Highlights
- Although social media has positive effects in that it can highlight seldom-discussed issues, the doctor must ultimately validate individual concerns and educate patients to better understand their situation.
- Although the relationship between silicone implants and various systemic disorders is becoming clearer, establishment of global registers to collect data could assist in understanding this relationship better.
Highlights
- Although social media has positive effects in that it can highlight seldom-discussed issues, the doctor must ultimately validate individual concerns and educate patients to better understand their situation.
- Although the relationship between silicone implants and various systemic disorders is becoming clearer, establishment of global registers to collect data could assist in understanding this relationship better.
Abstract
Introduction. The number of implant-related complaints is constantly rising, a phenomenon probably accentuated by the extensive use of social media by patients. Material and method. A group of signs and symptoms considered to be caused by mammary implants is known as “Breast Implant Illness”. This paper analyzes the increased number of posts by patients on social media in which they describe their symptoms, their disappointment with the decision of using breast implants, and the beneficial effects of explantation. The case of a patient with breast implants who visited our clinic is reported here. The patient complained of two palpable masses, located in the left axilla and in the superolateral quadrant of the left breast. The pathophysiological mechanism by which lymphadenopathy occurred after a long period of time remains uncertain. Discussion. A review of the literature was conducted to identify the underlying causes of implant-related complaints, allowing evaluation of the presence of local complications, cancer with large anaplastic cells, and autoimmune diseases. The possibility of a somatization effect has also been considered. Conclusions. Plastic surgeons must remain the best source of information, taking on the role of educating the patient in order to better understand this condition.
Introduction
The frequency of surgical procedures requiring implants has been steadily increasing over the past years, currently estimated at about 10 million women who have undergone breast implant surgery. Of these, about 75% involved cosmetic enhancements and 25% involved reconstruction after mastectomy [1,2].
Breast implantation has raised many controversies since its initial use. Numerous side effects have been attributed to implants, which can be classified into 3 major groups: systemic illnesses that include connective tissue diseases or neoplasia, non-specific symptoms such as fatigue, and pain and local complications of the implant insertion such as capsular contracture, implant rupture, or infection [3].
Breast Implant Illness
Breast Implant Illness is a term used to describe a group of symptoms and signs presumably caused by implants [4]. In 1998, Tugwell conducted a comprehensive study examining all the symptoms described by women with mammary implants, and he noted that these symptoms do not significantly differ from women without implants [5].
Although there is no known pathophysiological explanation for the many patient complaints and there is no specific diagnostic test, the number of women who request explantation surgery is increasing. This phenomenon is probably augmented by the large number of women who express opinions regarding their breast implant experiences on social networks. It is, however, difficult to quantify these symptoms due to their highly subjective nature. In most cases, physical examination performed by the physician does not reveal any clear basis for the complaints.
More than 50,000 women report a range of symptoms referred to as "breast implant illness" on Facebook pages like Breast Implant Illness and Healing by Nicole. This group has more than 90,000 members (being female represents one of the conditions in order to be accepted), and their number is growing weekly by about 1,000 members. About 315 new posts related to breast disorders are posted daily. Other examples of such pages are Breast Implant Illness Healing Warriors (more than 5,000 members) and Breast Implant Illness Support Group (more than 3,000 followers). When more than 450 posts and related comments were reviewed, 186 (41.33%) described common symptoms like fatigue, chronic pain, rash, xeroderma, anxiety, irregular heart rate, neurological abnormalities (brain fog, dizziness, insomnia), weight gain, rhinorrhea, hair loss, endocrine dysfunction, and so on.
Questions about explantation surgery, the doctors who perform such interventions, the explantation experience itself, and the post-surgical response are frequent topics within these groups. Topics about the beneficial effects of the intervention are also evident, e.g., the objective diminution of the symptoms, the improvement of vision, the disappearance of skin problems, resting sleep, better mental concentration, etc. Each woman’s case evokes great empathy, and support is offered to women who for any reason want to remove the implants or learn more about the procedure. Posts and comments do not express regret after explantation, although some women express frustration about their new physical appearance. Patients apparently focus on the surgical removal of the implants instead of attempting to figure out the reason for their discomfort through a medical check-up. Their anxiety and worry may lead them to opt for unreasonable treatment decisions [7].
In 2001, Dush suggested that many of the psychological symptoms of women with silicone breast implants might be attributed to mass somatization or stress [3]. Researchers have also noted that these symptoms may overlap with common symptoms of conditions such as fibromyalgia, chronic fatigue syndrome, and irritable bowel syndrome. Given such symptoms, Barsky and Borus have proposed guidelines for the medical management of the potential somatization phenomena [6], thus providing an extended view for possible treatment. However, controlled studies to test these assumptions are required.
Breast implant-associated anaplastic large cell lymphoma
No medical device is without risk. Anaplastic large cell lymphoma (ALCL) is a rare type of non-Hodgkin's lymphoma (NHL) accounting for about 1% of all NHL cancers. In 2011, the FDA announced that this rare form of cancer had an increased incidence among women with breast implants compared to the general population. Tumor cells have been identified from the fluid around the implant and the scarring capsule [8].
Studies have shown that this condition is associated with textured implants, and thus far no documented cases of cancer have been associated with implants having a smooth surface. A link between bacterial biofilm and T cell hyperplasia has been suggested, which can lead to the disease in question [9]. Symptoms may include pain, inflammation, breast enlargement due to late seroma or a tumor mass, and capsular contraction [10].
The disease typically develops at least 10 years after the implant placement. The estimated incidence ranges between 0.1 and 0.3 per 100,000 women with mammary implants. However, in order to elucidate predisposing and genetic risk factors for these diseases [11], greater worldwide evidence is needed. In the meantime, we consider it important for the cosmetic surgeon to discuss the ALCL risk associated with the implant before performing the breast augmentation surgery. Patients also need to know that this condition is curable using specific treatment protocols if detected at the early stages.
Autoimmune disease
Another question often raised is whether silicone implants can cause a form of cancer of the immune system and/or whether they might cause other immune disorders. Several case reports describing the development of systemic rheumatic manifestations have occurred since 1964. Silicone implants cause a non-specific body reaction, with the appearance of antibodies against the implant, especially in the capsular tissue. Studies suggest an increased incidence of diseases such as Sjögren's syndromes, scleroderma, and rheumatoid arthritis, but the limited number of cases and the lack of global evidence currently limit drawing strong conclusions [12]. Furthermore, patients with multiple allergies are prone to aggravation or development of other autoimmune conditions after breast implant surgery. However, in order to determine a causal relationship between silicone implants and autoimmune diseases, longitudinal studies are needed [12].
Local Complications
Some local symptoms of implants may be attributable to indolent infection after implantation, the infection being the main cause of readmission after mammary augmentation [13]. Other symptoms might also appear due to the capsular contracture in which bacterial colonization plays an important role, because bacterial stimuli accelerate the inflammation and fibrosis [14]. Capsular contracture is a complication that occurs in about 8% of the cases of cosmetic augmentation and in 16% of the cases of reconstruction [15]. This condition may require removal of the capsule tissue and of the implant.
Breast implants can eventually break, with the first signs being breast pain and changes in breast shape. This outcome can be assessed through Magnetic Resonance Imaging. In addition, silicone exposure may cause a granulomatosis reaction which requires a biopsy to exclude malignancy [16]. Many studies report the occurrence of lymphadenopathy through mechanisms such as silicone implant rupture and silicone leakage through the prosthetic micropores, documented through histopathological examinations. No cases of lymphadenopathy with no silicone involvement have been described [17].
Case Report
We examined a case of lymphadenopathy with no silicone leakage, the case of a 44-year old woman admitted to our Plastic Surgery Department. The patient complained about two palpable masses, found in the left axilla and in the superolateral quadrant of the left breast. These masses had evolved slowly over the course of a year. The patient underwent breast augmentation surgery with submuscular silicone implants 13 years ago and a laparoscopic excision surgery of ovarian cysts 4 years ago.
Physical examination revealed an approximately 3 cm solid tumor, mobile, located in the left axilla and another similar mass with a 1 cm diameter located in the superolateral quadrant of the left breast. The mass from the axilla was painful on palpation and the patient also complained of a slight pain that irradiated to the external chest wall. Blood tests revealed that the tumor markers CA- 125, CA15-3, CA19-9, and CEA were within normal limits. A mammography was performed and described the regular contour of the implant in the left breast with no other changes of the breast parenchyma (Figure 1).
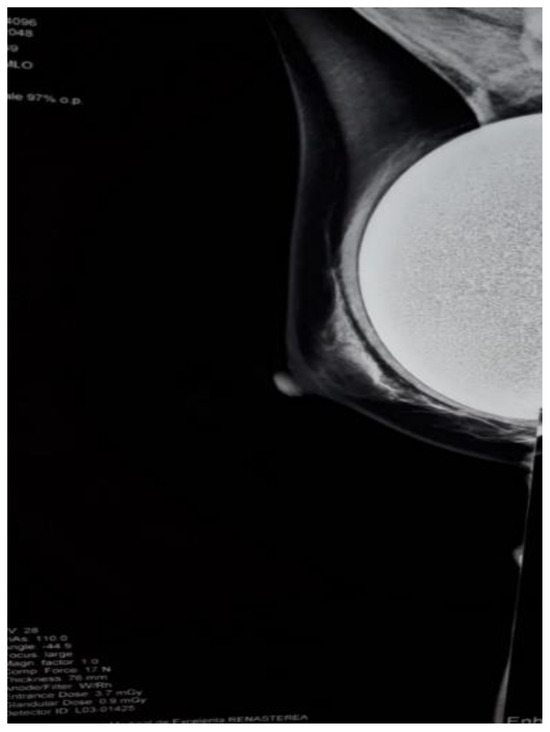
Figure 1.
Mammography showing the regular contour of the left breast implant and no radiodense mass in the left axilla.
In order to establish the structure and mobility of the tumor, a mammary ultrasound was performed describing a 1.35/0.58 cm lymph node image located at the periphery of the external breast pocket, near the implant, with increased vascularization, smooth contours, and mobile from adjacent planes (Figure 2).
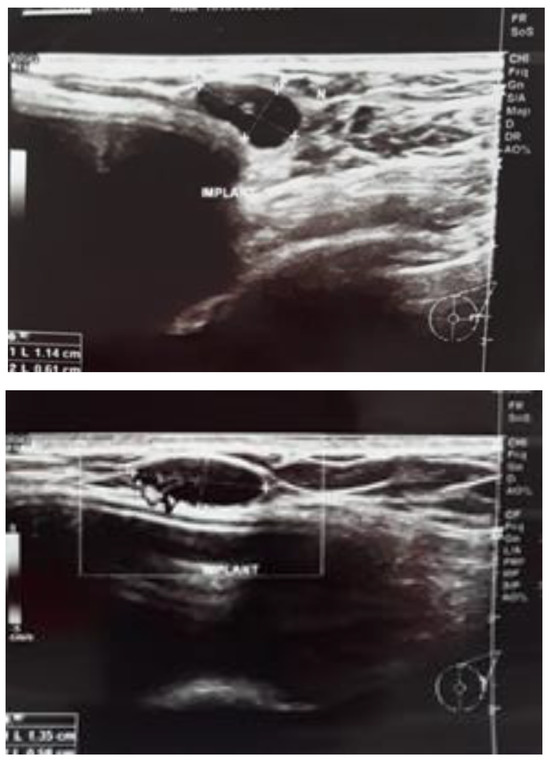
Figure 2.
(a,b). Mammary ultrasound showing a lymph node image located at the periphery of the external breast pocket.
Surgical treatment was established and excision of the tumor masses of the axilla and the left breast was performed. The postoperative evolution was favorable, the symptomatology disappeared, and the patient was discharged after 4 days. The histopathological examination revealed two lymph nodes with paracortical lymphoid hyperplasia and fatty degeneration. No presence of silicone compounds was noted. The immunohistochemical tests performed were positive for different non-tumoral lymphocyte populations.
In this case, axillary and local lymphadenopathy did not occur due to silicone leakage, the implant being integral as it could be seen in the mammography and also intraoperatively. Other etiologies were considered, thereby excluding infection, neoplasia, and autoimmune diseases. The pathophysiological mechanism by which lymphadenopathy occurred after a long period of time and without having a carcinogenic nature remains uncertain, which might result in the description of a novel condition that might reveal another mechanism of lymphocyte activation due to implant proximity.
Discussions
A preoperative psychological examination is important and can draw attention to factors that can negatively affect the patient’s evolution. Studies have shown that depression and anxiety can influence the immune system and predispose to infections. Thus, patients require prolonged hospitalization periods and an increased number of subsequent postoperative consultations. They also have an increased risk of complaining of nonspecific symptoms. [18] One important factor related to their post-surgical experience is the patient’s involvement in the whole process. Patients who show a proactive attitude usually understand and respect the surgeon’s preoperative and postoperative indications. They also have a better progression and fewer complications. [19]
When the patient decides on explantation surgery, the surgeon must restore her normal breast aspect. The goal is to achieve beautiful female features that increase the patient’s confidence and improve emotional appearance. [20,21]
Conclusions
A novel phenomenon that brings plastic surgery under scrutiny is known as “Breast Implant Illness”. Due to the influence of online media, women worldwide share their opinions regarding their surgical experiences. Although social media has positive effects in that it can highlight seldom-discussed issues, the doctor must ultimately validate individual concerns and educate patients to better understand their situation. Moreover, a better-informed consent process should be implemented, especially for breast augmentation surgery in order to avoid legal issues, should the patient request the explantation surgery.
Surgeons should closely follow up with their patients and respect their wishes by removing the implants when requested, informing them that over half of the women with symptoms may improve after explantation. Although the relationship between silicone implants and various systemic disorders is becoming clearer, establishment of global registers to collect data could assist in understanding this relationship better.
Conflict of interest disclosure
There are no known conflicts of interest in the publication of this article. The manuscript was read and approved by all authors.
Compliance with ethical standards
Any aspect of the work covered in this manuscript has been conducted with the ethical approval of all relevant bodies and that such approvals are acknowledged within the manuscript.
References
- U.S. Epidemiology of Breast Implant-Associated Anaplastic Large Cell Lymphoma. Plast Reconstr Surg. 2017, 139, 1042–1050. [CrossRef] [PubMed]
- ASPS. “Report of the 2017 Statistics.” American Society of Plastic Surgeons (ASPS). 2018. Available online: https://www.plasticsurgery.org/documents/News/Stati stics/2017/plastic-surgerystatistics-report-2017.pdf.
- Dush, D.M. Breast implants and illness: A model of psychological factors. Ann Rheum Dis. 2001, 60, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Healing Breast Implant Illness. Breast implant safety. Available online: http://healingbreastimplantillness.com/breastimplant-safety/. (accessed on 18 April 2017).
- Tugwell, P. Rheumatology: Clinical case definitions/diagnoses and clinical associations. In: Diamond BA, Hulka BS, Kerkvliet NI, Tugwell P, eds. Silicone breast implants in relationton connective tissue disease and immunologic dysfunction. A Report by a National Science Panel to Hon. Sam C Pointer Jr, Coordinating Judge for Federal Breast Implant Multidistrict Litigation. United States District Court, District of Oregon: 1998.
- Barsky, A.J.; Borus, J.F. Functional somatic syndromes. Ann Intern Med. 1999, 130, 910–921. [Google Scholar] [CrossRef] [PubMed]
- Jewell, M.L.; Jewell, H.L. Breast Implant-Associated Illness: Medicine by Belief, So Says Dr. Google. Aesthet Surg J. 2019, 39, NP87–NP89. [Google Scholar] [CrossRef] [PubMed]
- Zuckerman, D.; Srinivasan, V. Breast Implant Illnesses: What’s the Evidence National Center for Health Research, Washington, DC 20036.
- Hu, H.; Jacombs, A.; Vickery, K.; Merten, S.L.; Pennington, D.G.; Deva, A.K. Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: Implications for breast implant- associated lymphoma. Plast Reconstr Surg. 2015, 135, 319–329. [Google Scholar] [CrossRef]
- Cozma, C.C.; Avino, A.; Balcangiu-Strescu, A.E.; Balan, D.G.; Tanasescu, M.D.; Timofte, D.; Sinescu, D.R.; Stoicescu, S.M.; Ionescu, D. Textured Breast Implants and Anaplastic Large Cell Lymphoma. Materiale Plastice. 2019, 56, 71–72. [Google Scholar] [CrossRef]
- Doren, E.L.; Miranda, R.N.; Selber, J.C.; Garvey, P.B.; Liu, J.; Medeiros, L.J.; Butler, C.E.; Clemens, M.W. U.S. Epidemiology of Breast Implant–Associated Anaplastic Large Cell Lymphoma. Plast Reconstr Surg. 2017, 139, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Shen, G.Q.; Ojo-Amaize, E.A.; Agopian, M.S.; Peter, J.B. Silicate antibodies in women with silicone breast implants: Development of an assay for detection of humoral immunity. Clin Diagn Lab Immunol. 1996, 3, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.B.; Carroll, C.; Tenenbaum, M.M.; Myckatyn, T.M. Breast Implant–Associated Infections: The Role of the National Surgical Quality Improvement Program and the Local Microbiome. Plast Reconstr Surg. 2015, 136, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Schreml, S.; Heine, N.; Eisenmann-Klein, M.; Prantl, L. Bacterial Colonization Is of Major Relevance for High- Grade Capsular Contracture After Augmentation Mammoplasty. Ann Plast Surg. 2007, 59, 126–130. [Google Scholar] [CrossRef] [PubMed]
- General and Plastic Surgery Devices Panel Transcript. 14 October 2003. Available online: http://wayback.archiveit. org/8871/20170429032345/https://www.fda.gov/ohrms/dockets/ac/03/transcripts/3989T1.htm.
- Adams, S.T.; Cox, J.; Rao, G.S. Axillary silicone lymphadenopathy presenting with a lump and altered sensation in the breast: A case report. J Med Case Rep. 2009, 3, 6442. [Google Scholar] [CrossRef] [PubMed]
- Zambacos, G.J.; Molnar, C.; Mandrekas, A.D. Silicone lymphadenopathy after breast augmentation: Case reports, review of the literature, and current thoughts. Aesthetic Plast Surg. 2013, 37, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Scăunașu, R.V.; Voiculescu, Ș.; Popescu, B.; Popa, R.; Bălălău, D.O.; Răducu, L.; Cozma, C.N.; Jecan, C.R. Depression and breast cancer; postoperative short-term implications. J Mind Med Sci. 2018, 5, 82–84. [Google Scholar] [CrossRef]
- Scaunasu, R.V.; Voiculescu, S.; Popescu, B.; Cozma, C.; Jecan, R.; Balalau, C. The psychological influence of the diagnosis of breast cancer on therapeutic options selection. J Mind Med Sci. 2017, 4, 172–177. [Google Scholar] [CrossRef]
- Jecan, R.C.; Hernic, A.D.; Filip, I.C.; Răducu, L. Clinical Data Related to Breast Reconstruction; Looking Back on the 21th Century and Forward to the Next Steps. J Mind Med Sci. 2015, 2, 34–42. [Google Scholar]
- Mark Magnusson, M.R.; Cooter, R.D.; Rakhorst, H.; McGuire, P.A.; Adams, W.P., Jr.; Deva, A.K. Breast Implant Illness: A Way Forward. Plast Reconstr Surg. 2019, 143, 74S–81S. [Google Scholar] [CrossRef] [PubMed]


© 2019 by the authors. 2019 Răzvan Danciu, Cristina N. Marina, Valeriu Ardeleanu, Romeo Marin, Răzvan-Valentin Scăunașu, Laura Răducu