
The Effect of Faecal Microbiota Transplantation on Cognitive Function in Cognitively Healthy Adults with Irritable Bowel Syndrome: Protocol for a Randomised, Placebo-Controlled, Double-Blinded Pilot Study

 , and
, and 
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Experimental Design
2.1. Outcome Measures
- Primary outcome: Cognitive performance, assessed using the Cambridge Neuropsychological Test Automated Battery (CANTAB), which includes subtests for memory, attention, processing speed, and executive function.
- Secondary outcomes: Mood, measured using the Depression Anxiety Stress Scale (DASS-42), and IBS symptom severity, measured using the IBS Symptom Severity Score (IBS-SSS). The IBS Quality of Life (IBS-QoL) questionnaire is administered but will not be analysed in this sub-study.
- Tertiary outcomes: Stool-based gut microbiome composition and function (via shotgun metagenomic sequencing and SCFA quantification) and plasma-based biomarkers, including pro-inflammatory cytokines, short-chain fatty acids, and tryptophan metabolites.
2.2. Materials
- ColOff stool collection device (Zymo Research, Irvine, CA, USA, R1101-2-5).
- DNA/RNA Shield Fecal Collection Tube (Zymo Research, Irvine, CA, USA, R1101).
- Glycerol, for molecular biology, ≥99.0% (Sigma Aldrich, Burlington, MA, USA, G5516).
- Phosphate-buffered saline, pH 7.4, sterile-filtered, suitable for cell culture (Sigma Aldrich, Burlington, MA, USA, P4474).
- Transfer pipette (Sigma Aldrich, Burlington, MA, USA, HS206371C).
- 60 mL syringes without needle (Terumo, Tokyo, Japan, SS60L).
2.3. Equipment
- iPad (7th generation, Apple Inc., Cupertino, CA, USA);
- −80 °C freezer (ThermoFisher Scientific, Waltham, MA, USA, TSX60086FA);
- LC-MS system (SCIEX QTRAP 7500);
- Proteomics for cytokines (Olink Target 48 cytokines).
3. Procedure
3.1. Intervention Preparation
- Screen potential stool donors according to TGA Therapeutic Goods Order 105 for eligibility.
- Collect stool in a sterile bucket within 6 h after defaecation.
- Weigh stool.
- Mix stool with phosphate-buffered saline and ten per cent pharmaceutical-grade glycerol to reach a ten percent concentration of stool.
- Draw the resulting faecal suspension into 60 mL syringes labelled according to TGA Therapeutic Goods Order 107.
- Produce placebo by mixing glycerol and saline solution (ratio 5:1), 5 g fibre, and 2 mL food colouring per litre.
- Draw the resulting suspension into 60 mL syringes.
- Cover all syringes in aluminium foil to ensure blinding.
- Store at −80 °C.
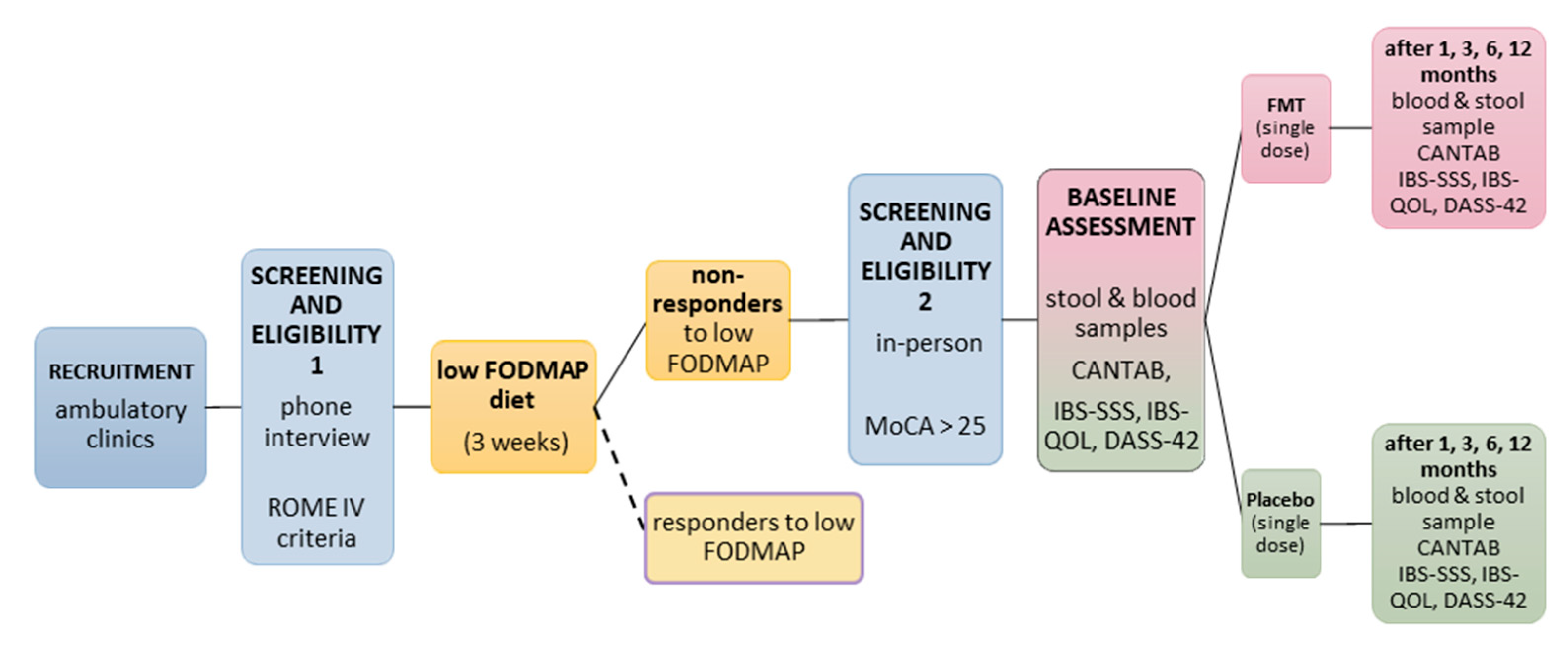
3.2. Pre-Treatment Phase (~3 Weeks)
- Recruit participants, provide study information, and obtain written informed consent (for the consent form, see Supplementary Materials).
- Conduct MoCA and confirm a score of ≥26.
- Refer potential participants to study dietician for introduction to low FODMAP diet.
- Study dietician supervises the diet for three weeks. Adherence is monitored through food diaries and weekly phone calls.
- Participants complete the IBS-SSS during their first appointment with the dietician and again after 21 days on the diet.
- Score IBS-SSS.
 CRITICAL STEP Only invite participants with a <50-point IBS-SSS reduction and a MocA score of >25 to the baseline visit.
CRITICAL STEP Only invite participants with a <50-point IBS-SSS reduction and a MocA score of >25 to the baseline visit.3.3. Baseline Assessment (~2 h)
- Administer CANTAB, DASS-42, and IBS-SSS.
- Draw blood (2 × 9 mL EDTA tubes).
- Provide participant with a stool sampling kit (see Supplementary File S2).
- Centrifuge whole blood samples at 4 °C for 10 min to obtain plasma. Aliquot plasma into 1.5 mL Eppendorf tubes and store at −80 °C.
CRITICAL STEP Process whole blood samples within 60 min of collection.3.4. Intervention Visit (~1 h)
- Thaw FMT or placebo syringes in an ice bath for two hours.
- Collect stool sample from participant and store at −80 °C.
- Provide participant with a fresh stool sampling kit for use before the follow-up visit.
- Administer 60 mL of the assigned treatment via rectal retention enema while the participant lies in a left lateral position.
 PAUSE STEP Ask participants to remain in the lateral position for 20 min under medical supervision to ensure adherence.
PAUSE STEP Ask participants to remain in the lateral position for 20 min under medical supervision to ensure adherence.3.5. Follow-Up Visits (1, 3, 6, 12 Months After Intervention)
4. Expected Results
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACTRN | Australian New Zealand Clinical Trials Registry Number |
| AD | Alzheimer’s Disease |
| CANTAB | Cambridge Neuropsychological Test Automated Battery |
| DASS-42 | Depression Anxiety Stress Scale (42-item version) |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| FMT | Faecal Microbiota Transplantation |
| IBS | Irritable Bowel Syndrome |
| IBS-QoL | IBS Quality of Life Instrument |
| IBS-SSS | IBS Symptom Severity Score |
| IL-6 | Interleukin-6 |
| LBP | Lipopolysaccharide-Binding Protein |
| LC-MS | Liquid Chromatography–Mass Spectrometry |
| MoCA | Montreal Cognitive Assessment |
| OTS | One-Touch Stockings of Cambridge |
| PAL | Paired Associates Learning |
| PRM | Pattern Recognition Memory |
| rCDI | Recurrent Clostridioides difficile Infection |
| RTI | Reaction Time |
| SCFA | Short-Chain Fatty Acid |
| SPIRIT | Standard Protocol Items: Recommendations for Interventional Trials |
| SWM | Spatial Working Memory |
| TGA | Therapeutic Goods Administration |
| TGO | Therapeutic Goods Order |
| VRM | Verbal Recognition Memory |
References
- Green, J.E.; Davis, J.A.; Berk, M.; Hair, C.; Loughman, A.; Castle, D.; Athan, E.; Nierenberg, A.A.; Cryan, J.F.; Jacka, F.; et al. Efficacy and safety of fecal microbiota transplantation for the treatment of diseases other than clostridium difficile infection: A systematic review and meta-analysis. Gut Microbes 2020, 12, 1854640. [Google Scholar] [CrossRef] [PubMed]
- Jemimah, S.; Chabib, C.M.M.; Hadjileontiadis, L.; AlShehhi, A. Gut microbiome dysbiosis in alzheimer’s disease and mild cognitive impairment: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0285346. [Google Scholar] [CrossRef]
- Segal, J.P.; Mullish, B.H.; Quraishi, M.N.; Iqbal, T.; Marchesi, J.R.; Sokol, H. Mechanisms underpinning the efficacy of faecal microbiota transplantation in treating gastrointestinal disease. Ther. Adv. Gastroenterol. 2020, 13, 1756284820946904. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; O’Riordan, K.J.; Cowan, C.S.M.; Sandhu, K.V.; Bastiaanssen, T.F.S.; Boehme, M.; Codagnone, M.G.; Cussotto, S.; Fulling, C.; Golubeva, A.V.; et al. The microbiota-gut-brain axis. Physiol. Rev. 2019, 99, 1877–2013. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, W.; Lin, Z.; Zheng, C.; Chen, S.; Zhou, H.; Liu, Z. Preliminary evidence for developing safe and efficient fecal microbiota transplantation as potential treatment for aged related cognitive impairments. Front. Cell. Infect. Microbiol. 2023, 13, 1103189. [Google Scholar] [CrossRef]
- Cheng, Y.; Tan, G.; Zhu, Q.; Wang, C.; Ruan, G.; Ying, S.; Qie, J.; Hu, X.; Xiao, Z.; Xu, F.; et al. Efficacy of fecal microbiota transplantation in patients with parkinson’s disease: Clinical trial results from a randomized, placebo-controlled design. Gut Microbes 2023, 15, 2284247. [Google Scholar] [CrossRef]
- Park, S.H.; Lee, J.H.; Kim, J.S.; Kim, T.J.; Shin, J.; Im, J.H.; Cha, B.; Lee, S.; Kwon, K.S.; Shin, Y.W.; et al. Fecal microbiota transplantation can improve cognition in patients with cognitive decline and clostridioides difficile infection. Aging 2022, 14, 6449–6466. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Gavis, E.A.; Fagan, A.; Wade, J.B.; Thacker, L.R.; Fuchs, M.; Patel, S.; Davis, B.; Meador, J.; Puri, P.; et al. A randomized clinical trial of fecal microbiota transplant for alcohol use disorder. Hepatology 2021, 73, 1688–1700. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Salzman, N.; Acharya, C.; Takei, H.; Kakiyama, G.; Fagan, A.; White, M.B.; Gavis, E.A.; Holtz, M.L.; Hayward, M.; et al. Microbial functional change is linked with clinical outcomes after capsular fecal transplant in cirrhosis. JCI Insight 2019, 4, e133410. [Google Scholar] [CrossRef]
- Shi, S.; Zhang, Q.; Sang, Y.-X.; Ge, S.; Wang, Q.; Wang, R.; He, J. Probiotic bifidobacterium longum bb68s improves cognitive functions in healthy older adults: A randomized, double-blind, placebo-controlled trial. Nutrients 2022, 15, 51. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-C.; Jin, H.-M.; Cui, Y.; Kim, D.S.; Jung, J.M.; Park, J.-I.; Jung, E.-S.; Choi, E.-K.; Chae, S.-W. Fermented milk of lactobacillus helveticus idcc3801 improves cognitive functioning during cognitive fatigue tests in healthy older adults. J. Funct. Foods 2014, 10, 465–474. [Google Scholar] [CrossRef]
- Cheng, Y.; Liu, J.; Ling, Z. Short-chain fatty acids-producing probiotics: A novel source of psychobiotics. Crit. Rev. Food Sci. Nutr. 2021, 62, 7929–7959. [Google Scholar] [CrossRef]
- Mirzaei, R.; Bouzari, B.; Hosseini-Fard, S.R.; Mazaheri, M.; Ahmadyousefi, Y.; Abdi, M.; Jalalifar, S.; Karimitabar, Z.; Teimoori, A.; Keyvani, H.; et al. Role of microbiota-derived short-chain fatty acids in nervous system disorders. Biomed. Pharmacother. 2021, 139, 111661. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M.; Kristoffersen, A.B.; Valeur, J.; Casen, C.; Hatlebakk, J.G.; Gilja, O.H.; Hausken, T. Long-term effects of fecal microbiota transplantation (fmt) in patients with irritable bowel syndrome. Neurogastroenterol. Motil. 2022, 34, e14200. [Google Scholar] [CrossRef]
- Schwarcz, R.; Foo, A.; Sathyasaikumar, K.; Notarangelo, F. The probiotic lactobacillus reuteri preferentially synthesizes kynurenic acid from kynurenine. Int. J. Mol. Sci. 2024, 25, 3679. [Google Scholar] [CrossRef] [PubMed]
- Solvang, S.-E.H.; Nordrehaug, J.E.; Tell, G.S.; Nygård, O.; McCann, A.; Ueland, P.M.; Midttun, Ø.; Meyer, K.; Vedeler, C.A.; Aarsland, D.; et al. The kynurenine pathway and cognitive performance in community-dwelling older adults. The hordaland health study. Brain Behav. Immun. 2019, 75, 155–162. [Google Scholar] [CrossRef]
- Gao, K.; Mu, C.L.; Farzi, A.; Zhu, W.Y. Tryptophan metabolism: A link between the gut microbiota and brain. Adv. Nutr. 2020, 11, 709–723. [Google Scholar] [CrossRef]
- El Aidy, S.; Dinan, T.G.; Cryan, J.F. Gut microbiota: The conductor in the orchestra of immune–neuroendocrine communication. Clin. Ther. 2015, 37, 954–967. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.M.; Charych, E.; Lee, A.W.; Möller, T. Kynurenines in cns disease: Regulation by inflammatory cytokines. Front. Neurosci. 2014, 8, 12. [Google Scholar] [CrossRef]
- Purton, T.; Staskova, L.; Lane, M.M.; Dawson, S.L.; West, M.; Firth, J.; Clarke, G.; Cryan, J.F.; Berk, M.; O’Neil, A.; et al. Prebiotic and probiotic supplementation and the tryptophan-kynurenine pathway: A systematic review and meta analysis. Neurosci. Biobehav. Rev. 2021, 123, 1–13. [Google Scholar] [CrossRef]
- Zhan, G.; Yang, N.; Li, S.; Huang, N.; Fang, X.; Zhang, J.; Zhu, B.; Yang, L.; Yang, C.; Luo, A. Abnormal gut microbiota composition contributes to cognitive dysfunction in SAMP8 mice. Aging 2018, 10, 1257–1267. [Google Scholar] [CrossRef]
- Parker, A.; Romano, S.; Ansorge, R.; Aboelnour, A.; Le Gall, G.; Savva, G.M.; Pontifex, M.G.; Telatin, A.; Baker, D.; Jones, E.; et al. Fecal microbiota transfer between young and aged mice reverses hallmarks of the aging gut, eye, and brain. Microbiome 2022, 10, 68. [Google Scholar] [CrossRef]
- Elangovan, S.; Borody, T.J.; Holsinger, R.M.D. Fecal microbiota transplantation reduces pathology and improves cognition in a mouse model of alzheimer’s disease. Cells 2022, 12, 119. [Google Scholar] [CrossRef]
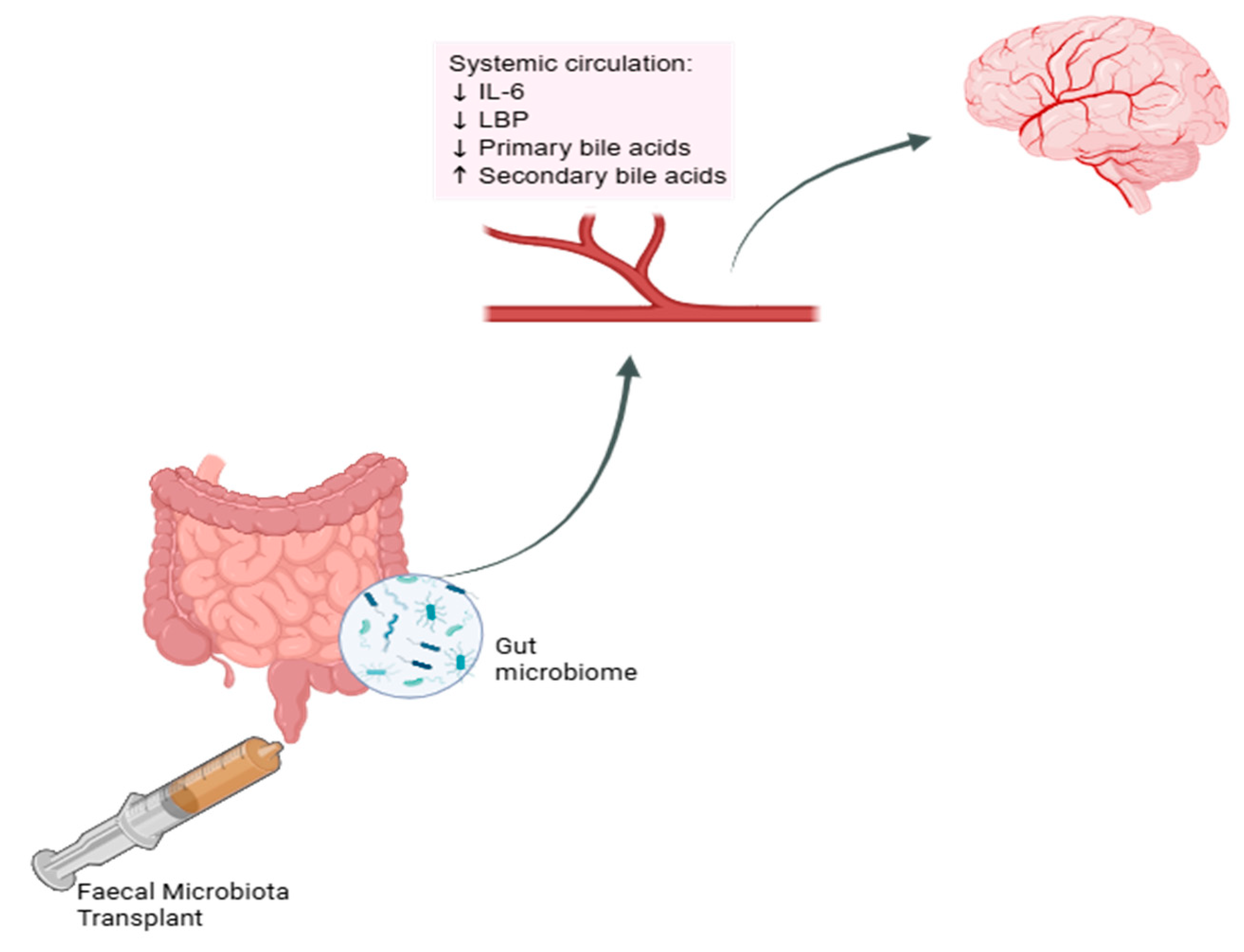
- Alaeddin, S.; Steiner-Lim, G.Z.S. Effect of Fmt on Systemic Circulation Markers; BioRender: Toronto, ON, Canada, 2025; Available online: https://BioRender.com/0a408uy (accessed on 23 April 2025).
- Baldi, S.; Mundula, T.; Nannini, G.; Amedei, A. Microbiota shaping—The effects of probiotics, prebiotics, and fecal microbiota transplant on cognitive functions: A systematic review. World J. Gastroenterol. 2021, 27, 6715–6732. [Google Scholar] [CrossRef] [PubMed]
- Freijy, T.M.; Cribb, L.; Oliver, G.; Metri, N.J.; Opie, R.S.; Jacka, F.N.; Hawrelak, J.A.; Rucklidge, J.J.; Ng, C.H.; Sarris, J. The impact of a prebiotic-rich diet and/or probiotic supplements on human cognition: Secondary outcomes from the ‘gut feelings’ randomised controlled trial. Nutr. Neurosci. 2025, 28, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Mayneris-Perxachs, J.; Castells-Nobau, A.; Arnoriaga-Rodríguez, M.; Garre-Olmo, J.; Puig, J.; Ramos, R.; Martínez-Hernández, F.; Burokas, A.; Coll, C.; Moreno-Navarrete, J.M.; et al. Caudovirales bacteriophages are associated with improved executive function and memory in flies, mice, and humans. Cell Host Microbe 2022, 30, 340–356.e8. [Google Scholar] [CrossRef]
- Nagpal, R.; Neth, B.J.; Wang, S.; Mishra, S.P.; Craft, S.; Yadav, H. Gut mycobiome and its interaction with diet, gut bacteria and alzheimer’s disease markers in subjects with mild cognitive impairment: A pilot study. EBioMedicine 2020, 59, 102950. [Google Scholar] [CrossRef]
- Fujimoto, K.; Kimura, Y.; Allegretti, J.R.; Yamamoto, M.; Zhang, Y.-Z.; Katayama, K.; Tremmel, G.; Kawaguchi, Y.; Shimohigoshi, M.; Hayashi, T.; et al. Functional restoration of bacteriomes and viromes by fecal microbiota transplantation. Gastroenterology 2021, 160, 2089–2102.e12. [Google Scholar] [CrossRef] [PubMed]
- Bagga, D.; Reichert, J.L.; Koschutnig, K.; Aigner, C.S.; Holzer, P.; Koskinen, K.; Moissl-Eichinger, C.; Schöpf, V. Probiotics drive gut microbiome triggering emotional brain signatures. Gut Microbes 2018, 9, 486–496. [Google Scholar] [CrossRef]
- Drossman, D.A.; Hasler, W.L. Rome iv—Functional gi disorders: Disorders of gut-brain interaction. Gastroenterology 2016, 150, 1257–1261. [Google Scholar] [CrossRef]
- Gibson, P.R. Use of the low-fodmap diet in inflammatory bowel disease. J. Gastroenterol. Hepatol. 2017, 32, 40–42. [Google Scholar] [CrossRef]
- Black, C.J.; Ford, A.C. Best management of irritable bowel syndrome. Frontline Gastroenterol. 2021, 12, 303–315. [Google Scholar] [CrossRef]
- Altobelli, E.; Del Negro, V.; Angeletti, P.M.; Latella, G. Low-fodmap diet improves irritable bowel syndrome symptoms: A meta-analysis. Nutrients 2017, 9, 940. [Google Scholar] [CrossRef]
- Sharma, N.; Dhiman, S.; Bodh, V.; Sharma, D.; Sharma, R.; Sharma, S.; Sharma, B. Cognitive dysfunction in ulcerative colitis patients in remission and its comparison with patients with irritable bowel syndrome and healthy controls. Indian J. Gastroenterol. 2021, 40, 169–175. [Google Scholar] [CrossRef]
- El-Salhy, M.; Hatlebakk, J.G.; Gilja, O.H.; Kristoffersen, A.B.; Hausken, T. Efficacy of faecal microbiota transplantation for patients with irritable bowel syndrome in a randomised, double-blind, placebo-controlled study. Gut 2020, 69, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, N.D.; Tamhane, A.; Walker, J.B.; Morrow, C.D.; Rodriguez, J.M. Comparative effectiveness of faecal microbiota transplant by route of administration. J. Hosp. Infect. 2017, 96, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Zhang, B.; Wu, Y.; Wang, Q.; Wang, J.; Shen, F. The value of fecal microbiota transplantation in the treatment of ulcerative colitis patients: A systematic review and meta-analysis. Gastroenterol. Res. Pract. 2018, 2018, 5480961. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Singh, S.K.; Corrie, L.; Kaur, I.P.; Chandwani, L. Delivery routes for faecal microbiota transplants: Available, anticipated and aspired. Pharmacol. Res. 2020, 159, 104954. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alaeddin, S.; Ko, Y.; Steiner-Lim, G.Z.; Jensen, S.O.; Roberts, T.L.; Ho, V. The Effect of Faecal Microbiota Transplantation on Cognitive Function in Cognitively Healthy Adults with Irritable Bowel Syndrome: Protocol for a Randomised, Placebo-Controlled, Double-Blinded Pilot Study. Methods Protoc. 2025, 8, 83. https://doi.org/10.3390/mps8040083
Alaeddin S, Ko Y, Steiner-Lim GZ, Jensen SO, Roberts TL, Ho V. The Effect of Faecal Microbiota Transplantation on Cognitive Function in Cognitively Healthy Adults with Irritable Bowel Syndrome: Protocol for a Randomised, Placebo-Controlled, Double-Blinded Pilot Study. Methods and Protocols. 2025; 8(4):83. https://doi.org/10.3390/mps8040083
Chicago/Turabian StyleAlaeddin, Sara, Yanna Ko, Genevieve Z. Steiner-Lim, Slade O. Jensen, Tara L. Roberts, and Vincent Ho. 2025. "The Effect of Faecal Microbiota Transplantation on Cognitive Function in Cognitively Healthy Adults with Irritable Bowel Syndrome: Protocol for a Randomised, Placebo-Controlled, Double-Blinded Pilot Study" Methods and Protocols 8, no. 4: 83. https://doi.org/10.3390/mps8040083
APA StyleAlaeddin, S., Ko, Y., Steiner-Lim, G. Z., Jensen, S. O., Roberts, T. L., & Ho, V. (2025). The Effect of Faecal Microbiota Transplantation on Cognitive Function in Cognitively Healthy Adults with Irritable Bowel Syndrome: Protocol for a Randomised, Placebo-Controlled, Double-Blinded Pilot Study. Methods and Protocols, 8(4), 83. https://doi.org/10.3390/mps8040083