1. Introduction
Kyphotic spinal deformities are common among the elderly [
1]. A reduction in the lumbar lordosis angle (LL) and pelvic tilt angle (PT) are also characteristic of aging. Kyphosis is considered age-related and is well tolerated in the majority of the population; however, it reduces spinal extension [
2,
3,
4]. Shoulder elevation is accompanied by spinal extension. In the clinical situation, limitation of the shoulder elevation in the kyphotic elderly person is common; however, little has been reported on the relationship between spine alignment and shoulder elevation, particularly in the elderly. The purpose of this study was to clarify the relationship between spine alignment and shoulder elevation in a kyphotic elderly population.
2. Materials and Methods
We recruited 23 consecutive female patients (mean age, 76 ± 6.3 years; height, 149.3 ± 6.7 cm; weight, 48.1 ± 10.4 kg) who underwent balloon kyphoplasty for spinal compression fractures at our institute (
Table 1). Patients with shoulder complaints or a history of shoulder surgery or trauma were excluded.
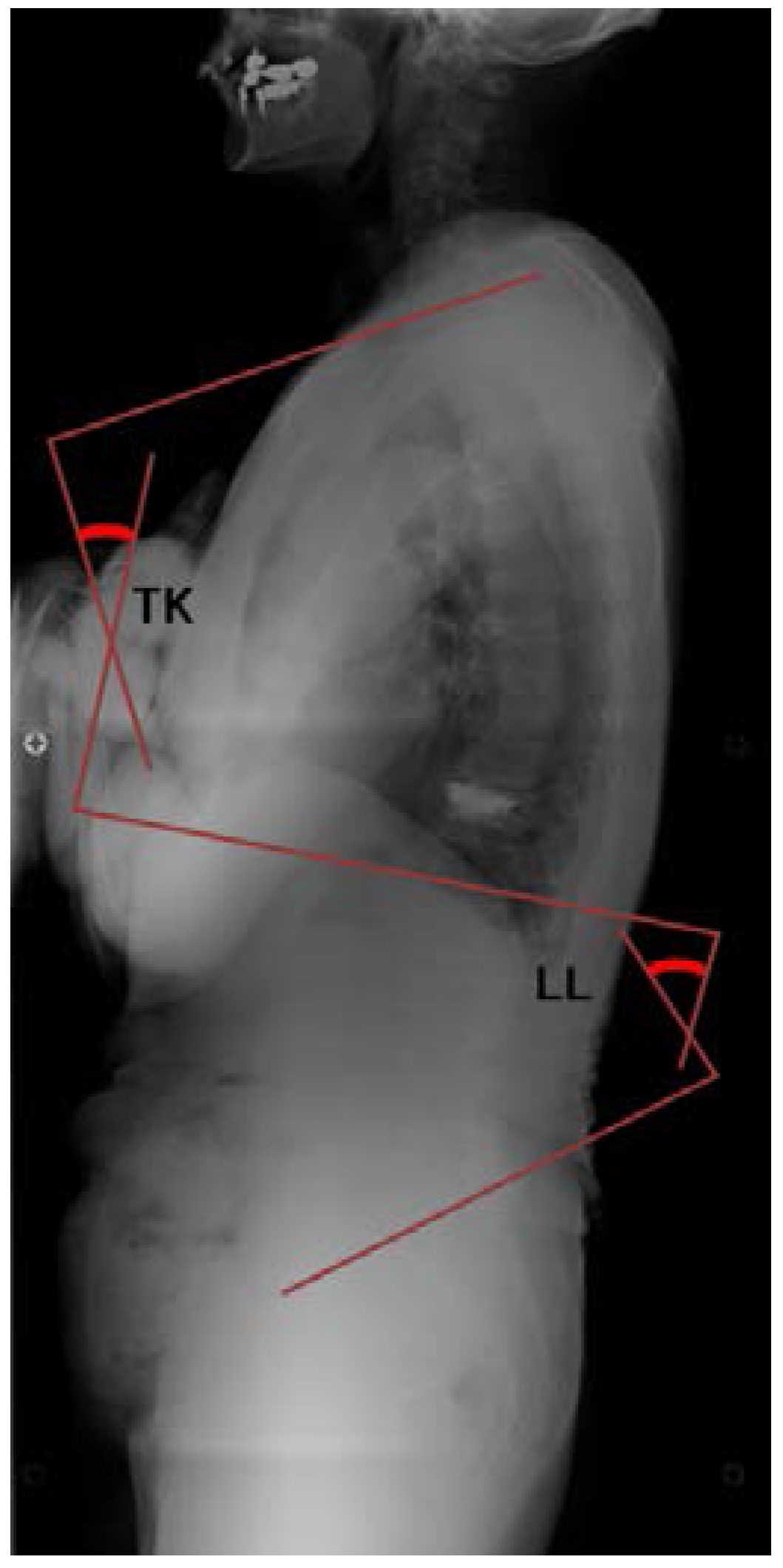
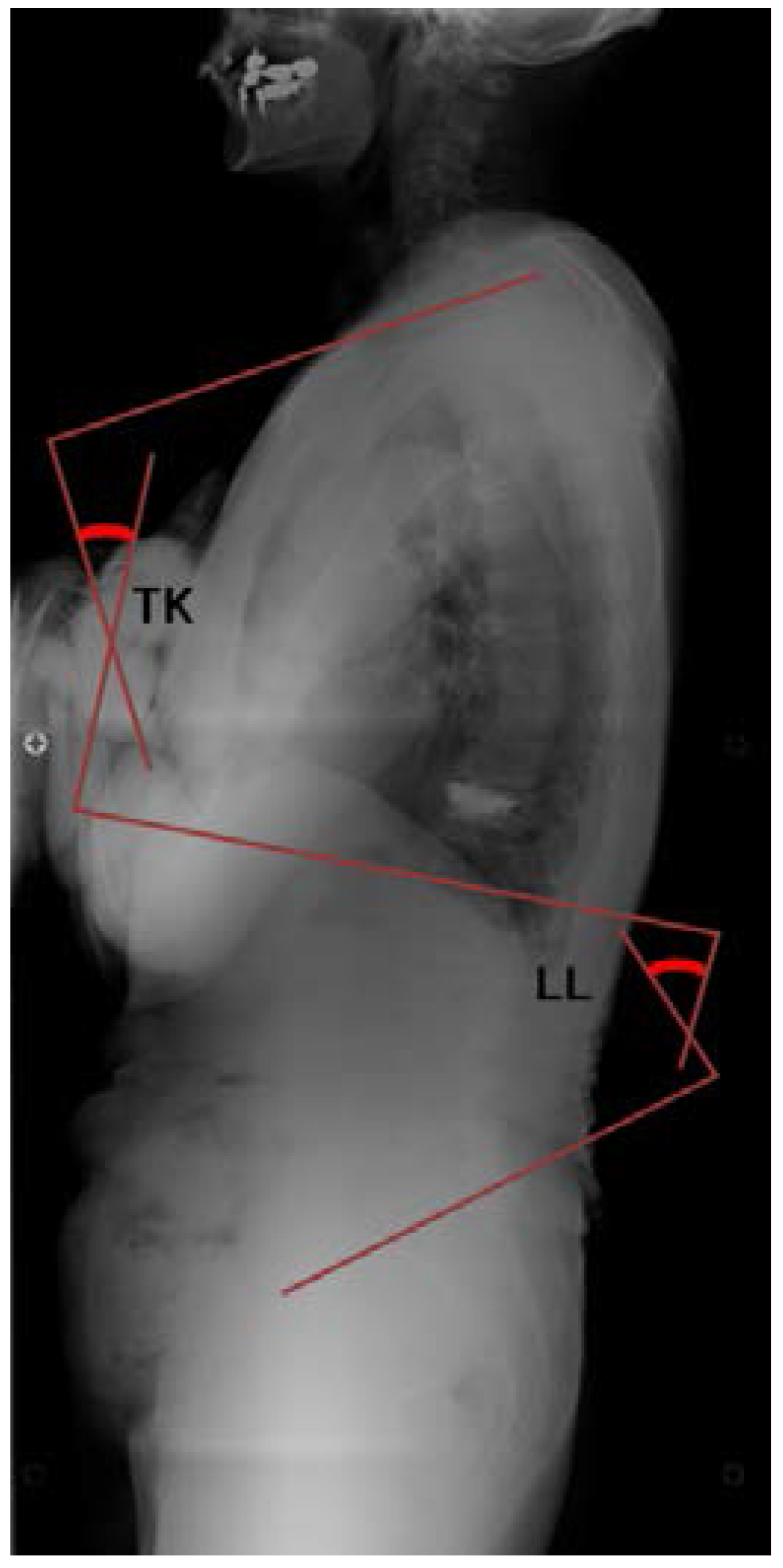
Spine alignment was evaluated on standing true lateral radiographs of the whole spine. The thoracic kyphosis angle (TK), LL, and PT were measured for each subject (
Figure 1 and
Figure 2). The TK was defined as the angle between the superior endplate of T1 and the inferior endplate of T12. LL was the angle between the inferior endplate of T12 and the superior endplate of S1. PT was the angle between the line connecting the midpoint of the superior endplate of S1 with the center of the femoral head and the vertical line.
The shoulder active range of motion was measured in the sitting position. Elevation was measured in two ways: without scapular fixation (combined motion of the scapulothoracic and glenohumeral (GH) joint, total elevation angle) and with the scapula fixed (GH joint motion, GH angle). The University of California Los Angeles (UCLA) Shoulder Score was recorded as the functional evaluation. Recorded values of TK, LL, and PT were compared with reported reference values.
Statistical analyses were performed with Pearson correlations with significance set at p < 0.05.
3. Results
The average total elevation angle was 128.9° ± 22°, the GH angle was 80.7° ± 10.9°, and the UCLA Score was 32.4 ± 2.1. The TK was 36.7°, the LL was −29.1°, and the PT was 30.5° (
Table 2 and
Table 3). Compared with the reported reference values [
5], TK was within the normal range and LL and PT were slightly larger, showing lumbar lordosis and decreased pelvic tilt. The total elevation angle was significantly negatively correlated with LL (
Table 4). TK and PT were not significantly correlated with any parameters.
4. Discussion
The total shoulder elevation angle was limited in the kyphotic elderly women in the current study. This study also showed that the GH angle was maintained, indicating that kyphotic changes may interfere with spinal extension and reduce the total elevation arc without GH motion deficit [
2,
3,
4]. Kapandji reported that spinal extension accompanied shoulder elevation when the angle exceeded 120° [
2]. At the final stage of the elevation, spinal extension enhances lumbar lordosis. This lumbar lordotic motion reportedly contributes to shoulder elevation. Drzał-Grabiec and colleagues evaluated parameters characterizing the posture of women over the age of 60 years compared with a control group to determine the dynamics of body posture changes in the following decades [
1]. They found that thoracic kyphosis depth significantly deepened with age and there were statistically significant differences in the thoracic-lumbar spine slope and upper thoracic spine slope while the lumbar spine slope did not show significant differences between age groups.
In this study, given the significant negative correlation between the shoulder elevation angle and LL, it seemed that the decreased lumbar lordosis angle restricted total shoulder elevation. Imagama and colleagues reported that increased thoracic kyphosis, increased spinal inclination and weak back muscle strength are the risk factors for limited shoulder ROM [
6]. Theoretically, thoracic kyphosis, which reduces scapular upward rotation, could lead to decreased shoulder elevation; however, we found no statistically significant correlation between TK/PT and shoulder elevation. Pelvic tilt was also not associated with shoulder elevation. However, a reduction of LL was thought to compensate for the increased TK, and advancement of the kyphotic angle was thought to indirectly decrease shoulder elevation.
The current study suggested that women aged over 60 years have a greater risk of ROM restriction and lesser postoperative scores. The mean UCLA Shoulder Score in kyphotic elderly patients without shoulder symptoms was approximately 32 in this study. Because of recent advances in shoulder surgery and anesthesia, shoulder arthroplasty or reconstruction surgery in the elderly population is increasing [
7,
8,
9]. The UCLA Shoulder Score does not have an age-adjusted equation, as seen in the Constant-Murray score [
10,
11,
12]. The expected maximum score would be approximately 32 (which is ordinarily rated “good”), and the maximum expected elevation angle would be 130° for the kyphotic elderly population.
There are several limitations of our study. The subjects were limited to women, all of whom underwent vertebroplasty although they had no shoulder symptoms. Spinal alignments were examined in the static setting and thus did not account for dynamic vertebral mobility. Further study (such as motion capture analysis) is necessary.
5. Conclusions
The total shoulder elevation angle and clinical score were limited in kyphotic elderly women. The average total elevation angle was 129° and the UCLA Score was 32.4. Kyphotic changes seemed to interfere with spinal extension and reduced the total elevation arc without GH motion deficit. A reduction in total shoulder elevation was negatively correlated with LL.
Author Contributions
Manami Yamamoto and Yumi Kubo conducted the acquisition of data. Manami Yamamoto, Yumi Kubo and Kotaro Yamakado were drafting of manuscript and wrote the main paper. All authors discussed the study conception and design, the results and implications at all stages.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Drzał-Grabiec, J.; Snela, S.; Rykała, J.; Podgórska, J.; Banaś, A. Changes in the body posture of women occurring with age. BMC Geriatr. 2013, 13, 108. [Google Scholar] [CrossRef] [PubMed]
- Kapandji, I.A. The Physiology of the Joints: Upper Limb; Churchill Livingstone: London, UK, 2007. [Google Scholar]
- Crawford, H.J.; Jull, G.A. The influence of thoracic posture and movement on range of arm elevation. Physiother. Theory Pract. 1993, 9, 143–148. [Google Scholar] [CrossRef]
- Stewart, S.G.; Jull, G.A.; Ng, J.K.-F.; Willems, J.M. An initial analysis of thoracic spine movement during unilateral arm elevation. J. Man. Manip. Ther. 1995, 3, 15–20. [Google Scholar] [CrossRef]
- Kanemura, T.; Satake, K.; Yamaguchi, H. Sagittal spino-pelvic alignment in an asymptomatic Japanese population. Seisaigai 2013, 56, 805–814. (In Japanese) [Google Scholar]
- Imagama, S.; Hasegaw, Y.; Wakao, N.; Hirano, K.; Muramoto, A.; Ishiguro, N. Impact of spinal alignment and back muscle strength on shoulder range of motion in middle-aged and elderly people in a prospective cohort study. Eur. Spine J. 2014, 23, 1414–1419. [Google Scholar] [CrossRef] [PubMed]
- Kaisidis, A.; Pantos, P.G.; Heger, H.; Bochlos, D.; Selimas, S.; Oikonomoulas, V. Reverse shoulder arthroplasty for the treatment of three and four part fractures of the proximal humerus in patients older than 75 years old. Acta Orthop. Belg. 2014, 80, 99–105. [Google Scholar] [PubMed]
- Churchill, R.S. Elective shoulder arthroplasty in patients older than ninety years of age. J. Shoulder Elbow Surg. 2008, 17, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Ricchetti, E.T.; Abboud, J.A.; Kuntz, A.F.; Ramsey, M.L.; Glaser, D.L.; Williams, G.R. Total shoulder arthroplasty in older patients: Increased perioperative morbidity? Clin. Orthop. Relat. Res. 2011, 469, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, H.C.; Sew Hoy, A.L.; Clarke, I.C. UCLA anatomic total shoulder arthroplasty. Clin. Orthop. Relat. Res. 1981, 155, 7–20. [Google Scholar] [CrossRef]
- Nutton, R.W.; McBirnie, J.M.; Phillips, C. Treatment of chronic rotator-cuff impingement by arthroscopic subacromial decompression. J. Bone Jt. Surg. 1997, 79, 73–76. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).






{kind=link}
{kind=link}