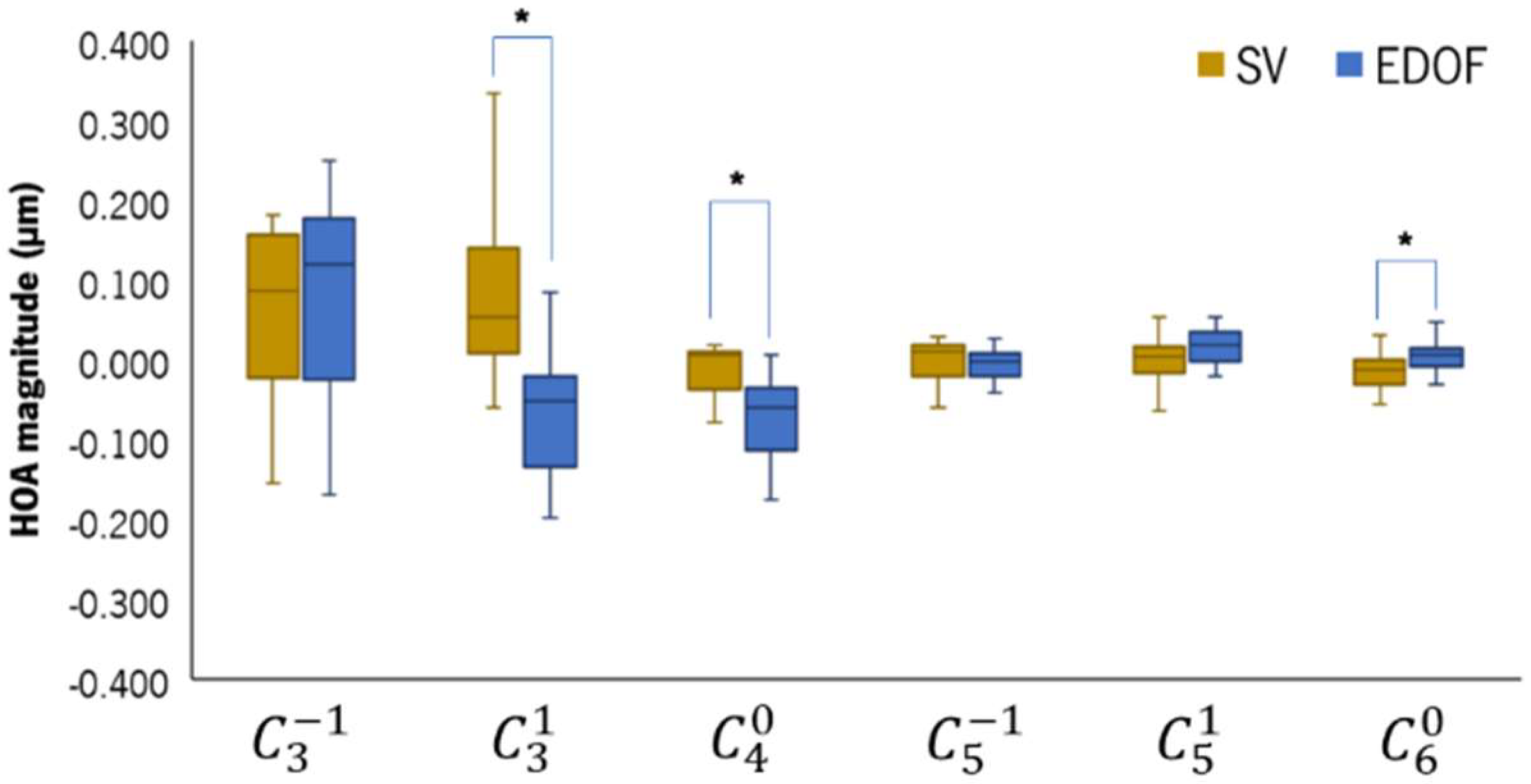
2.6. Aberrometry
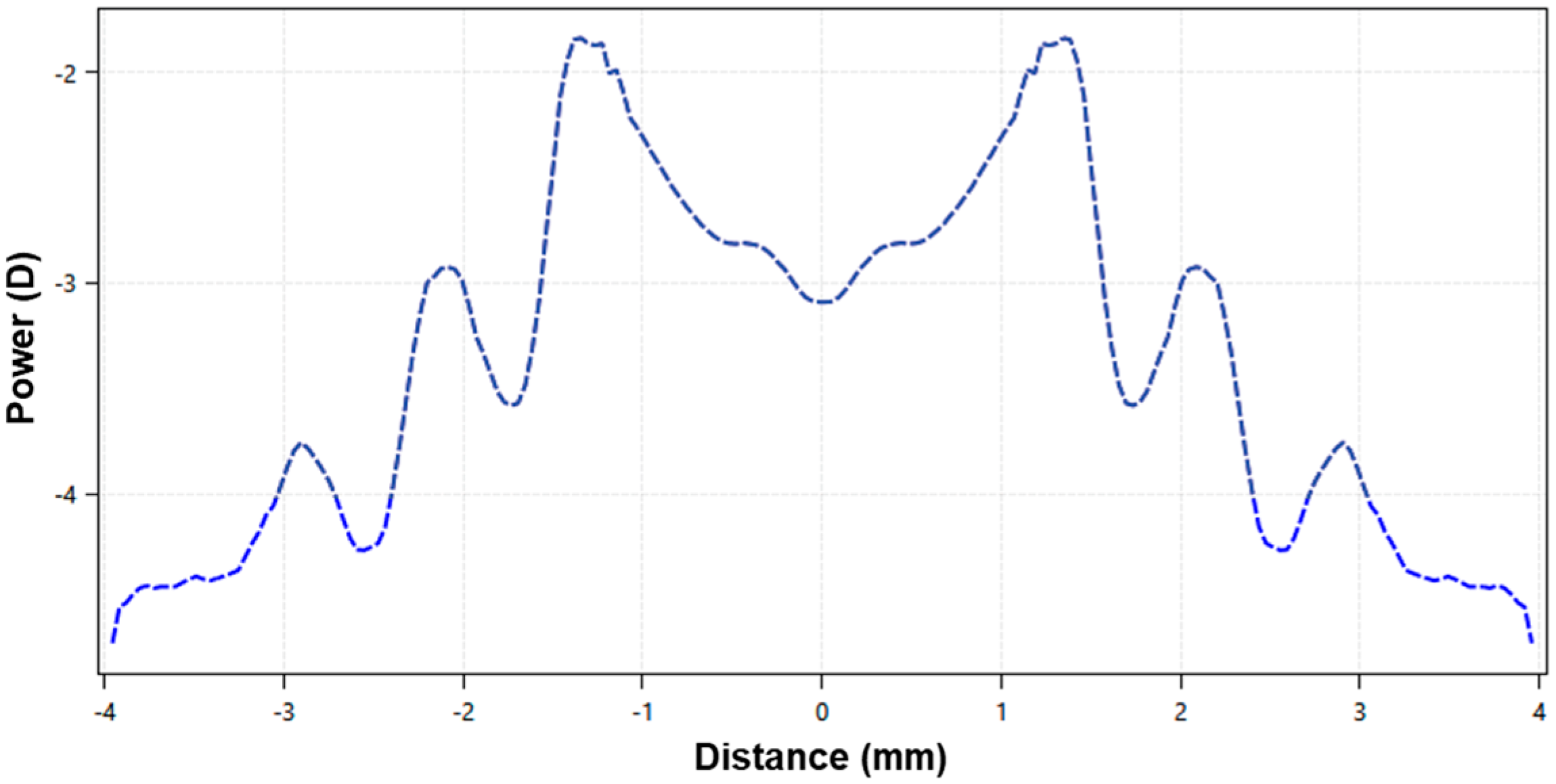
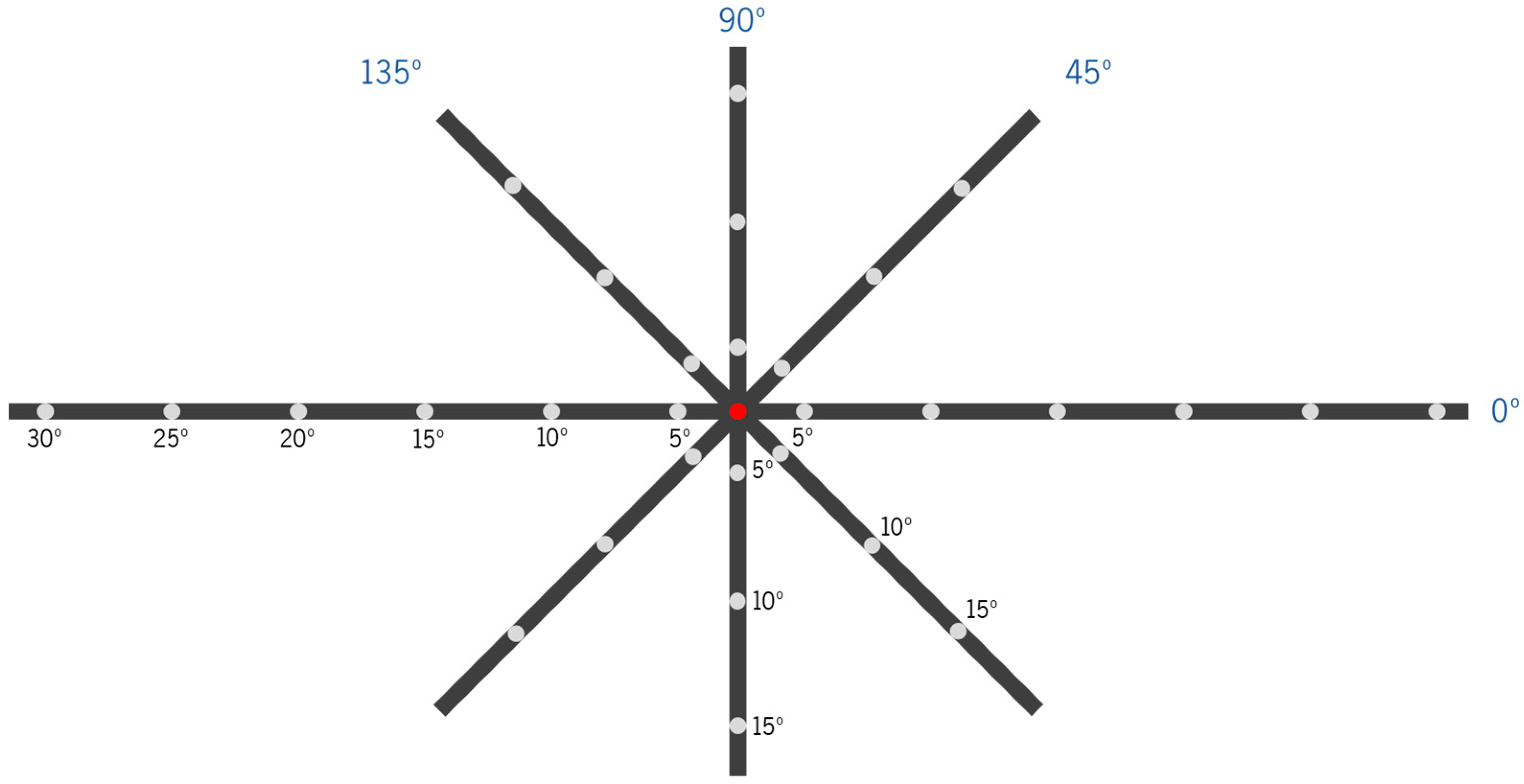
2.7. Peripheral Refraction
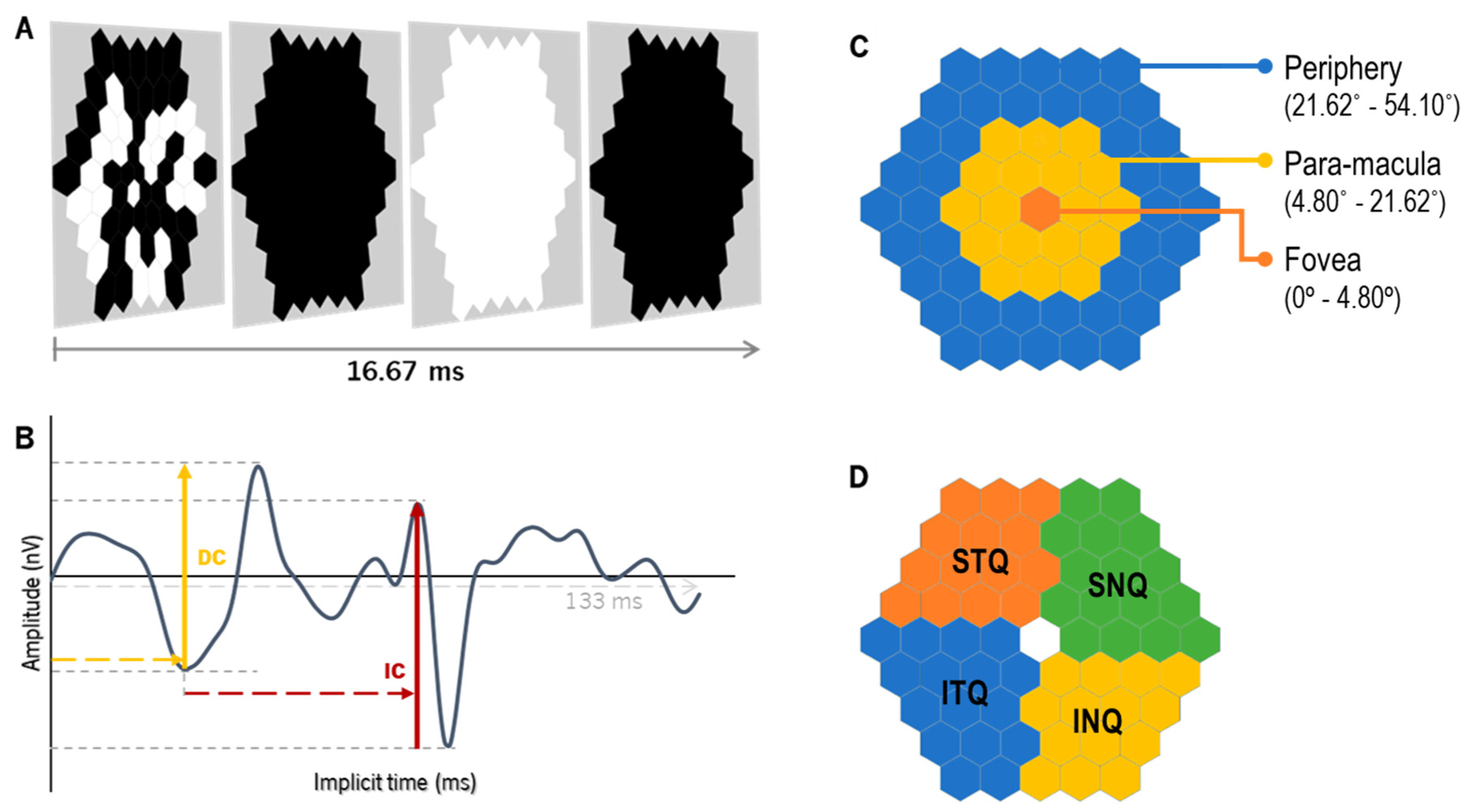
2.8. Electroretinography: Global-Flash Multifocal Electroretinogram
2.9. Statistics
3. Results
3.1. Sample Characteristics and Lens Centration
3.2. Visual Acuity (VA) and High-Order Aberrations (HOAs)
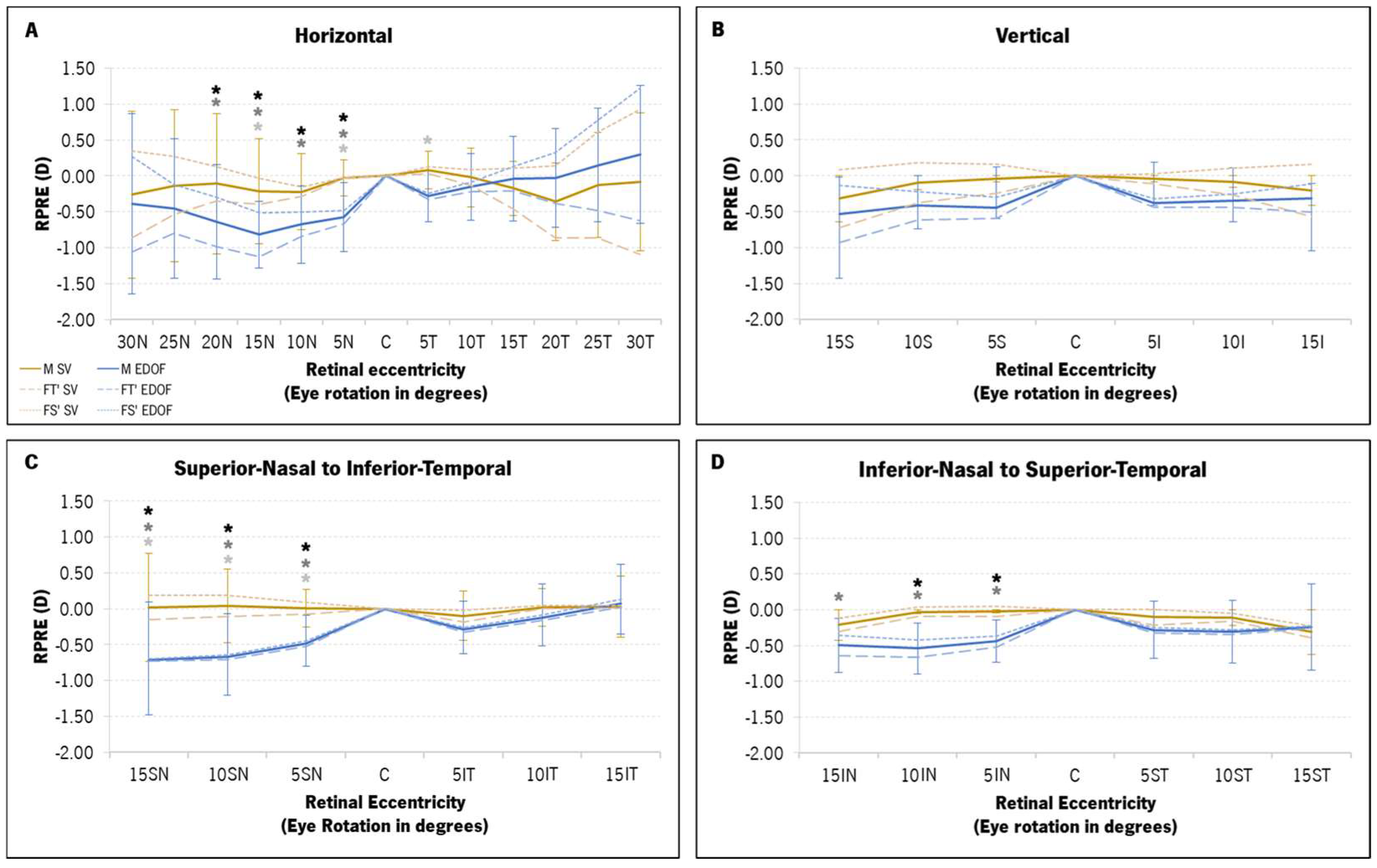
3.3. Peripheral Refraction
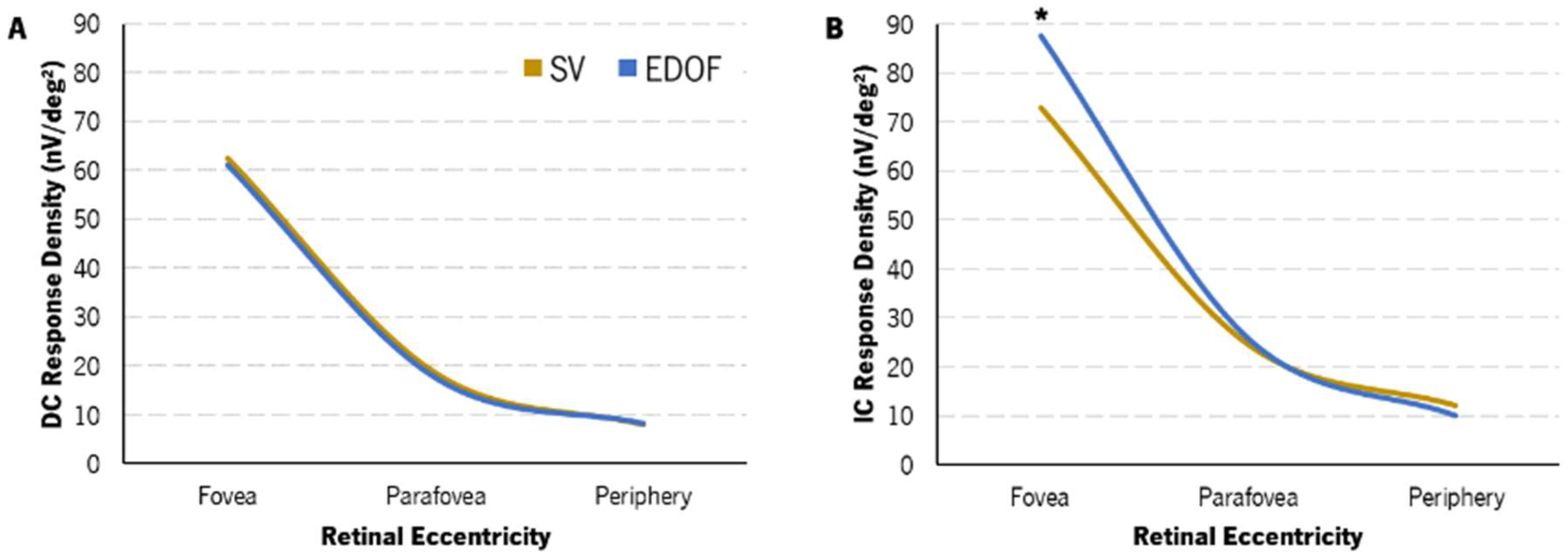
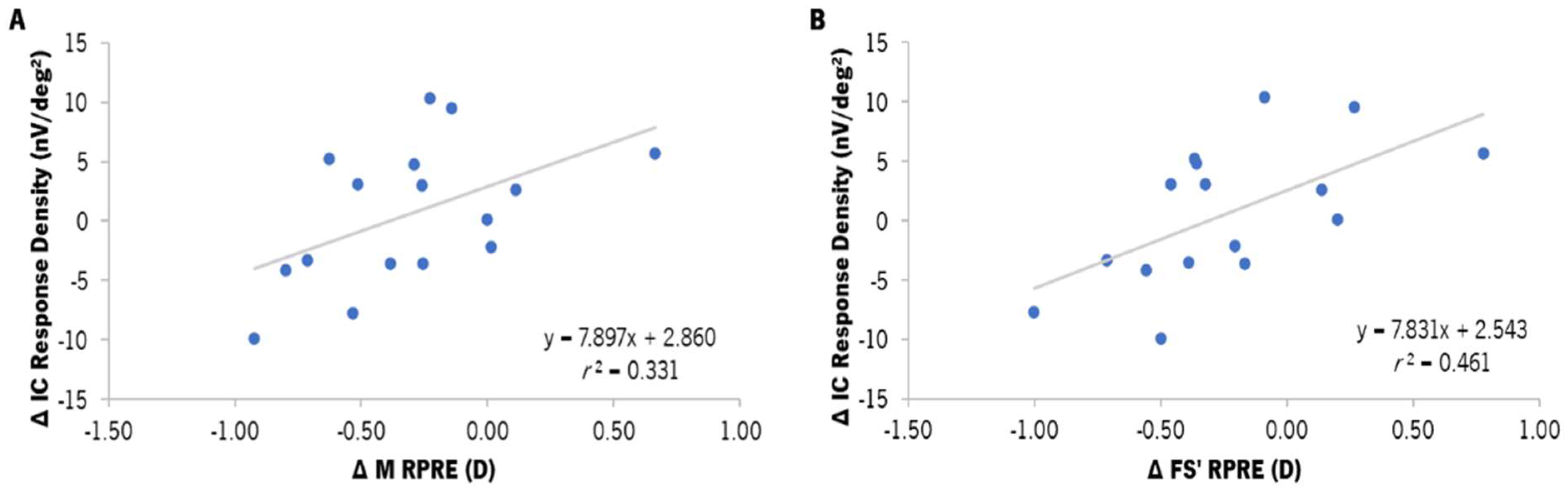
3.4. Global-Flash mfERG Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, J.; Wen, D.; Wang, Q.; McAlinden, C.; Flitcroft, I.; Chen, H.; Saw, S.M.; Chen, H.; Bao, F.; Zhao, Y.; et al. Efficacy comparison of 16 interventions for myopia control in children: A network meta-analysis. Ophthalmology 2016, 123, 697–708. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef] [PubMed]
- Sankaridurg, P. Contact lenses to slow progression of myopia. Clin. Exp. Optom. 2017, 100, 432–437. [Google Scholar] [CrossRef]
- Skidmore, K.V.; Tomiyama, E.S.; Rickert, M.E.; Richdale, K.; Kollbaum, P. Retrospective review of the effectiveness of orthokeratology versus soft peripheral defocus contact lenses for myopia management in an academic setting. Ophthalmic Physiol. Opt. 2023, 43, 534–543. [Google Scholar] [CrossRef]
- Tang, K.; Si, J.; Wang, X.; Lu, X.; Bi, H. Orthokeratology for Slowing Myopia Progression in Children: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eye Contact Lens. 2023, 49, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pomeda, A.; Pérez-Sánchez, B.; Valls, I.; Prieto-Garrido, F.L.; Gutiérrez-Ortega, R.; Villa-Collar, C. MiSight Assessment Study Spain (MASS). A 2-year randomized clinical trial. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1011–1021. [Google Scholar] [CrossRef]
- Chamberlain, P.; Peixoto-de-Matos, S.; Logan, N.; Ngo, C.; Jones, D.; Young, G. A 3-year Randomized Clinical Trial of MiSight Lenses for Myopia Control. Optom. Vis. Sci. 2019, 96, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, P.; Bradley, A.; Arumugam, B.; Hammond, D.; McNally, J.; Logan, N.S.; Jones, D.; Ngo, C.; Peixoto-de-Matos, S.C.; Hunt, C.; et al. Long-term Effect of Dual-Focus Contact Lenses on Myopia Progression in Children. Optom. Vis. Sci. 2022, 99, 204–212. [Google Scholar] [CrossRef]
- Sankaridurg, P.; Bakaraju, R.C.; Naduvilath, T.; Chen, X.; Weng, R.; Tilia, D.; Xu, P.; Li, W.; Conrad, F.; Smith, E.L., III; et al. Myopia control with novel central and peripheral plus contact lenses and extended depth of focus contact lenses: 2 year results from a randomised clinical trial. Ophthalmic Physiol. Opt. 2019, 39, 294–307. [Google Scholar] [CrossRef]
- Díaz-Gómez, S.; Burgos-Martínez, M.; Sankaridurg, P.; Urkia-Solorzano, A.; Carballo-Álvarez, J. Two-year myopia management efficacy of extended depth of focus soft contact lenses (MYLO) in Caucasian children. Am. J. Ophthalmol. 2023, 260, 122–131. [Google Scholar] [CrossRef]
- Lam, C.S.; Tang, W.C.; Tse, D.Y.; Tang, Y.Y.; To, C.H. Defocus Incorporated Soft Contact (DISC) lens slows myopia progression in Hong Kong Chinese schoolchildren: A 2-year randomised clinical trial. Br. J. Ophthalmol. 2014, 98, 40–45. [Google Scholar] [CrossRef] [PubMed]
- García-Marqués, J.V.; Macedo-De-Araújo, R.J.; Cerviño, A.; García-Lázaro, S.; McAlinden, C.; González-Méijome, J.M. Comparison of short-term light disturbance, optical and visual performance outcomes between a myopia control contact lens and a single-vision contact lens. Ophthalmic Physiol. Opt. 2020, 40, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Tilia, D.; Munro, A.; Chung, J.; Sha, J.; Delaney, S.; Kho, D.; Thomas, V.; Ehrmann, K.; Bakaraju, R.C. Short-term comparison between extended depth-of-focus prototype contact lenses and a commercially-available center-near multifocal. J. Optom. 2017, 10, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Redondo, B.; Vera, J.; Molina, R.; Galán, T.; Machado, P.; Jiménez, R. Changes in accommodation and behavioural performance with a contact lens for myopia management: A comparison between a dual-focus and a single-vision soft contact lens. Ophthalmic Physiol. Opt. 2022, 42, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, R.; na Park, H.; Hanif, A.M.; Sidhu, C.S.; Iuvone, P.M.; Pardue, M.T. ON pathway mutations increase susceptibility to form-deprivation myopia. Exp. Eye Res. 2015, 137, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Amorim-de-Sousa, A.; Schilling, T.; Fernandes, P.; Seshadri, Y.; Bahmani, H.; González-Méijome, J.M. Blue light blind-spot stimulation upregulates b-wave and pattern ERG activity in myopes. Sci. Rep. 2021, 11, 9273. [Google Scholar] [CrossRef] [PubMed]
- Schilling, T.; Amorim-de-Sousa, A.; Wong, N.A.; Bahmani, H.; González-Méijome, J.M.; Fernandes, P. Increase in b-wave amplitude after light stimulation of the blind spot is positively correlated with the axial length of myopic individuals. Sci. Rep. 2022, 12, 4785. [Google Scholar] [CrossRef]
- Chan, H.L.; Mohidin, N. Variation of multifocal electroretinogram with axial length. Ophthalmic Physiol. Opt. 2003, 23, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Kader, M.A. Electrophysiological study of myopia. Saudi J. Ophthalmol. 2012, 26, 91–99. [Google Scholar] [CrossRef]
- Flitcroft, D.I. Retinal dysfunction and refractive errors: An electrophysiological study of children. Br. J. Ophthalmol. 2005, 89, 484–488. [Google Scholar] [CrossRef]
- Pardue, M.T.; Faulkner, A.E.; Fernandes, A.; Yin, H.; Schaeffel, F.; Williams, R.W.; Pozdeyev, N.; Iuvone, P.M. High Susceptibility to Experimental Myopia in a Mouse Model with a Retinal ON Pathway Defect. Investig. Ophthalmol. Vis. Sci. 2008, 49, 706. [Google Scholar] [CrossRef] [PubMed]
- Luu, C.D.; Lau, A.M.; Lee, S.Y. Multifocal electroretinogram in adults and children with myopia. Arch. Ophthalmol. 2006, 124, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Li, S.Z.; Yu, W.Y.; Choi, K.Y.; Lam, C.H.; Lakshmanan, Y.; Wong, F.S.; Chan, H.H. Subclinical Decrease in Central Inner Retinal Activity Is Associated with Myopia Development in Children. Investig. Ophthalmol. Vis. Sci. 2017, 58, 4399–4406. [Google Scholar] [CrossRef] [PubMed]
- Palmowski, A.; Berninger, T.; Allgayer, R.; Andrielis, H.; Heinemann-Vernaleken, B.; Rudolph, G. Effects of refractive blur on the multifocal electroretinogram. Doc. Ophthalmol. 1999, 99, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.; Siu, A.W. Effect of optical defocus on multifocal ERG responses. Clin. Exp. Optom. 2003, 86, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Ho, W.C.; Wong, O.Y.; Chan, Y.C.; Wong, S.W.; Kee, C.S.; Chan, H.H.L. Sign-dependent changes in retinal electrical activity with positive and negative defocus in the human eye. Vision Res. 2012, 52, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Chin, M.P.; Chu, P.H.W.; Cheong, A.M.Y.; Chan, H.H.L. Human electroretinal responses to grating patterns and defocus changes by global flash multifocal electroretinogram. PLoS ONE 2015, 10, e0123480. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.M.Y.; Choi, K.Y.; Chan, H.H.L. The effect of simultaneous dual-focus integration on the global flash multifocal electroretinogram in the human eye. Ophthalmic Physiol. Opt. 2021, 41, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Delshad, S.; Collins, M.J.; Read, S.A.; Vincent, S.J. The time course of the onset and recovery of axial length changes in response to imposed defocus. Sci. Rep. 2020, 10, 8322. [Google Scholar] [CrossRef]
- Amorim-de-Sousa, A.; Moreira, L.; Macedo-de-Araújo, R.; Amorim, A.; Jorge, J.; Fernandes, P.R.; Queirós, A.; González-Méijome, J.M. Impact of contact lens materials on the mfERG response of the human retina. Doc. Ophthalmol. 2020, 140, 103–113. [Google Scholar] [CrossRef]
- Thibos, L.N.; Horner, D. Power vector analysis of the optical outcome of refractive surgery. J. Cataract. Refract. Surg. 2001, 27, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Queirós, A.; Lopes-Ferreira, D.; González-Méijome, J.M. Astigmatic Peripheral Defocus with Different Contact Lenses: Review and Meta-Analysis. Curr. Eye Res. 2016, 41, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Miguel-Jiménez, J.M.; Ortega, S.; Boquete, L.; Rodríguez-Ascariz, J.M.; Blanco, R. Multifocal ERG wavelet packet decomposition applied to glaucoma diagnosis. Biomed. Eng. Online 2011, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.B.; Bach, M.; Kondo, M.; Li, S.; Walker, S.; Holopigian, K.; Viswanathan, S.; Robson, A.G. ISCEV standard for clinical multifocal electroretinography (mfERG) (2021 update). Doc. Ophthalmol. 2021, 142, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.C.; Bach, M.; Brigell, M.; Keating, D.; Kondo, M.; Lyons, J.S.; Marmor, M.F.; McCulloch, D.L.; Palmowski-Wolfe, A.M.; for the International Society For Clinical Electrophysiology of Vision. ISCEV standard for clinical multifocal electroretinography (mfERG) (2011 edition). Doc. Ophthalmol. 2012, 124, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Queirós, A.; Pereira-Da-mota, A.F.; Costa, J.; Amorim-De-sousa, A.; Fernandes, P.R.B.; González-Méijome, J.M. Retinal response of low myopes during orthokeratology treatment. J. Clin. Med. 2020, 9, 2649. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, P.R.; Ferreira, C.; Domingues, J.; Amorim-de-Sousa, A.; Faria-Ribeiro, M.; Queirós, A.; González-Meijome, J.M. Short-term delay in neural response with multifocal contact lens might start at the retinal level. Doc. Ophthalmol. 2022, 145, 37–51. [Google Scholar] [CrossRef]
- Anstice, N.S.; Phillips, J.R. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology 2011, 118, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Mojumder, D.; Wensel, T. Topical mydriatics affect light-evoked retinal responses in anesthetized mice. Investig. Ophthalmol. Vis. Sci. 2010, 51, 567–576. [Google Scholar] [CrossRef][Green Version]
- Mazinani, B.A.E.; Repas, T.; Weinberger, A.W.A.; Vobig, M.A.; Walter, P. Amplitude calculation in multifocal ERG: Comparison of repeatability in 30 Hz flicker and first order kernel stimulation. Graefes Arch. Clin. Exp. Ophthalmol. 2007, 245, 338–344. [Google Scholar] [CrossRef]
- Flitcroft, D.I. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog. Retin Eye Res. 2012, 31, 622–660. [Google Scholar] [CrossRef]
- Luu, C.D.; Foulds, W.S.; Tan, D.T. Features of the multifocal electroretinogram may predict the rate of myopia progression in children. Ophthalmology 2007, 114, 1433–1438. [Google Scholar] [CrossRef]
- Ho, W.C.; Kee, C.S.; Chan, H.H. Myopia progression in children is linked with reduced foveal mfERG response. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5320–5325. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Venkataraman, A.P.; Winter, S.; Unsbo, P.; Lundström, L. Blur adaptation: Contrast sensitivity changes and stimulus extent. Vis. Res. 2015, 110, 100–106. [Google Scholar] [CrossRef]
- Venkataraman, A.P.; Radhakrishnan, A.; Dorronsoro, C.; Lundström, L.; Marcos, S. Role of parafovea in blur perception. Vis. Res. 2017, 138, 59–65. [Google Scholar] [CrossRef]
- Webster, S.M.; Webster, M.A.; Taylor, J.; Jaikumar, J.; Verma, R. Simultaneous blur contrast. In Human Vision and Electronic Imaging VI; Rogowitz, B.E., Pappas, T.N., Eds.; Society of Photo-Optical Instrumentation Engineers (SPIE) Conference Series; SPIE: Bellingham, WA, USA, 2001; Volume 4299, pp. 414–422. [Google Scholar]
- Panorgias, A.; Aigbe, S.; Jeong, E.; Otero, C.; Bex, P.J.; Vera-Diaz, F.A. Retinal Responses to Simulated Optical Blur Using a Novel Dead Leaves ERG Stimulus. Investig. Ophthalmol. Vis. Sci. 2021, 62, 1. [Google Scholar] [CrossRef]
- Thibos, L.N.; Bradley, A.; Liu, T.; López-Gil, N. Spherical aberration and the sign of defocus. Optom. Vis. Sci. 2013, 90, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Belenky, M.; Sollars, P.; Pickard, G.; McMahon, D. Melanopsin mediates retrograde visual signaling in the retina. PLoS ONE 2012, 7, e42647. [Google Scholar] [CrossRef] [PubMed]
- Mani, A.; Schwartz, G.W. Circuit Mechanisms of a Retinal Ganglion Cell with Stimulus-Dependent Response Latency and Activation Beyond Its Dendrites. Curr. Biol. 2017, 27, 471–482. [Google Scholar] [CrossRef]
- Turnbull, P.R.K.; Goodman, L.K.; Phillips, J.R. Global-flash mfERG responses to local differences in spherical and astigmatic defocus across the human retina. Ophthalmic Physiol. Opt. 2020, 40, 24–34. [Google Scholar] [CrossRef]
- Singh, N.K.; Meyer, D.; Jaskulski, M.; Kollbaum, P. Retinal defocus in myopes wearing dual-focus zonal contact lenses. Ophthalmic Physiol. Opt. 2022, 42, 8–18. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SV | EDOF | |
|---|---|---|
| Optical design | Spherical | Extended-depth-of-focus |
| Substitution | Monthly | |
| Material | Filcon 5B (Silicone hydrogel) | |
| Hydration (%) | 75 | |
| DK/t | 50 | |
| Diameter (mm) | 13.00–16.00 (0.50 steps) | 13.50–15.50 (0.50 steps) |
| Radius (mm) | 6.80–9.80 (0.30 steps) | 7.10–9.80 (0.30 steps) |
| Eyes (N) | 16 |
|---|---|
| Gender (no. of eyes) | 3 male/13 female |
| Age (years) | 27.5 ± 5.7 [18.9–38.4] |
| M (D) | −3.09 ± 1.50 |
| J0 (D) | 0.03 ± 0.16 |
| J45 (D) | −0.03 ± 0.15 |
| kflat (mm) | 7.86 ± 0.21 |
| ksteep (mm) | 7.70 ± 0.22 |
| kmean (mm) | 7.78 ± 0.21 |
| HDVI (mm) | 11.70 ± 0.25 |
| HCVA (LogMAR) | LCVA (LogMAR) | |||
|---|---|---|---|---|
| Monocular | Binocular | Monocular | Binocular | |
| SV | −0.10 [0.01] | −0.13 [0.00] | 0.16 [0.02] | 0.06 [0.00] |
| EDOF | −0.03 [0.01] | −0.08 [0.01] | 0.34 [0.01] | 0.21 [0.01] |
| p-value | 0.005 * | 0.003 * | 0.001 * | 0.001 * |
| DC (nV/deg2) | SV | EDOF | p | |
|---|---|---|---|---|
| SUM | 9.63 [11.14–7.83] | 9.71 [11.18–8.81] | 0.776 | |
| Eccentricity | Fovea | 62.50 [73.87–53.15] | 61.08 [74.42–50.37] | 0.703 |
| Para-macula | 18.62 [22.26–15.26] | 17.62 [19.78–15.72] | 0.819 | |
| Periphery | 8.11 [9.28–7.28] | 8.31 [9.85–7.32] | 0.964 | |
| p | <0.001 * | |||
| Quadrants | INQ | 9.64 [13.89–8.48] | 10.55 [11.95–9.32] | 0.986 |
| SNQ | 8.28 [10.41–7.34] | 9.05 [10.53–8.15] | 0.667 | |
| STQ | 9.22 [12.37–7.83] | 9.79 [10.64–7.95] | 0.663 | |
| ITQ | 10.75 [12.24–9.05] | 11.03 [12.69–8.65] | 0.858 | |
| p | 0.363 | |||
| IC (nV/deg2) | SV | EDOF | p | |
|---|---|---|---|---|
| SUM | 11.13 [11.86–8.25] | 11.07 [11.95–7.29] | 0.069 | |
| Eccentricity | Fovea | 73.00 [99.58–64.77] | 87.62 [100.35–70.00] | 0.036 * |
| Para-macula | 24.52 [30.26–21.40] | 25.79 [30.48–21.91] | 0.943 | |
| Periphery | 12.03 [12.86–10.30] | 10.04 [12.63–9.21] | 0.930 | |
| p | <0.001 * | |||
| Quadrants | INQ | 11.53 [14.58–8.82] | 11.80 [14.15–8.59] | 0.811 |
| SNQ | 9.79 [10.86–6.95] | 7.37 [10.20–6.41] | 0.492 | |
| STQ | 11.22 [13.74–8.93] | 10.86 [13.59–8.10] | 0.673 | |
| ITQ | 12.31 [15.59–8.49] | 10.51 [13.74–8.95] | 0.285 | |
| p | 0.018 * | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amorim-de-Sousa, A.; Macedo-de-Araújo, R.J.; Fernandes, P.; González-Méijome, J.M.; Queirós, A. Enhancement of the Inner Foveal Response of Young Adults with Extended-Depth-of-Focus Contact Lens for Myopia Management. Vision 2024, 8, 19. https://doi.org/10.3390/vision8020019
Amorim-de-Sousa A, Macedo-de-Araújo RJ, Fernandes P, González-Méijome JM, Queirós A. Enhancement of the Inner Foveal Response of Young Adults with Extended-Depth-of-Focus Contact Lens for Myopia Management. Vision. 2024; 8(2):19. https://doi.org/10.3390/vision8020019
Chicago/Turabian StyleAmorim-de-Sousa, Ana, Rute J. Macedo-de-Araújo, Paulo Fernandes, José M. González-Méijome, and António Queirós. 2024. "Enhancement of the Inner Foveal Response of Young Adults with Extended-Depth-of-Focus Contact Lens for Myopia Management" Vision 8, no. 2: 19. https://doi.org/10.3390/vision8020019
APA StyleAmorim-de-Sousa, A., Macedo-de-Araújo, R. J., Fernandes, P., González-Méijome, J. M., & Queirós, A. (2024). Enhancement of the Inner Foveal Response of Young Adults with Extended-Depth-of-Focus Contact Lens for Myopia Management. Vision, 8(2), 19. https://doi.org/10.3390/vision8020019