Abstract
Research suggests that the impact of childhood sexual trauma (CST) on adult well-being varies in relation to characteristics of CST experiences (e.g., age of onset and duration/frequency) that influence the degree of trauma severity. Yet there remains a need for a CST severity measure that consistently delineates survivors with an elevated risk of adverse adult outcomes (AAOs) and accounts for correlations between severity characteristics. We compared two theory-based, categorical proxy measures of CST severity (duration and developmental timing) in their relationship with three AAOs, among a national probability sample of U.S. adult CST survivors (N = 568). We found a strong relationship between CST duration and developmental timing (p < 0.001), and redundancy in their impact on AAOs (i.e., no meaningful difference in how well they predicted AAOs). Participants with more chronic CST (≥4 years duration or occurring across childhood and adolescence) were twice as likely to report AAOs as other participants. Findings support the importance of assessing trauma chronicity in research and practice, to focus prevention and intervention strategies on CST survivors with the greatest long-term health risk. A categorical CST duration measure offers a theory-based assessment strategy that accounts for both the temporal and developmental effects of trauma severity on health outcomes.
1. Introduction
Childhood sexual trauma (CST, i.e., before age 18) is a persistent and pervasive public health problem in the United States. Prevalence estimates suggest that over 16 million adults in the U.S. have experienced CST, including many with chronic victimization during youth [1]. For some, CST has ongoing and wide-reaching consequences for health and functioning into adulthood (e.g., elevated risk of mental health diagnoses, chronic health problems, and sexual functioning difficulties) [1,2,3,4,5,6,7,8]. More broadly, the ongoing CST epidemic has considerable socioeconomic costs for families, communities, and society as a whole (e.g., high healthcare utilization and costs; productivity losses; intergenerational cycles of violence) [9,10,11,12].
The nature and degree of CST’s long-term effects over the lifecourse vary widely, with some survivors experiencing less detrimental impacts than others [13,14]. In part, this variation can be attributed to characteristics of CST experiences (e.g., degree of force or coercion involved; number or duration of CST occurrences) that may differentially influence the severity of the trauma and, in turn, produce varying levels of long-term health risk. In research and practice, assessing CST severity helps to capture information about the complexities of CST experiences and delineate sub-groups of CST survivors who may have an elevated risk of adverse adult outcomes (AAOs).
Empirical approaches to CST severity measurement have involved assessing CST characteristics as proxies for the degree of trauma severity; yet these characteristics are highly likely to be correlated with one another (e.g., age at the time of CST onset and the duration of CST victimization). CST scholars have used a variety of severity measures, often based on precedent rather than a strong theoretical basis, which has created difficulties in identifying those that consistently predict AAO risk [15,16,17,18]. Correlations between severity-related characteristics impede the ability to distinguish the unique effects of any one characteristic on long-term outcomes. An important methodological imperative in CST research is to identify severity measurement strategies that (a) are grounded in theoretical perspectives on how CST severity influences long-term outcomes, (b) account for relationships between severity-related characteristics, and (c) have practical value for distinguishing CST survivor sub-groups to prioritize in efforts to mitigate and address AAO risk.
The current study uses data from a large national sample of U.S. adults to compare two proxy measures for CST severity (i.e., CST duration and CST developmental timing) that are based on the same underlying metric (i.e., ages when CST occurred) and reflect theoretical approaches to CST measurement. To our knowledge, no prior study has compared these CST severity indicators and their impact on AAOs among a probability sample of U.S. adults.
1.1. Theoretical Perspectives on CST Severity and Long-Term Health Risk
1.1.1. CST Severity and Traumatic Stress Theory
From a traumatic stress perspective, CST severity involves the confluence of intensity (i.e., degree of fear or pain), uncontrollability (i.e., degree of helplessness), and temporality (i.e., frequency or duration) [13,19]. Temporal characteristics are considered particularly salient in driving long-term traumatic effects. More chronic trauma results in learned patterns of stress response (e.g., physiological arousal, meaning-making, and behavioral coping) that strengthen with longer periods of trauma exposure and extended anticipatory stress between traumatic incidents [13,19,20]. Over time, this reinforces and generalizes adverse emotional reactions (e.g., fear and self-blame), cognitive patterns (e.g., distrust and negative appraisals of others), and coping strategies (e.g., dissociation and avoidance) in response to perceived stressors, increasing susceptibility to long-term adversities [13,14,19,21,22]. Additionally, sustained activation of physiological stress responses due to chronic trauma may lead to more rapid cellular aging and increased inflammation, setting the stage for a variety of health consequences [23,24]. Indeed, chronic CST experiences have been linked to an elevated risk of AAOs spanning physical, psychological, and social-emotional domains of well-being [1,25,26,27,28,29].
1.1.2. CST Severity and Developmental/Lifecourse Theory
The age at which an individual experiences CST has long been considered a trauma characteristic that may predict long-term outcomes, in that the unique tasks or milestones associated with the developmental stage during which the trauma occurs (i.e., developmental timing) may differentially influence risk [2,25,30]. For instance, early childhood trauma can disrupt the development of key socioemotional and neurobiological processes (e.g., self-regulation, attachment, and socialization) [31,32,33] which, in turn, may stall or prevent the achievement of subsequent developmental tasks and produce long-term alterations in emotion regulation, stress response, and coping systems that heighten health risk [22,34,35,36]. Adolescent CST may be especially deleterious since older youth have a greater conceptualization of what constitutes a violation, and are experiencing substantial biopsychosocial changes (e.g., development of self-concept, sexual identity, and peer relationships) that can be significantly altered by CST, contributing to long-term risk [22,34]. Like traumatic stress theory, developmental perspectives highlight that repeated trauma may foster physiological and social–emotional conditions that elevate the risk of long-term adverse outcomes [22,31,33,34,35,37,38]. That is, CST that is chronic or that occurs over multiple developmental stages may generate altered stress-response, self-regulation, affective, and coping processes that continuously disrupt development and lead to an accumulation of long-term health risks over time.
1.2. Limitations in CST Severity Measurement: Overlooking Trauma Chronicity
Despite theoretical and empirical support for the importance of CST chronicity in driving long-term outcomes, it remains underutilized in severity measurement [39]. Many CST severity measures assess characteristics that may influence trauma intensity or uncontrollability (e.g., age of CST onset, involvement of penetration or physical force) while overlooking temporal effects. For instance, some measures are limited to one instance of CST (e.g., first or most severe experience), neglecting the effects of chronic experiences. Many studies collect chronicity-related data (e.g., frequency or number of CST occurrences) but collapse it into dichotomous measures (any vs. no CST) for analysis. While this approach may be beneficial for examining CST among smaller samples, it assumes all CST experiences are of equal severity and similarly influence AAO risk, which is not empirically supported [16,25]. In contrast, our study utilized perpetrator-specific assessments of CST to capture the duration of specific CST experiences and the overall duration (i.e., total number of years) of CST exposure in childhood and adolescence.
Prior research on CST developmental timing has not identified a clear relationship with AAO risk. Childhood CST has been found to more strongly predict some outcomes (e.g., anxiety and depression) [40,41,42], while adolescent CST may be a stronger predictor of others (e.g., sexual dysfunction and adult sexual victimization) [43,44,45]. Other studies have found minimal effects of developmental timing on AAO risk [2,24,46,47,48,49,50]. Measurement limitations likely contribute to the lack of empirical consensus. Many studies assess age at CST onset (i.e., when the first CST experience began) or use dichotomous assessments of CST occurring in different developmental stages (i.e., not mutually exclusive categories); both approaches overlook chronic trauma and the amplified AAO risk that may be associated with CST spanning multiple developmental stages. Few studies have delineated individuals who experienced CST in both childhood and adolescence from those for whom CST occurred only in one stage [27,28,47]. For the current study, we developed a categorical measure of developmental timing based on perpetrator-specific CST assessments, which delineates survivors who experienced CST in both childhood and adolescence from those with CST experiences in either developmental period.
1.3. Correlations and Comparisons Between CST Severity Characteristics
CST severity-related characteristics are often correlated, making it difficult to determine the unique relationships of a single characteristic with long-term outcomes [26,51,52,53,54,55,56]. For instance, a person’s age at the time they experienced CST may relate to other aspects of the experience, such as the degree of force or coercion involved and the likelihood of repeated victimization. Therefore, CST developmental timing measures inherently carry information on other trauma characteristics that influence the degree of severity. This complicates the ability to distinguish the unique effects of individual severity characteristics on long-term outcomes and to identify sub-groups of CST survivors with elevated AAO risk. Nonetheless, researchers and practitioners need a valid and reliable approach for measuring CST severity that allows for comparing results across studies, explicating relationships with AAOs, and establishing evidence-based standards for identifying CST survivor sub-groups to prioritize for tailored intervention and support strategies [17,36,57].
Our study compares measures of CST duration and developmental timing among a national sample of U.S. adults. Empirical comparisons of CST severity measures have value for identifying those that are most strongly linked to long-term outcomes, working toward measurement standardization, and improving the ability to synthesize findings across studies [15,40,46]. We developed and compared two proxy measures of CST severity that are rooted in theory and based on the same underlying metric [i.e., age(s) when CST occurred], to examine for similarities and differences in how each severity measure relates to AAOs spanning multiple life domains.
1.4. Current Study
This study aims to (1) examine the relationship between measures of CST duration and developmental timing, and (2) compare the two measures in their relationships with AAOs. Data are drawn from the National Sexual Health Survey (NSHS; 1995–1996), which is uniquely suited to address the study aims due to the use of a national probability sample of U.S. adults, direct assessments of up to five perpetrator-specific CST experiences, and a range of AAO measures spanning multiple life domains. Large historical samples, like the NSHS, are highly valuable for examining theoretically relevant relationships between variables, with data that address limitations of more recent studies [58,59,60,61]. We aimed to test theoretical relationships between measures of CST severity and adult health outcomes, with a sample large enough to delineate sub-groups of participants reporting AAOs and chronic CST experiences that are relatively low-prevalence [1]. CST research has often been limited by small or non-probability samples, and CST measures that neglect chronicity or severity altogether (e.g., dichotomous measures of any vs. no CST). Despite its age, the NSHS is unique in providing a large, probability-based national sample and perpetrator-specific CST assessments; this allowed for the development of time-based, categorical measures of CST duration and developmental timing to compare multiple sub-groups of survivors for differences in AAO risk.
This study expands on a prior analysis of NSHS data [1], which found strong evidence for the impact of CST duration on the risk of AAOs across multiple life domains, following a dose–response pattern (longer duration = higher risk), compared to participants without CST. The current analysis includes only participants with CST to examine the impact of severity more specifically.
2. Materials and Methods
2.1. Sampling, Data Collection, and Participants
The National Sexual Health Survey (NSHS) is a national random-digit-dial study of U.S. adults (1995–1996; cooperation rate = 65%); detailed procedures are available online [62]. As noted above, the NSHS was selected due to the use of a large probability-based sample and comprehensive perpetrator-specific CST measures, which are uncommon in more recent CST studies. A primary concern with using historical data is limited generalizability to current populations. However, we have previously found CST prevalence to remain relatively stable when comparing the NSHS to more recent samples, with small variation potentially due to methodological differences or changes in trauma disclosure over time [1]. Further, the theoretical relationships of focus in the current study are grounded in fundamental and relatively stable psychosocial and developmental processes that are affected by trauma (e.g., stress response and emotion regulation processes), as supported by more recent conceptualizations of how trauma impacts long-term health (e.g., Refs. [13,14,23]). Although further study of relationships between CST duration, developmental timing, and AAOs with more recent cohorts is warranted, NSHS data regarding these relationships can be considered valid and applicable in a contemporary context.
NSHS participants completed telephone survey interviews (1 h, English and Spanish) that covered a range of topics related to sexual health and other aspects of well-being, including perpetrator-specific assessments of CST experiences (see Measures). All survey measures were pre-tested using quantitative and qualitative techniques, and sexual health measures were reviewed by a panel of clinical sex therapists and researchers. Although the use of retrospective self-report measures may have introduced recall bias, the NSHS has produced similar CST prevalence estimates as subsequent probability-based studies and other studies using random-digit-dial methods [1].
Participants in the current analysis included adults who reported at least one experience of CST (before age 18; N = 568). The mean age of participants was 34.6 years (SE: 0.44; Range: 18–70 years), and the majority (73%) were women. Most participants identified as heterosexual (89%) and white (78%), with smaller proportions identifying as gay/lesbian/bisexual (11%), Black/African American (9%), and Hispanic/Latino (8%).
2.2. Measures
2.2.1. CST Duration and CST Developmental Timing
The current analysis builds on a prior investigation [1] that developed and tested a categorical measure of CST duration in relation to AAOs spanning multiple life domains. Categorical measures, which allow for non-linear relationships between CST severity and AAOs, are highly valuable for identifying CST survivor sub-groups with a higher risk of long-term adverse outcomes [63]. We developed a categorical measure of CST developmental timing for the current study.
The NSHS included a root question to screen for sexual trauma history: “Have you ever been forced or frightened into doing something sexually that you did not want to do?” Participants who responded “yes” were asked about the number of people who forced or frightened them into an unwanted sexual situation (i.e., number of perpetrators). A series of perpetrator-specific items was then asked for up to five perpetrators, including the participant’s age at the onset of each experience and the duration of each experience (<12 months, 12–23 months, ≥24 months). Participants who indicated at least one unwanted sexual experience before age 18 were considered to have experienced CST (N = 568, 8.9% of NSHS sample). This measure has previously demonstrated construct, predictive, and known-groups validity among U.S. adult samples [1,64,65].
We computed the total duration of CST exposure by subtracting the participants’ age at their first reported CST experience from their age at their last reported CST experience, and adding the duration (years) of their last CST experience. This resulted in a continuous CST duration variable, which we categorized into three groups (excluding those with no CST, N = 5950) using a taxometric-based approach [63,66,67], in which we compared categories of CST duration with various thresholds to identify significant between-group differences [1]. That is, we determined cut points for categorization by first using logistic regression models to assess differences between adjacent duration values (0, 1, 2, … > 5 years) in their association with nine AAOs, and then collapsing adjacent duration values that did not demonstrate significance differences with respect to any AAO. This resulted in a duration measure with three discrete categories: single-event CST (i.e., one time; N = 236, 41.6%), intermediate duration CST (1–3 yrs; N = 238, 41.9%), and extreme duration CST (≥4 years; N = 94, 16.6%); the measure has demonstrated construct and known-groups validity among the NSHS sample [1].
Our measure of CST developmental timing was derived from perpetrator-specific questions about participants’ age at the onset of each reported CST experience (≤5 perpetrators). Like other CST studies that have compared developmental groups, we defined adolescence as beginning at age 14 [41,68]. We generated a categorical variable that differentiated participants who reported CST experiences only before age 14 (childhood only; N = 226, 38.5%), those who reported CST experiences only between ages 14 and 17 (adolescence only; N = 285, 48.6%), and those who reported CST experiences both before age 14 and between ages 14–17 (childhood and adolescence; N = 76, 12.9%).
2.2.2. Dependent Variables: Adverse Adult Outcomes
Recent emotional health problems were assessed with one item: “In the past 4 weeks, have you had any emotional problems?” [1 = Yes (N = 134, 22.8%), 0 = No (N = 453, 77.2%)] [68]. We used a global assessment of overall health, which asked, “How would you rate your overall health?” [68], and dichotomized responses as Fair/Poor (N = 72, 12.3%) and Excellent/Very Good/Good (N = 515, 87.7%). Low sexual satisfaction was assessed with one item: “In the last 12 months, has there been something either physical or emotional that has made it difficult for you to have a satisfying sexual relationship?” [1 = Yes (N = 179, 30.8%); 0 = No (N = 403, 69.2%)].
2.2.3. Demographic Correlate Variables
Age was assessed as a continuous variable, and gender as dichotomous (0 = Male, 1 = Female). A dichotomous variable for race/ethnicity was derived from two items assessing racial identity (“Which would you say best describes your racial background?”) and ethnicity (“Are you of Spanish, Hispanic, or Latino origin?”). We constructed a dichotomous variable for sexual orientation using items that assessed participants’ gender and the genders of their sexual partners since age 18.
2.3. Data Analysis
We used Stata 15 software for data management and analysis. All analyses were conducted on unweighted data. Bivariate associations between CST duration and developmental timing were assessed using omnibus chi-square analyses and bivariate logistic regression models for post hoc comparisons. To examine CST duration and developmental timing in relation to AAOs, we conducted bivariate chi-square analyses followed by a series of adjusted multivariate logistic regression models to assess the effects of independent variables on each outcome: (1) CST duration as the primary predictor (Model 1, duration model), and (2) CST developmental timing as the primary predictor (Model 2, developmental timing model). We used penalized likelihood estimation methods for models with small sub-groups (n < 30 in a cell) and Pearson testing to examine model fit (all p > 0.05). All models controlled for any significant demographic covariates (age, race/ethnicity, and/or sexual orientation; gender was not significantly associated with any AAO). We also examined variable inflation factor (VIF) data to rule out multicollinearity between predictors (mean VIF: 1.05 = no significant collinearity).
For each outcome, we examined Akaike Information Criterion (AIC) scores for the duration and developmental timing models to compare how well they fit the data. AIC is a well-known model selection strategy, which provides a robust estimation of model quality in terms of goodness of fit and model simplicity; a lower AIC score indicates a better-fitting model [69,70]. In comparing the AIC scores between two models, similar scores (i.e., difference ≤ 10) indicate that there is no considerable difference between how well the models fit the data for a given outcome; a difference of 4 or less indicates a high level of redundancy between the two models [69]. In the current study, similar AIC scores between Models 1 and 2 would suggest that there is no significant difference in the effects of CST duration and developmental timing on the outcome.
3. Results
3.1. Association Between CST Duration and CST Developmental Timing
Descriptive statistics for CST duration and developmental timing are reported in Table 1. Chi-square analyses demonstrated a significant relationship between the two variables [χ2(4, N = 568) = 389.9, p < 0.001]. We examined post hoc comparisons using bivariate logistic regression models to compare developmental timing sub-groups (childhood only vs. adolescence only vs. childhood and adolescence) in the likelihood of reporting each CST duration category. All between-group differences were found to be statistically significant (all p-values < 0.001; see Table 1 and Figure 1). For instance, participants who experienced CST in both childhood and adolescence were significantly more likely to report CST of extreme duration compared to those with CST in childhood or adolescence only; and those with CST in childhood only were significantly more likely to report extreme duration than those with CST in adolescence only. CST in adolescence only was significantly more likely to be a single event (occur one time) compared to CST in childhood only.

Table 1.
Association between CST duration and CST developmental timing.
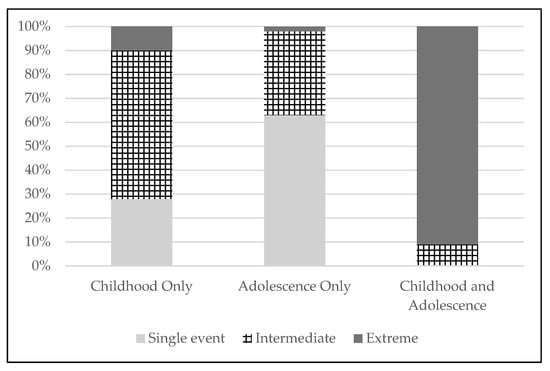
Figure 1.
Distribution of CST duration categories across CST developmental timing sub-groups. Percentages within each bar reflect the proportions of each CST developmental timing sub-group (Childhood only—CST only before age 14 yrs; Adolescence only—CST only between ages 14–17 yrs; Childhood and adolescence—CST both before age 14 and between ages 14–17 yrs) that reported each CST duration category (Single event—one time; Intermediate—1–3 yrs; Extreme—≥ 4 yrs).
3.2. Effects of CST Duration and CST Developmental Timing on Adverse Adult Outcomes
We examined the effects of CST duration and developmental timing on three AAOs: recent emotional health problems, fair/poor overall health, and low sexual satisfaction. Bivariate analyses found both duration and developmental timing to be significantly related to all outcomes (see Table 2). Higher proportions of participants in the extreme duration group and the childhood/adolescence group reported each outcome compared to other sub-groups. For instance, nearly half of participants in the extreme duration sub-group (46%) and the childhood/adolescence sub-group (45%) reported low sexual satisfaction, compared to <30% of other participants (see Table 2).
Table 2.
Adverse adult outcomes by CST duration and developmental timing †.
Multivariate logistic regression models were used to examine the effects of CST duration and developmental timing on each outcome. For all models, categories expected to have the highest odds of AAOs were selected as reference groups (extreme duration CST and childhood/adolescence CST). CST duration models demonstrated significant effects on all AAOs (see Table 3). Participants with single-event CST were significantly less likely to report emotional health problems (p = 0.004), fair/poor overall health (p = 0.044), and low sexual satisfaction (p = 0.001) than those with extreme duration CST (≥4 yrs). Participants with intermediate duration CST (1–3 yrs) were significantly less likely to report fair/poor overall health (p = 0.019) and low sexual satisfaction (p = 0.005) than those with extreme duration CST. There were no significant differences between participants with single-event and intermediate duration CST (p’s > 0.05).
Table 3.
Multivariate effects of CST duration and developmental timing on adverse adult outcomes †.
CST developmental timing models also demonstrated significant effects on all AAOs (see Table 3). Participants with CST in childhood only were significantly less likely to report emotional health problems (p = 0.015) and low sexual satisfaction (p = 0.009) than those with CST in childhood/adolescence. CST occurring only in adolescence conferred lower odds of emotional health problems (p = 0.004), fair/poor overall health (p = 0.047), and low sexual satisfaction (p = 0.010) than CST occurring in childhood/adolescence. We found no significant differences in AAO risk between participants with childhood-only vs. adolescence-only CST (p’s > 0.05).
3.3. Comparing CST Duration and Developmental Timing Models in Predicting AAOs
We examined AIC scores to compare how well Model 1 (CST duration) and Model 2 (CST developmental timing) fit the data for each outcome. For all three AAOs, Models 1 and 2 had similar AIC scores (difference ≤ 10; see Table 3), suggesting that the two models do not meaningfully differ in how well they predict each AAO. AIC scores were highly similar (difference = 4) for fair/poor overall health and low sexual satisfaction, suggesting the two models are considerably redundant in predicting these AAOs.
To further examine for differences in how well CST duration and developmental timing predicted each outcome, we conducted a supplemental analysis using Vuong’s closeness test (data available by request). Vuong’s test is used to assess whether one model is closer to the true data-generating process than another, and is particularly sensitive to subtle differences in model fit [66]. For all AAOs, findings suggested that Model 2 (developmental timing) was significantly closer to the true model than Model 1 (duration). Although Vuong’s test indicated a statistically significant improvement with Model 2, the improvement is subtle and of limited practical significance as demonstrated by marginal differences in AIC scores. Given the strong bivariate association between CST duration and developmental timing [χ2 = 389.9, p < 0.001], it is reasonable and parsimonious to consider them conceptually redundant.
4. Discussion
The current study compared two conceptually related proxy measures of CST severity that are grounded in theoretical perspectives regarding CST’s effects on long-term well-being. We found measures of CST duration and developmental timing to be strongly correlated and redundant in their effects on three adverse adult outcomes. Participants who experienced CST lasting more than three years and those for whom CST occurred in both childhood and adolescence had a significantly elevated risk of reporting emotional health problems, fair/poor overall health, and low sexual satisfaction. Findings emphasize the role of trauma chronicity in driving long-term health outcomes and highlight the reflexive relationship between traumatic stress and developmental explanations for how CST influences well-being over the lifecourse, with key implications for future research and practice. Importantly, examinations of how CST chronicity influences long-term health trajectories among more recent populations are warranted.
4.1. Redundancy in the Effects of CST Duration and Developmental Timing on Adult Outcomes
In the current study, participants who experienced CST of extreme duration (≥4 years) or CST that occurred in both childhood and adolescence had roughly twice the risk of adverse adult outcomes (AAOs) as other participants. Approximately 11% of participants fell into both higher-risk categories (i.e., reported extreme duration CST that spanned across childhood and adolescence), representing a substantial sub-group of survivors who may be most vulnerable to AAOs across multiple life domains. Participants with childhood- or adolescent-only CST had similar AAO risk, which was significantly lower than those with CST in both periods. Our findings align with prior research that has linked trauma occurring in both childhood and adolescence to an elevated risk of anxiety, depression, and substance use [38], sexual victimization [71], endometriosis [27], hypertension [28], sleep problems [47], and reduced telomere length (i.e., faster cellular aging) [24] in adulthood. Collectively, this evidence points to the importance of prioritizing survivors of chronic CST that spanned multiple developmental periods, in efforts to establish best practices for CST screening and linkage-to-care among adult populations.
Our measures of CST duration and developmental timing were based on the same underlying metric (the ages at which CST experiences occurred), and similarly predicted each of the three AAOs. This suggests a redundancy in their effects that was further confirmed by the significant association between the two measures (e.g., 90% of participants with extreme duration CST had experiences that occurred in both childhood and adolescence). The lack of a meaningful difference in how the two measures predicted long-term health outcomes highlights the reflexive relationship between developmental and traumatic stress explanations for how CST influences adult well-being. The central parallel between these two explanations is the critical role of trauma chronicity in driving long-term effects.
Prior empirical work suggests that the developmental timing of CST may be an antecedent to duration, in that earlier onset CST increases the risk of repeated victimization [32,34,38,41,54,71,72,73]. Moreover, chronic trauma that begins earlier in youth may interrupt subsequent developmental tasks (e.g., impaired development of emotion regulation and coping skills) that increase the risk of repeated victimization [38,74]. Earlier onset and chronic CST may also be indicative of a higher-risk environment (e.g., co-occurring physical or emotional abuse) that enhances risk for a wide range of AAOs [38,75]. The relationship between CST duration and developmental timing creates methodological challenges in identifying the unique effects of either characteristic on AAO risk [30,38,74]. In utilizing measures of CST duration or developmental timing, researchers should use caution in interpreting findings as supporting either a traumatic stress or developmental explanation without accounting for the other.
Measures that assess the age of CST onset without accounting for duration may overlook chronic trauma experiences that confer the greatest long-term risk. This approach also neglects factors beyond age that influence developmental processes and related health outcomes (e.g., pubertal onset; prior experiences of trauma or chronic stress) [23,36,76,77]. For instance, adolescents from working-class or racially marginalized communities may experience daily stressors that continually activate stress response systems, contributing to higher health risks associated with faster cellular aging, elevated blood pressure, and inflammation [23]. In this context, CST victimization may have different impacts on health trajectories than for adolescents with lower degrees of chronic social stress. Thus, CST severity measures that rely on age overlook the array of biopsychosocial influences on relationships between age and health over the lifecourse [23], and may not be reliable indicators of CST’s developmental effects. In contrast, severity measures that address trauma chronicity allow for the examination of both developmental and traumatic stress-related explanations of CST’s long-term effects, and provide critical information on chronic CST experiences (e.g., duration of perpetrator-specific CST experiences; months/years between CST experiences) that confer the greatest long-term risk.
4.2. Research and Practice Implications
4.2.1. Implications for CST Severity Assessment
The ability of both CST duration and developmental timing measures to identify a sub-group of chronic CST survivors with significantly elevated AAO risk supports the measures’ validity in predicting differences in long-term outcomes. It is important that future research continues examining CST severity measurement strategies that account for trauma chronicity and establish evidence-based standards that can be translated into prevention and practice settings. Our measures of CST duration and developmental timing were based on retrospective reports of perpetrator-specific CST experiences; although these measures reflect an oversimplification of CST chronicity, they were successful in identifying survivor sub-groups with the greatest AAO risk. These and other strategies for assessing CST chronicity should be examined and applied across a variety of populations and settings to work toward a standardized measurement approach for use in research, prevention, and intervention efforts. Measures that allow for generating both duration and developmental timing variables are particularly valuable for examining how CST chronicity affects long-term well-being.
Findings from the current analysis and our prior investigation [1] suggest that a categorical, perpetrator-specific CST duration measure offers a precise, time-based approach for capturing both temporal and developmental effects of CST, and an effective tool to differentiate adult CST survivors with an elevated risk of adverse outcomes. Our approach assessed and categorized duration in terms of the total period (years) over which CST occurred, in line with other studies on childhood trauma [54,55,78,79,80]. In research and practice contexts, categorical measures are particularly advantageous for identifying sub-groups of CST survivors to prioritize in treatment and prevention efforts [63,81]. Our duration measure was developed with a rigorous, taxometric-based approach [63,66,67] to identify cut-points for categorization that aligned with significantly different levels of AAO risk [1]. Evidence of significant relationships between CST duration, developmental timing, and AAOs provides further support for the construct and known-groups validity of the duration measure. There is a need for additional research to examine and replicate relationships between CST duration categories and adult health outcomes among more current national samples.
Few prior studies have utilized CST severity measures that allow for differentiating sub-groups of survivors with elevated long-term health risk tied to chronic trauma. Some studies, including several of the larger U.S. adult studies that have retrospectively assessed CST (e.g., Refs. [82,83]), have examined the temporal aspects of severity by measuring the subjective frequency of CST. For instance, the Childhood Trauma Questionnaire is often used to assess how often participants experienced CST and other forms of childhood trauma (never, rarely, sometimes, often, or very often) [83,84,85]. However, this type of measure may introduce bias by conflating duration (e.g., number of months/years) with individuals’ perceptions of time. Moreover, frequency categories are often analyzed as continuous or binary variables (any vs. no CST), which inhibits the delineation of chronic CST survivor sub-groups who may face higher AAO risk. In research and practice, these types of subjective or global CST measures may be most beneficial as an initial screening tool to identify individuals with CST histories. Among those who report CST, a categorical severity measure can be administered to delineate and characterize chronic CST experiences that may confer a higher risk of adverse health outcomes.
Our findings are bolstered by a growing consensus in the field that measures which aggregate childhood trauma experiences (e.g., counts of adverse childhood experiences or dichotomous measures that combine multiple types of trauma) or severity characteristics (e.g., measures that combine characteristics into a continuous severity scale) may be insufficient for detecting survivors with elevated AAO risk [16,86,87,88,89,90]. Aggregated measures often mask the temporal effects of trauma by neglecting severity altogether, or by relying on assumptions that some trauma characteristics are inherently more severe than others, regardless of chronicity. In contrast, assessing duration provides a theoretically grounded approach for identifying chronic CST survivors who may have elevated AAO risk, while capturing information on developmental timing and other trauma characteristics that may influence severity (e.g., number of CST perpetrators or occurrences).
4.2.2. Implications for CST Study Design
In the U.S., most research on how CST relates to adult outcomes has utilized cross-sectional and retrospective CST assessment, which is subject to bias [15,30]. Cross-sectional designs are unable to address ongoing associations between trauma duration, developmental timing, and other severity-related characteristics (e.g., frequency, degree of force), hindering the ability to detect the impacts of severity characteristics on outcomes over time [8,30,31,32]. Recent work examining the agreement between prospective and retrospective reports of childhood trauma has produced mixed results and suggests that the validity of retrospective measures may vary in relation to the study methodology and sample [91,92,93].
To address these methodological challenges, more prospective and longitudinal studies to examine how CST relates to health trajectories over time are needed. For instance, some countries have used birth cohorts to examine associations between CST and AAOs across life domains [4,94,95,96]. In the U.S., several prospective youth cohorts have assessed childhood trauma and associated adult outcomes (e.g., The National Longitudinal Study of Adolescent Health [41]; Longitudinal Studies on Child Abuse and Neglect [74]). However, some of these cohorts have been limited to substantiated CST cases (e.g., formal reports to child welfare services) [74,97,98], which excludes many cases that go unreported [8,99]. Other studies use CST measures that overlook substantial proportions of survivors and obscure differences in long-term risk (e.g., assessments of CST perpetrated by parents/caregivers only; dichotomous CST exposure measures) [41,100]. Future research and policy efforts should consider strategies to improve prospective investigations of CST and other childhood trauma by using theory- and evidence-based measures with population-based longitudinal samples.
4.3. Strengths and Limitations
The NSHS provided a large, probability-based national sample of U.S. adults for the analyses of relationships between CST duration, developmental timing, and AAOs. Although prevalence estimates from historical samples may have limited generalizability to current cohorts, our prior work suggests that CST prevalence has remained relatively stable in the 30 years since the NSHS (for a detailed analysis comparing sample-weighted prevalence CST estimates from the NSHS with more recent U.S. adult samples, see [1]). We did not apply sample weights in the current analysis, which may also limit the generalizability of findings. Importantly, the NSHS sample was large enough to delineate a sample of over 500 CST survivors and compare moderately sized sub-groups in terms of AAO risk, which is uncommon among U.S. studies.
The NSHS included perpetrator-specific assessments of sexual trauma over the lifecourse, which allowed for the examination of chronic experiences of CST during childhood and adolescence. This approach offered a precise strategy for measuring CST severity that facilitated the identification of high-priority sub-groups of CST survivors for efforts to mitigate long-term health risk. Although the association between CST and AAOs is inherently sequential, retrospective CST reports may be biased due to memory lapses, avoidance coping, and cognitive stress responses that impact recall. Our analysis focused on three AAOs, using self-report measures that assessed more global dimensions of well-being; this may limit the comparability of our findings to other studies that have assessed specific physical, emotional, or sexual health outcomes or diagnoses. However, the use of global AAO measures reflects the reality that CST survivors may be susceptible to a range of long-term physical and psychosocial effects that impact overall well-being in multiple ways.
Our analysis demonstrates that measuring trauma duration offers a useful strategy for assessing the temporal and developmental aspects of CST severity and for identifying CST survivors with elevated long-term health risk. However, it was beyond the scope of this paper to examine the array of psychosocial, cultural, and structural factors that may influence relationships between CST severity and well-being over the lifecourse, or how these factors may have shifted over time (e.g., changes in public awareness of CST, technology-facilitated abuse, and mandatory reporting policies). For instance, the processes of disclosing CST and seeking formal/informal support are highly dynamic, and influenced by a wide range of psychological (e.g., shame or fear of not being believed), interpersonal (e.g., family of origin dynamics and social isolation), and socio-cultural factors (e.g., beliefs related to gender roles and sexual taboos) [101,102,103]. Over the last 30 years, factors such as increasing social support for sexual trauma survivors and access to online disclosure/support systems may have influenced how and when survivors seek help for CST-related health concerns. Chronic CST survivors may be more likely to seek support than other CST survivors [1], but more work is needed to understand how socio-cultural determinants influence long-term health trajectories following chronic CST. Further, since the current analysis was limited to U.S. adults in the 1990s, additional studies are needed to examine relationships between CST chronicity and health trajectories within other age groups, cultural contexts, and more contemporary samples.
Finally, our analysis did not account for other types of childhood trauma that often co-occur with CST and influence long-term trajectories of well-being (e.g., physical or emotional abuse) [4,87]. As a result, CST’s effects on AAOs may also reflect the impacts of other trauma experienced during youth. However, CST has demonstrated unique effects on long-term well-being, over and above other types of childhood trauma [24,40,87,104,105]. Moreover, CST assessment captures information about physical, psychological, and emotional components of sexual victimization (e.g., violence or coercion). Therefore, our findings regarding the importance of CST chronicity in driving AAO risk may provide insight into the effects of other chronic victimization experiences, warranting further examination of the chronicity of CST and other types of childhood trauma in future work.
5. Conclusions
Our study builds on prior work demonstrating the value of assessing chronic trauma in efforts to identify CST survivors with elevated risk of long-term adverse outcomes. We found that the effects of the developmental timing of CST on AAOs were redundant with the effects of duration, suggesting that measures of chronic CST offer information on both the developmental and traumatic stress-related effects of CST. There is a need for more current, national samples that include CST chronicity measures so that NSHS findings can be replicated in contemporary populations. In turn, this data can collectively inform efforts to develop standardized CST severity measures by prioritizing the assessment of chronic trauma. Standardizing CST measurement has important implications for research, practice, and policy aimed at better understanding the complexities of CST experiences, identifying survivors who are most at-risk for long-term adverse outcomes, and providing linkages to appropriate services and resources.
Author Contributions
Conceptualization, A.C.S. and J.A.C. (Joseph A. Catania); methodology, A.C.S., J.A.C. (Joseph A. Catania) and J.A.C. (Jesse A. Canchola); formal analysis, A.C.S. and J.A.C. (Jesse A. Canchola); writing—original draft preparation, A.C.S. and J.A.C. (Joseph A. Catania); writing—review and editing, A.C.S., J.A.C. (Joseph A. Catania), J.A.C. (Jesse A. Canchola) and M.M.D.; supervision, J.A.C. (Joseph A. Catania) and M.M.D.; funding acquisition, J.A.C. (Joseph A. Catania) and M.M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded through National Institutes of Health Grants to Drs. Catania (MH51523; MH105180; HD085780) and Dolcini (MH120512), as well as a P.F. & Nellie Buck Yerex Graduate Scholarship and a Postdoctoral Research Scholarship from Oregon State University to Dr. Schuyler.
Institutional Review Board Statement
The NSHS study was approved by the Institutional Review Board of the University of California, San Francisco. As this manuscript is only a secondary data analysis, Ethical approval is not necessary.
Informed Consent Statement
This study did not involve humans.
Data Availability Statement
The data that support the findings of this study are available in Sociometrics at https://www.socio.com/products/aids-petra-0204 (accessed 20 May 2025).
Acknowledgments
The authors would like to acknowledge the contributions of Lance Pollack to statistical support and of Erin Cosgrove to manuscript preparation. The authors also thank the study participants and interviewers for their time and contributions.
Conflicts of Interest
Jesse Canchola is affiliated with StatCon Statistical Consulting. His contributions to this manuscript were provided pro bono (uncompensated), and StatCon Statistical Consulting did not receive any payment related to this work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CST | Childhood sexual trauma |
| AAOs | Adverse adult outcomes |
| NSHS | National Sexual Health Survey |
| AIC | Akaike Information Criterion |
References
- Schuyler, A.C.; Catania, J.A. Trauma chronicity and the long-term needs of childhood sexual trauma survivors. Sexes 2022, 3, 367–384. [Google Scholar] [CrossRef]
- Browne, A.; Finkelhor, D. Impact of child sexual abuse: A review of the research. Psychol. Bull. 1986, 99, 66–77. [Google Scholar] [CrossRef]
- Fergusson, D.M.; McLeod, G.F.H.; Horwood, L.J. Childhood sexual abuse and adult developmental outcomes: Findings from a 30-year longitudinal study in New Zealand. Child Abus. Negl. 2013, 37, 664–674. [Google Scholar] [CrossRef]
- Guiney, H.; Caspi, A.; Ambler, A.; Belsky, J.; Kokaua, J.; Broadbent, J.; Cheyne, K.; Dickson, N.; Hancox, R.J.; Harrington, H.; et al. Childhood sexual abuse and pervasive problems across multiple life domains: Findings from a five-decade study. Dev. Psychopathol. 2024, 36, 219–235. [Google Scholar]
- Hailes, H.P.; Yu, R.; Danese, A.; Fazel, S. Long-term outcomes of childhood sexual abuse: An umbrella review. Lancet Psychiatry 2019, 6, 830–839. [Google Scholar] [CrossRef]
- Maniglio, R. The impact of child sexual abuse on health: A systematic review of reviews. Clin. Psychol. Rev. 2009, 29, 647–657. [Google Scholar] [CrossRef]
- Polusny, M.A.; Follette, V.M. Long-term correlates of child sexual abuse: Theory and review of the empirical literature. Appl. Prev. Psychol. 1995, 4, 143–166. [Google Scholar] [CrossRef]
- Putnam, F.W. Ten-Year Research Update Review: Child Sexual Abuse. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 269–278. [Google Scholar] [CrossRef]
- Fang, X.; Brown, D.S.; Florence, C.S.; Mercy, J.A. The economic burden of child maltreatment in the United States and implications for prevention. Child Abus. Negl. 2012, 36, 156–165. [Google Scholar] [CrossRef]
- Langevin, R.; Hébert, M.; Cabecinha-Alati, S. Multilevel factors associated with the intergenerational continuity of child sexual abuse. Child. Youth Serv. Rev. 2020, 113, 105007. [Google Scholar] [CrossRef]
- Letourneau, E.J.; Brown, D.S.; Fang, X.; Hassan, A.; Mercy, J.A. The economic burden of child sexual abuse in the United States. Child Abus. Negl. 2018, 79, 413–422. [Google Scholar] [CrossRef]
- Strohacker, E.R.; Pontes, N.M.; Pontes, M.C. Interactions Between Forced Sexual Intercourse Victimization and Gender on Violent Behaviors: Youth Risk Behavior Survey 2017–2019. Violence Vict. 2024, 39, 475–2022. [Google Scholar] [CrossRef] [PubMed]
- Boxer, P.; Sloan-Power, E. Coping With Violence: A Comprehensive Framework and Implications for Understanding Resilience. Trauma Violence Abus. 2013, 14, 209–221. [Google Scholar]
- Walsh, K.; Fortier, M.A.; DiLillo, D. Adult coping with childhood sexual abuse: A theoretical and empirical review. Aggress. Violent Behav. 2010, 15, 1–13. [Google Scholar] [CrossRef]
- Hulme, P.A. Retrospective Measurement of Childhood Sexual Abuse: A Review of Instruments. Child Maltreat 2004, 9, 201–217. [Google Scholar]
- Kilimnik, C.D.; Pulverman, C.S.; Meston, C.M. Methodologic Considerations for the Study of Childhood Sexual Abuse in Sexual Health Outcome Research: A Comprehensive Review. Sex. Med. Rev. 2018, 6, 176–187. [Google Scholar] [CrossRef]
- Laajasalo, T.; Cowley, L.E.; Otterman, G.; Lamela, D.; Rodrigues, L.B.; Jud, A.; Kemp, A.; Naughton, A.; Hurt, L.; Soldino, V.; et al. Current issues and challenges in the definition and operationalization of child maltreatment: A scoping review. Child Abus. Negl. 2023, 140, 106187. [Google Scholar] [CrossRef]
- Mathews, B.; Pacella, R.; Dunne, M.P.; Simunovic, M.; Marston, C. Improving measurement of child abuse and neglect: A systematic review and analysis of national prevalence studies. PLoS ONE 2020, 15, e0227884. [Google Scholar] [CrossRef]
- Hoier, T.S.; Shawchuck, C.R.; Pallotta, G.M.; Freeman, T.; Inderbitzen-Pisaruk, H.; MacMillan, V.M.; Malinosky-Rummell, R.; Greene, A.L. The impact of sexual abuse: A cognitive-behavioral model. In The Sexual Abuse of Children: Clinical Issues; O’Donohue, W., Geer, J.H., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1992; pp. 100–142. [Google Scholar]
- Aldwin, C. Stress, Coping, & Development: An Integrative Perspective, 2nd ed.; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Blaustein, M.; Kinniburgh, K. Treating Traumatic Stress in Children and Adolescents: How to Foster Resilience Through Attachment, Self-Regulation, and Competency, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Pynoos, R.S.; Steinberg, A.M.; Wraith, R. A developmental model of childhood traumatic stress. In Developmental Psychopathology: Risk, Disorder, and Adaptation; John Wiley & Sons: Hoboken, NJ, USA, 1995. [Google Scholar]
- Geronimus, A.T. Weathering: The Extraordinary Stress of Ordinary Life in an Unjust Society; Little Brown Spark: New York, NY, USA, 2023. [Google Scholar]
- Warner, E.T.; Zhang, Y.; Gu, Y.; Taporoski, T.P.; Pereira, A.; DeVivo, I.; Spence, N.D.; Cozier, Y.; Palmer, J.R.; Kanaya, A.M.; et al. Physical and sexual abuse in childhood and adolescence and leukocyte telomere length: A pooled analysis of the study on psychosocial stress, spirituality, and health. PLoS ONE 2020, 15, e0241363. [Google Scholar]
- Beitchman, J.H.; Zucker, K.J.; Hood, J.E.; DaCosta, G.A.; Akman, D.; Cassavia, E. A review of the long-term effects of child sexual abuse. Child Abus. Negl. 1992, 16, 101–118. [Google Scholar] [CrossRef]
- Casey, E.A.; Nurius, P.S. Trauma Exposure and Sexual Revictimization Risk: Comparisons Across Single, Multiple Incident, and Multiple Perpetrator Victimizations. Violence Against Women 2005, 11, 505–530. [Google Scholar]
- Harris, H.R.; Wieser, F.; Vitonis, A.F.; Rich-Edwards, J.; Boynton-Jarrett, R.; Bertone-Johnson, E.R.; Missmer, S.A. Early life abuse and risk of endometriosis. Hum. Reprod. 2018, 33, 1657–1668. [Google Scholar] [CrossRef]
- Riley, E.H.; Wright, R.J.; Jun, H.J.; Hibert, E.N.; Rich-Edwards, J.W. Hypertension in adult survivors of child abuse: Observations from the Nurses’ Health Study II. J. Epidemiol. Community Health 2010, 64, 413–418. [Google Scholar] [CrossRef]
- van Veen, T.; Wardenaar, K.J.; Carlier, I.V.E.; Spinhoven, P.; Penninx, B.W.J.H.; Zitman, F.G. Are childhood and adult life adversities differentially associated with specific symptom dimensions of depression and anxiety? Testing the tripartite model. J. Affect. Disord. 2013, 146, 238–245. [Google Scholar] [CrossRef]
- Trickett, P.K.; McBride-Chang, C. The developmental impact of different forms of child abuse and neglect. Dev. Rev. 1995, 15, 311–337. [Google Scholar] [CrossRef]
- Cicchetti, D.; Toth, S.L. A developmental perspective on child abuse and neglect. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 541–565. [Google Scholar] [CrossRef]
- Dunn, E.C.; Nishimi, K.; Gomez, S.H.; Powers, A.; Bradley, B. Developmental timing of trauma exposure and emotion dysregulation in adulthood: Are there sensitive periods when trauma is most harmful? J. Affect. Disord. 2018, 227, 869–877. [Google Scholar] [CrossRef]
- Hagele, D.M. The impact of maltreatment on the developing child. N. Carol. Med. J. 2005, 66, 356–359. [Google Scholar] [CrossRef]
- Downs, W.R. Developmental considerations for the effects of childhood sexual abuse. J. Interpers. Violence 1993, 8, 331–345. [Google Scholar] [CrossRef]
- Bremner, J.D.; Vermetten, E. Stress and development: Behavioral and biological consequences. Dev. Psychopathol. 2001, 13, 473–489. [Google Scholar] [CrossRef]
- Scoglio, A.A.J.; Kraus, S.W.; Saczynski, J.; Jooma, S.; Molnar, B.E. Systematic Review of Risk and Protective Factors for Revictimization After Child Sexual Abuse. Trauma Violence Abus. 2019, 22, 41–53. [Google Scholar]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar]
- Russotti, J.; Warmingham, J.M.; Duprey, E.B.; Handley, E.D.; Manly, J.T.; Rogosch, F.A.; Cicchetti, D. Child maltreatment and the development of psychopathology: The role of developmental timing and chronicity. Child Abus. Negl. 2021, 120, 105215. [Google Scholar] [CrossRef]
- Jackson, Y.; McGuire, A.; Tunno, A.M.; Makanui, P.K. A reasonably large review of operationalization in child maltreatment research: Assessment approaches and sources of information in youth samples. Child Abus. Negl. 2019, 87, 5–17. [Google Scholar] [CrossRef]
- Capretto, J.J. Developmental Timing of Childhood Physical and Sexual Maltreatment Predicts Adult Depression and Post-Traumatic Stress Symptoms. J. Interpers. Violence 2020, 35, 2558–2582. [Google Scholar] [CrossRef]
- Dunn, E.C.; McLaughlin, K.A.; Slopen, N.; Rosand, J.; Smoller, J.W. Developmental timing of child maltreatment and symptoms of depression and suicidal ideation in young adulthood: Results from The National Longitudinal Study of Adolescent Health. Depress. Anxiety 2013, 30, 955–964. [Google Scholar]
- Freeman, R.C.; Collier, K.; Parillo, K.M. Early life sexual abuse as a risk factor for crack cocaine use in a sample of community-recruited women at high risk for illicit drug use. Am. J. Drug Alcohol. Abus. 2002, 28, 109–131. [Google Scholar]
- Strathdee, S.A.; Hogg, R.S.; Martindale, S.L.; Cornelisse, P.G.; Craib, K.J.; Montaner, J.S.; O’SHaughnessy, M.V.; Schechter, M.T. Determinants of sexual risk-taking among young HIV-negative gay and bisexual men. J. Acquir. Immune Defic. Syndr. Hum. Retrovirol 1998, 19, 61–66. [Google Scholar][Green Version]
- Miron, L.R.; Orcutt, H.K. Pathways from childhood abuse to prospective revictimization: Depression, sex to reduce negative affect, and forecasted sexual behavior. Child Abus. Negl. 2014, 38, 1848–1859. [Google Scholar] [CrossRef]
- Maseroli, E.; Scavello, I.; Campone, B.; Di Stasi, V.; Cipriani, S.; Felciai, F.; Camartini, V.; Magini, A.; Castellini, G.; Ricca, V.; et al. Psychosexual correlates of unwanted sexual experiences in women consulting for female sexual dysfunction according to their timing across the life span. J. Sex. Med. 2018, 15, 1739–1751. [Google Scholar] [CrossRef]
- Adams, J.; Mrug, S.; Knight, D.C. Characteristics of child physical and sexual abuse as predictors of psychopathology. Child Abus. Negl. 2018, 86, 167–177. [Google Scholar] [CrossRef]
- McWhorter, K.L.; Parks, C.G.; D’Aloisio, A.A.; Rojo-Wissar, D.M.; Sandler, D.P.; Jackson, C.L. Traumatic childhood experiences and multiple dimensions of poor sleep among adult women. Sleep 2019, 42, zsz108. [Google Scholar] [CrossRef]
- Kaukinen, C.; DeMaris, A. Age at First Sexual Assault and Current Substance Use and Depression. J. Interpers. Violence 2005, 20, 1244–1270. [Google Scholar] [CrossRef]
- Hannan, S.M.; Orcutt, H.K.; Miron, L.R.; Thompson, K.L. Childhood Sexual Abuse and Later Alcohol-Related Problems: Investigating the Roles of Revictimization, PTSD, and Drinking Motivations Among College Women. J. Interpers. Violence 2015, 32, 2118–2138. [Google Scholar] [CrossRef]
- Williams, J.K.; Wilton, L.; Magnus, M.; Wang, L.; Wang, J.; Dyer, T.P.; Koblin, B.A.; Hucks-Ortiz, C.; Fields, S.D.; Shoptaw, S.; et al. Relation of Childhood Sexual Abuse, Intimate Partner Violence, and Depression to Risk Factors for HIV Among Black Men Who Have Sex With Men in 6 US Cities. Am. J. Public Health 2015, 105, 2473–2481. [Google Scholar] [CrossRef]
- Boroughs, M.S.; Valentine, S.E.; Ironson, G.H.; Shipherd, J.C.; Safren, S.A.; Taylor, S.W.; Dale, S.K.; Baker, J.S.; Wilner, J.G.; O’cLeirigh, C. Complexity of Childhood Sexual Abuse: Predictors of Current Post-Traumatic Stress Disorder, Mood Disorders, Substance Use, and Sexual Risk Behavior Among Adult Men Who Have Sex with Men. Arch. Sex. Behav. 2015, 44, 1891–1902. [Google Scholar] [CrossRef]
- Loeb, T.B.; Gaines, T.; Wyatt, G.E.; Zhang, M.; Liu, H. Associations between child sexual abuse and negative sexual experiences and revictimization among women: Does measuring severity matter? Child. Abus. Negl. 2011, 35, 946–955. [Google Scholar] [CrossRef]
- Paul, J.; Catania, J.A.; Pollack, L.M. Childhood/adolescent sexual coercion among men who have sex with men: Understanding patterns of sexual behavior and sexual risk. In Sexual Development in Childhood; Indiana University Press: Bloomington, IN, USA, 2003; pp. 327–358. [Google Scholar]
- Rodriguez, N.; Ryan, S.W.; Rowan, A.B.; Foy, D.W. Posttraumatic stress disorder in a clinical sample of adult survivors of childhood sexual abuse. Child. Abus. Negl. 1996, 20, 943–952. [Google Scholar] [CrossRef]
- Ullman, S.E. Relationship to Perpetrator, Disclosure, Social Reactions, and PTSD Symptoms in Child Sexual Abuse Survivors. J. Child Sex. Abus. 2007, 16, 19–36. [Google Scholar] [CrossRef]
- Godbout, N.; Sabourin, S.; Lussier, Y. Child Sexual Abuse and Adult Romantic Adjustment: Comparison of Single- and Multiple-Indicator Measures. J. Interpers. Violence 2009, 24, 693–705. [Google Scholar] [CrossRef]
- Bigras, N.; Vaillancourt-Morel, M.P.; Nolin, M.C.; Bergeron, S. Associations between Childhood Sexual Abuse and Sexual Well-being in Adulthood: A Systematic Literature Review. J. Child Sex. Abus. 2021, 30, 332–352. [Google Scholar] [CrossRef]
- Mahoney, J.; Rueschemeyer, D. Comparative historical analysis. In Comparative Historical Analysis in the Social Sciences; Cambridge University Press: Cambridge, UK, 2003; pp. 3–38. [Google Scholar]
- McGuire, W.J. Historical comparisons: Testing psychological hypotheses with cross-era data (1). Int. J. Psychol. 1976, 11, 161–183. [Google Scholar] [CrossRef]
- Sandfort, T.G.M.; Orr, M.; Hirsch, J.S.; Santelli, J. Long-Term Health Correlates of Timing of Sexual Debut: Results From a National US Study. Am. J. Public Health 2008, 98, 155–161. [Google Scholar] [CrossRef]
- Hyland, A.; Piazza, K.M.; Hovey, K.M.; Ockene, J.K.; Andrews, C.A.; Rivard, C.; Wactawski-Wende, J. Associations of lifetime active and passive smoking with spontaneous abortion, stillbirth and tubal ectopic pregnancy: A cross-sectional analysis of historical data from the Women’s Health Initiative. Tob. Control 2015, 24, 328–335. [Google Scholar]
- University of California San Francisco, Department of Medicine. Prevention Science. National Sexual Health Survey (NSHS). 2016. Available online: https://prevention.ucsf.edu/research-project/national-sexual-health-survey-nshs (accessed on 15 May 2025).
- Kessler, R.C. The Categorical versus Dimensional Assessment Controversy in the Sociology of Mental Illness. J. Health Soc. Behav. 2002, 43, 171–188. [Google Scholar] [CrossRef]
- Catania, J.A.; Paul, J.; Osmond, D.; Folkman, S.; Pollack, L.; Canchola, J.; Chang, J.; Neilands, T. Mediators of childhood sexual abuse and high-risk sex among men-who-have-sex-with-men. Child. Abus. Negl. 2008, 32, 925–940. [Google Scholar] [CrossRef]
- Paul, J.P.; Catania, J.; Pollack, L.; Stall, R. Understanding childhood sexual abuse as a predictor of sexual risk-taking among men who have sex with men: The Urban Men’s Health Study. Child. Abus. Negl. 2001, 25, 557–584. [Google Scholar] [CrossRef]
- Ruscio, J.; Ruscio, A.M.; Carney, L.M. Performing Taxometric Analysis to Distinguish Categorical and Dimensional Variables. J. Exp. Psychopathol. 2011, 2, 170–196. [Google Scholar] [CrossRef]
- Sakaluk, J.K. Expanding statistical frontiers in sexual science: Taxometric, invariance, and equivalence testing. J. Sex Res. 2019, 56, 475–510. [Google Scholar] [CrossRef]
- Humphrey, J.A.; White, J.W. Women’s vulnerability to sexual assault from adolescence to young adulthood. J. Adolesc. Health 2000, 27, 419–424. [Google Scholar] [CrossRef]
- RAND Corporation. 36-Item Short Form Survey (SF-36). 1990. Available online: https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form.html (accessed on 15 May 2025).
- Burnham, K.P.; Anderson, D.R. Information and Likelihood Theory: A basis for model selection and inference. In Model Selection and Multimodal Inference: A Practical Information-Theoretic Approach, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Pho, K.H.; Ly, S.; Ly, S.; Lukusa, T.M. Comparison among Akaike Information Criterion, Bayesian Information Criterion, and Vuong’s Test in model selection: A case study of violated speed regulation in Taiwan. J. Adv. Eng. Comput. 2019, 3, 293–303. [Google Scholar]
- Kim, H.; Drake, B. Cumulative Prevalence of Onset and Recurrence of Child Maltreatment Reports. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 1175–1183. [Google Scholar] [CrossRef]
- Proctor, L.J.; Aarons, G.A.; Dubowitz, H.; English, D.J.; Lewis, T.; Thompson, R.; Hussey, J.M.; Litrownik, A.J.; Roesch, S.C. Trajectories of Maltreatment Re-Reports From Ages 4 to 12: Evidence for Persistent Risk After Early Exposure. Child Maltreat. 2012, 17, 207–217. [Google Scholar] [CrossRef]
- English, D.J.; Graham, J.C.; Litrownik, A.J.; Everson, M.; Bangdiwala, S.I. Defining maltreatment chronicity: Are there differences in child outcomes? Child Abus. Negl. 2005, 29, 575–595. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. Re-victimization patterns in a national longitudinal sample of children and youth. Child Abus. Negl. 2007, 31, 479–502. [Google Scholar] [CrossRef]
- Mathews, B.; Collin-Vézina, D. Child sexual abuse: Toward a conceptual model and definition. Trauma Violence Abus. 2019, 20, 131–148. [Google Scholar]
- Kilimnik, C.D.; Meston, C.M. A Developmentally Relevant Approach to Classifying Nonconsensual Sexual Experiences in the Study of Women’s Sexual Well-Being. J. Sex Res. 2018, 55, 824–836. [Google Scholar] [CrossRef]
- Hodgdon, H.B.; Spinazzola, J.; Briggs, E.C.; Liang, L.J.; Steinberg, A.M.; Layne, C.M. Maltreatment type, exposure characteristics, and mental health outcomes among clinic referred trauma-exposed youth. Child. Abus. Negl. 2018, 82, 12–22. [Google Scholar]
- Lombera, A.; Lee, A.H.; Sharma-Patel, K.; Brown, E.J. Threat-specific maltreatment exposure: Comparison of measurement models and associations with internalizing, externalizing, and PTSD symptoms. Child. Abus. Negl. 2021, 115, 105010. [Google Scholar] [CrossRef]
- Otten, D.; Schalinski, I.; Fegert, J.M.; Jud, A.; Brähler, E.; Bürgin, D.; Clemens, V. Child Maltreatment Characteristics and Adult Physical Multimorbidity in Germany. JAMA Netw. Open 2025, 8, e2456050. [Google Scholar] [CrossRef]
- Coghill, D.; Sonuga-Barke, E.J.S. Annual Research Review: Categories versus dimensions in the classification and conceptualisation of child and adolescent mental disorders—Implications of recent empirical study. J. Child Psychol. Psychiatry 2012, 53, 469–489. [Google Scholar] [CrossRef] [PubMed]
- Afifi, T.O.; Sareen, J.; Fortier, J.; Taillieu, T.; Turner, S.; Cheung, K.; Henriksen, C.A. Child maltreatment and eating disorders among men and women in adulthood: Results from a nationally representative United States sample. Int. J. Eat. Disord. 2017, 50, 1281–1296. [Google Scholar] [CrossRef] [PubMed]
- Kuhlman, K.R.; Robles, T.F.; Bower, J.E.; Carroll, J.E. Screening for childhood adversity: The what and when of identifying individuals at risk for lifespan health disparities. J. Behav. Med. 2018, 41, 516–527. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar] [CrossRef]
- Mishra, A.A.; Marceau, K. Co-occurring childhood maltreatment exposure and depressive symptoms in adulthood: Testing differential effects of stress dysregulation and perceived stress. Aging Ment. Health 2019, 24, 1837–1846. [Google Scholar] [CrossRef]
- Baldwin, J.R.; Caspi, A.; Meehan, A.J.; Ambler, A.; Arseneault, L.; Fisher, H.L.; Harrington, H.; Matthews, T.; Odgers, C.L.; Poulton, R.; et al. Population vs Individual Prediction of Poor Health From Results of Adverse Childhood Experiences Screening. JAMA Pediatr. 2021, 175, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Briggs, E.C.; Amaya-Jackson, L.; Putnam, K.T.; Putnam, F.W. All adverse childhood experiences are not equal: The contribution of synergy to adverse childhood experience scores. Am. Psychol. 2021, 76, 243–252. [Google Scholar] [CrossRef]
- Buczó, D.; Koós, M.; Nagy, L.; Demetrovics, Z.; Bőthe, B. Further Investigation on Sexual Abuse Experiences: Revisiting the Psychometric Properties of the Sexual Abuse History Questionnaire and the Content of its Open-Ended Item. Sex. Res. Soc. Policy 2025, 22, 211–225. [Google Scholar] [CrossRef]
- DeLisi, M.; Drury, A.J.; Elbert, M.J. Frequency, chronicity, and severity: New specification of adverse childhood experiences among federal sexual offenders. Forensic Sci. Int. Mind Law 2021, 2, 100051. [Google Scholar] [CrossRef]
- Dolson, R.A.; Morelen, D.M.; Dodd, J.C.; Clements, A.D. Pocket ACE: Child sexual abuse survivors missed by the ACEs Study Questionnaire. Child Abus. Negl. 2021, 117, 105049. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, J.R.; Reuben, A.; Newbury, J.B.; Danese, A. Agreement Between Prospective and Retrospective Measures of Childhood Maltreatment: A Systematic Review and Meta-analysis. JAMA Psychiatry 2019, 76, 584–593. [Google Scholar]
- Coleman, O.; Baldwin, J.R.; Dalgleish, T.; Rose-Clarke, K.; Widom, C.S.; Danese, A. Research Review: Why do prospective and retrospective measures of maltreatment differ? A narrative review. J. Child Psychol. Psychiatry 2024, 65, 1662–1677. [Google Scholar] [CrossRef]
- Nivison, M.D.; Filetti, C.R.; Carlson, E.A.; Jacobvitz, D.B.; Roisman, G.I. Agreement between retrospective and prospective assessments of childhood abuse revisited. Dev. Psychopathol. 2024, 37, 1190–1199. [Google Scholar] [CrossRef]
- Newbury, J.B.; Arseneault, L.; Moffitt, T.E.; Caspi, A.; Danese, A.; Baldwin, J.R.; Fisher, H.L. Measuring childhood maltreatment to predict early-adult psychopathology: Comparison of prospective informant-reports and retrospective self-reports. J. Psychiatr. Res. 2018, 96, 57–64. [Google Scholar] [PubMed]
- Dunn, E.C.; Soare, T.W.; Raffeld, M.R.; Busso, D.S.; Crawford, K.M.; Davis, K.A.; Fisher, V.A.; Slopen, N.; Smith, A.D.; Tiemeier, H.; et al. What life course theoretical models best explain the relationship between exposure to childhood adversity and psychopathology symptoms: Recency, accumulation, or sensitive periods? Psychol. Med. 2018, 48, 2562–2572. [Google Scholar] [CrossRef]
- Dunn, E.C.; Nishimi, K.; Neumann, A.; Renaud, A.; Cecil, C.A.M.; Susser, E.S.; Tiemeier, H. Time-Dependent Effects of Exposure to Physical and Sexual Violence on Psychopathology Symptoms in Late Childhood: In Search of Sensitive Periods in Development. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 283–295.e4. [Google Scholar] [CrossRef] [PubMed]
- Negriff, S.; Schneiderman, J.U.; Trickett, P.K. Child maltreatment and sexual risk behavior: Maltreatment types and gender differences. J. Dev. Behav. Pediatr. 2015, 36, 708–716. [Google Scholar]
- Shenk, C.E.; Felt, J.M.; Ram, N.; O’Donnell, K.J.; Sliwinski, M.J.; Pokhvisneva, I.; Benson, L.; Meaney, M.J.; Putnam, F.W.; Noll, J.G. Cortisol trajectories measured prospectively across thirty years of female development following exposure to childhood sexual abuse: Moderation by epigenetic age acceleration at midlife. Psychoneuroendocrinology 2022, 136, 105606. [Google Scholar]
- Finkelhor, D. Current information on the scope and nature of child sexual abuse. Future Child. 1994, 4, 31–53. [Google Scholar] [CrossRef] [PubMed]
- Gewirtz-Meydan, A.; Finkelhor, D. Sexual Abuse and Assault in a Large National Sample of Children and Adolescents. Child Maltreat. 2019, 25, 203–214. [Google Scholar]
- Alaggia, R.; Collin-Vézina, D.; Lateef, R. Facilitators and barriers to child sexual abuse (CSA) disclosures: A research update (2000–2016). Trauma Violence Abus. 2019, 20, 260–283. [Google Scholar] [CrossRef]
- Lemaigre, C.; Taylor, E.P.; Gittoes, C. Barriers and facilitators to disclosing sexual abuse in childhood and adolescence: A systematic review. Child Abus. Negl. 2017, 70, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Tener, D.; Murphy, S.B. Adult Disclosure of Child Sexual Abuse: A Literature Review. Trauma Violence Abus. 2015, 16, 391–400. [Google Scholar] [CrossRef] [PubMed]
- MacIntosh, H.B.; Ménard, A.D. Couple and parenting functioning of childhood sexual abuse survivors: A systematic review of the literature (2001–2018). J. Child Sex. Abus. 2021, 30, 353–384. [Google Scholar] [CrossRef] [PubMed]
- Noll, J.G. Child Sexual Abuse as a Unique Risk Factor for the Development of Psychopathology: The Compounded Convergence of Mechanisms. Annu. Rev. Clin. Psychol. 2021, 17, 439–464. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.