
Elaboration and Analysis of SARS-CoV-2 Data in the Frame of Occupational Safety and Health Assessment in Sustainable Engineering Systems



Abstract
1. Introduction
2. Materials and Methods
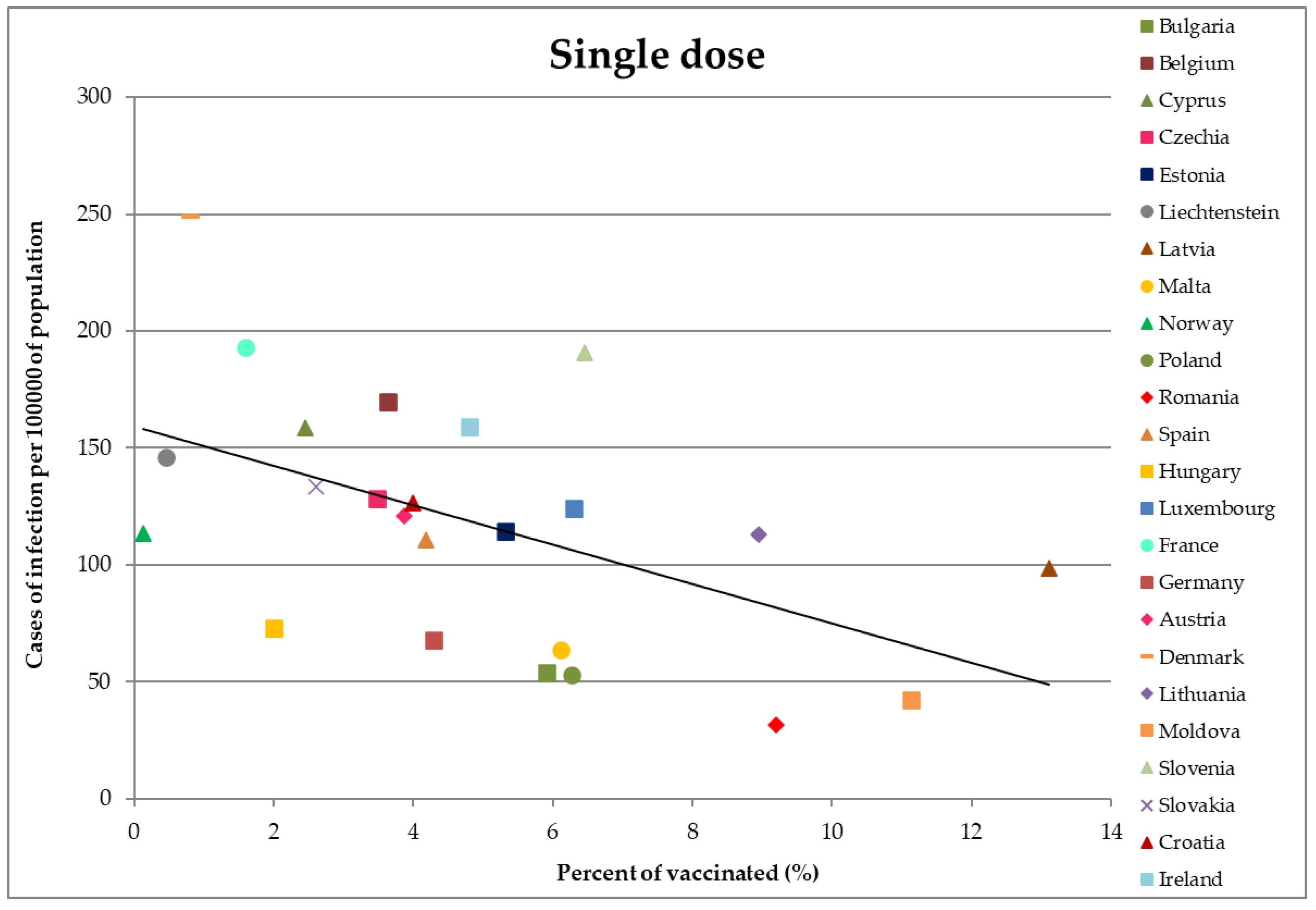
- Vaccinated with one dose of the single dose vaccine program,
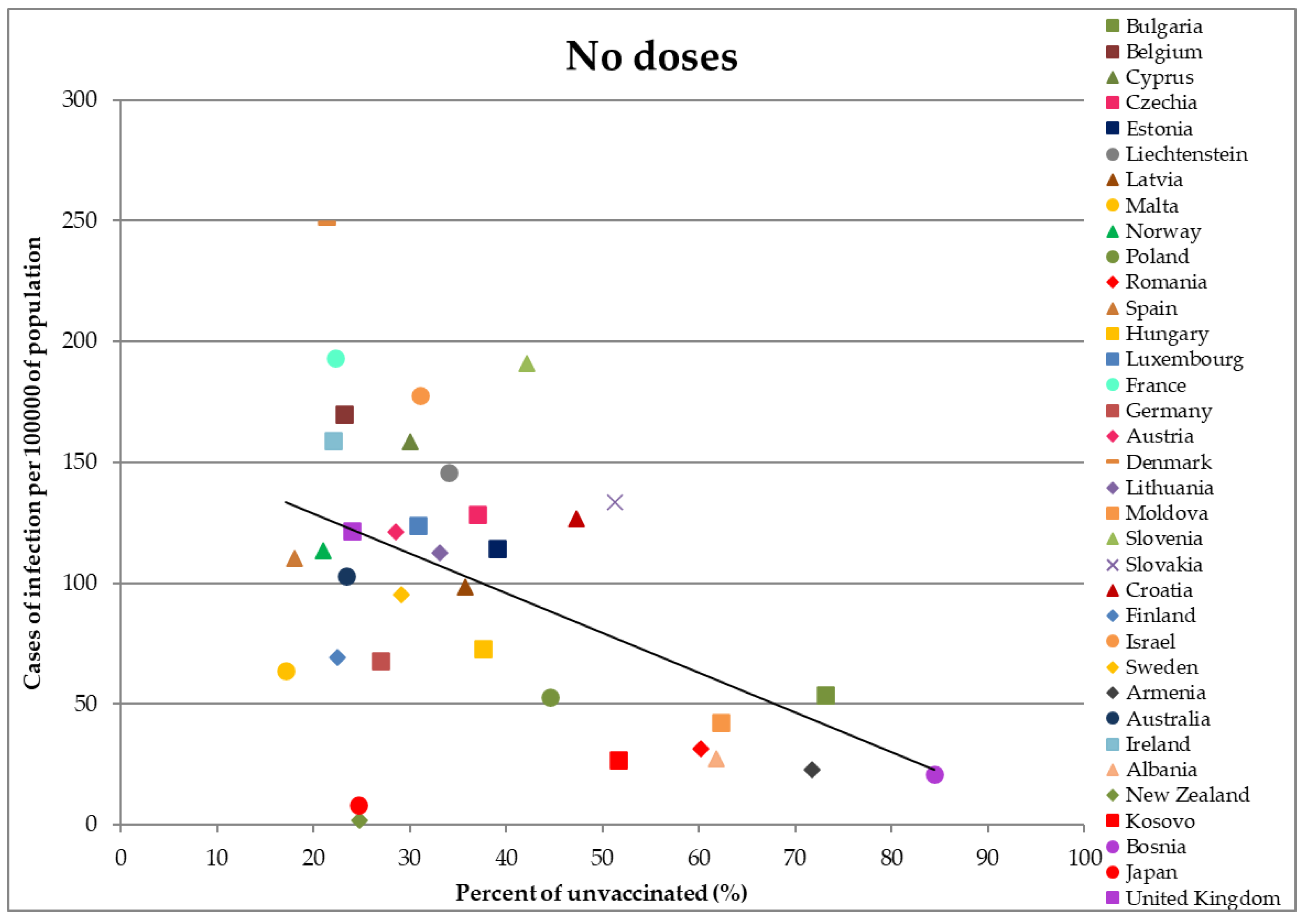
- Not vaccinated,
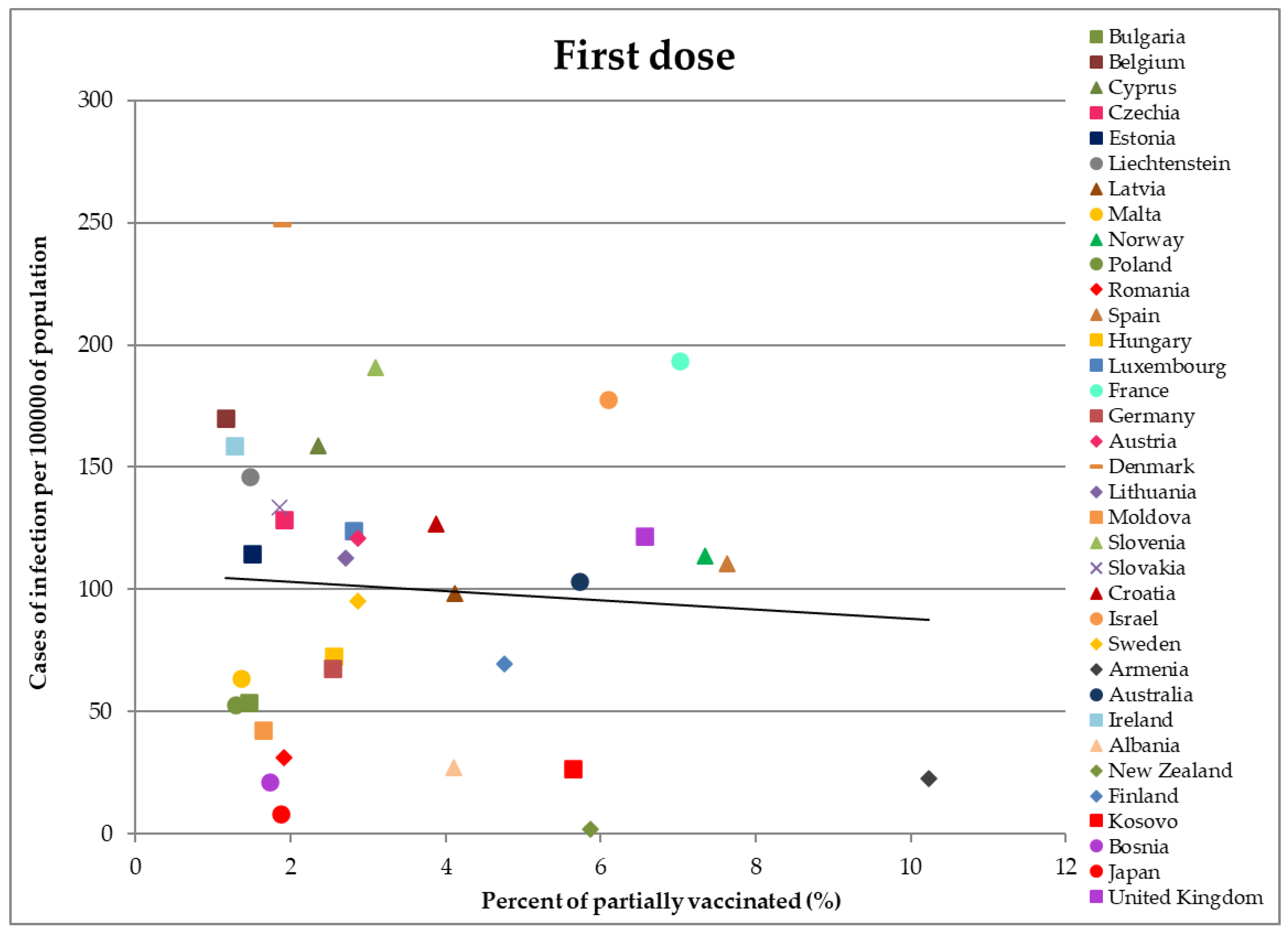
- Vaccinated with the first dose of a two-dose vaccination program,
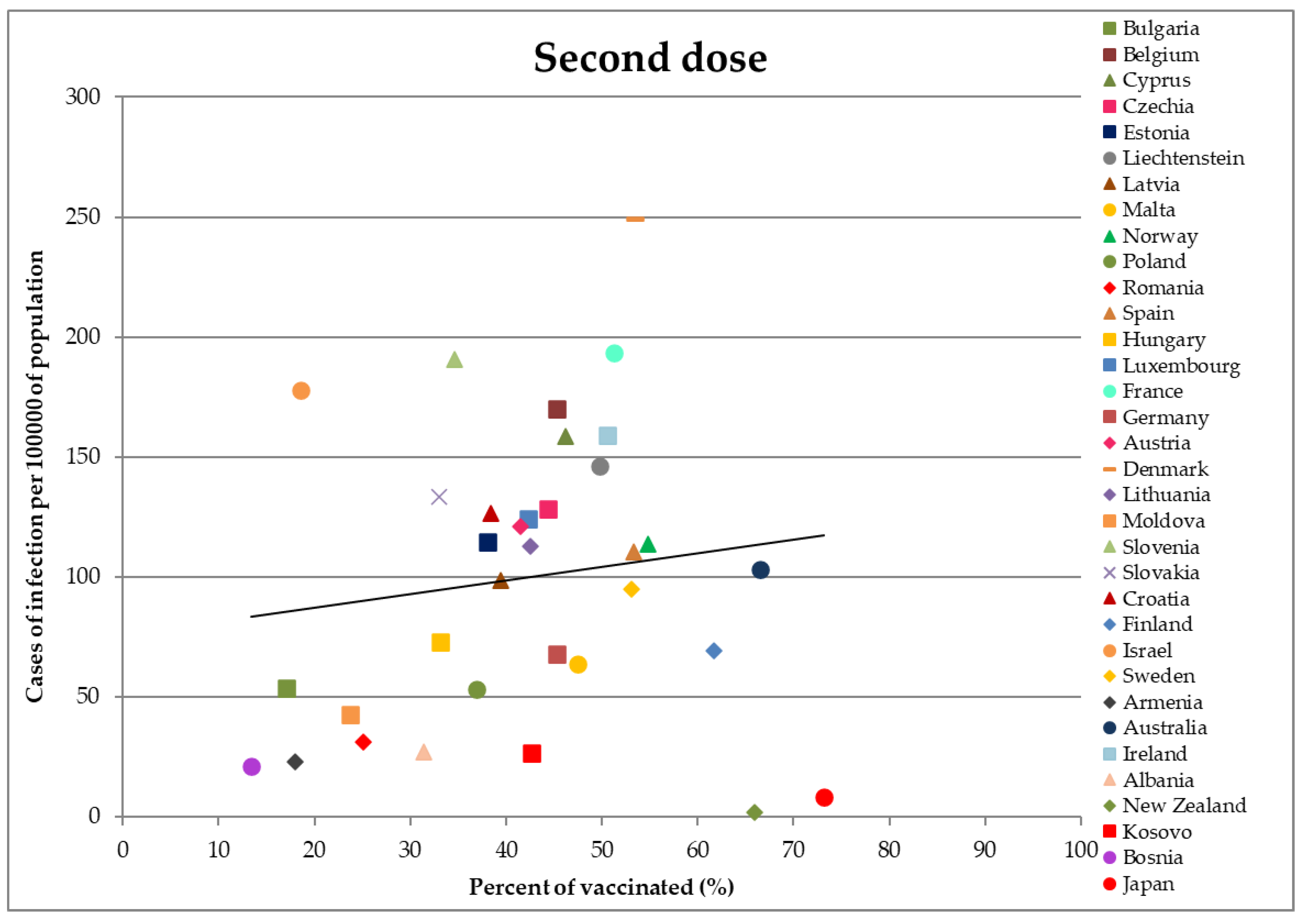
- Vaccinated with two doses,
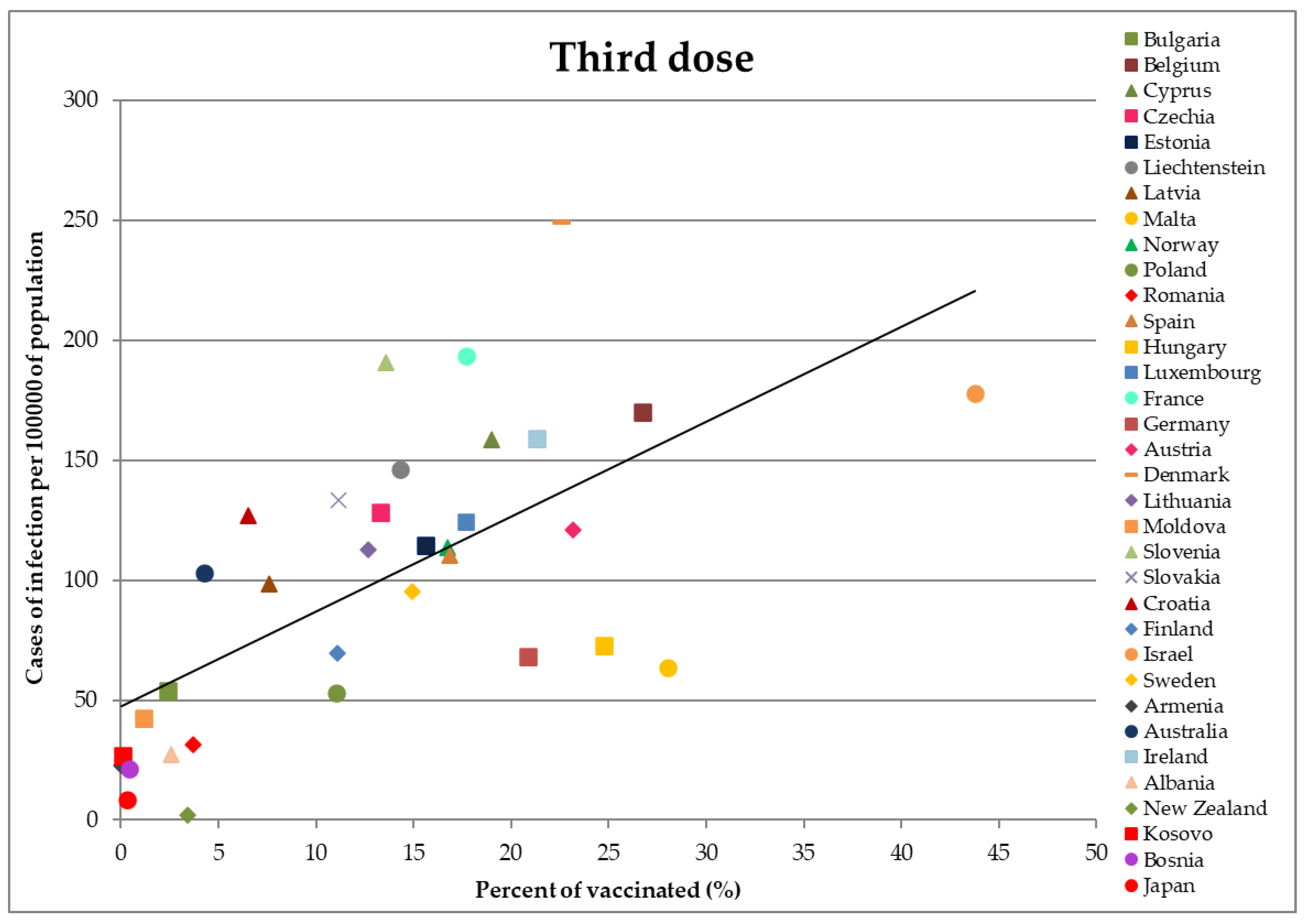
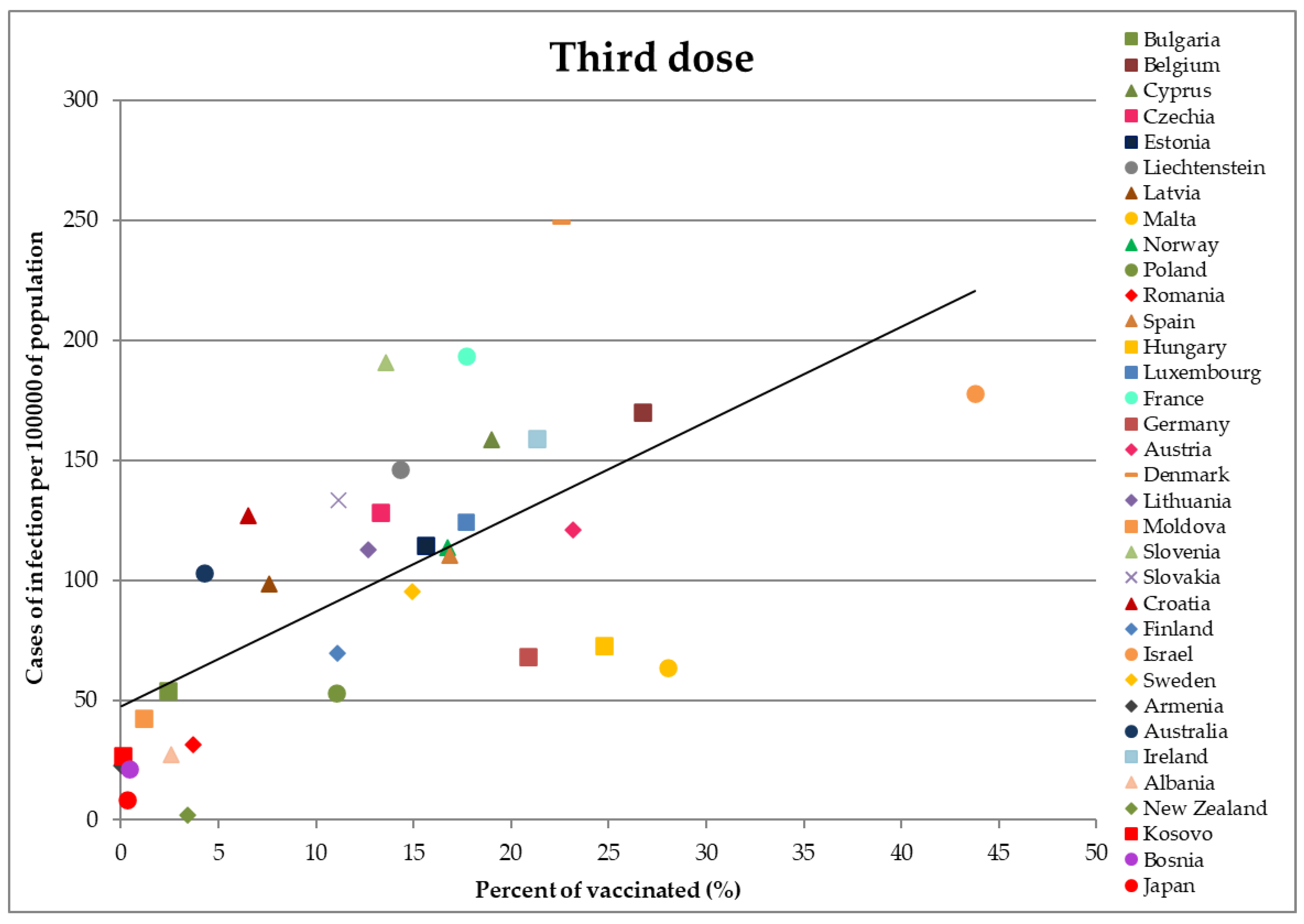
- Vaccinated with three doses,
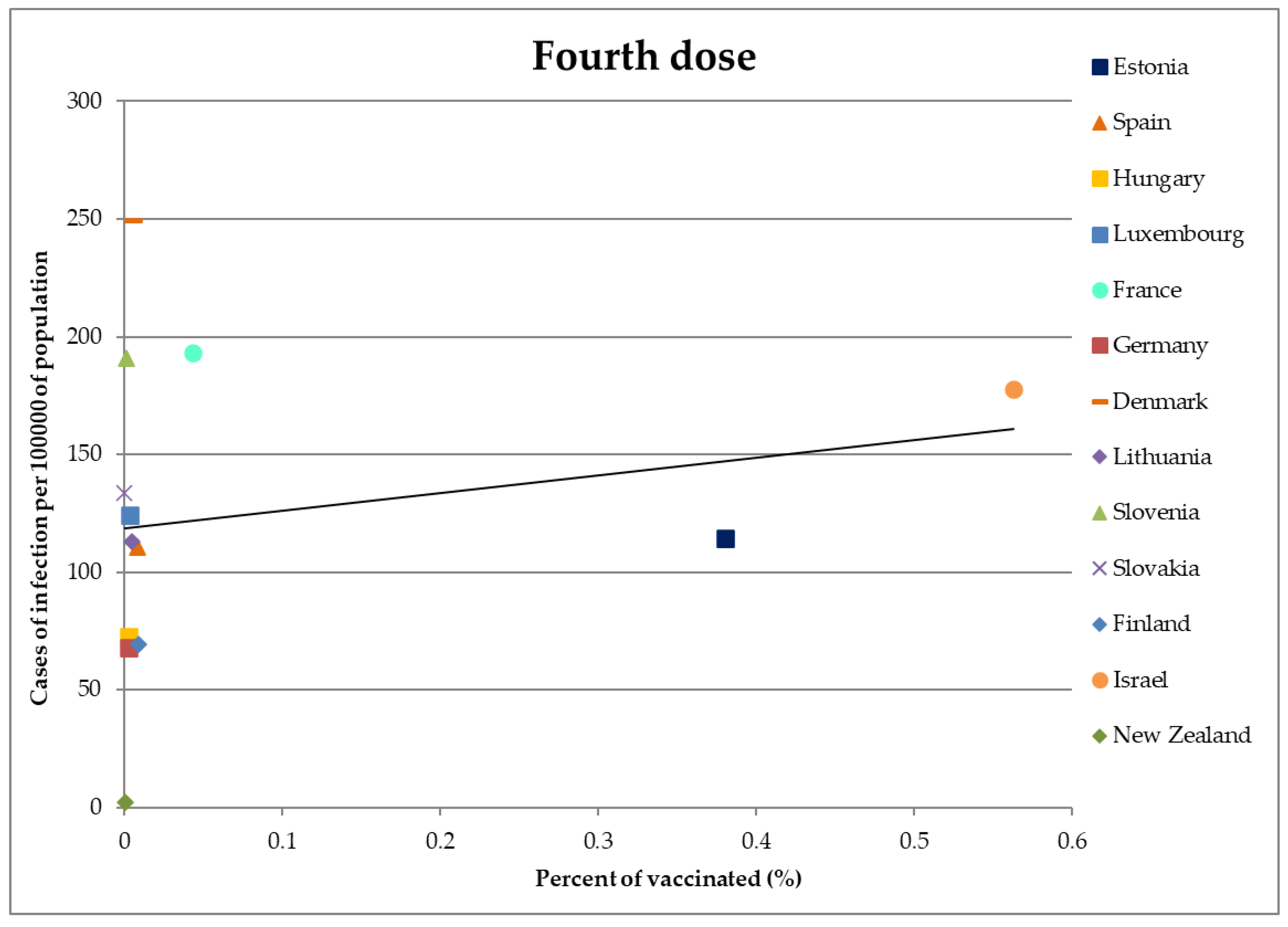
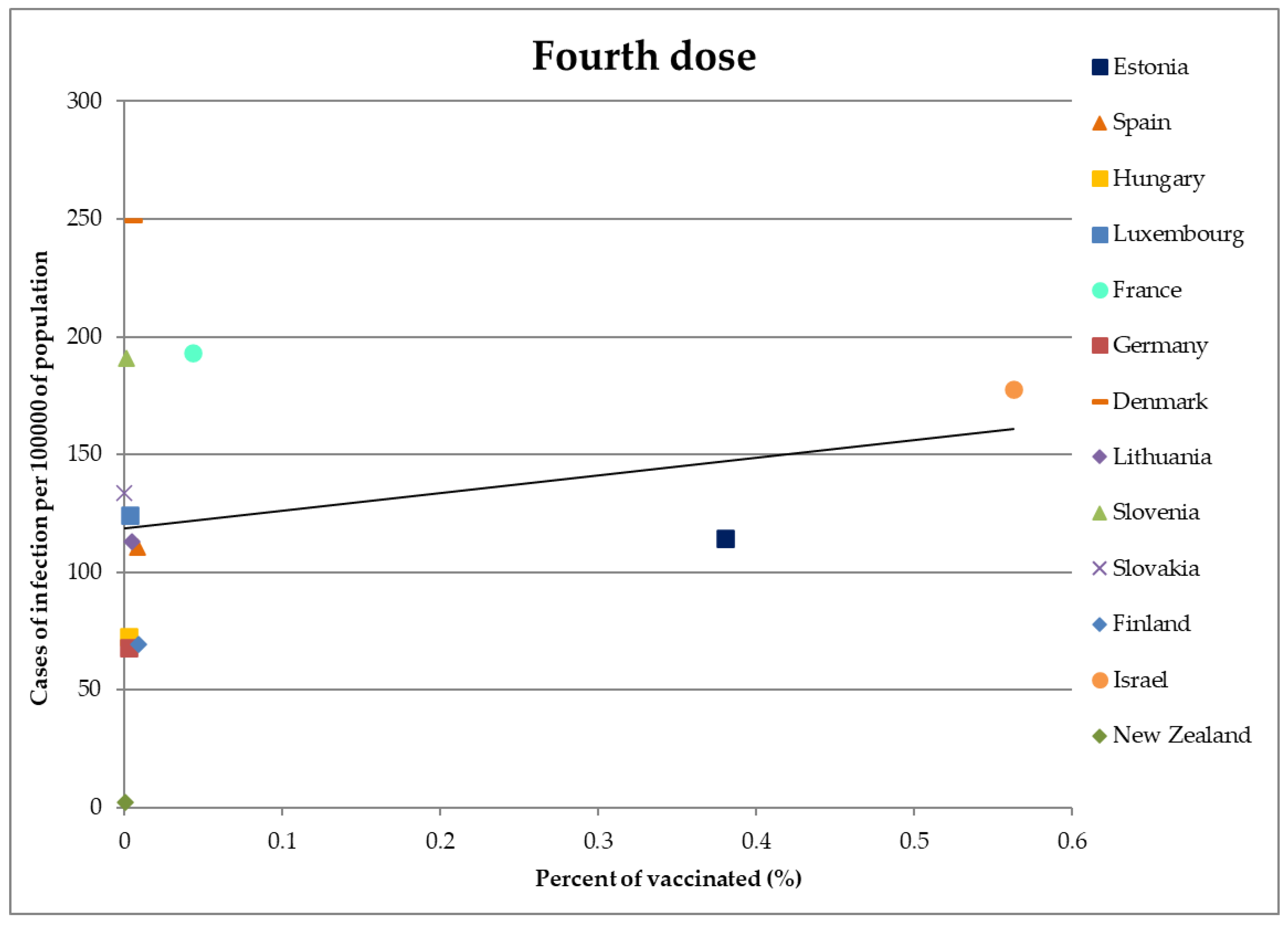
- Vaccinated with four doses.
3. Results
4. Discussion
4.1. Discussion of the Results and Interpretation
4.2. Limitations
4.3. Future Research Directions
5. Conclusions
- Indications that vaccination could not stop vaccinated individuals from transmitting the virus should not be disregarded.
- It was crucial to control the pandemic through workplaces, since humans spend almost half of their waking day working and they have a greater chance of getting infected in the workplace.
- Ignoring the possibility of both parties (vaccinated and non-vaccinated employees) transmitting the virus to the work environment, segregation measures and restrictions taken to divide workers by their vaccination status were unjust and inefficient.
- From the OSH point of view, such behavior posed a threat and a workplace risk, as vaccinated workers were not obligated to be tested and they entered the workplace with an unknown and possibly dangerous health condition.
- The absolute privilege of vaccinated employees to enter their workplaces without mandatory COVID-19 testing intensified the virus transmission, escalated occupational risk, downgraded the safety level at the worksites of sustainable engineering systems, and amplified the OSH risk management difficulties.
- Failure to establish efficient OSH policies to protect workers from the virus endangered their health and well-being, their financial status, and their social life.
- The financial charge of compulsory unemployment and repeated COVID-19 testing was not justified and economically viable for unvaccinated people in the midst of a worldwide economic crisis.
- Τhe topic is very complex and it is necessary to be very cautious in interpreting the observations made from the graphs.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/docs/default-source/coronaviruse/getting-workplace-ready-for-covid-19.pdf (accessed on 17 July 2023).
- World Health Organization. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Adjusting_PH_measures-Workplaces-2020.1 (accessed on 17 July 2023).
- Occupational Health and Safety Administration (OSHA). Available online: https://www.osha.gov/sites/default/files/publications/OSHA3990.pdf (accessed on 17 July 2023).
- International Labour Organization (ILO). Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_norm/---normes/documents/genericdocument/wcms_739937.pdf (accessed on 17 July 2023).
- European Agency for Safety and Health at Work (EU-OSHA). Available online: https://oshwiki.osha.europa.eu/en/themes/covid-19-back-workplace-adapting-workplaces-and-protecting-workers (accessed on 17 July 2023).
- European Parliament. Directive 2000/54/EC of the European Parliament and of the Council of 18 September 2000 on the protection of workers from risks related to exposure to biological agents at work (seventh individual directive within the meaning of Article 16(1) of Directive 89/391/EEC). Off. J. Eur. Commun. 2000, L262/2. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32000L0054 (accessed on 17 July 2023).
- European Parliament. Commission Directive (EU) 2020/739 of 3 June 2020 amending Annex III to Directive 2000/54/EC of the European Parliament and of the Council as regards the inclusion of SARS-CoV-2 in the list of biological agents known to infect humans and amending Commission Directive (EU) 2019/1833. Off. J. Eur. Union 2020, L175/11. Available online: https://eur-lex.europa.eu/eli/dir/2020/739/oj (accessed on 18 July 2023).
- Melnick, J.P.; Ioannidis, E.R. Should governments continue lockdown to slow the spread of COVID-19. BMJ 2020, 369, m1924. [Google Scholar] [CrossRef]
- Atalan, A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and economy-perspective. Ann. Med. Surg. 2020, 56, 38–42. [Google Scholar] [CrossRef]
- Moser, D.A.; Glaus, J.; Frangou, S.; Schechter, D.S. Years of life lost due to the psychosocial consequences of COVID-19 mitigation strategies based on Swiss data. Eur. Psychiatry 2020, 63, e58. [Google Scholar] [CrossRef]
- European Parliament. Regulation (EU) 2021/953 of the European Parliament and of the Council of 14 June 2021 on a framework for the issuance, verification and acceptance of interoperable COVID-19 vaccination, test and recovery certificates (EU Digital COVID Certificate) to facilitate free movement during the COVID-19 pandemic (Text with EEA relevance). Off. J. Eur. Union 2021, L211/1. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32021R0953 (accessed on 25 July 2023).
- Austria Passes Covid Vaccine Mandate, but Question Marks Linger over Enforcement. Available online: https://www.theguardian.com/world/2022/feb/04/austria-passes-covid-vaccine-mandate-but-question-marks-linger-over-enforcement (accessed on 10 August 2023).
- Hellenic Government. Definition of the procedure for determining principals and imposition of administrative pecuniary penalty in paragraph 4 of Article 24 of Law 4865/2021 (A’ 238). Off. Gaz. Hell. Repub. 2022, B’608. Available online: https://www.et.gr/api/DownloadFeksApi/?fek_pdf=20220200608 (accessed on 10 August 2023). (In Greek).
- Oglesby, K. Unvaccinated to Take Daily Covid Test to Enter Workplace. Available online: https://www.luxtimes.lu/luxembourg/unvaccinated-to-take-daily-covid-test-to-enter-workplace/1335640.html (accessed on 19 March 2023).
- Douglas, E. COVID: New Restrictions for Germany’s Unvaccinated. Available online: https://www.dw.com/en/covid-new-rules-for-the-unvaccinated-in-germany/a-59261647 (accessed on 19 March 2023).
- Lee, J.; Jackson, M. COVID-19: Vaccines to be Compulsory for Frontline NHS Staff in England. Available online: https://www.bbc.com/news/health-59215282 (accessed on 19 March 2023).
- Trois Milles oignants suspendus: L’estimation «Parcellaire» d’Olivier Véran. Available online: https://www.lemonde.fr/les-decodeurs/article/2021/09/20/3-000-soignants-suspendus-l-estimation-parcellaire-d-olivier-veran_6095356_4355770.html (accessed on 19 March 2023).
- Garamone, J. Service Members Must Be Vaccinated or Face Consequences, DOD Official Says. Available online: https://www.defense.gov/News/News-Stories%20/Article/Article/2881481%20/service-members-must-be-vaccinated-or-face-consequences-dod-official-says/ (accessed on 19 March 2023).
- Oliu-Barton, M.; Pradelski, B.S.R.; Woloszko, N.; Guetta-Jeanrenaud, L.; Aghion, P.; Artus, P.; Fontanet, A.; Martin, P.; Wolff, G.B. The effect of COVID certificates on vaccine uptake, health outcomes, and the economy. Nat. Commun. 2022, 13, 3942. [Google Scholar] [CrossRef]
- Mills, M.C.; Rüttenauer, T. The effect of mandatory COVID-19 certificates on vaccine uptake: Synthetic-control modelling of six countries. Lancet Public Health 2022, 7, e15–e22. [Google Scholar] [CrossRef]
- Karaivanov, A.; Kim, D.; Lu, S.E.; Shigeoka, H. COVID-19 vaccination mandates and vaccine uptake. Na.t Hum. Behav. 2022, 6, 1615–1624. [Google Scholar] [CrossRef]
- Butler Harrington, L.M. Sustainability Theory and Conceptual Considerations: A Review of Key Ideas for Sustainability, and the Rural Context. Pap. Appl. Geogr. 2016, 2, 365–382. [Google Scholar] [CrossRef]
- Purvis, B.; Mao, Y.; Robinson, D. Three pillars of sustainability: In search of conceptual origins. Sustain. Sci. 2019, 14, 681–695. [Google Scholar] [CrossRef]
- Fernandes, N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy; IESE Business School Working Paper No. WP-1240-E; Rochester: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Feyisa, H.L. The World Economy at COVID-19 Quarantine: Contemporary Review. Int. J. Econ. Financ. Manag. Sci. 2020, 8, 63–74. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Kalogiannidis, S.; Chatzitheodoridis, F.; Kontsas, S. An Eclectic Discussion of the Effects of COVID-19 Pandemic on the World Economy During the First Stage of the Spread. Int. J. Financ. Res. 2020, 11, 137–153. [Google Scholar] [CrossRef]
- Mou, J. Research on the Impact of COVID-19 on Global Economy. IOP Conf. Ser. Earth Environ. Sci. 2020, 546, 032043. [Google Scholar] [CrossRef]
- Reis, C.; Oliveira, C.; Braga, P.; Silva, J.F.; Silva, L.T. Occupational Health and Safety-Sustainable Development and the Changes in Organizations. In Occupational and Environmental Safety and Health II, 1st ed.; Arezes, P.M., Ed.; Studies in Systems, Decision and Control; Springer Nature Switzerland AG: Cham, Switzerland, 2020; Volume 277, pp. 677–687. [Google Scholar] [CrossRef]
- Jilcha, K.; Kitaw, D. Industrial occupational safety and health innovation for sustainable development. Eng. Sci. Technol. Int. J. 2016, 20, 372–380. [Google Scholar] [CrossRef]
- Kavouras, S.; Vardopoulos, I.; Mitoula, R.; Zorpas, A.A.; Kaldis, P. Occupational Health and Safety Scope Significance in Achieving Sustainability. Sustainability 2022, 14, 2424. [Google Scholar] [CrossRef]
- Johanson, U.; Aboagye, E.; Yao, J. Integrating business model for sustainability and performance management to promote occupational health and safety—A discussion of value. Front. Sustain. 2022, 3, 950847. [Google Scholar] [CrossRef]
- Cutler, D.M.; Summers, L.H. The COVID-19 Pandemic and the $16 Trillion Virus. JAMA 2020, 324, 1495–1496. [Google Scholar] [CrossRef]
- Murphy, Κ. The social pillar of sustainable development: A literature review and framework for policy analysis. Sustain. Sci. Pract. Policy 2012, 8, 15–29. [Google Scholar] [CrossRef]
- Magnavita, N.; Soave, P.M.; Antonelli, M. Treating Anti-Vax Patients, a New Occupational Stressor—Data from the 4th Wave of the Prospective Study of Intensivists and COVID-19 (PSIC). Int. J. Environ. Res. Public Health 2022, 19, 5889. [Google Scholar] [CrossRef]
- Subramanian, S.V.; Kumar, A. Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States. Eur. J. Epidemiol. 2021, 36, 1237–1240. [Google Scholar] [CrossRef]
- Muttappallymyalil, J.; ChandrasekharNair, S.; Changerath, R.; Sreejith, A.; Manda, S.; Sreedharan, J. Vaccination Rate and Incidence of COVID-19 and Case Fatality Rate (CFR): A Correlational Study Using Data from 2019 to 2021. Cureus 2022, 14, e28210. [Google Scholar] [CrossRef]
- Greiner, A.; Owusu, B. Effects of the vaccination against SARS-CoV-2 on infections and on hospitalizations in European countries. SN Bus. Econ. 2023, 3, 67. [Google Scholar] [CrossRef]
- Kampf, G. The epidemiological relevance of the COVID-19-vaccinated population is increasing. Lancet Reg. Health Eur. 2021, 11, 100272. [Google Scholar] [CrossRef]
- Brown, C.M.; Vostok, J.; Johnson, H.; Burns, M.; Gharpure, R.; Sami, S.; Sabo, R.T.; Hall, N.; Foreman, A.; Schubert, P.L.; et al. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings—Barnstable County, Massachusetts, July 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1059–1062. [Google Scholar] [CrossRef]
- Ko, L.; Malet, G.; Chang, L.L.; Nguyen, H.; Mayes, R. COVID-19 Infection Rates in Vaccinated and Unvaccinated Inmates: A Retrospective Cohort Study. Cureus 2023, 15, e44684. [Google Scholar] [CrossRef]
- Salvatore, P.P.; Lee, C.C.; Sleweon, S.; McCormick, D.W.; Nicolae, L.; Knipe, K.; Dixon, T.; Banta, R.; Ogle, I.; Young, C.; et al. Transmission potential of vaccinated and unvaccinated persons infected with the SARS-CoV-2 Delta variant in a federal prison. Vaccine 2023, 41, 1808–1818. [Google Scholar] [CrossRef]
- Singanayagam, A.; Hakki, S.; Dunning, J.; Madon, K.J.; Crone, M.A.; Koycheva, A.; Derqui-Fernandez, N.; Barnett, J.L.; Whitfield, M.G.; Varro, R.; et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. Lancet Infect Dis. 2022, 22, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Mavridis, C.; Aidonidis, G.; Evangelou, M.; Kalogeridis, A. Mandatory vaccinations, the segregation of citizens, and the promotion of inequality in the modern democracy of Greece and other democratic countries in the era of COVID-19. Hist. Philos. Life Sci. 2022, 44, 72. [Google Scholar] [CrossRef]
- Bardosh, K.; de Figueiredo, A.; Gur-Arie, R.; Jamrozik, E.; Doidge, J.; Lemmens, T.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Glob. Health 2022, 7, e008684. [Google Scholar] [CrossRef]
- Voo, T.C.; Savulescu, J.; Schaefer, O.; Ling, A.H.Z.; Tam, C.C. COVID-19 differentiated measures for unvaccinated individuals: The need for clear goals and strong justifications. Vaccine 2022, 40, 5333–5337. [Google Scholar] [CrossRef]
- Agba, A.M.O.; Ocheni, S.I.; Agba, M.S. COVID-19 and the World of Work Dynamics: A Critical Review. JESR 2020, 10, 119–130. [Google Scholar] [CrossRef]
- Dehghani, F.; Omidi, F.; Yousefinejad, S.; Taheri, E. The hierarchy of preventive measures to protect workers against the COVID-19 pandemic: A review. Work 2020, 67, 771–777. [Google Scholar] [CrossRef]
- Ingram, C.; Downey, V.; Roe, M.; Chen, Y.; Archibald, M.; Kallas, K.A.; Kumar, J.; Naughton, P.; Uteh, C.O.; Rojas-Chaves, A.; et al. COVID-19 Prevention and Control Measures in Workplace Settings: A Rapid Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7847. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus (accessed on 21 August 2022).
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/publications-data/download-historical-data-20-june-2022-weekly-number-new-reported-covid-19-cases (accessed on 19 July 2022).
- UK Health Security Agency. Available online: https://coronavirus.data.gov.uk/details/vaccinations?areaType=overview&areaName=United%20Kingdom (accessed on 19 July 2022).
- Prime Minister’s Office of Japan. Available online: https://www.kantei.go.jp/jp/headline/kansensho/vaccine.html (accessed on 13 August 2022).
- Institute for Public Health FB&H. Available online: https://www.zzjzfbih.ba/pregled-epidemioloske-situacije-covid-19/ (accessed on 8 December 2022).
- Ministry of Health of Albania. Available online: https://shendetesia.gov.al/ (accessed on 19 August 2022).
- Government of Ireland. Available online: https://covid-19.geohive.ie/search (accessed on 20 November 2022).
- Ministry of Health of Armenia. Available online: https://www.moh.am/#1/News (accessed on 19 August 2022).
- Government of the Republic of Croatia. Available online: https://www.koronavirus.hr/o-cijepljenju/dnevna-izvjesca-o-cijepljenju/953 (accessed on 20 August 2022).
- Public Health France. Available online: https://www.data.gouv.fr/fr/datasets/donnees-relatives-aux-personnes-vaccinees-contre-la-covid-19-1/ (accessed on 18 August 2022).
- Ministry of Health of Israel. Available online: https://datadashboard.health.gov.il/portal/dashboard/corona (accessed on 14 August 2022).
- Ministry of Health of Austria. Available online: https://impfdaten.at/ (accessed on 13 August 2022).
- Robert Koch Institute and Federal Ministry of Health of Germany. Available online: https://impfdashboard.de/daten (accessed on 13 August 2022).
- Statens Serum Institut. Available online: https://covid19.ssi.dk/overvagningsdata%20/download-fil-med-vaccinationsdata (accessed on 13 August 2022).
- Finnish Institute for Health and Welfare. Available online: https://sampo.thl.fi/pivot/prod/en/vaccreg/cov19cov/fact_cov19cov?column=measure-533185.533172.433796.533175&row=cov_vac_dose-533174L (accessed on 16 October 2022).
- Government of the Republic of Moldova. Available online: https://vaccinare.gov.md/rapoarte-saptaminale (accessed on 18 August 2022).
- Ministry of Health of New Zealand. Available online: https://www.health.govt.nz/covid-19-novel-coronavirus/covid-19-data-and-statistics/covid-19-vaccine-data (accessed on 17 August 2022).
- National Institute for Public Health of Slovenia. Available online: https://app.powerbi.com/view?r=eyJrIjoiYWQ3NGE1NTMtZWJkMi00NzZmLWFiNDItZDc5YjU5MGRkOGMyIiwidCI6ImFkMjQ1ZGFlLTQ0YTAtNGQ5NC04OTY3LTVjNjk5MGFmYTQ2MyIsImMiOjl9 (accessed on 15 October 2022).
- Statistics Lithuania State Data Agency. Available online: https://experience.arcgis.com/experience/cab84dcfe0464c2a8050a78f817924ca/page/Atviri-duomenys/ (accessed on 9 October 2022).
- Department of Health and Aged Care of the Government of Australia. Available online: https://www.health.gov.au/resources/collections/covid-19-vaccination-rollout-update (accessed on 19 August 2022).
- Covid Base AU. Available online: https://covidbaseau.com/vaccinations/ (accessed on 19 August 2022).
- Ministry of Health of the Republic of Kosovo. Available online: https://www.facebook.com/Ministria.Shendetesise.RKS (accessed on 1 November 2022).
- European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/publications-data/data-covid-19-vaccination-eu-eea (accessed on 9 December 2022).
- Centers for Disease Control and Prevention. CDC Real-World Study Confirms Protective Benefits of mRNA COVID-19 Vaccines. Available online: https://www.cdc.gov/media/releases/2021/p0329-COVID-19-Vaccines.html (accessed on 29 August 2023).
- UK Government. Available online: https://www.gov.uk/government/news/react-study-shows-fully-vaccinated-are-three-times-less-likely-to-be-infected (accessed on 29 August 2023).
- European Centre for Disease and Control. Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-report-examines-sars-cov-2-transmission-risk-vaccinated-previously-infected-individuals (accessed on 29 August 2023).
- After More than 500 Days, Denmark Has Ended Its COVID Restrictions. Available online: https://www.npr.org/2021/09/10/1036136246/covid-denmark-eu-restrictions (accessed on 31 August 2023).
- Denmark Proposes Corona Pass Mandate for Workers. Available online: https://www.reuters.com/world/europe/denmark-proposes-corona-pass-mandate-workers-2021-11-12/ (accessed on 31 August 2023).
- Where France’s COVID-19 ‘Health Pass’ Is Now Mandatory. Available online: https://www.france24.com/en/france/20210802-france-s-covid-19-health-pass-where-it-is-mandatory-and-what-will-change-on-august-9 (accessed on 7 September 2023).
- France Suspends 3,000 Unvaccinated Health Workers without Pay. Available online: https://www.theguardian.com/world/2021/sep/16/france-suspends-3000-unvaccinated-health-workers-without-pay-covid-jab (accessed on 31 August 2023).
- Lytras, T.; Tsiodras, S. Total patient load, regional disparities and in-hospital mortality of intubated COVID-19 patients in Greece, from September 2020 to May 2021. Scand. J. Public Health 2022, 50, 671–675. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Cases per Capita | Vaccination Coverage (%) |
|---|---|---|
| Portugal | 162.46 | 82.86 |
| Iceland | 151.32 | 76.37 |
| Netherlands | 144.26 | 67.65 |
| Greece | 124.02 | 65.47 |
| Italy | 114.15 | 75.13 |
| Serbia | 78.27 | 45.62 |
| Lebanon | 53.62 | 31.58 |
| Jordan | 34.16 | 33.59 |
| Belarus | 16.16 | 33.63 |
| Azerbaijan | 13.31 | 44.79 |
| Vaccination Status | Correlation Coefficient | R-Squared |
|---|---|---|
| Single dose | −0.519 | 0.269 |
| No doses | −0.479 | 0.230 |
| First dose | −0.074 | 0.005 |
| Second dose | 0.135 | 0.018 |
| Third dose | 0.652 | 0.425 |
| Fourth dose | 0.205 | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tatli, S.F.; Marhavilas, P.K. Elaboration and Analysis of SARS-CoV-2 Data in the Frame of Occupational Safety and Health Assessment in Sustainable Engineering Systems. Safety 2024, 10, 6. https://doi.org/10.3390/safety10010006
Tatli SF, Marhavilas PK. Elaboration and Analysis of SARS-CoV-2 Data in the Frame of Occupational Safety and Health Assessment in Sustainable Engineering Systems. Safety. 2024; 10(1):6. https://doi.org/10.3390/safety10010006
Chicago/Turabian StyleTatli, Stefania F., and Panagiotis K. Marhavilas. 2024. "Elaboration and Analysis of SARS-CoV-2 Data in the Frame of Occupational Safety and Health Assessment in Sustainable Engineering Systems" Safety 10, no. 1: 6. https://doi.org/10.3390/safety10010006
APA StyleTatli, S. F., & Marhavilas, P. K. (2024). Elaboration and Analysis of SARS-CoV-2 Data in the Frame of Occupational Safety and Health Assessment in Sustainable Engineering Systems. Safety, 10(1), 6. https://doi.org/10.3390/safety10010006