

Using the C14:1/Medium-Chain Acylcarnitine Ratio Instead of C14:1 to Reduce False-Positive Results for Very-Long-Chain Acyl-CoA Dehydrogenase Deficiency in Newborn Screening in Japan

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Subjects
2.2. NBS Test for VLCAD Deficiency
2.3. Confirmatory Tests for VLCAD Deficiency
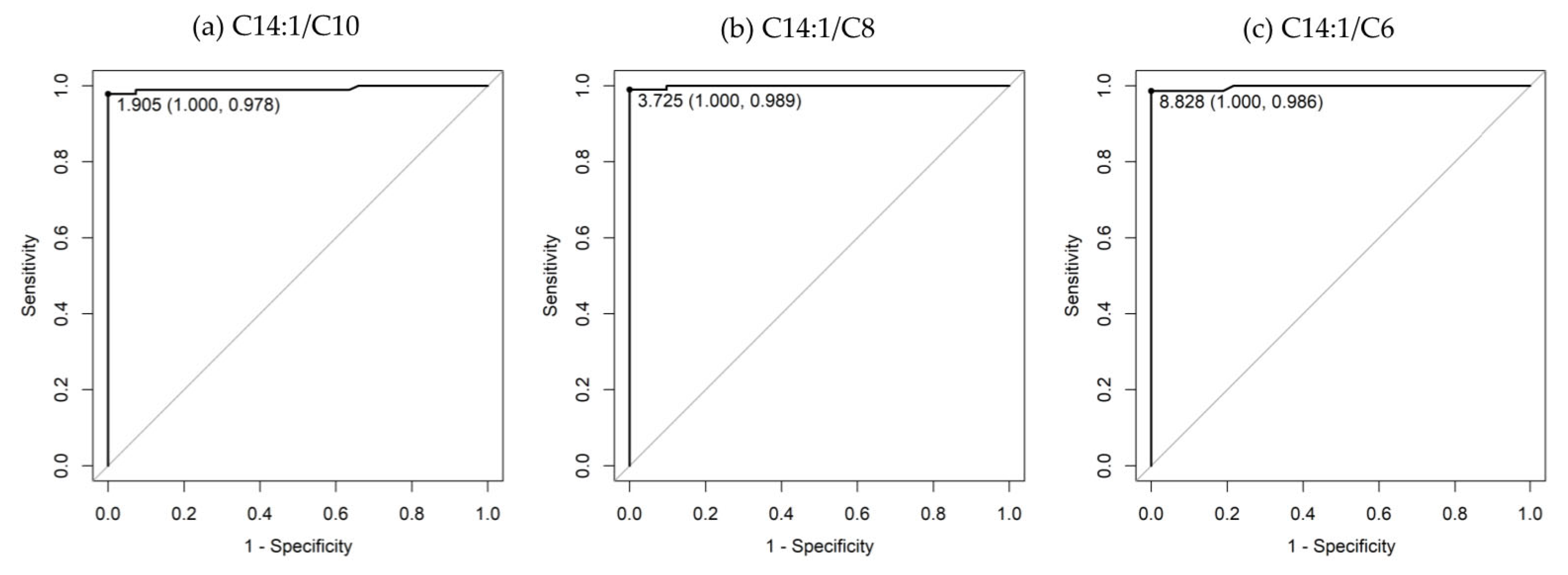
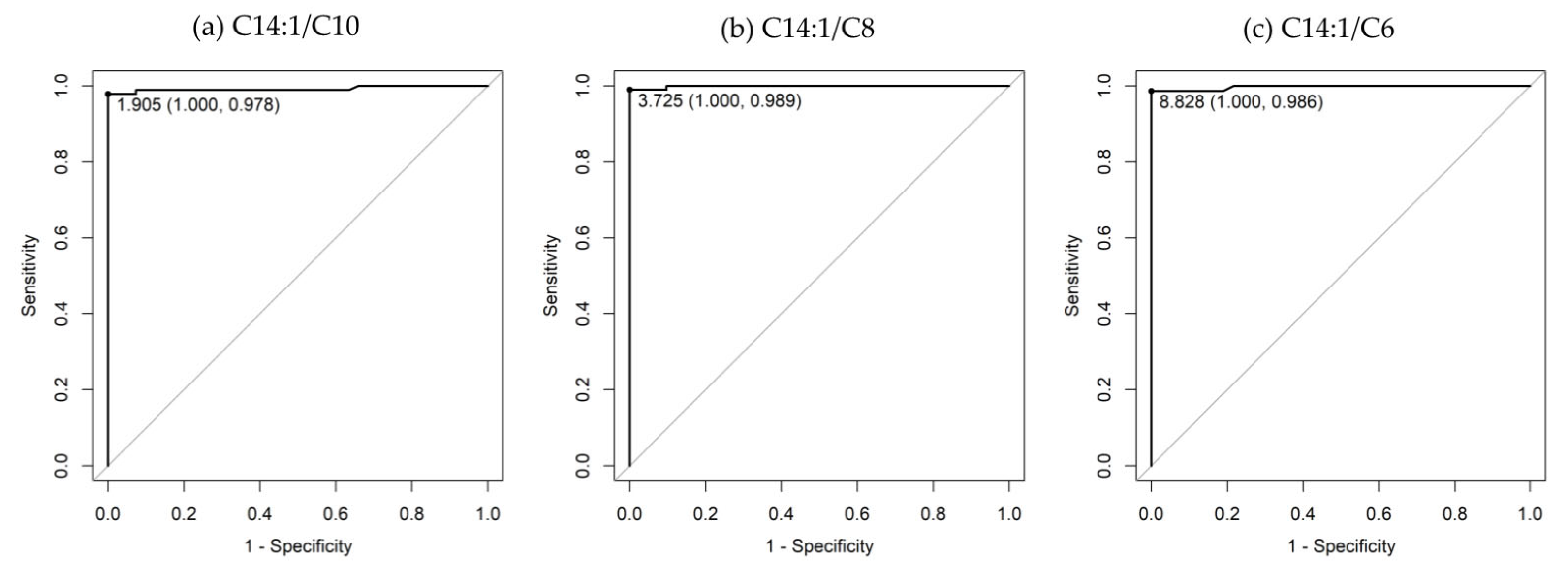
2.4. Receiver Operating Characteristic Analysis
3. Results
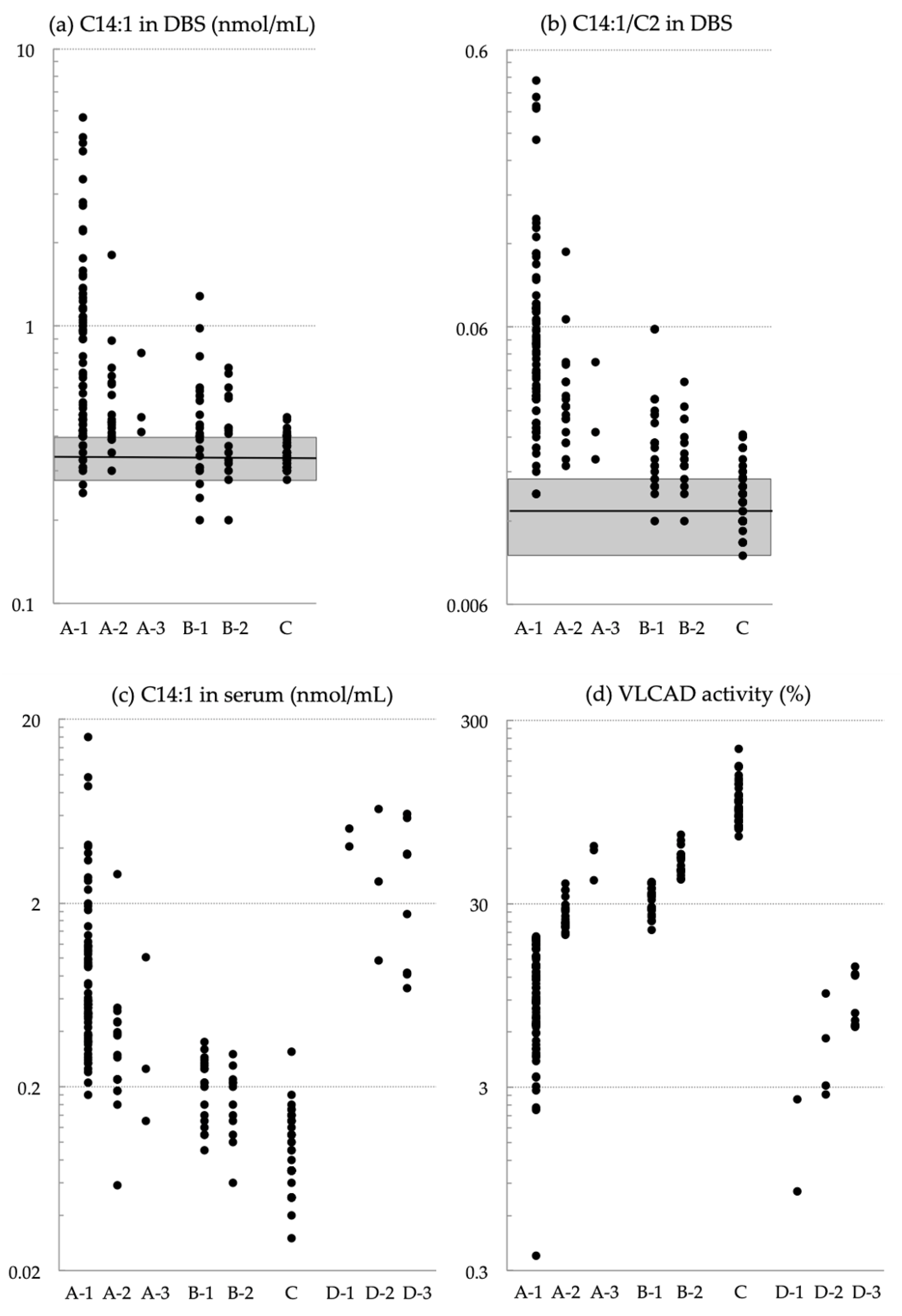
3.1. Diagnosis of NBS Positivity and Levels of Currently Used Markers
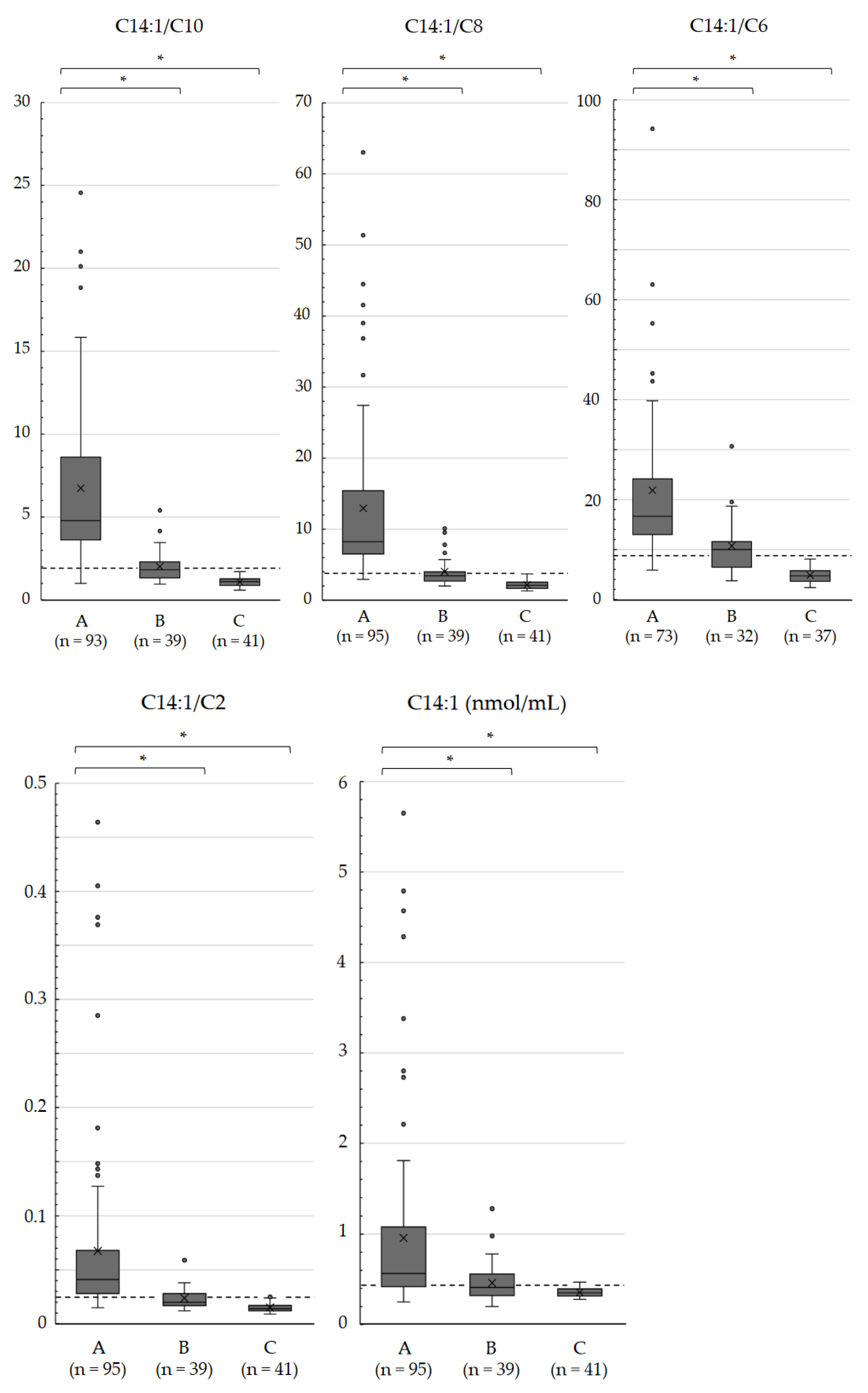
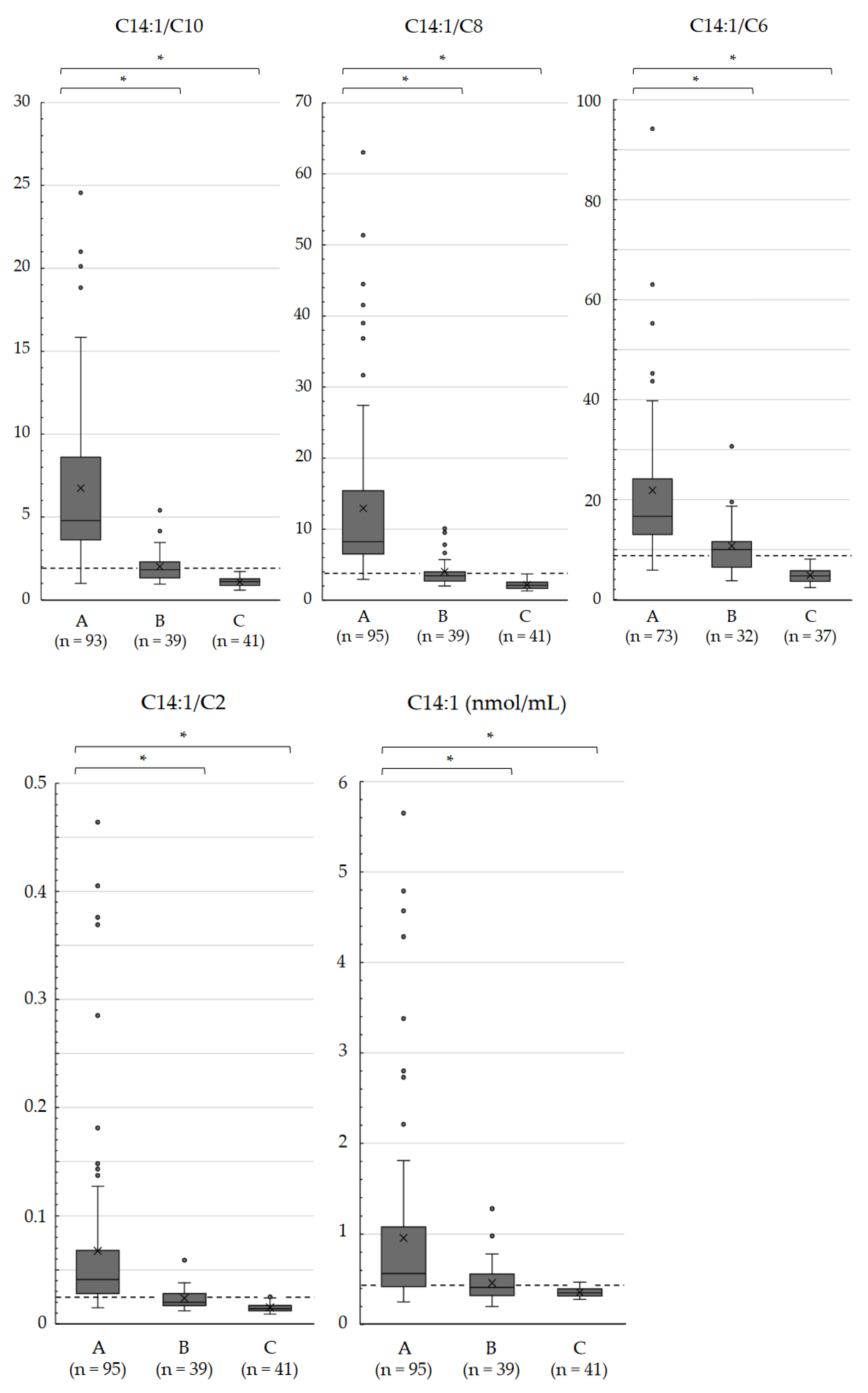
3.2. Comparing the C14:1 Level and C14:1/C2 Ratio to Various Acylcarnitines in DBSs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bertrand, C.; Largillière, C.; Zabot, M.T.; Mathieu, M.; Vianey-Saban, C. Very-long-chain acyl-CoA dehydrogenase deficiency: Identification of new inborn error of mitochondrial fatty acid oxidation in fibroblasts. Biochim. Biophys. Acta 1993, 1180, 327–329. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, T.; Uchida, Y.; Kelley, R.I.; Marble, M.; Hofman, K.; Tonsgard, J.H.; Rhead, W.J.; Hashimoto, T. A novel disease with deficiency of mitochondrial very-long-chain acyl-CoA dehydrogenase. Biochem. Biophys. Res. Commun. 1993, 191, 1369–1372. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Indo, Y.; Coates, P.M.; Hashimoto, T.; Tanaka, K. Identification of very-long-chain acyl-CoA dehydrogenase deficiency in three patients previously diagnosed with long-chain acyl-CoA dehydrogenase deficiency. Pediatr. Res. 1993, 34, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Andresen, B.S.; Olpin, S.; Poorthuis, B.J.; Scholte, H.R.; Vianey-Saban, C.; Wanders, R.; Ijlst, L.; Morris, A.; Pourfarzam, M.; Bartlett, K.; et al. Clear correlation of genotype with disease phenotype in very-long-chain acyl-CoA dehydrogenase deficiency. Am. J. Hum. Genet. 1999, 64, 479–494. [Google Scholar] [CrossRef]
- McHugh, D.; Cameron, C.A.; Abdenur, J.E.; Abdulrahman, M.; Adair, O.; Al Nuaimi, S.A. Clinical validation of cutoff target ranges in newborn screening of metabolic disorders by tandem mass spectrometry: A worldwide collaborative project. Genet. Med. 2011, 13, 230–254. [Google Scholar] [CrossRef] [PubMed]
- Knottnerus, S.J.G.; Bleeker, J.C.; Wüst, R.C.I.; Ferdinandusse, S.; IJlst, L.; Wijburg, F.A.; Wanders, R.J.A.; Visser, G.; Houtkooper, R.H. Disorders of mitochondrial long-chain fatty acid oxidation and the carnitine shuttle. Rev. Endocr. Metab. Disord. 2018, 19, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Liebig, M.; Schymik, I.; Mueller, M.; Wendel, U.; Mayatepek, E.; Ruiter, J.; Strauss, A.W.; Wanders, R.J.; Spiekerkoetter, U. Neonatal screening for very long-chain acyl-coA dehydrogenase deficiency: Enzymatic and molecular evaluation of neonates with elevated C14:1-carnitine levels. Pediatrics 2006, 118, 1065–1069. [Google Scholar] [CrossRef]
- Spiekerkoetter, U.; Haussmann, U.; Mueller, M.; Ter Veld, F.; Stehn, M.; Santer, R.; Lukacs, Z. Tandem mass spectrometry screening for very long-chain acyl-CoA dehydrogenase deficiency: The value of second-tier enzyme testing. J. Pediatr. 2010, 157, 668–673. [Google Scholar] [CrossRef]
- Hesse, J.; Braun, C.; Behringer, S.; Matysiak, U.; Spiekerkoetter, U.; Tucci, S. The diagnostic challenge in very-long chain acyl-CoA dehydrogenase deficiency (VLCADD). J. Inherit. Metab. Dis. 2018, 41, 1169–1178. [Google Scholar] [CrossRef]
- Diekman, E.; de Sain-van der Velden, M.; Waterham, H.; Kluijtmans, L.; Schielen, P.; van Veen, E.B.; Ferdinandusse, S.; Wijburg, F.; Visser, G. The newborn screening paradox: Sensitivity vs. overdiagnosis in VLCAD deficiency. JIMD Rep. 2015, 27, 101–106. [Google Scholar] [CrossRef]
- Merritt, J.L., 2nd; Vedal, S.; Abdenur, J.E.; Au, S.M.; Barshop, B.A.; Feuchtbaum, L.; Harding, C.O.; Hermerath, C.; Lorey, F.; Sesser, D.E.; et al. Infants suspected to have very-long chain acyl-CoA dehydrogenase deficiency from newborn screening. Mol. Genet. Metab. 2014, 111, 484–492. [Google Scholar] [CrossRef]
- Merinero, B.; Alcaide, P.; Martín-Hernández, E.; Morais, A.; García-Silva, M.T.; Quijada-Fraile, P.; Pedrón-Giner, C.; Dulin, E.; Yahyaoui, R.; Egea, J.M.; et al. Four years’ experience in the diagnosis of very long-chain acyl-CoA dehydrogenase deficiency in infants detected in three Spanish newborn screening centers. JIMD Rep. 2018, 39, 63–74. [Google Scholar] [CrossRef]
- Wang, B.; Zhang, Q.; Gao, A.; Wang, Q.; Ma, J.; Li, H.; Wang, T. New ratios for performance improvement for identifying acyl-CoA dehydrogenase deficiencies in expanded newborn screening: A retrospective study. Front. Genet. 2019, 10, 811. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Osawa, Y.; Kobayashi, H.; Hasegawa, Y.; Fukuda, S.; Yamaguchi, S.; Taketani, T. Serum C14:1/ C12:1 ratio is a useful marker for differentiating affected patients with very long-chain acyl-CoA dehydrogenase deficiency from heterozygous carriers. Mol. Genet. Metab. Rep. 2019, 21, 100535. [Google Scholar] [CrossRef]
- Remec, Z.I.; Groselj, U.; Drole Torkar, A.; Zerjav Tansek, M.; Cuk, V.; Perko, D.; Ulaga, B.; Lipovec, N.; Debeljak, M.; Kovac, J.; et al. Very long-chain acyl-CoA dehydrogenase deficiency: High incidence of detected patients with expanded newborn screening program. Front. Genet. 2021, 12, 648493. [Google Scholar] [CrossRef]
- Upadia, J.; Noh, G.; Lefante, J.J.; Andersson, H.C. Biochemical and molecular characteristics among infants with abnormal newborn screen for very-long-chain acyl-CoA dehydrogenase deficiency: A single center experience. Mol. Genet. Metab. Rep. 2023, 37, 101002. [Google Scholar] [CrossRef] [PubMed]
- Yamada, K.; Taketani, T. Management and diagnosis of mitochondrial fatty acid oxidation disorders: Focus on very-long-chain acyl-CoA dehydrogenase deficiency. J. Hum. Genet. 2019, 64, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Osawa, Y.; Kobayashi, H.; Tajima, G.; Hara, K.; Yamada, K.; Fukuda, S.; Hasegawa, Y.; Aisaki, J.; Yuasa, M.; Hata, I.; et al. The frequencies of very long-chain acyl-CoA dehydrogenase deficiency genetic variants in Japan have changed since the implementation of expanded newborn screening. Mol. Genet. Metab. 2022, 136, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Bo, R.; Awano, H.; Nishida, K.; Fujioka, K.; Nishiyama, A.; Miyake, O.; Iijima, K. False positive cases of elevated tetradecenoyl carnitine in newborn mass screening showed significant loss of body weight. Mol. Genet. Metab. Rep. 2020, 24, 100634. [Google Scholar] [CrossRef]
- Shigematsu, Y.; Hata, I.; Kikawa, Y.; Mayumi, M.; Tanaka, Y.; Sudo, M.; Kado, N. Modifications in electrospray tandem mass spectrometry for a neonatal-screening pilot study in Japan. J. Chromatogr. B Biomed. Sci. Appl. 1999, 731, 97–103. [Google Scholar] [CrossRef]
- Hanai, J. Current status and future tasks of quality assurance in newborn screening. Jpn. J. Neonatal Screen. 2023, 33, 31–40. [Google Scholar]
- Tajima, G.; Sakura, N.; Shirao, K.; Okada, S.; Tsumura, M.; Nishimura, Y.; Ono, H.; Hasegawa, Y.; Hata, I.; Naito, E.; et al. Development of a new enzymatic diagnosis method for very-long-chain acyl-CoA dehydrogenase deficiency by detecting 2-hexadecenoyl-CoA production and its application in tandem mass spectrometry-based selective screening and newborn screening in Japan. Pediatr. Res. 2008, 64, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, Y.; Hasegawa, Y.; Murayama, K.; Ogawa, M.; Hasegawa, T.; Kawai, M.; Sakata, N.; Yoshida, K.; Yarita, H.; Imai, K.; et al. A new diagnostic test for VLCAD deficiency using immunohistochemistry. Neurology 2004, 62, 2209–2213. [Google Scholar] [CrossRef] [PubMed]
- Nakama, M.; Sasai, H.; Kubota, M.; Hasegawa, Y.; Fujiki, R.; Okuyama, T.; Ohara, O.; Fukao, T. Novel HADHB mutations in a patient with mitochondrial trifunctional protein deficiency. Hum. Genome Var. 2020, 7, 10. [Google Scholar] [CrossRef]
- Wanders, R.J.A.; Vreken, P.; den Boer, M.E.J.; Wijburg, F.A.; van Gennip, A.H.; IJlst, L. Disorders of fatty acyl-CoA β-oxidation. J. Inherit. Metab. Dis. 1999, 22, 442–487. [Google Scholar] [CrossRef] [PubMed]
- Boneh, A.; Andresen, B.S.; Gregersen, N.; Ibrahim, M.; Tzanakos, N.; Peters, H.; Yaplito-Lee, J.; Pitt, J.J. VLCAD deficiency: Pitfalls in newborn screening and confirmation of diagnosis by mutation analysis. Mol. Genet. Metab. 2006, 88, 166–170. [Google Scholar] [CrossRef]
- Tong, F.; Chen, T.; Jiang, P.; Yang, R.; Zhao, Z.; Shu, Q. Analysis of ACADVL gene variations among nine neonates with very long-chain acyl-CoA dehydrogenase deficiency. Zhonghua Yi Xue Chuan Xue Za Zhi 2019, 36, 310–313. (In Chinese) [Google Scholar]
- Baker, J.J.; Burton, B.K. Diagnosis and clinical management of long-chain fatty-acid oxidation disorders: A review. touchREVIEWS Endocrinol. 2021, 17, 108–111. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Groups and Descriptions of Infants with NBS-Positive Results for VLCAD Deficiency (Groups A–C) and Symptomatic Patients (Group D) | n | Case ID *1 | VLCAD Activity *2 | |
|---|---|---|---|---|
| Group A-1 | Biallelic ACADVL variants detected, VLCAD activity lower than 20% | 73 | N-01 to N-73 | 0.36–19.88% (10.28 ± 5.13) |
| Group A-2 | Biallelic ACADVL variants detected, VLCAD activity between 20% and 40% | 19 | N-74 to N-92 | 20.32–38.70% (27.01 ± 5.35) |
| Group A-3 | Biallelic ACADVL variants detected, VLCAD activity higher than 40% | 3 | N-93 to N-95 | 40.55–58.73%, 62.00% |
| Group B-1 | Heterozygous ACADVL variants detected, VLCAD activity between 20% and 40% | 23 | N-96 to N-118 | 21.62–39.35% (31.80 ± 5.56) |
| Group B-2 | Heterozygous ACADVL variants detected, VLCAD activity higher than 40% | 16 | N-119 to N-134 | 40.66–71.32% (51.74 ± 9.17) |
| Group C | VLCAD activity higher than 70% without confirmation with ACADVL sequencing | 41 | N-135 to N-175 | 70.27–208.67% (107.96 ± 29.43) |
| Group D-1 | Severe phenotype | 2 | S-01, S-02 | 0.81–2.59% |
| Group D-2 | Hypoglycemic phenotype | 4 | S-03 to S-06 | 2.75–9.75% |
| Group D-3 | Myopathic phenotype | 8 | S-07 to S-14 | 6.41–13.72% |
| Characteristic | Acylcarnitine and Free Carnitine Levels | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C18:1 | C18 | C16 | C16-OH | C14:1 | C14 | C12 | C10 | C8 | C6 | C4 | C3 | C2 | C0 | |
| Optimal cutoff (nmol/mL) | 1.358 | 0.853 | 2.627 | 0.031 | 0.417 | 0.421 | 0.403 | 0.215 | 0.110 | 0.047 | 0.175 | 1.230 | 21.859 | 17.780 |
| Sensitivity | 0.435 | 0.624 | 0.543 | 0.840 | 0.768 | 0.419 | 0.329 | 0.892 | 0.853 | 0.808 | 0.686 | 0.613 | 0.863 | 0.696 |
| Specificity | 0.795 | 0.634 | 0.902 | 0.732 | 0.927 | 0.951 | 0.927 | 0.976 | 0.976 | 0.973 | 0.919 | 0.512 | 0.756 | 0.732 |
| Area under the ROC curve | 0.594 | 0.626 | 0.744 | 0.807 | 0.881 | 0.681 | 0.432 | 0.938 | 0.954 | 0.928 | 0.840 | 0.518 | 0.877 | 0.749 |
| Characteristic | Acylcarnitine Ratios | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C14:1/ C18:1 | C14:1/ C18 | C14:1/ C16 | C14:1/ C16-OH | C14:1/ C14 | C14:1/ C12 | C14:1/ C10 | C14:1/ C8 | C14:1/ C6 | C14:1/ C4 | C14:1/ C3 | C14:1/ C2 | C14:1/ C0 | |
| Optimal cutoff | 0.319 | 0.600 | 0.153 | 19.444 | 1.398 | 1.264 | 1.905 | 3.725 | 8.828 | 1.959 | 0.394 | 0.023 | 0.025 |
| Sensitivity | 0.788 | 0.634 | 0.915 | 0.926 | 0.709 | 0.941 | 0.978 | 0.989 | 0.986 | 0.914 | 0.559 | 0.895 | 0.696 |
| Specificity | 0.949 | 0.854 | 0.976 | 1.000 | 0.805 | 0.902 | 1.000 | 1.000 | 1.000 | 0.892 | 0.951 | 0.951 | 0.610 |
| Area under the ROC curve | 0.919 | 0.797 | 0.972 | 0.991 | 0.814 | 0.972 | 0.992 | 0.999 | 0.997 | 0.942 | 0.768 | 0.978 | 0.694 |
| Index: C14:1 ≥ 0.417 nmol/mL | ||||
|---|---|---|---|---|
| Group A | Data Available 95 | Positive 73 | Negative 22 | Sensitivity 0.768 |
| Group C | Data Available 41 | Positive 3 | Negative 38 | Specificity 0.927 |
| Group A + C | Positive predictive value 0.961 | Negative predictive value 0.633 | ||
| Group B-1/B-2 | Data Available 23/16 | Positive 10/8 | Negative 13/8 | Positive rate 0.435/0.500 |
| Index: C14:1/C2 ≥ 0.023 | ||||
| Group A | Data Available 95 | Positive 85 | Negative 10 | Sensitivity 0.895 |
| Group C | Data Available 41 | Positive 2 | Negative 39 | Specificity 0.951 |
| Group A + C | Positive predictive value 0.977 | Negative predictive value 0.796 | ||
| Group B-1/B-2 | Data Available 23/16 | Positive 11/6 | Negative 12/10 | Positive rate 0.478/0.375 |
| Index: C14:1/C10 ≥ 1.905 | ||||
| Group A | Data Available 93 | Positive 91 | Negative 2 | Sensitivity 0.978 |
| Group C | Data Available 41 | Positive 0 | Negative 41 | Specificity 1 |
| Group A + C | Positive predictive value 1 | Negative predictive value 0.953 | ||
| Group B-1/B-2 | Data Available 23/16 | Positive 13/3 | Negative 10/13 | Positive rate 0.565/0.188 |
| Index: C14:1/C8 ≥ 3.725 | ||||
| Group A | Data Available 95 | Positive 94 | Negative 1 | Sensitivity 0.989 |
| Group C | Data Available 41 | Positive 0 | Negative 41 | Specificity 1 |
| Group A + C | Positive predictive value 1 | Negative predictive value 0.976 | ||
| Group B-1/B-2 | Data Available 23/16 | Positive 11/4 | Negative 12/12 | Positive rate 0.478/0.250 |
| Index: C14:1/C6 ≥ 8.828 | ||||
| Group A | Data Available 73 | Positive 72 | Negative 1 | Sensitivity 0.986 |
| Group C | Data Available 37 | Positive 0 | Negative 37 | Specificity 1 |
| Group A + C | Positive predictive value 1 | Negative predictive value 0.974 | ||
| Group B-1/B-2 | Data Available 21/11 | Positive 12/5 | Negative 9/6 | Positive rate 0.571/0.455 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tajima, G.; Aisaki, J.; Hara, K.; Tsumura, M.; Kagawa, R.; Sakura, F.; Sasai, H.; Yuasa, M.; Shigematsu, Y.; Okada, S. Using the C14:1/Medium-Chain Acylcarnitine Ratio Instead of C14:1 to Reduce False-Positive Results for Very-Long-Chain Acyl-CoA Dehydrogenase Deficiency in Newborn Screening in Japan. Int. J. Neonatal Screen. 2024, 10, 15. https://doi.org/10.3390/ijns10010015
Tajima G, Aisaki J, Hara K, Tsumura M, Kagawa R, Sakura F, Sasai H, Yuasa M, Shigematsu Y, Okada S. Using the C14:1/Medium-Chain Acylcarnitine Ratio Instead of C14:1 to Reduce False-Positive Results for Very-Long-Chain Acyl-CoA Dehydrogenase Deficiency in Newborn Screening in Japan. International Journal of Neonatal Screening. 2024; 10(1):15. https://doi.org/10.3390/ijns10010015
Chicago/Turabian StyleTajima, Go, Junko Aisaki, Keiichi Hara, Miyuki Tsumura, Reiko Kagawa, Fumiaki Sakura, Hideo Sasai, Miori Yuasa, Yosuke Shigematsu, and Satoshi Okada. 2024. "Using the C14:1/Medium-Chain Acylcarnitine Ratio Instead of C14:1 to Reduce False-Positive Results for Very-Long-Chain Acyl-CoA Dehydrogenase Deficiency in Newborn Screening in Japan" International Journal of Neonatal Screening 10, no. 1: 15. https://doi.org/10.3390/ijns10010015
APA StyleTajima, G., Aisaki, J., Hara, K., Tsumura, M., Kagawa, R., Sakura, F., Sasai, H., Yuasa, M., Shigematsu, Y., & Okada, S. (2024). Using the C14:1/Medium-Chain Acylcarnitine Ratio Instead of C14:1 to Reduce False-Positive Results for Very-Long-Chain Acyl-CoA Dehydrogenase Deficiency in Newborn Screening in Japan. International Journal of Neonatal Screening, 10(1), 15. https://doi.org/10.3390/ijns10010015