
Low Molecular Weight Hyaluronic Acid (500–730 Kda) Injections in Tendinopathies—A Narrative Review



Abstract
:1. Introduction
- Low molecular weight: <1000 KDa;
- Medium molecular weight: 1000 KDa < MW < 2000 KDa;
- High molecular weight: >2000 KDa.
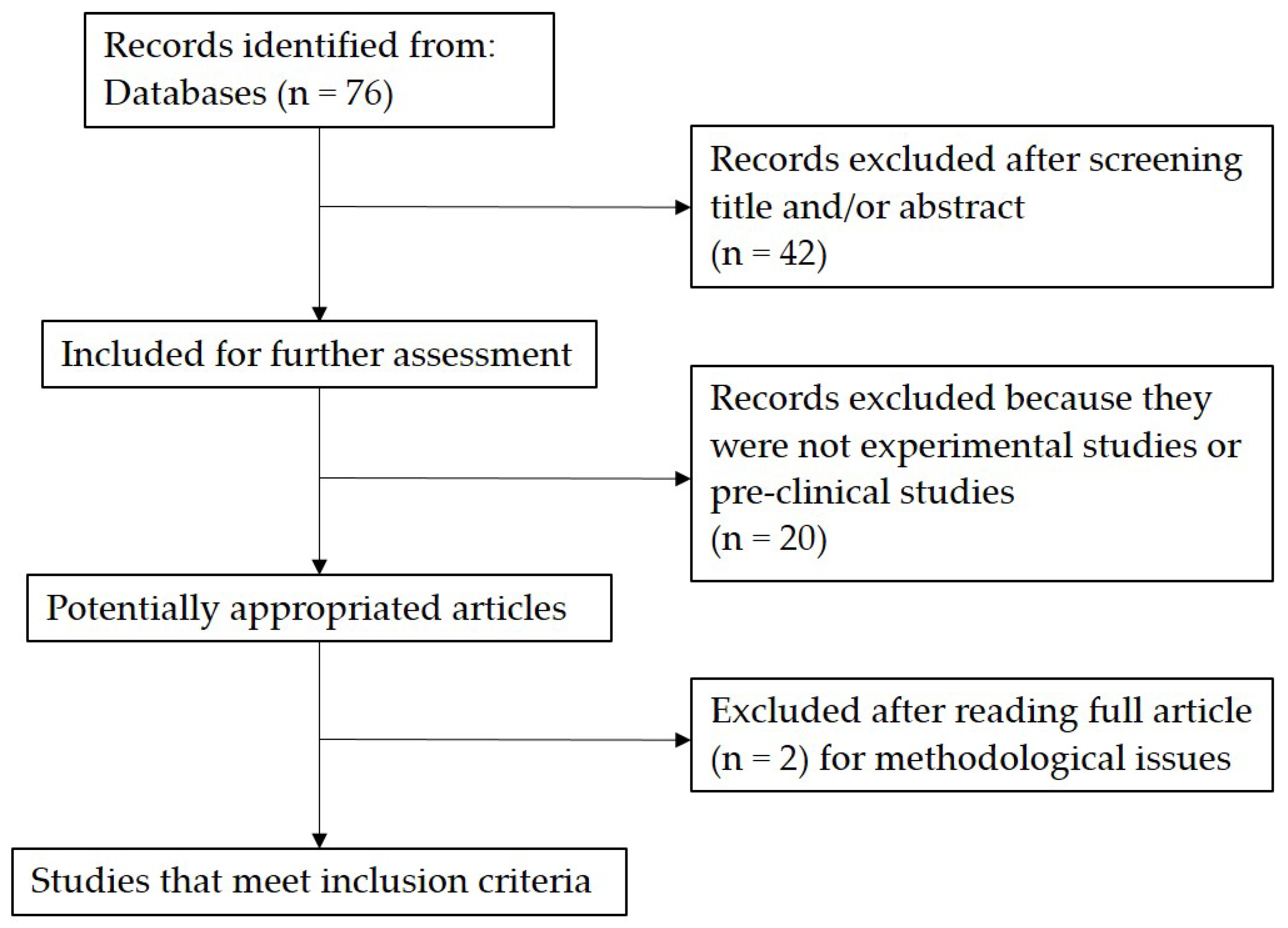
2. Materials and Methods
Study Selection
3. Results
3.1. In Vitro Studies
3.2. Pre-Clinical Studies
3.3. Clinical Studies
4. Discussion
5. Conclusions
6. Limitations of the Review
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Challoumas, D.; Biddle, M.; Millar, N.L. Recent advances in tendinopathy. Fac. Rev. 2020, 9, 16. [Google Scholar] [CrossRef]
- Merolla, G.; Singh, S.; Paladini, P.; Porcellini, G. Calcific tendinitis of the rotator cuff: State of the art in diagnosis and treatment. J. Orthop. Traumatol. 2016, 17, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmento, M. Long head of biceps: From anatomy to treatment. Acta Reum. Port. 2014, 40, 26–33. [Google Scholar]
- Patrick, N.C.; Hammert, W.C. Hand and Wrist Tendinopathies. Clin. Sports Med. 2020, 39, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Sirico, F.; Palermi, S.; Massa, B.; Corrado, B. Tendinopathies of the hip and pelvis in athletes: A narrative review. J. Hum. Sports Exerc. 2020, 15, S748–S762. [Google Scholar] [CrossRef]
- Tarantino, D.; Palermi, S.; Sirico, F.; Balato, G.; D’Addona, A.; Corrado, B. Achilles tendon pathologies: How to choose the best treatment. J. Hum. Sport Exerc. 2020, 15, S1300–S1321. [Google Scholar]
- Simpson, M.R.; Howard, T.M. Tendinopathies of the foot and ankle. Am. Fam. Physician 2009, 80, 1107–1114. [Google Scholar] [PubMed]
- Sharma, P.; Maffulli, N. Basic biology of tendon injury and healing. Surgeon 2005, 3, 309–316. [Google Scholar] [CrossRef]
- Waldecker, U.; Hofmann, G.; Drewitz, S. Epidemiologic investigation of 1394 feet: Coincidence of hindfoot malalignment and Achilles tendon disorders. Foot Ankle Surg. 2012, 18, 119–123. [Google Scholar] [CrossRef]
- Riley, G.P.; Curry, V.; DeGroot, J.; van El, B.; Verzijl, N.; Hazleman, B.L.; Bank, R.A. Matrix metalloproteinase activities and their relationship with collagen remodelling in tendon pathology. Matrix Biol. 2002, 21, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, F.; Papalia, R.; Paciotti, M.; Franceschetti, E.; Di Martino, A.; Maffulli, N.; Denaro, V. Obesity as a Risk Factor for Tendinopathy: A Systematic Review. Int. J. Endocrinol. 2014, 2014, 670262. [Google Scholar] [CrossRef]
- Longo, U.G.; Ronga, M.; Maffulli, N. Achilles tendinopathy. Sports Med. Arthrosc. Rev. 2009, 17, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Oliva, F.; Piccirilli, E.; Berardi, A.C.; Frizziero, A.; Tarantino, U.; Maffulli, N. Hormones and tendinopathies: The current evidence. Br. Med Bull. 2016, 117, 39–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frizziero, A.; Vittadini, F.; Gasparre, G.; Masiero, S. Impact of oestrogen deficiency and aging on tendon: Concise review. Muscle Ligaments Tendons J. 2019, 4, 324–328. [Google Scholar] [CrossRef]
- Maffulli, N.; Reaper, J.A.; Waterston, S.W.; Ahya, R. ABO Blood Groups and Achilles Tendon Rupture in the Grampian Region of Scotland. Clin. J. Sport Med. 2000, 10, 269–271. [Google Scholar] [CrossRef]
- Maffulli, N.; Sharma, P.; Luscombe, K.L. Achilles tendinopathy: Aetiology and management. J. R. Soc. Med. 2004, 97, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Frizziero, A.; Fini, M.; Salamanna, F.; Veicsteinas, A.; Maffulli, N.; Marini, M. Effect of training and sudden detraining on the patellar tendon and its enthesis in rats. BMC Musculoskelet. Disord. 2011, 12, 20. [Google Scholar] [CrossRef]
- van der Linden, P.D.; Sturkenboom, M.C.J.M.; Herings, R.M.C.; Leufkens, H.M.G.; Rowlands, S.; Stricker, B.H.C. Increased risk of achilles tendon rupture with quinolone antibacterial use, especially in elderly patients taking oral corticosteroids. Arch. Intern. Med. 2003, 163, 1801–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisaccia, D.R.; Aicale, R.; Tarantino, D.; Peretti, G.; Maffulli, N. Biological and chemical changes in fluoroquinolone-associated tendinopathies: A systematic review. Br. Med Bull. 2019, 130, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Di Meglio, F.; Sacco, A.M.; Belviso, I.; Romano, V.; Sirico, F.; Loiacono, C.; Palermi, S.; Pempinello, C.; Montagnani, S.; Nurzynska, D.; et al. Influence of Supplements and Drugs used for the Treatment of Musculoskeletal Disorders on Adult Human Tendon-Derived Stem Cells. Muscle Ligaments Tendons J. 2020, 10, 376. [Google Scholar] [CrossRef]
- Romero, E.A.S.; Pollet, J.; Pérez, S.M.; Pérez, J.L.A.; Fernández, A.C.M.; Pedersini, P.; Carballar, C.B.; Villafañe, J.H. Lower Limb Tendinopathy Tissue Changes Assessed through Ultrasound: A Narrative Review. Medicina 2020, 56, 378. [Google Scholar] [CrossRef] [PubMed]
- Ker, R.F. Dynamic tensile properties of the plantaris tendon of sheep (Ovisaries). J. Exp. Biol. 1981, 93, 283–302. [Google Scholar] [CrossRef]
- Cook, J.L.; Purdam, C.R. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br. J. Sports Med. 2009, 43, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frizziero, A.; Bonsangue, V.; Trevisan, M.; Ames, P.R.J.; Masiero, S. Foot tendinopathies in rheumatic diseases: Etiopathogenesis, clinical manifestations and therapeutic options. Clin. Rheumatol. 2012, 32, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Aicale, R.; Bisaccia, R.D.; Oliviero, A.; Oliva, F.; Maffulli, N. Current pharmacological approaches to the treatment of tendinopathy. Expert Opin. Pharmacother. 2020, 21, 1467–1477. [Google Scholar] [CrossRef]
- Frizziero, A.; Vittadini, F.; Fusco, A.; Giombini, A.; Masiero, S. Efficacy of eccentric exercise for lower limb tendinopathies in athletes. J. Sports Med. Phys. Fit. 2015, 56, 1352–1358. [Google Scholar]
- Frizziero, A.; Trainito, S.; Oliva, F.; Aldini, N.N.; Masiero, S.; Maffulli, N. The role of eccentric exercise in sport injuries rehabilitation. Br. Med Bull. 2014, 110, 47–75. [Google Scholar] [CrossRef] [Green Version]
- Frizziero, A.; Vittadini, F.; Barazzuol, M.; Gasparre, G.; Finotti, P.; Meneghini, A.; Maffulli, N.; Masiero, S. Extracorporeal shockwaves therapy versus hyaluronic acid injection for the treatment of painful non-calcific rotator cuff tendinopathies: Preliminary results. J. Sports Med. Phys. Fit. 2017, 57, 1162–1168. [Google Scholar] [CrossRef] [PubMed]
- Galletti, S.; Oliva, F.; Masiero, S.; Frizziero, A.; Galletti, R.; Schiavone, C.; Salini, V.; Abate, M. Sonoelastography in the diagnosis of tendinopathies: An added value. Muscle Ligaments Tendons J. 2015, 5, 325–330. [Google Scholar] [CrossRef]
- Frizziero, A.; Vittadini, F.; Bigliardi, D.; Costantino, C. The Role of Hyaluronic Acid Injection for the Treatment of Tendinopathy. Muscle Ligaments Tendons J. 2020, 10, 548. [Google Scholar] [CrossRef]
- Collins, T.; Alexander, D.; Barkatali, B. Platelet-rich plasma: A narrative review. EFORT Open Rev. 2021, 6, 225–235. [Google Scholar] [CrossRef]
- Kakkos, G.A.; Klontzas, M.E.; Koltsakis, E.; Karantanas, A.H. US-guided high-volume injection for Achilles tendinopathy. J. Ultrason. 2021, 21, e127–e133. [Google Scholar] [CrossRef]
- Arias-Vázquez, P.I.; Tovilla-Zárate, C.A.; González-Graniel, K.; Burad-Fonz, W.; González-Castro, T.B.; López-Narváez, M.L.; Castillo-Avila, R.G.; Arcila-Novelo, R. Efficacy of hypertonic dextrose infiltrations for pain control in rotator cuff tendinopathy: Systematic review and meta-analysis. Acta Reum. Port. 2021, 46, 156–170. [Google Scholar]
- Morath, O.; Beck, M.; Taeymans, J.; Hirschmüller, A. Sclerotherapy and prolotherapy for chronic patellar tendinopathies—A promising therapy with limited available evidence, a systematic review. J. Exp. Orthop. 2020, 7, 1–11. [Google Scholar] [CrossRef]
- Von Wehren, L.; Pokorny, K.; Blanke, F.; Sailer, J.; Majewski, M. Injection with autologous conditioned serum has better clinical results than eccentric training for chronic Achilles tendinopathy. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2744–2753. [Google Scholar] [CrossRef]
- Fernández, A.C.M.; Carballar, C.B.; Villafañe, J.H.; Pérez, M.M.; Pérez, J.L.; Díaz-Meco, R.; Jiménez, D.G.; Romero, E.A.S. A new ultrasound-guided percutaneous electrolysis and exercise treatment in patellar tendinopathy: Three case reports. Front. Biosci. 2021, 26, 1166–1175. [Google Scholar]
- Necas, J.; Bartosikova, L.; Brauner, P.; Kolar, J. Hyaluronic acid (hyaluronan): A review. Vet. Med. 2008, 53, 397–411. [Google Scholar] [CrossRef] [Green Version]
- Kaux, J.-F.; Samson, A.; Crielaard, J.-M. Hyaluronic acid and tendon lesions. Muscle Ligaments Tendons J. 2015, 5, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Altman, R.; Hackel, J.; Niazi, F.; Shaw, P.; Nicholls, M. Efficacy and safety of repeated courses of hyaluronic acid injections for knee osteoarthritis: A systematic review. Semin. Arthritis Rheum. 2018, 48, 168–175. [Google Scholar] [CrossRef]
- Frizziero, A.; Maffulli, N.; Masiero, S.; Frizziero, L. Six-months pain relief and functional recovery after intra-articular injections with hyaluronic acid (mw 500–730 KDa) in trapeziometacarpal osteoarthritis. Muscle Ligaments Tendons J. 2019, 4, 256–261. [Google Scholar] [CrossRef]
- Foti, C.; Cisari, C.; Carda, S.; Giordan, N.; Rocco, A.; Frizziero, A.; Della Bella, G. A prospective observational study of the clinical efficacy and safety of intra-articular sodium hyaluronate in synovial joints with osteoarthritis. Eur. J. Phys. Rehabil. Med. 2011, 47, 407–415. [Google Scholar]
- Frizziero, A.; Vittadini, F.; Oliva, F.; Abatangelo, G.; Bacciu, S.; Berardi, A. IS Mu. LT Hyaluronic acid injections in musculoskeletal disorders guidelines. Muscles Ligaments Tendons J. 2018, 8, 364–398. [Google Scholar] [CrossRef] [Green Version]
- Osti, L.; Berardocco, M.; Di Giacomo, V.; Di Bernardo, G.; Oliva, F.; Berardi, A.C. Hyaluronic acid increases tendon derived cell viability and collagen type I expression in vitro: Comparative study of four different Hyaluronic acid preparations by molecular weight. BMC Musculoskelet. Disord. 2015, 16, 284, Erratum in BMC Musculoskelet Disord. 2015, 16, 334. [Google Scholar] [CrossRef] [Green Version]
- Gallorini, M.; Berardi, A.C.; Berardocco, M.; Gissi, C.; Maffulli, N.; Cataldi, A.; Oliva, F. Hyaluronic acid increases tendon derived cell viability and proliferation in vitro: Comparative study of two different hyaluronic acid preparations by molecular weight. Muscle Ligaments Tendons J. 2017, 7, 208–214. [Google Scholar] [CrossRef]
- Salamanna, F.; Frizziero, A.; Pagani, S.; Giavaresi, G.; Curzi, D.; Falcieri, E.; Marini, M.; Abruzzo, P.M.; Martini, L.; Fini, M. Metabolic and cytoprotective effects ofin vivoperi-patellar hyaluronic acid injections in cultured tenocytes. Connect. Tissue Res. 2014, 56, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, A.; Salamanna, F.; Giavaresi, G.; Ferrari, A.; Martini, L.; Marini, M.; Veicsteinas, A.; Maffulli, N.; Masiero, S.; Fini, M.; et al. Hyaluronic acid injections protect patellar tendon from detraining-associated damage. Histol. Histopathol. 2015, 30, 1079–1088. [Google Scholar] [CrossRef]
- Meloni, F.; Milia, F.; Cavazzuti, M.; Doria, C.; Lisai, P.; Profili, S.; Meloni, G. Clinical evaluation of sodium hyaluronate in the treatment of patients with sopraspinatus tendinosis under echographic guide: Experimental study of periarticular injections. Eur. J. Radiol. 2008, 68, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Blaine, T.; Moskowitz, R.; Udell, J.; Skyhar, M.; Levin, R.; Friedlander, J.; Daley, M.; Altman, R. Treatment of Persistent Shoulder Pain with Sodium Hyaluronate: A Randomized, Controlled Trial. J. Bone Jt. Surg.-Am. Vol. 2008, 90, 970–979. [Google Scholar] [CrossRef]
- Fogli, M.; Giordan, N.; Mazzoni, G. Efficacy and safety of hyaluronic acid (500–730 kDa) Ultrasound-guided injections on painful tendinopathies: A prospective, open label, clinical study. Muscles Ligaments Tendons J. 2017, 7, 388–395. [Google Scholar] [CrossRef]
- Frizziero, A.; Oliva, F.; Vittadini, F.; Vetrano, M.; Bernetti, A.; Giordan, N.; Vulpiani, M.C.; Santilli, V.; Masiero, S.; Maffulli, N. Efficacy of ultrasound-guided hyaluronic acid injections in achilles and patellar tendinopathies: A prospective multicentric clinical trial. Muscles Ligaments Tendons J. 2019, 9, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Kanchanathepsak, T.; Pichyangkul, P.; Suppaphol, S.; Watcharananan, I.; Tuntiyatorn, P.; Tawonsawatruk, T. Efficacy Comparison of Hyaluronic Acid and Corticosteroid Injection in Treatment of Trigger Digits: A Randomized Controlled Trial. J. Hand Surg. 2020, 25, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Mohebbi, R.; Rezasoltani, Z.; Mir, M.; Mohebbi, M.; Vatandoost, S.; Esmaily, H. High-Versus Low-Molecular-Weight Hyaluronic Acid for the Treatment of Rotator Cuff Tendinopathy: A Triple-Blind Randomized Comparative Trial. Ann. Pharmacother. 2021, 55, 1203–1214. [Google Scholar] [CrossRef] [PubMed]
- Rezasoltani, Z.; Esmaily, H.; Dadarkhah, A.; Rousta, M.; Mohebbi, R.; Vashaei, F. Low Molecular-weight Hyaluronic Acid Versus Physiotherapy for the Treatment of Supraspinatus Tendinopathy: A Randomized Comparative Clinical Trial. J. Am. Acad. Orthop. Surg. 2021, 29, e979–e992. [Google Scholar] [CrossRef]


{kind=link}
| In Vitro Studies | ||||
| Article | Sample Description | Experimental Group | Control Group | Outcome |
| Osti et al., 2015 | Human rotator cuff tears tendon-derived cells | 250 μg/mL GROUP-MW 500–730 KDa, 500 μg/mL GROUP-MW 500–730 KDa, 1000 μg/mL GROUP-MW 500–730 KDa, 250 μg/mL GROUP-MW 1000 KDa, 500 μg/mL GROUP-MW 1000 KDa, 1000 μg/mL GROUP-MW 1000 KDa, 1000 μg/mL GROUP-MW 1600 KDa, 1000 μg/mL GROUP-MW 2200 KDa, | Untreated cells | Tenocyte viability and proliferation, Apoptosis induction, Immunofluorescence staining |
| Gallorini et al., 2019. | Human supraspinatus tendon-derived cells | H2O2 GROUP: cultured cells were exposed to 2 mM H2O2 1000 KDa MW GROUP 2200 KDa MW GROUP 500–730 KDa MW GROUP 1600 KDa MW GROUP H2O2+ HA GROUPS: cells were treated with different hyaluronic acids in the presence of 2 mM H2O2 | Untreated cells | Cytotoxicity-lactate dehydrogenase (LDH) release assay, immunofluorescence staining of CD4, measurement of mitochondrial membrane potential (TMRE assay) by flow cytometry, cell lysis and protein extraction, immunoblotting, catalase activity |
| Pre-Clinical Studies | ||||
| Article | Sample Description | Experimental Group | Control Group | Outcome |
| Salamanna et al., 2014 | 24 male Sprague-Dawley rats, aged 8 weeks, 280 ± 40 g body weight, Patellar tendon 18 rats run on a treadmill 1 h a day, three times a week for 10 weeks. The other six rats underwent no training | TRAINED GROUP (6 rats)–euthanized at the end of the 10-week training. Detrained group (12 rats)-euthanized after 10-week training + 4 weeks without exercise DETRAINED-HA GROUP (6 of the 12 detrained rats)-at the end of the 1, 2, 3, and 4 weeks without exercise a peri-patellar infiltration of 300 μL of 20 mg/2 mL HA (500–730 KDa) was injected in the right patellar tendon DETRAINED-NaCl GROUP (remaining 6 of the 12 detrained rats)-at the end of the 1, 2, 3, and 4 weeks without exercise, at the level of the right patellar tendon, received a peri-patellar infiltration of 300 μL of physiological saline solution (Fresenius Kabi) | UNTRAINED GROUP (6 rats)-euthanized without training | Tenocyte morphology and morphometric analysis (transmission electron microscopy), tenocyte viability and proliferation (Alamar blue dye test), tenocyte synthetic activity |
| Frizziero et al., 2015 | 24 male Sprague-Dawley rats, aged 8 weeks, 280 ± 40 g body weight, Patellar tendon 18 rats run on a treadmill 1 h a day, three times a week for 10 weeks. The other six rats underwent no training | TRAINED GROUP (6 rats)–euthanized at the end of the 10-week training. Detrained group (12 rats)-euthanized after 10-week training + 4 weeks without exercise DETRAINED-HA GROUP (6 of the 12 detrained rats)-at the end of the 1, 2, 3, and 4 weeks without exercise a peri-patellar infiltration of 300 μL of 20 mg/2 mL HA (500–730 KDa, Fidia) was injected in the right patellar tendon DETRAINED-NaCl GROUP (remaining 6 of the 12 detrained rats)-at the end of the 1, 2, 3, and 4 weeks without exercise, at the level of the right patellar tendon, received a peri-patellar infiltration of 300 μL of physiological saline solution (Fresenius Kabi) | UNTRAINED GROUP (6 rats)-euthanized without training | TENDON ASSESSMENTS–modified semi-quantitative Movin grading scale (variables included: fiber structure, fiber arrangement, rounding of the nuclei, regional variation of cellularity, increased vascularity, collagen stainability, hyalinization), Tear density. ENTHESIS ASSESSMENTS-semi-quantitative score (variables included: patellar enthesis structure; cell morphology in calcified cartilage; cell morphology in non-calcified cartilage; chondrocyte cluster formation in calcified cartilage; chondrocyte cluster formation in non-calcified cartilage; tidemark integrity between calcified and non-calcified cartilage; matrix staining; vascularization). |
| Clinical Studies | ||||||||
|---|---|---|---|---|---|---|---|---|
| Article | Sample Description | Pathology | Injection Technique | Experimental Group | Control Group | Follow-Up | Outcome | Adverse Events |
| Meloni et al., 2007 | Age = 31–71 N =56 | Supraspinatus tendinosis (unresponsive to physical and medical therapy) | 5 periarticularinjections (1/week) under ultrasoundguide | 20 mg Sodium hyaluronate (MW = 500–730 KDa) together with 2 mL of 1% lidocaine and 2 mL of 0.9% sodium chloride solution | 4 mL of 0.9% sodium chloride solution, together with 2 mL of 1% lidocaine | ultrasound exam controls at 3, 6 and 12 months from the last injection | Shoulder Range of motion (goniometer), Pain (VAS), degree of discomfort | There were no complications such as infections and no aggravations of symptoms compared with the pre-treatment state in either group |
| Blaine et al., 2008 | Age = 50–79 N = 79 | Shoulder pain due to glenohumeral joint osteoarthritis, rotator cuff tear (partial or complete), and/or adhesive capsulitis for at least 6 months but less than 5 years’ refractory to standard treatments (physical therapy, corticosteroid injections and the administration of oral pain medications) | 5 intra-articular glenohumeralinjections (1/week) | 5 INJECTION HYALURONATE GROUP-2 mL sodium hyaluronate (molecular weight, 500–730 kDa) 3 INJECTION HYALURONATE GROUP-three injections of sodium hyaluronate (500–730 KDa) followed by two injections of phosphate-buffered saline solution | CONTROL GROUP-2 mL injections of phosphate-buffered saline solution | 7, 9, 13, 17, and 26 weeks after the initiation of therapy | Pain (VAS), maintenance of visual analogic scale pain relief, night pain improvement, patient global assessments, shoulder range of motion, general health questionnaire (short-form health survey-12) | All treatments were well tolerated. The most frequently reported adverse event considered to be related to study treatment was injection-site pain. |
| Frizziero et al., 2017 | Age = 18–85 N = 34 | Painful non-calcific rotator cuff tendinopathies confirmed by Instrumental diagnosis (US or MRI) | 3 sub-acromial space injections (1/week) under ultrasound guidance | 2 mL Hyaluronic acid (MW = 500–730 kDa) | 4 weeks (1/week) low energy extracorporeal shockwave therapy (MODULITH®); each session consisted of 1600 shots at a frequency of 4 Hz. The applied maximum energy (0.15 mJ/mm2) was adjusted on the basis of the patient’s tolerance, Mean session duration: 10 min. | Parameters were evaluated at baseline (V0), at the end of the treatment (V1) and after 3 months of follow-up (V2) | Disabilities of the arm (DASH score and Constant-Murley scales) | No serious adverse events were recorded |
| Fogli et al., 2017 | Age = 33–59 N = 62 | lateral elbow (26), Achilles (34) or patellar (11) tendinopathies | 3 peritendinous injections (1/week) under ecographic guide | 2 mL Hyaluronic acid (MW = 500–730 kDa) | 7, 14, and 56 days after first treatment | Pain (VAS), ultrasound assessment (changes in tendon thickness and neovascularization) | No serious adverse events were recorded | |
| Frizziero et al., 2019 | Age = 18–65 N = 35 | Achilles (26) and patellar (9) mid-portion tendinopathies for ≥6 weeks duration and confirmed by ultrasound evaluation | 3 peritendinous injection (1/week) between paratenon and tendon under Ecographic guide | 20 mg/2 mL Hyaluronic acid (HyaloTend®, Fidia, MW = 500–730 KDa) | 14, 45 and 90 days after the procedure | VISA-A and VISA-P at 90 days of follow-up, pain (NRS-11), US parameters (tendon appearance and neovascularization), Patient Global Assessment (PGA), Clinical Observer Global Assessment (COGA), rescue medication consumption (paracetamol) and Health-related Quality of Life (EuroQoL EQ-5D-5L questionnaire) | The treatment was well tolerated with only one adverse events in Achilles tendinopathy group, probably related to the injection procedure | |
| Kanchanathepsak et al., 2020 | Age = 43–69 N = 66 | Trigger digits | 1 peritendinous injection under ecographic guide | 1 mL hyaluronic acid (500–730 kD, 20 mg/2 mL) | 1 mL of 10 mg/mL of triamcinolone acetate | 1, 3, 6 months | Residual symptoms (Quinell grading), Pain (VAS), disabilities of the Arm (DASH score) | There was no major complication found in the study. Three patients complained about local discomfort at 1 week after injection without any sign of local inflammation. |
| Mohebbi et al., 2021 | Age = 16–70 N = 56 | Rotator cuff tendinopathy (based on history, physical examination, and magnetic resonance imaging) with persistent shoulder pain for more than 6 weeks and less than 36 months | Single periarticular injection under ultrasound guidance | 20 mg (2 mL) LMW-HA 1% (500–730 kDa) | 20 mg (2 mL) HMW-HA 1% (>2000 kDa, Synogel, NikanTebKimia Pharmaceutical). | baseline, 1, 4 weeks, and 3 months after the interventions | Pain (VAS), shoulder range of motion (goniometer), quality of life (WHOQOL-Bref) | No serious adverse events were recorded. Nine patients in the HMW-HA group and 3 participants in the LMW-HA group showed signs of inflammation at the site of injection. Overall, the LMW-HA group showed more tolerance to injection pain |
| Rezasoltani et al., 2021 | Age = 20–65 N = 51 | Supraspinatus tendinopathy (based on history, physical examination, and magnetic resonance imaging) with persistent shoulder pain for more than 6 weeks and less than 3 months | Single subacromial injection under ultrasound guidance | 20 mg (2 mL) LMW-HA 1% (500–730 kDa). | Physiotherapy group: 36 sessions, 3/week. | Baseline, 1, 4, and 12 weeks postintervention. | Pain (VAS), shoulder range of motion (goniometer), disabilities of the Arm (DASH score), quality of life (WHOQOL-Bref) | No important adverse events occurred in the two groups |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frizziero, A.; Vittadini, F.; Bigliardi, D.; Costantino, C. Low Molecular Weight Hyaluronic Acid (500–730 Kda) Injections in Tendinopathies—A Narrative Review. J. Funct. Morphol. Kinesiol. 2022, 7, 3. https://doi.org/10.3390/jfmk7010003
Frizziero A, Vittadini F, Bigliardi D, Costantino C. Low Molecular Weight Hyaluronic Acid (500–730 Kda) Injections in Tendinopathies—A Narrative Review. Journal of Functional Morphology and Kinesiology. 2022; 7(1):3. https://doi.org/10.3390/jfmk7010003
Chicago/Turabian StyleFrizziero, Antonio, Filippo Vittadini, Davide Bigliardi, and Cosimo Costantino. 2022. "Low Molecular Weight Hyaluronic Acid (500–730 Kda) Injections in Tendinopathies—A Narrative Review" Journal of Functional Morphology and Kinesiology 7, no. 1: 3. https://doi.org/10.3390/jfmk7010003
APA StyleFrizziero, A., Vittadini, F., Bigliardi, D., & Costantino, C. (2022). Low Molecular Weight Hyaluronic Acid (500–730 Kda) Injections in Tendinopathies—A Narrative Review. Journal of Functional Morphology and Kinesiology, 7(1), 3. https://doi.org/10.3390/jfmk7010003