Abstract
Background: Medication adherence and persistence in treating chronic diseases present as a continuous challenge for healthcare providers in long-term management. The most frequent reasons that several diseases are poorly controlled in the population include suboptimal drug adherence and discontinuation of therapies. One main issue why physicians cannot detect patients with poor adherence is that they have relatively limited time and tools to do so. Aim: To review the critical role of medication adherence in the management of chronic diseases by addressing the following: what medication adherence is; its critical role; factors and strategies influencing it; challenges and consequences of poor adherence; patients at risk; present and future strategies in place to detect and improve adherence; implications for public health and health value creation for patients; key analytical frameworks for understanding it; determinants; how adherence improves health; the role of healthcare professionals and technological innovations; implications of medication adherence; adherence as a key area for exploring the psychological mechanisms underlying patient behavior; and patient adherence as a major social and public health challenge. Finally, this review considers strengths, limitations, recommendations, and future value. Methodology: The following databases were used to carry out the review: PubMed, Scopus, Google Scholar, and ScienceDirect. The following themes were combined in the search: what adherence is, why it is critical, why adherence occurs, and how to improve adherence. The following search terms were used: what adherence is and critical, why and adherence and occurs, and how and to improve adherence. Results: Under the theme of why adherence is critical, five sub-themes were reviewed; four sub-themes were reviewed under the theme of why adherence occurs; and five sub-themes were reviewed under the theme of how to improve adherence. Conclusions: Strategies to enhance medication adherence involve a comprehensive approach that includes patient education, streamlined treatment plans, digital tools, and effective communication from healthcare professionals.
1. Introduction
1.1. Definition of Adherence
The World Health Organization (WHO) defined adherence as “the execution of lifestyle changes in terms of medication, person’s behavior, following a diet all to correspond with agreed endorsements from a health care personnel” (Burleson et al., 2025) [1]. This definition highlights that adherence is a process between a patient and a healthcare provider, and it encompasses various health-related actions beyond just taking medication. WHO’s definition of adherence aligns with mutually agreed health recommendations from a provider and is a patient-centered concept emphasizing behavior.
Medication non-compliance is critical for managing chronic conditions. As stated by Religioni et al. (2025) [2], it prevents disease progression, reduces complications, and decreases hospitalization rates. Furthermore, it improves quality of life, thus lowering healthcare costs. According to Chauke et al. (2022) [3], a significant worldwide health issue is poor medication adherence. The WHO (2003) [4] further highlighted that up to half of patients with chronic conditions in high-income countries do not take their treatments as prescribed. This leads to increased healthcare costs, worsening health outcomes, and potential death.
1.2. Why Medication Adherence Is Critical
Mir TH (2023) [5] states that adherence is critical because it ensures medication is taken correctly and consistently, which is vital for controlling chronic conditions, preventing disease progression, avoiding drug resistance, and achieving the best health outcomes.
1.2.1. Prevents Disease Progression and Death
Medication adherence is defined as taking medication as prescribed by the provider. Furthermore, taking treatment as prescribed is essential to control chronic diseases and prevent them from worsening, which can be fatal. Medication adherence is heavily reliant on the experience of individuals and is an integral part of optimal clinical outcomes. Unni et al. (2023) [6] discuss that, as a basis for explaining medication adherence, a new hierarchical model was developed incorporating health literacy. The hierarchical steps to achieve medication adherence are beliefs towards illness and medication, and self-efficacy.
1.2.2. To Avoid Drug Resistance
The correct use of medicines—by taking them exactly as prescribed and for the full duration—prevents infections through good hygiene and vaccination, and supports public health efforts, like reducing unnecessary antibiotic use in agriculture. For specific treatments, like HIV, adhering strictly to the prescribed regimen, as directed by healthcare providers, helps maintain an undetectable viral load. As investigated by Ahmed et al. (2024) [7], antimicrobial resistance (AMR), leading to the emergence of resistant microorganisms, is a critical global health issue driven by antibiotic misuse and overuse in various sectors. One major psychosocial determinant of adherence to antibiotics is the way the public perceives the threat of AMR. Lee et al. (2023) [8] state that individuals appraise their vulnerability through the severity of the adverse consequences of an event or action and threat perceptions.
The increase in MDR pathogens causing important problems for healthcare systems worldwide dates back to the history of AMR discovery following penicillin, as shown in Scheme 1. Scheme 1 represents various mechanisms through which bacteria develop resistance to antibiotics (Vivekanandan et al., 2025) [9]. Bacteria have specialized proteins in their membranes that actively expel antibiotics from the cell. This prevents the antibiotic from reaching its target concentration inside the bacterial cell, making the treatment less effective; this mechanism is known as efflux pumps.
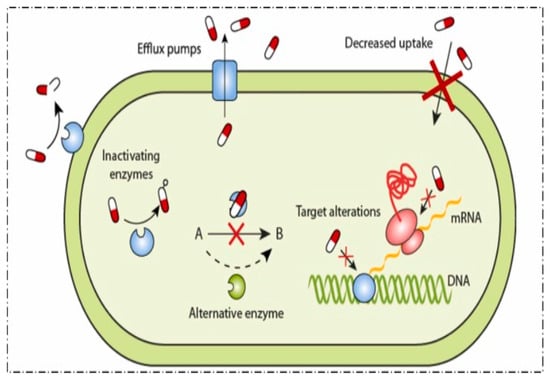
Scheme 1.
Various mechanisms through which bacteria develop resistance to antibiotics, adapted from Vivekanandan et al. (2025) [9]. CC BY 4.0.
1.2.3. Improve Health Outcomes
Patients who take their treatment as prescribed demonstrate good health outcomes, characterized by improved quality of life, enhanced functionality, and reduced disability. Religioni et al. (2025) [2], in agreement with this statement, say that patients’ compliance leads to fewer complications, better management of their disease, and improved long-term survival, with studies showing significant clinical benefits in chronic conditions like cardiovascular disease.
As reported by Howard et al. (2024) [10] in the United States, patients do not take their medicine as prescribed 50% of the time. Furthermore, 33% to 69% of drug-related hospital admissions are because of poor compliance with medication, at a cost of approximately USD 100 billion per year. Conversely, non-adherence often leads to higher hospital readmissions, increased mortality rates, and worse clinical outcomes.
1.2.4. Enhances Quality of Life
As supported by Religioni et al. (2025) [2], effective management of chronic conditions through patient adherence to treatment plans directly contributes to a high overall quality of life (QOL) by improving health outcomes. Furthermore, it contributes to fewer complications and enhances well-being. Adherence ensures that treatments, such as medications or lifestyle changes, are followed correctly, which helps control the condition, prevents disease progression, and minimizes potential health-related burdens.
Furthermore, Panayi et al. (2024) [11] support the above statement, indicating that medication adherence significantly enhances QOL by ensuring treatments are effective, leading to better disease management, fewer complications, and thus improving overall well-being. Consistent use of prescribed medication helps manage chronic conditions, reducing the severity of symptoms and the likelihood of negative health outcomes, like hospitalizations and mortality.
As discussed by Panah et al. (2022) [12], adherence to medical recommendations generally improves QOL by enhancing disease control and reducing complications, but factors like socioeconomic issues, patient beliefs, fear of side effects, psychological distress, and poor health literacy can hinder adherence. Berardinelli et al. (2024) [13], in agreement with the above authors, concludes that tailoring interventions through shared decision-making, clear communication, patient education, involvement of caregivers, and support for managing costs is crucial to overcome these barriers and personalize treatment for better adherence and outcomes.
1.3. How Adherence Improves Health
1.3.1. Better Disease Control
By following treatment plans, patients can effectively manage their conditions, preventing the progression of diseases and the onset of new complications. According to Huang et al. (2024) [14], following a treatment plan for chronic conditions improves health by controlling the disease, preventing serious complications, and enhancing the patient’s well-being. Following a treatment plan for chronic conditions is beneficial because it helps control the disease, prevents serious complications, and increases the patient’s overall quality of life. Jan et al. (2025) [15] advise that regular checkups, adhering to medication schedules, and engaging in self-management strategies are crucial for effectively managing chronic conditions over the long-term. This involves taking medications as prescribed, scheduling regular medical checkups, monitoring your health, and improving healthy lifestyle habits, like good sleep, exercising regularly, and eating a balanced diet.
1.3.2. Reduce Complications
In his study, Burnier, M (2024) [16] concluded that adhering to a treatment plan helps manage chronic diseases by averting serious illnesses and controlling symptoms. This leads to fewer hospitalizations, better quality of life, and improved patient health outcomes. For example, proper adherence to medication can prevent damage to the target organ, like left ventricular hypertrophy, reducing cardiovascular events such as myocardial infarction in hypertensive, diabetic, and dyslipidemia patients.
1.3.3. Lowers Hospitalization Rates
As discussed by Panah et al. (2022) [12], patients who follow their treatment plans are generally less likely to be hospitalized for complications or worsening of their health status. Treatment adherence plans are important, as they directly improve disease control, improve quality of life, reduce healthcare expenses, prevent hospital admissions, and lessen the risk of complications by ensuring patients follow their prescribed regimens effectively. According to Patel et al. (2025) [17], addressing barriers to adherence through patient knowledge, simplified regimens, and digital health tools, with strong healthcare professional support, is key to achieving these positive outcomes for individuals and healthcare systems.
1.4. Factors Influencing Medication Non-Adherence
Several determinants lead to non-compliance; therefore, knowing these various factors is important in planning appropriate interventions, as follows:
1.4.1. Factors Related to Patients
As discussed by Pourhabibi et al. (2022) [18], patients’ education, beliefs, and psychological factors significantly affect adherence. For example, as confirmed by Tariq et al. (2025) [19], low health knowledge and misinterpretation of the condition and its therapy can result in inappropriate utilization of drugs. Conditions affecting the mind like depression and anxiety significantly decrease treatment adherence, especially in those with chronic illnesses, creating a negative feedback loop. Hisan et al. (2025) [20] agreed with the statement that depression can diminish motivation, affect cognitive function, and induce feelings of hopelessness, making it difficult to follow complex treatment regimens. Anxiety, fueled by constant symptoms of worry and fear of complications, also interferes with daily functioning and adherence to therapies.
1.4.2. Factors Related to Treatment
The complexity of treatment protocols, including the number of times and number of drugs, plays a vital role in adherence. According to Ngcobo N.N (2025) [21], polypharmacy, common in the elderly due to multiple chronic conditions, significantly increases the risk of medication errors, adverse drug effects, hospitalizations, and reduced compliance because of the increased complexity of medication regimens, age-related physiological changes, and potential drug interactions.
Jandu et al. (2025) [22] advise that, to mitigate medication-related risks, healthcare providers should implement comprehensive medication reviews, deprescribe unnecessary drugs, enhance communication between patients and providers, and use tools like the Beers Criteria to identify and manage potentially unsuitable drugs. This systematic approach improves medication safety and effectiveness, especially for older adults who often take multiple medications. Furthermore, adverse drug effects, specifically with extended medication, can deter patients from continuing medication as ordered (Lustberg et al., 2023) [23].
1.4.3. Factors Related to the Healthcare System
Restricted access to the healthcare system includes insufficient communication between patient and provider and inadequate follow-up devices, as concluded by Sharkiya S.H (2023) [24], who emphasized that a high-quality patient–provider association is essential because poor association and insufficient trust between patients and healthcare providers significantly undermine adherence to prescribed treatments. Indeed, effective communication fosters trust, enabling patients to share their concerns, understand their treatment plans, and engage in self-management, all of which are vital for positive health outcomes. Moreover, Yenet et al. (2023) [25] concluded that structural barriers, such as insufficient access to drugs in certain areas and high out-of-pocket expenditures further exacerbate non-adherence.
1.4.4. Socioeconomic Factors
Socioeconomic status (SES) significantly impacts health and treatment adherence, as higher SES is often associated with increased adherence to medical treatments for non-communicable diseases like asthma and diabetes, as discussed by Hill-Briggs et al. (2020) [26]. This relationship is multifaceted, with components of SES, such as income, education, and occupation, influencing factors like health literacy, access to quality healthcare, housing, and reduced stress, all of which affect a person’s ability to comply with medical advice.
Socioeconomic status, as concluded by Pribisalić et al. (2021) [27], is one of the major determinants of compliance. Patients with lower incomes often find it difficult to afford medications, which can lead to dose rationing or missed doses. Moreover, social support networks, or the lack thereof, can either encourage or hinder adherence behaviors. Low SES can create barriers like financial strain, lack of access to care, and increased stress, negatively impacting adherence and health outcomes, as reflected in Scheme 2 of barriers to medication adherence (Kvarnström et al., 2025) [28].
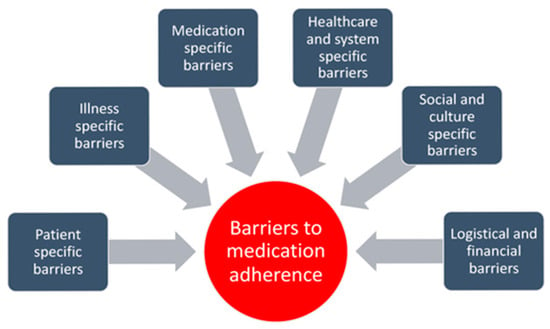
Scheme 2.
Barriers to medication adherence, adapted from Kvarnström et al. (2025) [28]. (CC BY 4.0).
1.5. Strategies to Improve Medication Adherence
Kardas P, (2024) [29] in his study on strategies to improve adherence, suggests that efforts should focus on simplifying treatment plans by providing clear and accessible education about the condition and treatment, using reminders and technology, empowering patients with self-management skills and social support, and ensuring affordability and easy access to medications and care.
A collaborative, multidisciplinary approach is indeed effective, especially when combined with patient education and tailored interventions that address individual barriers to treatment, including motivation, behavioral skills, healthcare access, information and knowledge, system-specific factors, and logistical and financial factors (Kvarnström et al., 2021) [28] (as shown in Figure 1).
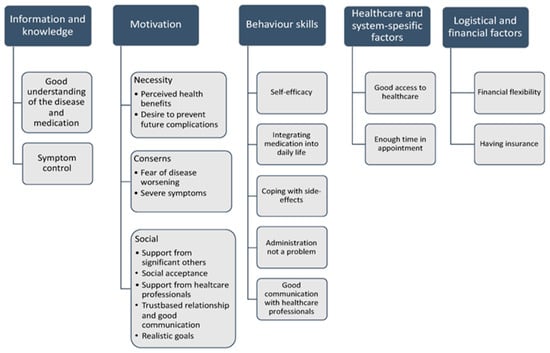
Figure 1.
Determinants of medication adherence, adapted from Kvarnström et al. (2021) [28].
Fragner et al. (2024) [30] suggests that this patient-centered model brings together various healthcare professionals to coordinate care, leveraging their combined expertise to provide comprehensive and individualized support for patients. Ricci et al. (2022) [31] further explain that patient education empowers individuals, fostering self-efficacy and improving treatment outcomes by helping them understand and overcome obstacles like lack of credible information or stress.
1.5.1. How to Improve Adherence
Improving adherence requires a multifaceted approach involving both patients and healthcare providers. Enhancing drug compliance requires a multifaceted view that includes patients, healthcare providers, and healthcare organizations. As concluded by Maniki et al. (2024) [32], for patients, this involves understanding their condition, managing their medication regimens effectively, and utilizing tools like reminders and educational materials. Providers play a key role by simplifying regimens, offering patient-centered education, and using technology for monitoring.
Health systems can improve medication adherence by lowering costs, coordinating care to create a seamless patient experience, and applying principles of implementation science to close the gap between knowledge-based interventions and actual medical practice. Jones et al. (2024) [33], in agreement with the above statement, state that these strategies work together to address system-level barriers, enhance patient education and engagement, and ensure new practices are effectively integrated into real-world healthcare settings. Health systems can further support adherence by reducing medication costs, promoting coordinated care models, and integrating implementation science into practice.
1.5.2. Patient-Centered Care
Effective interventions for medication adherence need to be patient-specific, complex, and patient-focused. This was discussed by Xu and others (2020) [34], whose research findings revealed that enhancing prolonged compliance requires phenomenological research, greater reliance on factual evidence, and deeper cooperation among partners. This also includes an intense focus on comprehending patients’ feelings. Interventions should be adjusted to individual patients’ requirements and beliefs.
1.5.3. Patient Education
Atolagbe et al. (2023) [35] dispute that patient education on medication adherence leads to a better understanding of strategies for improvement and the importance of simplified treatment regimens. The authors further support the need for more robust, well-planned educational interventions to enhance drugs compliance and health effects, noting that patients showed varied reactions to treatment and highlighting the significance of tailored, multifaceted methods to support both knowledge and adherence.
1.5.4. Simplified Treatment Regimens
Hiligsmann et al. (2025) [36] discuss two main barriers to medication adherence: practical barriers (e.g., amnesia) and emotional obstacles (e.g., hesitancy about treatment fundamentals). These can be addressed by using clarified simplified drug plans and personalized strategies. Questionnaires, like the 15-STARS tools, assist healthcare providers in ascertaining causes of non-adherence and guiding personalized interventions. Drug compliance is affected by patient attitudes, treatment burden, and factors influencing the healthcare system (Arnet et al. (2024) [37]).
1.5.5. Digital Health Tools
In their review on the application of digital health tools to medication adherence, Lu et al. (2025) [38] conclude that digital health tools, including mobile apps, wearables, smart devices, and telehealth, improve medication adherence in chronic conditions. Digital health tools provide personalized reminders, education, and real-time monitoring, leading to better patient outcomes. Mason et al. (2022) [39] express that online medical instruments, such as mobile applications, smart devices, and electronic pill dispensers, improve patient adherence by providing medication reminders, monitoring intake, and offering feedback. These data enable healthcare providers to identify adherence barriers, deliver targeted interventions, offer personalized guidance, and enhance pharmacotherapeutic follow-up, leading to better health outcomes. While promising, challenges like digital literacy, data privacy, and equitable access must be addressed to ensure widespread adoption and clinical validation.
1.5.6. Pharmacist-Led Services
To improve drug compliance among clients with chronic ailments, pharmacists play an important role through support and education. As Ciliberti et al. (2024) [40] dispute, pharmacists provide personalized information about medications, help resolve adherence barriers, conduct medication reviews, and work jointly with other healthcare providers to optimize care plans. These interventions empower patients to control their diseases better, leading to better health results and potentially minimizing healthcare costs.
Pharmacists also play a pivotal duty in educating patients about drug compliance through personalized patient education on how to take their treatment, major adverse effects, and drug interactions. In addition, they provide ongoing support through follow-up, medication reminders, and addressing patient-specific barriers. As stated by White et al. (2025) [41], their expertise in pharmacotherapy allows them to resolve medication-related problems, simplify complex regimens, improve patient health outcomes, and reduce hospital readmissions.
1.6. Approaches to Enhance Medication Adherence: The Responsibilities of Healthcare Personnels and Technological Innovations
Several plans have been formulated to enhance compliance adherence to treatment, many of these interventions have demonstrated good outcomes on both clinical outcomes and HRQOL. These strategies are summarized under the headings: strategy, description, and benefits, as shown in Table 1.

Table 1.
Strategies to improve therapy adherence, adapted from Religioni et al. (2025) [2].
1.6.1. Patient Education
Schnorrerova et al. (2025) [42] suggest that patient education is one of the most effective strategies for improving medication adherence. This involves improving patients’ literacy of their illness and adherence to treatment. Academic involvement aimed at improving drug compliance commonly utilize interventions such as therapy sessions with healthcare providers, electronic digital programs, and printed materials to educate patients about their diseases and therapy management.
These methods aim to address various barriers to adherence, including lack of understanding, forgetfulness, and negative beliefs about medication, by providing tailored, patient-centered information and support. As concluded by Ranjbar et al. (2024) [43], increasing patients’ knowledge and motivation enhances compliance and ultimately enhances HRQOL by reducing difficulties and encouraging a sense of control over the condition. This is explained by behavioral reasoning theory, which talks about values, attitudes, behavior, and perceived behavioral control, as demonstrated in the flow diagram below.
1.6.2. Digital Health Tools
According to Mason et al. (2022) [39], technological innovations that support adherence are mobile health applications and electronic medication monitoring systems. These instruments provide patients with reminders to identify compliance in real time, to take their medicines, and assist medical providers in intervening when essential. A study by Cheng et al. (2023) [44] disclosed that patients using such tools report better HRQOL and higher adherence levels, as they feel more engaged in their care and are less likely to skip doses. In chronic disease management, mobile tools, in particular, have been useful in allowing patients to take an engaging duty in observing their well-being, resulting in better results and higher satisfaction.
Paneerselvam and fellow authors (2025) [45] emphasized that technological innovations offer promising solutions for improving adherence, especially in the management of chronic diseases. Mobile apps are the most widely used tools for supporting adherence. These apps provide diverse tools such as medication reminders, real-time monitoring via wearables, educational resources, personalized feedback, and communication platforms that link patients with healthcare providers. Hsu et al. (2025) [46] indicated that, by leveraging features like gamification and data integration, mobile apps can enhance patient engagement, provide tailored support, and empower individuals to better manage their health conditions.
These apps often include features such as educational content, health tracking, and medication reminders. Research performed by Okolo and others (2024) [47] demonstrated that mobile health apps help patients maintain consistent medication schedules by providing real-time feedback on health outcomes. For example, medication intake and the use of apps that track blood sugar levels, better glycemic control in diabetic management, result in improved health outcomes in these patients.
Furthermore, electronic medication monitoring devices and mobile apps have emerged as useful devices for improving compliance. Ukoaka et al. (2024) [48] suggested that these tools monitor patients when they take their treatment and provide healthcare providers with compliance information, facilitating timely intervention when needed. Applications such as mySugr, Glucose Buddy, BookDoc, Diabetes M, Doctor2u, Blood Sugar Tracker–Diabetes, HealthifyMe, and Samsung Health are among the mHealth apps used by respondents.
1.6.3. Telemedicine
Telemedicine has also become a powerful tool for improving compliance, specifically in remote or underserved areas. Bokolo, A.J. (2021) [49] suggests that, through telemedicine platforms, healthcare providers can provide immediate guidance, track patient compliance, and conduct virtual consultations. For patients with chronic conditions such as hypertension or heart failure that require continuous monitoring, telemedicine is particularly beneficial. In conclusion, Ezenwaji et al. (2025) [50] state that telemedicine can assist in dealing with adherence problems early by enabling regular contact with healthcare personnel and preventing the severe rise in well-being issues.
1.6.4. Simplifying Treatment Regimens
Simplifying treatment regimens is another important strategy for improving adherence. Lower adherence rates are often associated with complicated regimens with many daily doses, because patients find it problematic to control or remember the intake of several drugs. Patel et al. (2025) [17] discuss that prescribing combination drugs or once-daily medications simplifies regimens. Medical personnels can thereby notably improve compliance and enhance patients’ HRQOL. When patients follow simpler regimens, they report less treatment burden and higher satisfaction, translating to fewer disruptions to their daily lives and better disease control.
1.6.5. Healthcare Professionals’ Involvement
Improving adherence to therapy and the deliberate implementation of technological transformations is a multifaceted challenge that requires the coordinated efforts of healthcare professionals. Mondesir et al. (2019) [51] support this statement by stating that physicians, pharmacists, and nurses are healthcare professionals who play vital roles in patient education and ongoing support, as they are at the forefront of efforts to improve adherence.
The physician’s role begins at the point of diagnosis and treatment planning, where clear communication is essential. Patients need to understand not only the possible repercussions of non-adherence but also the benefits of complying with their prescribed regimens. As concluded by Tian et al. (2024) [52], when physicians interact with patients in shared decision-making, patients feel more involved in their care, which tends to foster better adherence. Medication options are discussed together with patients. Moreover, simplifying therapy regimens enhances the likelihood of long-term compliance, and regimens ca be adjusted to individual patient needs.
Pharmacists also play a pivotal job by making sure that patients understand how to take their medications as prescribed through providing medication counseling. As contributed by Farhana et al. (2025) [53], pharmacist-led interventions, such as medication therapy management services, have been shown to remarkably improve adherence, particularly in patients with chronic conditions like diabetes, hypertension, and asthma. The use of pillboxes is another tool pharmacists can use to support adherence. As advised by Schnorrerova et al. (2025) [42], by addressing patient worries about side effects, dosage frequences, and serious drug interactions, pharmacists can help alleviate barriers to adherence.
Nurses are other healthcare personnels who contribute by supplying ongoing support through regular follow-ups. They identify early signs of non-adherence and follow-up on patient progress. Nurses have frequent contact with patients, particularly in effective chronic disease management programs. As contributed by Emanuel et al. (2020) [54], this helps reinforce adherence behaviors and ensure that any obstacles to adherence are quickly conveyed. Healthcare professionals play the role of helping to build trust and engagement with patients, which is essential for improving compliance by addressing key factors of adherence.
Intervention programs have the capacity to remarkably reduce healthcare costs. According to Kelepouris et al. (2023) [55], one of the most effective approaches that provide comprehensive patient support is the use of multidisciplinary teams. These teams, composed of physicians, pharmacists, nurses, and dietitians, work together to develop personalized care plans that address both clinical- and adherence-related challenges. Such programs, as quoted by Heo et al. (2023) [56], have been particularly successful in reducing hospital readmissions and emergency room visits in patients with chronic conditions like heart failure and diabetes, thus resulting in substantial cost savings.
Another important intervention strategy involves financial incentives that reduce the cost burden on patients. Dodd et al. (2018) [57] state that high out-of-pocket costs for drugs and treatments are a common barrier to adherence, particularly in low-income populations. Protocols that reduce or remove co-pays for important medicines have been shown to improve adherence and reduce overall healthcare costs by bringing down expensive complications and hospitalizations. Furthermore, as contributed by Qiao et al. (2020) [58], value-based insurance design programs reduce patient cost-sharing for high-value medications; in particular, these programs have demonstrated improvements in adherence in patients with chronic diseases such as diabetes and hypertension.
Pharmacist-led interventions, such as medication synchronization programs, have also proven effective in improving adherence and reducing expenditures. Medication synchronization enhances adherence by ensuring that all of a patient’s drugs are filled at the same time every month, lessening the complications of managing several prescriptions. A study conducted by Stewart et al. (2022) [59] revealed that patients registered in alignment plans are more likely to adhere to their drugs and experience less hospitalization and emergency room visits, leading to overall cost savings.
2. Problem Statement
Globally, medication non-adherence is a pervasive and complex problem among patients with chronic conditions (such as HIV/AIDS, hypertension, diabetes, epilepsy, asthma, and cardiovascular diseases) in primary healthcare (PHC) settings. Approximately 50% of patients in developed countries—and potentially more in low- and middle-income countries—do not take their medications as prescribed, despite the availability of effective medications and clinical guidelines (Oliveira et al., 2024) [60].
As stated by Patel et al. (2025) [17], while numerous research have identified several predictors influencing non-adherence (patient-related, medication-related, and healthcare system-related) and have tested different interventions, a key challenge is that physicians often have limited time and appliances to identify patients with impoverished adherence. Furthermore, many interventions shown to improve adherence in trials do not consistently translate into improved clinical outcomes in real-world primary care settings, suggesting a gap in understanding the most effective “critical control points” for intervention.
Therefore, Mackridge et al. (2025) [61] conclude that there is a need for a comprehensive review to systematically identify and synthesize the evidence on specific, high-impact “critical control points” within the primary healthcare workflow where targeted interventions can most effectively and efficiently enhance treatment adherence and, subsequently, clinical results for patients with chronic diseases. Such a review could help inform the development of practical, evidence-based strategies for primary care providers to address this persistent and costly challenge.
Research Question
The research question for this review on the critical role of medication adherence in patients with chronic diseases is as follows: “How do patient-related factors (perceived susceptibility, severity, benefits, and barriers) and social–environmental factors (social support, provider–patient relationship) influence the critical role of medication adherence, as analyzed through the lens of the Health Belief Model (HBM) and Albert Bandura’s Social Cognitive Theory, in the management of patients with chronic conditions in primary healthcare settings?”
3. Implications of Medication Adherence for Public Health and Health Value Creation for Patients
Patient adherence in chronic disease management is critical for creating both public and health value for patients by enhancing clinical results, improving quality of life, and notably reducing healthcare expenditures and the overall challenge on the healthcare system (Religioni et al., 2025) [2].
3.1. Value Creation for Public Health and Health Systems
From a public health and systems perspective, patient adherence is a cornerstone of sustainability and efficiency, offering substantial economic and societal value (Merchand. B, 2023) [62].
Significant cost savings: In countries like the US and UK, non-adherence results in billions of dollars in avoidable costs, while improved adherence frees up scarce healthcare resources and reduces the need for more intensive treatments, emergency room visits, and hospitalizations annually.
Increased system efficiency: When treatments work as intended due to adherence, it improves the efficiency of the entire healthcare system, from primary care to emergency services.
Improved population health: The WHO has suggested that improving adherence programs could have a greater effect on population well-being than the development of new medical treatments. Better-controlled diseases at the individual level lead to a healthier population overall.
Increased productivity: By maintaining patients’ health and ability to work, adherence reduces indirect costs associated with absenteeism, long-term disability, and premature death, contributing to a more productive economy.
Strengthened public trust: Successful patient outcomes and a more efficient healthcare system help build greater public trust and confidence in healthcare providers and institutions.
3.2. Health Value Creation for Patients
High patient adherence directly translates into tangible health benefits and improved quality of life (Kardas P, 2024) [29]:
Improved clinical outcomes: Adherence leads to better disease control (e.g., blood pressure and blood sugar levels), reduced incidence of complications (e.g., stroke, kidney failure, and amputations), and lower rates of morbidity and mortality (Kılıç and Güneş, 2024) [63].
Enhanced quality of life: Patients who comply with treatment regimens undergo fewer symptoms, less pain and fatigue, improved physical functioning, and greater independence, all of which contribute to an enhanced perception of well-being.
Reduced psychological distress: Effective disease management through adherence can mitigate feelings of helplessness, fear, anxiety, and depression that are often associated with poorly controlled chronic conditions.
Fewer hospitalizations and ER visits: By preventing disease exacerbations and complications, adherence reduces the need for emergency interventions and costly hospital stays.
The literature on medication adherence in chronic condition management features several robust conceptual and analytical frameworks. The most prominent models conceptualize adherence as a complicated, multidimensional behavior affected by a range of interacting agents (Zhang et al., 2025) [64].
3.3. Key Analytical Frameworks for Understanding Medication Adherence
3.3.1. The World Health Organization (WHO) Multidimensional Adherence Model (MAD) (Onwusah et al., 2025) [65]
This is one of the most widely recognized and comprehensive frameworks in the field. It conceptualizes adherence across five dimensions as shown in Scheme 3. Source: WHO, 2003 [4]. https://www.researchgate.net/figure/The-five-dimensions-of-adherence-Source-World-Health-Organization-WHO-2003_fig1_230858668 (accessed on 18 September 2025).
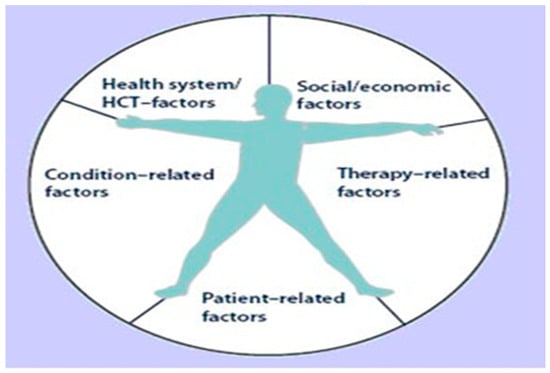
Scheme 3.
The WHO five dimensions of adherence, adapted from WHO (2003) [4].
Patient-related factors: Include individual demographics (age, education level), understanding of their illness and treatment, self-efficacy, and beliefs about the efficacy of medications.
Social and economic factors: Encompass social support from family and healthcare providers, cultural norms, financial resources, and health insurance coverage.
Therapy-related factors: Involves aspects of the treatment regimen itself, such as the complexity of the dosing schedule (polypharmacy), duration of treatment, and actual or perceived side effects.
Condition-related factors: Relates to the specific chronic condition, its severity, the presence of comorbidities, and whether the condition is symptomatic or asymptomatic.
Health system/healthcare team factors: Focuses on the healthcare delivery system, including accessibility of medications and services, the patient–provider relationship, quality of communication, and continuity of care.
3.3.2. The COM-B Model (Capacity, Opportunity, Motivation, and Behavior) (Michie et al., 2022) [66]
As an analytical framework in systematic reviews, the COM-B model is increasingly used to categorize determinants of health behaviors, including medication adherence. This model postulates that for a behavior (adherence) to occur, a person must have the motivation, opportunity, and capability to perform that behavior.
Capacity: Both physical (e.g., functional ability and memory) and psychological (e.g., knowledge, cognitive function, and emotional state) ability to take medication as prescribed.
Opportunity: The physical environment (e.g., access to pharmacy and medication packaging) and social environment (e.g., social support and financial situation) that enable the behavior.
Motivation: Reflective (e.g., beliefs, intentions, and illness perceptions) and automatic (e.g., habits and impulses) processes that direct behavior.
These frameworks provide a robust basis for researchers and clinicians to analyze the complex drivers of non-adherence, moving beyond single-factor analyses to develop tailored, multidimensional interventions for improving outcomes in chronic disease management.
3.4. Determinants of Patient Adherence
Determinants of patient adherence are multifaceted and are often categorized by the WHO (2003) [4] into the following five dimensions: patient-related (beliefs, motivation, self-efficacy, knowledge), therapy-related (complexity, side effects), condition-related (severity, symptoms), health system/provider-related (communication, access, cost), and socioeconomic (income, education, support) factors, all interacting to influence whether someone follows treatment plans, as explained by models like COM-B (Peh et al., 2021) [67].
3.4.1. Quality of Life in Relation to Health Value
According to Cai et al. (2025) [68], while Health-Related quality of life (HRQOL) is a health-focused subset that measures how health affects life domains like function, emotions, and social life—linking personal experience to broader “health value” by evaluating if health enables a fulfilling life rather than just the absence of disease—quality of life (QoL) is a vast concept of overall well-being. Health value is not just biological; it is how well someone lives, making HRQOL a key metric for healthcare goals beyond survival by assessing subjective well-being and functional capacity.
3.4.2. The Link to Health Value
Health as a means: Health is not the end goal but a means to achieving good QoL, representing one’s ability to pursue valued life possibilities.
Subjective and objective: Health value is subjective, as people value health differently based on their expectations, but it is measured through both self-reported feelings (HRQL) and objective measures of functioning.
Holistic well-being: Health value moves beyond just treating illness (e.g., cancer) to improvements in the patient’s overall experience, including social, emotional, and physical aspects.
3.5. Adherence as a Key Exploration of the Psychological Mechanisms Underlying Patient Behavior (Religion et al., 2025) [2]
A deeper exploration of patient adherence reveals a complex interplay of cognitive, emotional, and social factors, often explained through key psychological mechanisms and health behavior models. These mechanisms show that adherence is an active, and often intentional, decision-making process influenced by an individual’s personal context and environment.
3.5.1. Key Psychological Mechanisms
The primary psychological drivers of adherence behavior are as follows:
Beliefs and perceptions: Patients conduct a continuous, often subconscious, cost–benefit analysis, weighing beliefs about the necessity of medication against their concerns about potential side effects, long-term harm, or inconvenience. Their perceptions of illness severity and susceptibility to negative consequences are powerful motivators.
Self-efficacy: This refers to a patient’s confidence in their capability to effectively carry out the prescribed regimen, even when facing obstacles. Higher self-efficacy is a strong predictor of adherence and can be enhanced through positive experiences, social support, and skill development.
Motivation and intention: Behavior is often mediated by a patient’s intention to act, which is in turn shaped by attitudes, subjective norms (social pressure), and perceived behavioral control. Both intentional non-adherence (a conscious decision) and unintentional non-adherence (e.g., forgetfulness or financial issues) are prevalent and require different intervention strategies.
Habit and automaticity: Over time, adherence can become an non-intentional, automatic habit that requires less conscious cognitive effort. Integrating medication-taking into daily routines (e.g., taking pills during a regular meal) can facilitate this process.
Trust and communication: A strong, trusting relationship with healthcare providers is crucial. Patients are inclined to comply with therapy when they feel that their doctors are competent, concerned about their welfare, and involve them in shared decision-making.
3.5.2. Motivation and Barriers Affecting Adherence Among Patients with Chronic Illnesses
Compliance with medication plans for chronic illnesses is influenced by social, economic, healthcare system factors, and a complex interplay of personal factors (Chauke et al., 2022) [3].
Motivations for Adherence
Motivations are primarily driven by a particular patient’s belief in the necessity and effectiveness of treatment, personal well-being, and support systems (Zhang, 2025) [64]:
Belief in treatment efficacy and necessity: Patients are motivated to adhere if they believe the medication is necessary to control their disease and that the benefits outweigh the costs or side effects.
Perceived threat of illness: A strong understanding of the potential severe consequences and complications of the disease if left untreated can be a powerful motivator.
Positive health outcomes: Experiencing improvements in health or quality of life after starting treatment reinforces positive beliefs and encourages continued adherence.
Self-efficacy and personal responsibility: A patient’s trust in their capability to manage their illness, and sense of personal responsibility for their health, significantly improves adherence.
Strong healthcare provider relationship: Trust and good communication with doctors, pharmacists, and nurses can enhance a patient’s confidence and commitment to their treatment plan.
Social and family support: Emotional and practical support (e.g., reminders, financial help, and shared experiences) from family, friends, or support groups helps patients cope with daily challenges and stay on track.
Clear health goals: Having realistic and achievable treatment goals, along with a clear understanding of the treatment plan, improves motivation and compliance.
Barriers to Adherence
Barriers can be intentional (a conscious decision not to adhere) or unintentional (forgetfulness or practical difficulties).
Financial constraints and costs: The cost of medication, insurance issues, and transportation expenses are major barriers, especially for low-income patients.
Forgetfulness and complex regimens: Unintentional non-adherence often stems from simply forgetting to take medication, which is exacerbated by complex dosing schedules (multiple daily doses or many different pills).
Side effects and fear of medication: Concerns about actual or potential side effects, fear of lifelong dependency, or beliefs that medications are “toxic” are common reasons for avoiding or stopping treatment.
Lack of knowledge or misunderstanding: Patients may not fully understand their condition, the need for medication, or the proper way to take it, leading to self-adjustment of dosage or discontinuation.
Psychological factors: Depression, anxiety, stress, denial of the illness, and “treatment fatigue” (burnout from long-term management) can significantly hinder adherence.
Poor communication with healthcare providers: Inadequate patient counseling, short appointment times, and a lack of empathy or shared decision-making can lead to a breakdown in trust and information transfer.
Social and cultural norms: Stigma surrounding the disease (e.g., HIV/AIDS), pressure to participate in social ceremonies involving forbidden foods/drinks, and reliance on alternative traditional or spiritual healers can negatively impact adherence.
Healthcare system issues: Long waiting times, drug shortages, and remote healthcare facilities present logistical challenges to accessing treatment.
4. Method
The methodological perspective of the review.
This review was systematically constructed in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Respati et al., 2025) [69]:
4.1. Data Search Strategy
The following three major databases were used to conduct the literature search: Scopus, PubMed, and Google Scholar. To pinpoint studies centered on the critical role of medicine adherence in the management of chronic conditions, the search methodology involved utilizing a blend of keywords and Boolean operators. Across these databases, a detailed search strategy was used. The search was limited to studies published between 2020 and 2025 to capture advancements in treatment adherence and chronic disease management. This search strategy was designed to cover a complex range of literature covering the pivotal role of medication adherence in the context of patients with chronic illnesses.
4.2. Eligibility Requirements and Study Selection
Inclusion and exclusion criteria
4.2.1. Inclusion Criteria
This inclusion criteria were as follows: (1) analytical studies or literature reviews; (2) descriptive studies; and (3) articles published in English. The review explicitly addressed medication adherence, influencing factors, and patients with chronic diseases. Additionally, primary research focusing on adults over 18 years of age and diagnosed with chronic illnesses, were included. The review focused on original or peer-reviewed articles from 2020 onward to capture the most current advancements in healthcare, treatment protocols, and medication adherence strategies in patients with chronic diseases attending primary healthcare settings, as well as studies that delve into the factors influencing medication adherence and its measurement.
4.2.2. Exclusion Criteria
Firstly, duplicates through both automated and manual procedures were eliminated. Thereafter, to assess their alignment with the inclusion criteria, the author screened the titles and abstracts of the remaining studies. Then, the full texts of studies that appeared relevant were reviewed. Exclusion criteria included the following: (1) studies involving chronic disease patients under the age of 18; (2) patients who did not align with the objectives of this review; (3) news articles, commentaries, editorials, or conference abstracts; (4) publications in languages other than English; and (5) incomplete titles or abstracts. Furthermore, studies that primarily address a wider spectrum of treatment compliance in chronic diseases, as well as research that focuses on patients with multimorbidity and studies that only report that adherence levels do not match influencing predictors, were excluded.
4.3. The Scientific Rigor of a Systematic Review’s Screening and Selection Process
The scientific rigor of a systematic review’s selection procedure and screening procedures is evaluated by assessing adherence, reproducibility, and transparency with respect to protocols like PRISMA. The following stages involve the protocols as outlined by Respati et al. (2025) [69]:
Stages of the Screening and Selection Procedure
Identification of records: The process begins with a comprehensive exploration of pertinent databases (e.g., PubMed, Scopus, and Embase) and other sources (e.g., gray literature and trial registries) using a well-defined search strategy. The number of records identified from each source is recorded.
Removal of duplicates: All retrieved records are collected in a citation management tool, and duplicate entries are removed before screening begins.
Title and abstract screening (level 1 screening): Two self-reliant judges screen the titles and abstracts of all remaining records against the predefined inclusion and exclusion criteria. Studies are generally included if they are potentially relevant and excluded only if clearly irrelevant. Disagreements between reviewers are resolved through discussion or by consultation with a third reviewer.
Full-text retrieval: The complete texts of all records deemed probably pertinent are sought and retrieved. The number of reports that could not be retrieved is documented.
Full-text screening (level 2 screening/eligibility assessment): The full-text articles are then critically assessed by two independent reviewers against the detailed, pre-specified eligibility criteria (e.g., specific study design, population, intervention, and outcome measures).
Final inclusion: Studies that meet all eligibility criteria are included in the final review. The number of included studies and the specific reasons for exclusion at the full-text stage (e.g., “wrong population” or “not an empirical study”) are documented.
4.4. Ensuring and Assessing Scientific Rigor
The process should incorporate several best practices to allow for a proper assessment of the scientific rigor of the review on medication adherence in patients with chronic conditions in a primary healthcare setting:
A prior protocol and registration: The review’s methodology, including the research question, search strategy, and eligibility criteria, should be defined in advance in a publicly registered protocol (e.g., in PROSPERO or OSF Registries) to minimize bias.
Independent reviewers: Using at least two independent reviewers for both title/abstract and full-text screening is standard practice to ensure objectivity and reduce selection bias.
Clear documentation: A detailed and transparent account of the entire selection process is crucial. This is typically achieved using a PRISMA flow diagram, which visually maps the number of records at each stage (identified, screened, excluded, and finally included) and the reasons for exclusions.
Risk of bias assessment and quality: Validated tools (e.g., the Cochrane Risk of Bias tool) are used to assess the strength of the overall evidence. Beyond selection, the quality and risk of bias of the included primary studies must be systematically evaluated.
Reporting guidelines: Adherence to the PRISMA declaration ensures complete and transparent communication of procedures and outcomes, which is necessary for others to assess the trustworthiness of the review’s conclusions (Scheme 4).
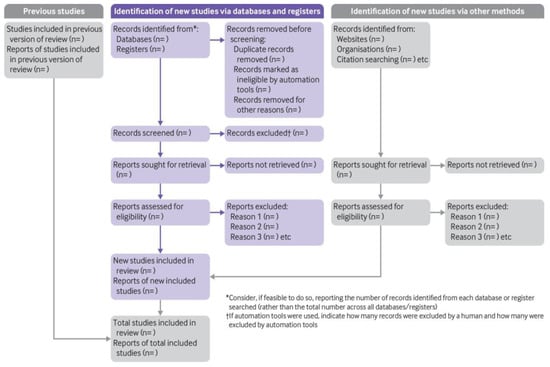
Scheme 4.
PRISMA 2020 flow diagram, adapted from Page et al. (2021) [70]. Creative Commons Attribution (CC BY 4.0) license.
4.5. Integrating a Broader and More Multidisciplinary Body of Work on Medication Adherence from the Social and Behavioral Sciences Perspective
As recommended by Patel et al. (2025) [17], the integration of broader and multidisciplinary work on medication adherence requires moving beyond individual compliance models toward a comprehensive, systemic approach that addresses the multifaceted nature of adherence. Adherence is affected by an interplay of determinants involving patient characteristics, social context, healthcare systems, condition-related issues, and therapy characteristics.
Key Social and Behavioral Factors
According to Zhang et al. (2025) [64], social and behavioral sciences research highlights that compliance is not merely a patient’s choice but is influenced by numerous determinants:
Beliefs and perceptions: Patient adherence is strongly influenced by the patient’s beliefs about the necessity of medication versus concerns about potential harm or side effects.
Knowledge and education: Inadequate awareness of disease consequences or the purpose of medication is a significant barrier. Clear communication and health literacy are crucial.
Social support: While a lack of support or social stigma can hinder adherence, support from family members, peers, and caregivers can significantly enhance it.
Socioeconomic status: Factors such as medication cost, insurance coverage, and accessibility to healthcare facilities are major determinants of adherence, with patients often prioritizing basic needs over medication.
Psychological factors: Mental health conditions like depression, forgetfulness, lack of motivation, and “treatment fatigue” from long-term regimens can negatively impact adherence.
Cultural norms: Social and cultural traditions can affect illness behaviors, for example, the use of alternative remedies or participation in social ceremonies where restricted foods/drinks are consumed.
There is need for a multidisciplinary approach which involves the following:
A single professional cannot address all the barriers to medication adherence, underscoring the need for multidisciplinary teams, as stated by Maxhakana and Sithole (2024) [71].
Holistic assessment: Multidisciplinary teams (including physicians, nurses, pharmacists, social workers, and psychologists) can conduct comprehensive, patient-tailored assessments to identify specific physical, psychological, and social barriers to adherence.
Integrated interventions: Interventions that merge scholastic, behavioral, and social elements are more successful than single-focus strategies. These may involve the following:
Patient education and empowerment: Tailored education programs that address patient-specific concerns and improve health literacy.
Behavioral support: Self-efficacy and planning skills are used to build techniques from models like the Social Cognitive Theory or the Theory of Planned Behavior.
Addressing systemic barriers: Pharmacists can help simplify medication regimens, use blister packs, or synchronize refills, while social workers can assist with financial and logistical challenges.
Enhanced communication: Burnie, M (2024) [16] says that fostering open communication and shared decision-making between patients and healthcare providers helps build trust and ensures that treatment plan aligns with the patient’s lifestyles and beliefs.
4.6. Outcome Measures
Evaluating the critical role of medication adherence in chronic disease management in a primary healthcare setting was the primary objective of this review. The specific objectives were to search for articles with the following topics: what medication adherence is; its critical role; factors influencing it; challenges and consequences of poor adherence; patients at risk; and present and future strategies in place to detect and improve adherence and assist non-adherent cases suffering from chronic diseases. Furthermore, the analysis of quantitative data from the studies reviewed, regardless of the reported importance of these factors, was included as an outcome measure covering the determinants that affect medication adherence. This perspective was deliberate to provide a comprehensive inspection of adherence issues.
Since this is not a systemic review, it was not possible to carry out data synthesis or analysis, nor to design an extraction tool.
5. Discussion
5.1. Patient Adherence as a Major Social and Public Health Challenge
Patient adherence to treatment plans in the context of chronic disease is indeed recognized as a major social and public health challenge. The WHO (2003) [4], noting that only 50% of patients with chronic diseases in developed countries adhere to treatment recommendations, highlighted the problem of low adherence rates.
This challenge has significant ramifications:
- Poorer health outcomes: Non-adherence leads to increased morbidity, reduced quality of life, and higher rates of disease complications, as conditions remain poorly managed.
- Increased healthcare costs: Poor adherence is associated with the need for more intensive and expensive medical interventions down the line, increased emergency room visits, and higher rates of hospitalizations. It is estimated to cost hundreds of billions of dollars annually in preventable healthcare expenditure.
- Public health burden: At a population level, widespread non-adherence hinders public health efforts to manage the rising prevalence of chronic diseases like asthma, hypertension, and diabetes, impacting overall population health metrics.
5.2. Contribution of This Review to the Current Knowledge About Medication Adherence
A review on chronic medication adherence in primary care (PHC) significantly adds to current knowledge by detailing real-world barriers (e.g., cost, side effects, lack of education, and beliefs), highlighting the crucial role of healthcare providers (HCPs) in collaborative care (education and support), emphasizing the need for better assessment tools, and identifying key intervention strategies like simplifying regimens and team-based care. These insights are vital for improving patient outcomes beyond clinical trials. It bridges gaps between research and practice by showing that suboptimal adherence (~50%) persists and impacts quality of life, thereby pushing for integrated solutions in PHC settings.
5.3. How Medication Adherence Contributes to Current Knowledge
- Identifies context-specific barriers: Moves beyond general factors to pinpoint common issues in PHC, such as side effects, forgetfulness, financial strain, and lack of clear instructions, showing why adherence fails locally.
- Highlights provider–patient dynamics: Underscores that HCPs (doctors, pharmacists, and nurses) are pivotal; their communication, education, and shared decision-making significantly influence adherence, even more than just clinical data.
- Validates suboptimal adherence rates: Confirms that many patients (often ~50%) struggle with long-term treatment, validating previous WHO findings and showing that this remains a major challenge despite extensive research.
- Guides practical interventions: Provides evidence for strategies like pillboxes, blister packs, team-based care, and patient education tailored to PHC needs, improving outcomes cost-effectively.
- Reveals assessment gaps: Shows that accurately measuring adherence in community settings is hard and inconsistent, prompting calls for better tools to interpret research and clinical data.
- Connects beliefs and behavior: Explores how personal, cultural, and religious beliefs, alongside health literacy, impact adherence, suggesting that holistic approaches are needed.
In essence, such a review translates complex adherence research into actionable insights for frontline healthcare, emphasizing a shift from just prescribing medications to actively managing patients’ ability and willingness to take long-term medications.
6. Collaboration
The aim of this review was achieved through specific objectives that revealed the following outcomes. Articles addressing the following topics were reviewed:
- What medication adherence is.
- Its critical role.
- Factors influencing it.
- Challenges and consequences of poor adherence.
- Patients at risk.
- Present and future strategies in place to detect and improve adherence and to assist non-adherent cases suffering from chronic diseases.
- Furthermore, other outcomes well-documented the factors that influence treatment compliance through the examination of numerical data from the studies analyzed, irrespective of the reported importance of these factors. This strategy was meant to provide a complete evaluation of adherence-related issues.
- A strong partnership between patients, healthcare providers, and healthcare systems can foster better adherence and improved outcomes. Keelson et al. (2024) [72] propose that medicine adherence is critical for managing chronic conditions by improving treatment effectiveness, preventing disease progression, reducing hospitalizations, and lowering overall healthcare costs for both patients and healthcare systems.
- According to Religioni et al. (2025) [2], poor adherence, affecting up to 50% of patients, can lead to serious adverse outcomes, like worsening conditions, increased disability, and mortality. A multifaceted approach considering factors like patient motivation, treatment complexity, and effective interaction between patients and medical personnels is therefore necessary to improve adherence and achieve better long-term health outcomes.
7. Strengths
The specific strengths of the review on the “Critical Role of Medication Adherence in Patients with Chronic Conditions Attending a Primary Health Care Setting.”
7.1. Multifactorial Approach
A multifactorial approach offers significant strengths by providing a holistic understanding of the problem and guiding the development of more effective, personalized interventions.
A few key strengths of such a review article, as described by Patel et al. (2025) [17], are as follows:
- Comprehensive understanding: By examining the five key dimensions of adherence (healthcare system factors, socioeconomic factors, patient-related factors, condition-related factors, and therapy-related factors), the article moves beyond single explanations, providing a robust and nuanced view of a complex issue.
- Identification of diverse barriers: The multifactorial approach effectively identifies a wide array of reasons for non-adherence, including forgetfulness, cost, lack of education, patient beliefs, or poor provider communication, which allows for targeted strategies to be developed.
- Guidance for tailored interventions: Acknowledging multiple factors is crucial for developing patient-centered, individualized interventions. The review highlights that “one-size-fits-all” solutions are often ineffective and advocates for personalized approaches that address specific barriers for different patient groups.
7.2. Justification of High Relevance to Public Health
To justify the high relevance to public health in a review article on the critical role of medication adherence in chronic diseases, Oliviera et al. (2024) [60] argue that the focus should be on the substantial effects of non-adherence on patient results, healthcare system burden, and overall population health and economics.
Key Arguments for Public Health Relevance are as follows:
- Prevalence and magnitude of non-adherence: Approximately 50% of patients in developed countries with chronic diseases (e.g., heart disease, diabetes, and hypertension) do not comply with their dosing schedule, a rate considered as a major public health challenge by the WHO, (2003) [4]. This high prevalence translates into a significant, unaddressed health issue across the population.
- Adverse health outcomes: Poor adherence is directly linked to negative patient outcomes, including increased mortality, higher rates of hospitalizations, reduced quality of life, disease progression, and increased morbidity. In fact, it has a greater effect on health consequences than the specific medication itself.
7.3. Validity of Content
The validity of a review article on the critical role of medication adherence in chronic diseases is determined by the rigor of its methodology, the comprehensiveness of its literature search, and the objectivity of its conclusions. According to Shaheen et al. (2023) [73], the following are indicators of content validity:
7.3.1. Methodological Rigor
- Clear research question: A valid review starts with a focused and well-defined research question or objective, such as specific factors influencing adherence in certain populations or diseases.
- Systematic search strategy: Authors should describe a comprehensive and systematic search for all relevant published and unpublished studies using specific keywords and multiple databases, thereby minimizing publication bias.
- Explicit selection criteria: The study selection process (e.g., using two independent reviewers) should be transparent and documented (e.g., via a PRISMA flowchart), with clearly defined inclusion and exclusion criteria.
7.3.2. Content and Scope
- Comprehensive coverage: The article should cover all relevant aspects of medication adherence (patient-, medication-, and healthcare system-related factors) rather than focusing on only a few dimensions to the exclusion of others.
- Accurate data synthesis: The review should use appropriate methods to synthesize findings from the included studies (e.g., meta-analysis or thematic content analysis). Combining studies that are too different (“apples and oranges”) can lead to invalid conclusions.
- Evidence-based conclusions: Conclusions drawn must be directly supported by the evidence presented in the reviewed literature and not by authors’ personal opinions or biases. Authors should avoid confusing correlation with causation.
7.3.3. Transparency and Credibility
- Peer review: The article should be published in a reputable, peer-reviewed academic publication, which means that experts in the field have evaluated its quality and scientific rigor.
- Acknowledgement of limitations: A valid review article will transparently discuss its limitations and potential sources of bias (e.g., reliance on self-reported adherence data that may overestimate adherence).
- Citations: The article should cite specific, recent, and relevant sources to back up its assertions, and these sources should be cross-referenced to ensure their reliability.
7.4. Future Vision
The future vision for medication adherence in chronic diseases centers on a paradigm shift towards a patient-centric, technologically integrated, and multidisciplinary ecosystem of care. As said by Moon and Walsh (2025) [74], the goal is to move beyond simply measuring adherence to actively predicting and resolving barriers in real time, thereby improving patient outcomes and reducing healthcare costs.
Personalized Medicine and Interventions include the following:
- Tailored interventions: Future approaches will move away from one-size-fits-all strategies. Interventions will be highly personalized, considering an individual’s specific behavioral, social, economic, and cultural factors to address both intended and unintended non-adherence.
- Predictive analytics: The advancement and verification of sophisticated, data-driven predictive analytics will be prioritized. These models, utilizing machine learning and big data, will recognize patients at high risk of non-compliance before it happens, allowing for proactive, targeted support.
- Patient empowerment: A greater emphasis will be placed on collaborative decision-making in treatment planning, where patients are actively involved to foster a stronger sense of control over their health, self-efficacy, and motivation.
Advanced Technology Integration
- Smart technologies and the Internet of Things (IoT): The incorporation of smart pill bottles, digital inhalers, and wearable sensors will provide continuous and objective monitoring of medication-taking behavior and clinical outcomes.
- Artificial Intelligence (AI) and machine learning: AI-powered mobile apps, chatbots, and virtual assistants will provide adaptive, timely reminders, educational content, and supportive counseling. AI will also optimize prescriptions and perform medication reconciliation, thereby reducing errors and improving safety.
System-Level and Collaborative Care Enhancements
- Integrated healthcare systems: The future will involve seamless integration of prescribing, dispensing, and patient-generated data into a unified, self-learning IT system (e.g., electronic health records and personal health portals).
- Multidisciplinary team-based care: Enhanced cooperation among physicians, pharmacists, nurses, and other healthcare professionals will ensure comprehensive patient support. Pharmacists, in particular, will take on a more clinical role in adherence management.
8. Limitations
Despite the above strengths of the review, there are limitations that emanate from the analysis of this review.
- Inaccurate measurement methods;
- The complexity of assessing various facets of adherence;
- Difficulty in capturing the full patient experience;
- Inadequate study populations that do not reflect diverse patient groups;
- Cost and practical challenges of intervention implementation;
- The presence of covert non-adherence (e.g., “white coat adherence”);
- The absence of a universally accepted “gold standard” assessment method.
9. Recommendations
It is recommended that further reviews focus on understanding patient motivations and barriers, tailoring interventions through team-based care and simplification. Furthermore, the review should employ comprehensive adherence assessment methods, like electronic monitoring alongside patient interviews. Strong patient–provider relationships should be developed by empowering patients with clear, personalized education to improve health literacy and address beliefs and concerns, while ensuring that study designs capture the complex interplay of patient-, provider-, and system-level factors.
10. Conclusions
Medication adherence is a critical determinant of healthcare outcomes. It directly impacts disease control, quality of life, and healthcare expenditure. Poor medication adherence leads to progression of the condition, increased treatment complexity, and higher healthcare costs. On the contrary, improved adherence leads to better management of chronic conditions. Strategies to enhance adherence involve a thorough and integrated strategy, including patient education, streamlined treatment strategies, digital tools, and effective communication from healthcare professionals, with pharmacists playing an important role in educating and supporting patients.
Adherence is significantly influenced by patient quality of life, healthcare costs, and clinical outcomes. Addressing barriers to adherence requires a comprehensive and personalized approach that considers individual patient needs and circumstances. To enhance compliance across diverse patient populations, future research should prioritize long-term evaluation of emerging online tools and the development of tailored interventions. Enhancing compliance is not only important for individual patient results but also for optimizing health services.
11. Future Directions
Considering the survey of the literature, to refine compliance with treatment instructions, it is essential to utilize different interventions simultaneously, including both a personalized approach to the system and the patient. An individual approach is extremely critical, taking into account the several determinants affecting patients’ compliance with treatment, involving a personal selection of therapy and taking into account the patient’s financial possibilities, lifestyle, and psychological aspects.
Furthermore, an integrative approach, including collaboration among nurses, pharmacists, and physicians in patient care, can further empower medication compliance. In parallel, wellness initiatives should structure educational plans covering the importance of compliance. These should be directed at healthcare providers, taking into account the need for a personal approach to the patient, as well as patients themselves.
Another direction of change is the application of high-tech solutions, such as monitoring devices or mobile applications, which enable continuous support for patients in complying with treatment. The development of digital tools that include access to educational content, real-time progress monitoring, and medicines reminders may be a breakthrough in improving adherence. These electronic tools should be adjusted to different patient groups, including older people, who may face challenges in applying high-tech equipment. Such innovations have the potential not only to significantly lower healthcare costs, but also to improve treatment results and patients’ quality of life.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Burleson, J.; Stephens, D.E.; Rimal, R.N. Adherence Definitions, Measurement Modalities, and Psychometric Properties in HIV, Diabetes, and Nutritional Supplementation Studies: A Scoping Review. Patient Prefer. Adherence 2025, 19, 319–344. [Google Scholar] [CrossRef]
- Religioni, U.; Barrios-Rodríguez, R.; Requena, P.; Borowska, M.; Ostrowski, J.; Ostrowski, J. Enhancing Therapy Adherence: Impact on Clinical Outcomes, Healthcare Costs, and Patient Quality of Life. Medicina 2025, 61, 153. [Google Scholar] [CrossRef]
- Chauke, D.; Nakwafila, O.; Chibi, B.; Sartorius, B.; Mashamba-Thompson, T. Factors influencing poor medication adherence amongst patients with chronic disease in low-and-middle-income countries: A systematic scoping review. Heliyon 2022, 8, e09716. [Google Scholar] [CrossRef]
- World Health Organisation. Adherence to Long-Term Therapies. Evidence for Action. WHO 2003. Available online: https://iris.who.int/bitstream/handle/10665/42682/9241545992.pdf (accessed on 15 September 2025).
- Mir, T.H. Adherence Versus Compliance. HCA Heal. J. Med. 2023, 4, 219–220. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Unni, E. Medicine Use in Chronic Diseases. Pharmacy 2023, 11, 100. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahmed, K.; Hussein, S.; Qurbani, K.; Ibrahim, R.H.; Fareeq, A.; Mahmood, K.A.; Mohamed, M.G. Antimicrobial resistance: Impacts, challenges, and future prospects. J. Med. Surg. Public Health 2024, 2, 100081. [Google Scholar] [CrossRef]
- Lee, S.Y.; Shanshan, Y.; Lwin, M.O. Are threat perceptions associated with patient adherence to antibiotics? Insights from a survey regarding antibiotics and antimicrobial resistance among the Singapore public. BMC Public Health 2023, 23, 532. [Google Scholar] [CrossRef] [PubMed]
- Vivekanandan, K.E.; Vinoth Kumar, P.V.; Jaysree, R.C.; Rajeshwari, T. Exploring molecular mechanisms of drug resistance in bacteria and progressions in RISPR/Cas9-based genome expurgation solutions. Glob. Med. Genet. 2025, 12, 42. [Google Scholar] [CrossRef]
- Mills, W.R.; Howard, S.; Pitzen, K.; Smitherman, J.; Cole, L.; Wolfram, J.; Deane, W.; Sender, S.; Poltavski, D. A Novel Home-Based Medication Management Program and Its Influence on Hospitalization Rates among Home Health Care Recipients. J. Am. Med. Dir. Assoc. 2024, 25, 155–157. [Google Scholar] [CrossRef]
- Panayi, M.; Charalambous, G.K.; Jelastopulu, E. Enhancing quality of life and medication adherence for people living with HIV: The impact of an information system. J. Patient Rep. Outcomes 2024, 8, 10. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panah, S.; Rathi, N.; Hurley, J.; Sundrud, J.; Lucero, M.; Kamimura, A. Patient Adherence to Health Care Provider Recommendations and Medication among Free Clinic Patients. J. Patient Exp. 2022, 9, 23743735221077523. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Berardinelli, D.; Conti, A.; Hasnaoui, A.; Casabona, E.; Martin, B.; Campagna, S.; Dimonte, V. Nurse-Led Interventions for Improving Medication Adherence in Chronic Diseases: A Systematic Review. Healthcare 2024, 12, 2337. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, Y.; Li, S.; Lu, X.; Chen, W.; Zhang, Y. The Effect of Self-Management on Patients with Chronic Diseases: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 2151. [Google Scholar] [CrossRef] [PubMed]
- Jan, M.; Alenezi, B.T.; Alshygi, S.G.; Eltom, E.; Hamayun, R.; Alanazi, A.K.; Alanazi, A.M.; Alhudhayyiri, M.A.; Alanaz, A.M.M. Assessing the Impact of Compliance and Health Literacy on the Management of Chronic Diseases in the City of Arar, KSA. Glob. J. Med. Pharm. Biomed. Updat. 2025, 20, 8. [Google Scholar] [CrossRef]
- Burnier, M. The role of adherence in patients with chronic diseases. Eur. J. Intern. Med. 2024, 119, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Huang, M.; Miliara, S. Understanding Treatment Adherence in Chronic Diseases: Challenges, Consequences, and Strategies for Improvement. J. Clin. Med. 2025, 14, 6034. [Google Scholar] [CrossRef]
- Pourhabibi, N.; Mohebbi, B.; Sadeghi, R.; Shakibazadeh, E.; Sanjari, M.; Tol, A.; Yaseri, M. Determinants of Poor Treatment Adherence among Patients with Type 2 Diabetes and Limited Health Literacy: A Scoping Review. J. Diabetes Res. 2022, 2022, 2980250. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tariq, R.A.; Vashisht, R.; Sinha, A.; Scherbak, Y. Medication Dispensing Errors and Prevention; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK519065/ (accessed on 8 October 2025).
- Hisan, U.K.; Widjanarko, B.; Sriatmi, A.; Shaluhiyah, Z. Association between depression and medication adherence in noncommunicable diseases: A narrative review. Korean J. Fam. Med. 2025, 46, 231–239. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ngcobo, N.N. Polypharmacy and deprescribing among geriatric patients. Aging Health Res. 2025, 5, 100256. [Google Scholar] [CrossRef]
- Jandu, J.S.; Mohanaselvan, A.; Dahal, R.; Bista, S. Strategies to Reduce Polypharmacy in Older Adults; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK574550 (accessed on 6 October 2025).
- Lustberg, M.B.; Kuderer, N.M.; Desai, A.; Bergerot, C.; Lyman, G.H. Mitigating long-term and delayed adverse events associated with cancer treatment: Implications for survivorship. Nat. Rev. Clin. Oncol. 2023, 20, 527–542. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sharkiya, S.H. Quality communication can improve patient-centred health outcomes among older patients: A rapid review. BMC Heal. Serv. Res. 2023, 23, 886. [Google Scholar] [CrossRef]
- Yenet, A.; Nibret, G.; Tegegne, B.A. Challenges to the Availability and Affordability of Essential Medicines in African Countries: A Scoping Review. Clin. Outcomes Res. 2023, 15, 443–458. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hill-Briggs, F.; Adler, N.E.; Berkowitz, S.A.; Chin, M.H.; Gary-Webb, T.L.; Navas-Acien, A.; Thornton, P.L.; Haire-Joshu, D. Social Determinants of Health and Diabetes: A Scientific Review. Diabetes Care 2020, 44, 258–279. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pribisalić, A.; Popović, R.; Salvatore, F.P.; Vatavuk, M.; Mašanović, M.; Hayward, C.; Polašek, O.; Kolčić, I. The Role of Socioeconomic Status in Adherence to the Mediterranean Diet and Body Mass Index Change: A Follow-Up Study in the General Population of Southern Croatia. Nutrients 2021, 13, 3802. [Google Scholar] [CrossRef]
- Kvarnström, K.; Westerholm, A.; Airaksinen, M.; Liira, H. Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research. Pharmaceutics 2021, 13, 1100. [Google Scholar] [CrossRef] [PubMed]
- Kardas, P. From non-adherence to adherence: Can innovative solutions resolve a longstanding problem? Eur. J. Intern. Med. 2024, 119, 6–12. [Google Scholar] [CrossRef]
- Fragner, T.; Hama, H.; Šerifović, A.; Kirchheiner, K. Patient-centered interprofessional education in cancer care: A systematic scoping review. BMC Med. Educ. 2024, 24, 1552. [Google Scholar] [CrossRef]
- Ricci, L.; Villegente, J.; Loyal, D.; Ayav, C.; Kivits, J.; Rat, A.C. Tailored patient therapeutic educational interventions: A patient-centred communication model. Health Expect. 2022, 25, 276–289. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maniki, P.T.; Chaar, B.B.; Aslani, P. Impact of Interventions on Medication Adherence in Patients With Coexisting Diabetes and Hypertension. Health Expect. 2024, 27, e70010. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.K.; Gidding, S.S.; Santos, R.D.; Libby, P.; Watts, G.F.; Mitchell, N.; Sarkies, M.N. Application of implementation science for improving the utilization of an international clinical practice guidance on familial hypercholesterolemia. J. Clin. Lipidol. 2024, 18, e525–e536. [Google Scholar] [CrossRef]
- Xu, H.Y.; Yu, Y.J.; Zhang, Q.H.; Hu, H.Y.; Li, M. Tailored Interventions to Improve Medication Adherence for Cardiovascular Diseases. Front. Pharmacol. 2020, 13, 510339. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Atolagbe, E.T.; Sivanandy, P.; Ingle, P.V. Effectiveness of educational intervention in improving medication adherence among patients with diabetes in Klang Valley, Malaysia. Front. Clin. Diabetes Health 2023, 4, 1132489. [Google Scholar] [CrossRef]
- Hiligsmann, M.; Gotay, C.; Sankaranarayanan, J.; Lazzaro, C.; Agh, T.; Maas, L.; Yantopoulos, J.; McMinn, R. Expert review of Pharmacoeconomics and outcomes research: High impact articles from 2024. Expert Rev. Pharmacoeconomics Outcomes Res. 2025, 6, 833–835. [Google Scholar] [CrossRef]
- Arnet, I.; Sahm, L.; Gregório, J.; Tuula, A.; Krüger, M.; Wurmbach, V.S.; Hoti, K.; Schulz, M.; Eickhof, C. Development and validation of the 15-STARS-A novel self-report pharmacy-based questionnaire to screen for medication non-adherence. Res. Soc. Adm. Pharm. 2024, 20, 308–320. [Google Scholar] [CrossRef]
- Lu, T.; Lin, Q.; Yu, B.; Hu, J. A systematic review of strategies in digital technologies for motivating adherence to chronic illness self-care. npj Heal. Syst. 2025, 2, 13. [Google Scholar] [CrossRef]
- Mason, M.; Cho, Y.; Rayo, J.; Gong, Y.; Harris, M.; Jiang, Y. Technologies for Medication Adherence Monitoring and Technology Assessment Criteria: Narrative Review. JMIR mHealth uHealth 2022, 10, e35157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ciliberti, R.; Bonsignore, A. New integrations in patient care: The role of the pharmacist between couselling and medication adherence. J. Prev. Med. Hyg. 2025, 66, E38–E44. [Google Scholar] [CrossRef]
- White, A.; Thompson, E.L.; Kim, S.; Osei, J.A.; Fulda, K.G.; Xiao, Y. Enhancing the Role of Community Pharmacists in Medication Safety: A Qualitative Study of Voices from the Frontline. Pharmacy 2025, 13, 94. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schnorrerova, P.; Matalova, P.; Wawruch, M. Medication Adherence and Intervention Strategies: Why Should We Care. Bratisl. Med. J. 2025, 126, 1196–1206. [Google Scholar] [CrossRef]
- Ranjbar, F.; Karimi, M.; Zare, E.; Ghahremani, L. The effect of educational intervention based on the behavioral reasoning theory on self-management behaviors in type 2 diabetes patients: A randomized controlled trial. BMC Public Health 2024, 24, 1761. [Google Scholar] [CrossRef]
- Cheng, C.; Donovan, G.; Al-Jawad, N.; Jalal, Z. The use of technology to improve medication adherence in heart failure patients: A systematic review of randomised controlled trials. J. Pharm. Policy Pract. 2023, 16, 81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Paneerselvam, G.S.; Lua, P.L.; Chooi, W.H.; Rehman, I.U.; Goh, K.W.; Ming, L.C. Effectiveness of Mobile Apps in Improving Medication Adherence Among Chronic Kidney Disease Patients: Systematic Review. J. Med. Internet Res. 2025, 27, e53144. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.H.; Lu, L.J.; Chou, P.C. Preliminary Efficacy of a Gamified Mobile App for Promoting Self-Health Management Among Nurses in the Post-COVID Era: Single-Group Pre-Post Study. JMIR Serious Games 2025, 13, e66262. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okolo, C.A.; Babawarun, O.; Arowoogun, J.O.; Adeniyi, A.O.; Chidi, R. The role of mobile health applications in improving patient engagement and health outcomes: A critical review. Int. J. Sci. Res. Arch. 2024, 11, 2566–2574. [Google Scholar] [CrossRef]
- Ukoaka, B.M.; Ugwuanyi, E.A.; Ukueku, O.U.; Ajah, K.U.; Udam, N.A.; Daniel, F.M.; Wali, T.A.; Gbuchie, M.A. Digital tools for improving antiretroviral adherence among people living with HIV in Africa. J. Med. Surg. Public Health 2024, 2, 100077. [Google Scholar] [CrossRef]
- Bokolo, A.J. Application of telemedicine and eHealth technology for clinical services in response to COVID-19 pandemic. Health Technol. 2021, 11, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Ezenwaji, C.O.; Alum, E.U.; Ugwu, O.P. Bridging the gap: Telemedicine as a solution for HIV care inequities in rural and vulnerable communities. Int. J. Equity Health 2025, 24, 205. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mondesir, F.L.; Levitan, E.B.; Malla, G.; Mukerji, R.; Carson, A.P.; Safford, M.M.; Turan, J.M. Patient Perspectives on Factors Influencing Medication Adherence Among People with Coronary Heart Disease (CHD) and CHD Risk Factors. Patient Prefer. Adherence 2019, 13, 2017–2027. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tian, C.Y.; Wong, E.L.; Qiu, H.; Zhao, S.; Wang, K.; Cheung, A.W.; Yeoh, E. Patient experience and satisfaction with shared decision-making: A cross-sectional study among outpatients. Patient Educ. Couns. 2024, 129, 108410. [Google Scholar] [CrossRef] [PubMed]
- Farhana, L.; Rahayu, F.P.; Sholihah, S.; Sweileh, W.; Abdulah, R.; Alfian, S.D. Effectiveness of Pharmacist-Led Intervention on Medication Adherence in Chronic Diseases: A Systematic Review of Randomized Controlled Trials. Patient Prefer. Adherence 2025, 19, 2161–2178. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Emanuel, E.J.; Gudbranson, E.; Van Parys, J.; Gørtz, M.; Helgeland, J.; Skinner, J. Comparing health outcomes of privileged US citizens with those of average residents of other developed countries. JAMA Intern. Med. 2020, 181, 339–344. [Google Scholar] [CrossRef]
- Kelepouris, E.; Peter, W.S.; Neumiller, J.J.; Wright, E.E. Optimizing Multidisciplinary Care of Patients with Chronic Kidney Disease and Type 2 Diabetes Mellitus. Diabetes Ther. 2023, 14, 1111–1136. [Google Scholar] [CrossRef] [PubMed]
- Heo, M.; Taaffe, K.; Ghadshi, A.; Teague, L.D.; Watts, J.; Lopes, S.S.; Tilkemeier, P.; Litwin, A.H. Effectiveness of Transitional Care Program among High-Risk Discharged Patients: A Quasi-Experimental Study on Saving Costs, Post-Discharge Readmissions and Emergency Department Visits. Int. J. Environ. Res. Public Health 2023, 20, 7136. [Google Scholar] [CrossRef]
- Dodd, R.; Palagyi, A.; Guild, L.; Jha, V.; Jan, S. The impact of out-of-pocket costs on treatment commencement and adherence in chronic kidney disease: A systematic review. Health Policy Plan. 2018, 33, 1047–1054. [Google Scholar] [CrossRef]
- Qiao, Y.; Tsang, C.H.S.; Hohmeier, K.C.; Hines, L.; Chiyaka, E.T.; Wang, J. Association Between Medication Adherence and Healthcare Costs Among Patients Receiving the Low-Income Subsidy. Health Policy Anal. 2020, 23, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.J.F.; Moon, Z.; Horne, R. Medication nonadherence: Health impact, prevalence, correlates and interventions. Psychol. Health 2022, 38, 726–765. [Google Scholar] [CrossRef]
- Oliveira, C.J.; José, H.M.G.; Costa, E.I.M.T.D. Medication Adherence in Adults with Chronic Diseases in Primary Healthcare: A Quality Improvement Project. Nurs. Rep. 2024, 14, 1735–1749. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mackridge, A.J.; Wood, E.M.; Hughes, D.A. Improving medication adherence in the community: A purposive umbrella review of effective patient-directed interventions that are readily implementable in the United Kingdom National Health Service. Int. J. Clin. Pharm. 2025, 47, 640–653. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Merchand, B. Medication Adherence: A Key to Effective Treatment. Int. Res. J. Pharm. Pharmacol. 2023, 11, 1–3. [Google Scholar]
- Kılıç, H.; Güneş, E.D. Patient adherence in healthcare operations: A narrative review. Socio-Econ. Plan. Sci. 2024, 91, 101795. [Google Scholar] [CrossRef]
- Zhang, J.; Hu, J.; Zheng, Y.; Dai, T. Factors affecting medication adherence in patients with chronic diseases: A systematic literature review. Chin. Gen. Pract. J. 2025, 2, 100072. [Google Scholar] [CrossRef]
- Onwusah, D.O.; Ojewole, E.B.; Manyangadze, T.; Chimbari, M.J. Barriers and Facilitators of Adherence to Oral Anticancer Medications Among Women with Breast Cancer: A Qualitative Study. Patient Prefer. Adherence 2023, 17, 2821–2839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Michie, S.; Atkins, L.; West, R. The COM-B Model and the Behavior Change Wheel. Model Basics 2022. Available online: https://www.habitweekly.com/models-frameworks/the-com-b-model (accessed on 16 December 2025).
- Peh, K.Q.E.; Kwan, Y.H.; Goh, H.; Ramchandani, H.; Phang, J.K.; Lim, Z.Y. An Adaptable Framework for Factors Contributing to Medication Adherence: Results from a Systematic Review of 102 Conceptual Frameworks. J. Gen. Intern. Med. 2021, 36, 2784–2795. [Google Scholar] [CrossRef]
- Cai, T.; Verze, P.; Bjerklund Johansen, T.E. The Quality-of-Life Definition: Where Are We Going? Uro 2021, 1, 14–22. [Google Scholar] [CrossRef]
- Respati, A.; Kusumawati, A.; Yulianto, E.; Fahrudi, A.N.L.I. Exploring Determinants and Theoretical Underpinnings of Revisit Intention in Tourism: A PRISMA-Based Systematic Literature Review. Sustainability 2025, 17, 11044. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Maxhakana, Z.; Sithole, M.S. Experiences of Social Workers in Working with Healthcare Practitioners: A Multidisciplinary Team Approach. Social Work/Maatskaplike Werk. A Prof. J. Soc. Work. 2024, 60, 98–122. [Google Scholar]
- Keelson, S.A.; Addo, J.O.; Amoah, J. The impact of patient engagement on service quality and customer well-being: An introspective analysis from the healthcare providers’ perspective. Cogent Public Health 2024, 11, 98–122. [Google Scholar] [CrossRef]
- Shaheen, N.; Shaheen, A.; Ramadan, A.; Hefnawy, M.T.; Ramadan, A.; Ibrahim, I.A.; Hassanein, M.E.; Ashour, M.E.; Flouty, O. Appraising systematic reviews: A comprehensive guide to ensuring validity and reliability. Front. Res. Metr. Anal. 2023, 8, 1268045. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moon, Z.; Walsh, J. Digital interventions in medication adherence: A narrative review of current evidence and challenges. Front. Pharmacol. 2025, 16, 1632474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the author. Published by MDPI on behalf of the JMMS. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.