
Autonomic Responses during Labor: Potential Implications for Takotsubo Syndrome

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
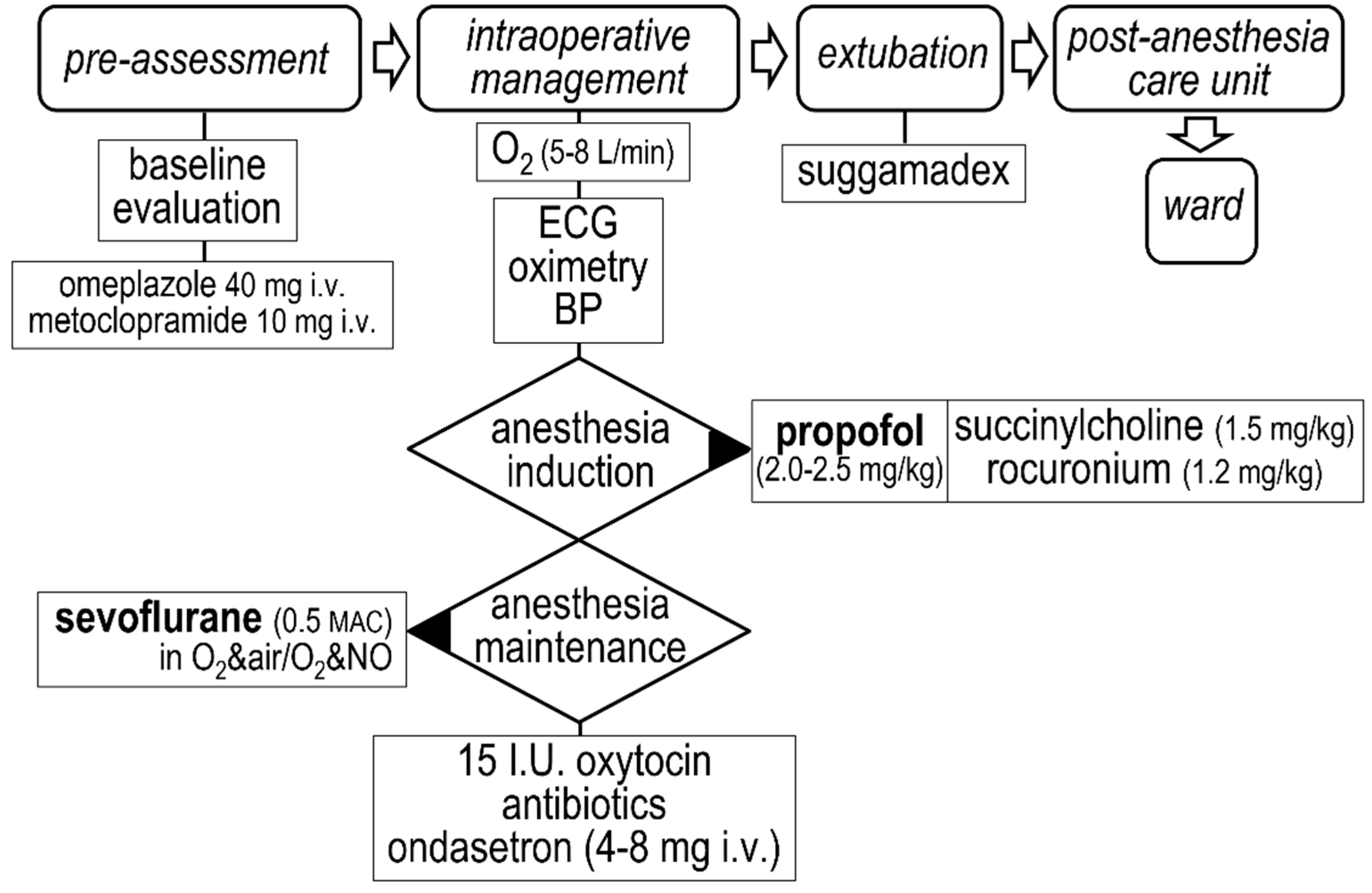
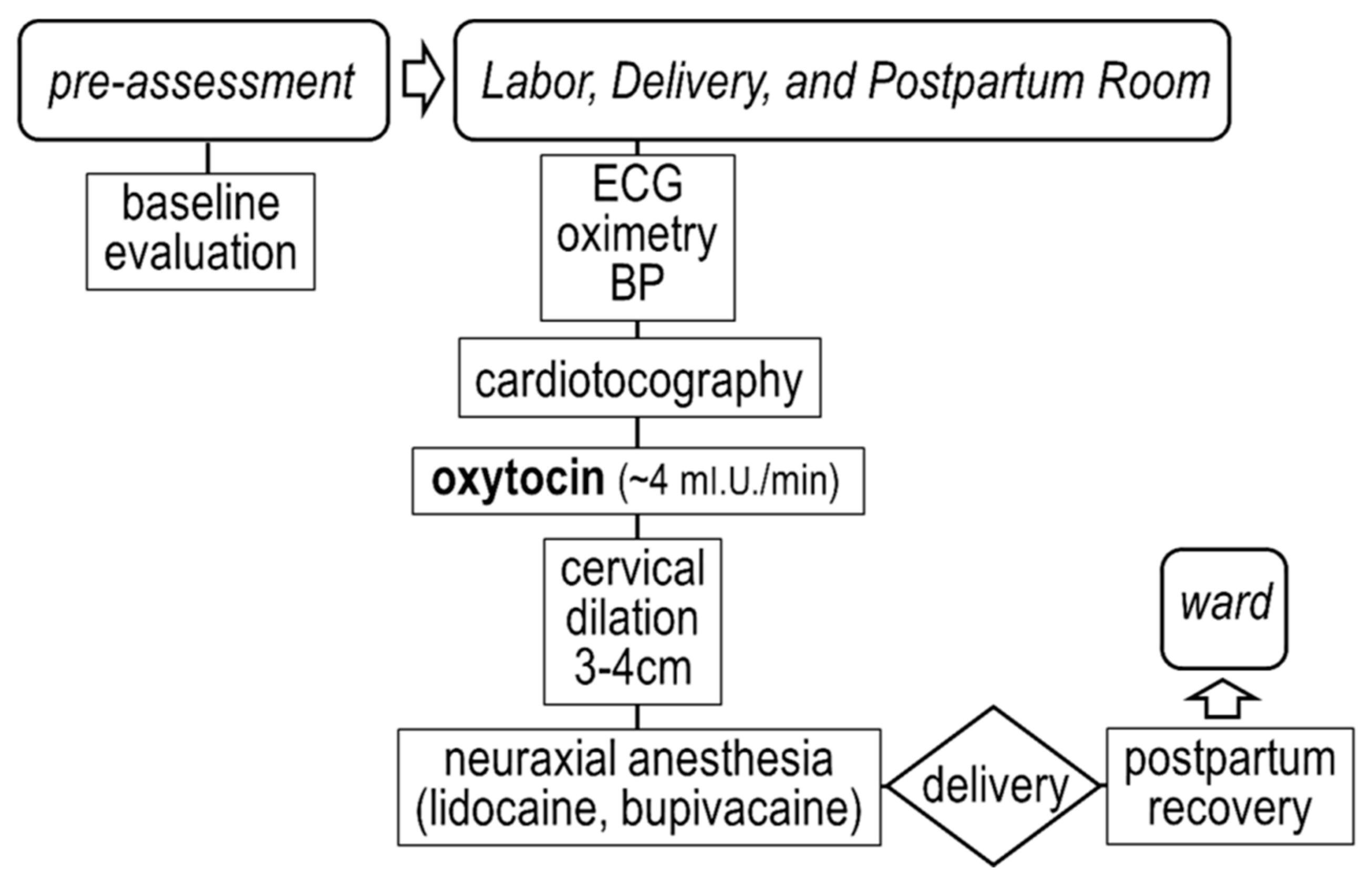
2.2. Delivery
2.3. Observation Time-Points
2.4. Heart Rate Variability Analysis
2.5. Assessment of Sympathetic and Vagal Activity
2.6. Statistics
3. Results
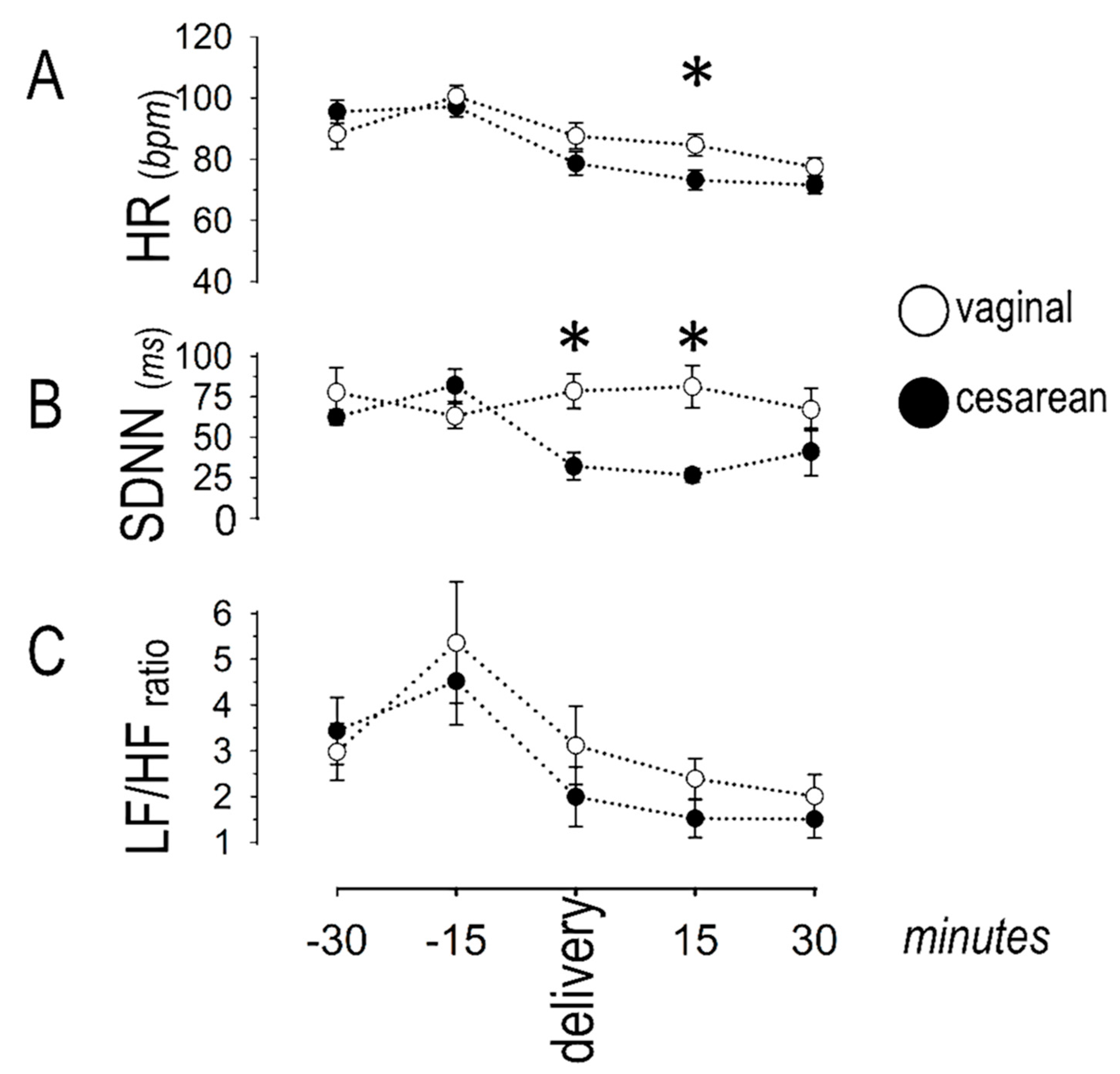
3.1. Sympatho-Vagal Balance
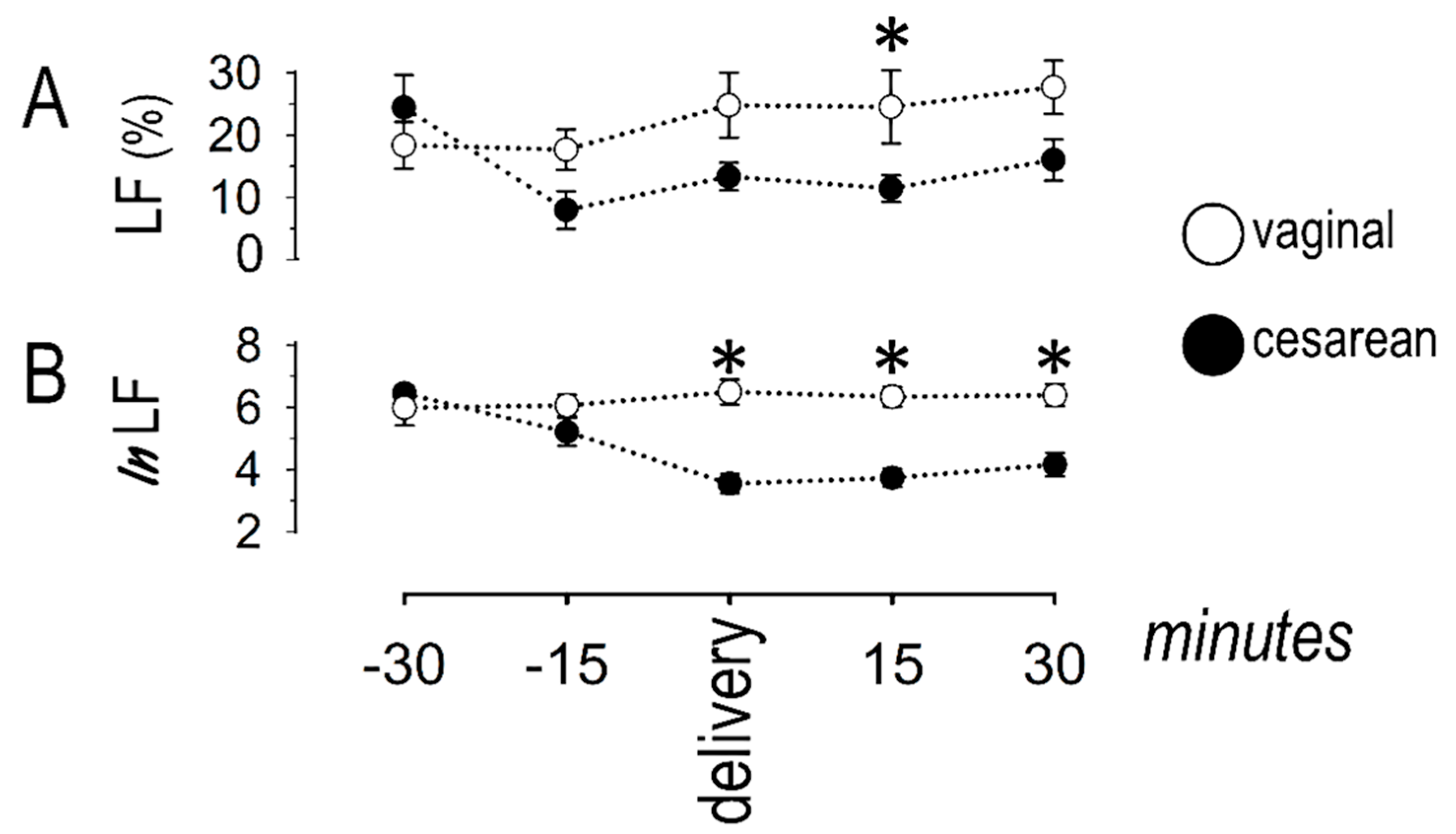
3.2. Sympathetic Response
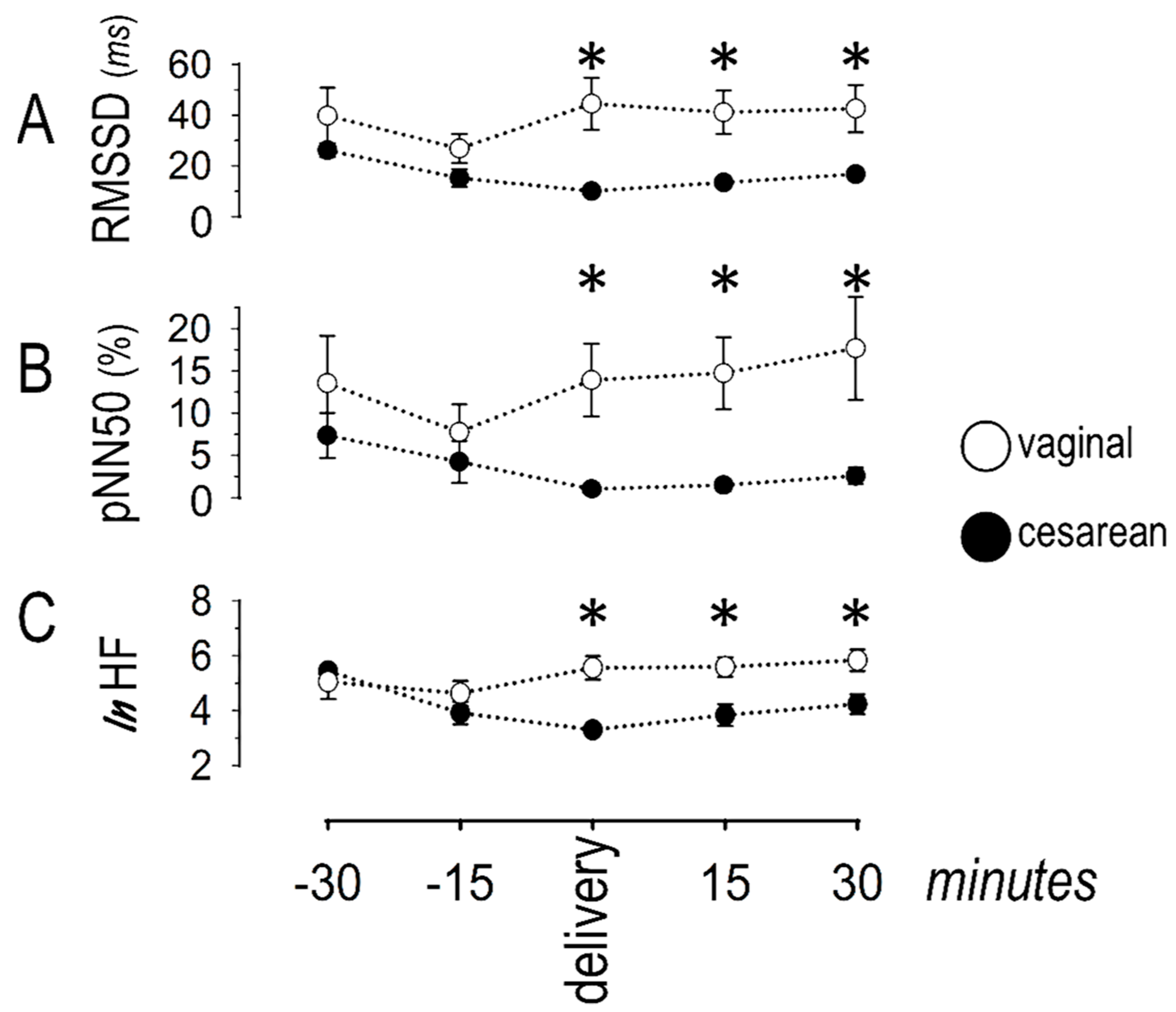
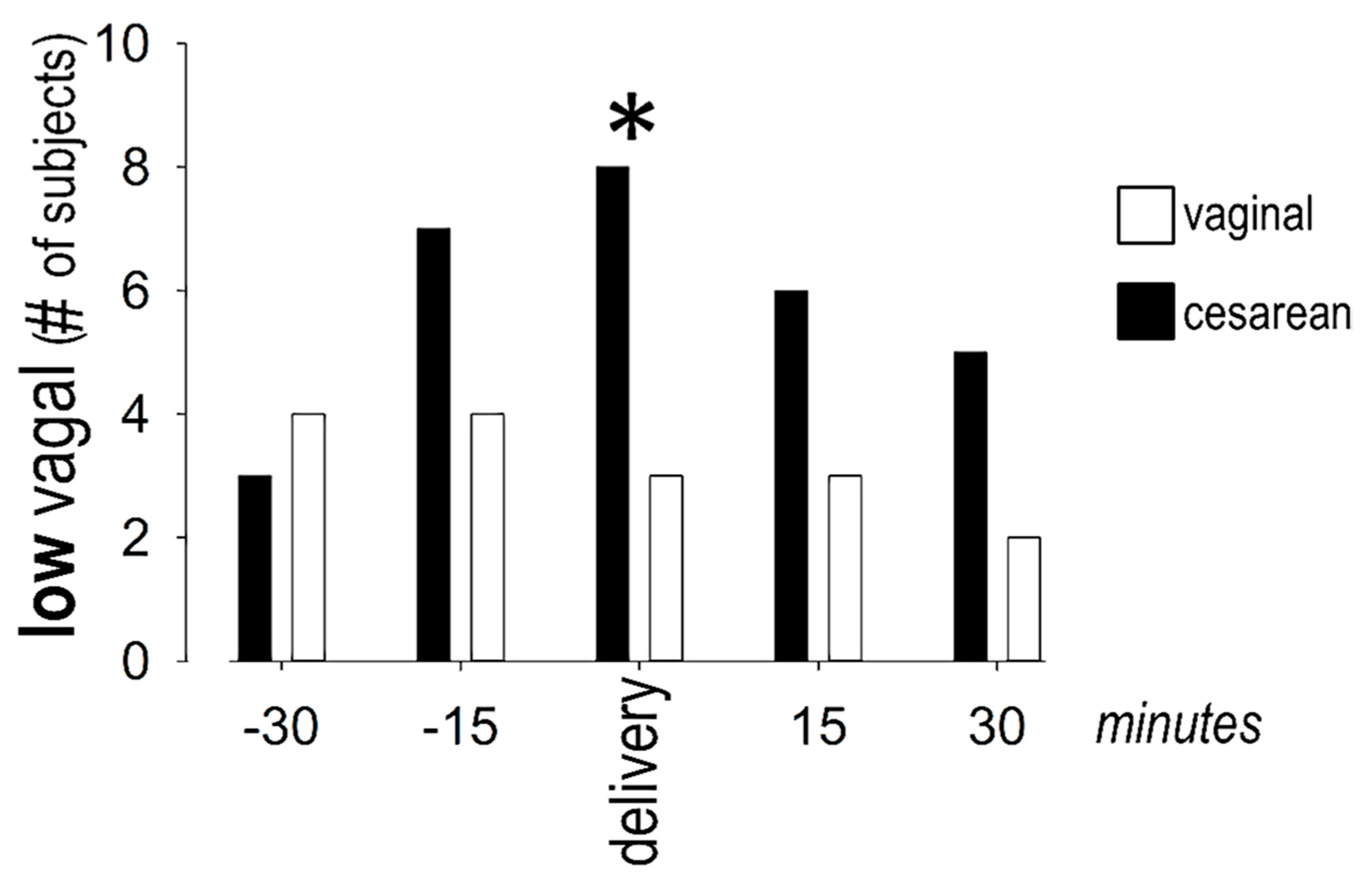
3.3. Vagal Response
4. Discussion
4.1. Main Findings
4.2. Autonomic Responses during Cesarean Delivery
4.3. Autonomic Responses during Vaginal Delivery
4.4. Implications for Takotsubo Syndrome
4.5. Implications for Other Clinical Conditions beyond Takotsubo Syndrome
4.6. Excessive Autonomic Changes Caused by Pharmacologic Agents
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Oindi, F.M.; Sequeira, E.; Sequeira, H.R.; Mutiso, S.K. Takotsubo cardiomyopathy in pregnancy: A case report and literature review. BMC Pregnancy Childbirth 2019, 19, 89. [Google Scholar] [CrossRef] [Green Version]
- Minatoguchi, M.; Itakura, A.; Takagi, E.; Nishibayashi, M.; Kikuchi, M.; Ishihara, O. Takotsubo cardiomyopathy after cesarean: A case report and published work review of pregnancy-related cases. J. Obstet. Gynaecol. Res. 2014, 40, 1534–1539. [Google Scholar] [CrossRef] [PubMed]
- Citro, R.; Lyon, A.; Arbustini, E.; Bossone, E.; Piscione, F.; Templin, C.; Narula, J. Takotsubo syndrome after cesarean section: Rare but possible. J. Am. Coll. Cardiol. 2018, 71, 1838–1839. [Google Scholar] [CrossRef]
- Zdanowicz, J.A.; Utz, A.C.; Bernasconi, I.; Geier, S.; Corti, R.; Beinder, E. “Broken heart” after cesarean delivery. Case report and review of literature. Arch. Gynecol. Obstet. 2011, 283, 687–694. [Google Scholar] [CrossRef]
- Pelliccia, F.; Kaski, J.C.; Crea, F.; Camici, P.G. Pathophysiology of takotsubo syndrome. Circulation 2017, 135, 2426–2441. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Sarcon, A.; Diekmann, J.; Bataiosu, D.R.; Cammann, V.L.; Jurisic, S.; Napp, L.C.; Jaguszewski, M.; Scherff, F.; Brugger, P.; et al. Happy heart syndrome: Role of positive emotional stress in takotsubo syndrome. Eur. Heart J. 2016, 37, 2823–2829. [Google Scholar] [CrossRef] [Green Version]
- Pinna, T.; Edwards, D.J. A Systematic review of associations between interoception, vagal tone and emotional regulation: Potential applications for mental health, wellbeing, psychological flexibility, and chronic conditions. Front. Psychol. 2020, 11, 1792. [Google Scholar] [CrossRef] [PubMed]
- Hauck, Y.; Fenwick, J.; Downie, J.; Butt, J. The influence of childbirth expectations on Western Australian women’s perceptions of their birth experience. Midwifery 2007, 23, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Nunan, D.; Sandercock, G.R.; Brodie, D.A. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin. Electrophysiol. 2010, 33, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Kuo, T.B.; Lin, T.; Yang, C.C.; Li, C.L.; Chen, C.F.; Chou, P. Effect of aging on gender differences in neural control of heart rate. Am. J. Physiol. 1999, 277, H2233–H2239. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones III, C.M.; Greiss, F.C., Jr. The effect of labor on maternal and fetal circulating catecholamines. Am. J. Obstet. Gynecol. 1982, 144, 149–153. [Google Scholar] [CrossRef]
- Kanaya, N.; Hirata, N.; Kurosawa, S.; Nakayama, M.; Namiki, A. Differential effects of propofol and sevoflurane on heart rate variability. Anesthesiology 2003, 98, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Ebert, T.J.; Muzi, M.; Berens, R.; Goff, D.; Kampine, J.P. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology 1992, 76, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Thorlacius, K.; Zhoujun, C.; Bodelsson, M. Effects of sevoflurane on sympathetic neurotransmission in human omental arteries and veins. Br. J. Anaesth. 2003, 90, 766–773. [Google Scholar] [CrossRef] [Green Version]
- Colson, P.; Barlet, H.; Roquefeuill, B.; Eledjam, J.J. Mechanism of propofol bradycardia. Anesth. Analg. 1988, 67, 906–907. [Google Scholar] [CrossRef]
- Tramer, M.R.; Moore, R.A.; McQuay, H.J. Propofol and bradycardia: Causation, frequency and severity. Br. J. Anaesth. 1997, 78, 642–651. [Google Scholar] [CrossRef]
- Suzuki, N.; Sugawara, J.; Kimura, Y.; Nagase, S.; Okamura, K.; Yaegashi, N. Assessment of maternal heart-rate variability during labor using wavelet-based power spectral analysis. Gynecol. Obs. Investig. 2012, 74, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Reyes, J.J.; Pena, M.A.; Echeverria, J.C.; Garcia, M.T.; Ortiz, M.R.; Vargas, C.; Gonzalez-Camarena, R. Short-term heart rate dynamics of women during labor. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2011, 2011, 1929–1932. [Google Scholar] [PubMed]
- Heinrichs, M.; Baumgartner, T.; Kirschbaum, C.; Ehlert, U. Social support and oxytocin interact to suppress cortisol and subjective responses to psychosocial stress. Biol. Psychiatry 2003, 54, 1389–1398. [Google Scholar] [CrossRef]
- Carter, C.S.; Kenkel, W.M.; MacLean, E.L.; Wilson, S.R.; Perkeybile, A.M.; Yee, J.R.; Ferris, C.F.; Nazarloo, H.P.; Porges, S.W.; Davis, J.M.; et al. Is oxytocin “nature’s medicine”? Pharm. Rev. 2020, 72, 829–861. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.J.; Cacioppo, J.T.; Morris, J.S.; Malarkey, W.B.; Berntson, G.G.; Devries, A.C. Oxytocin increases autonomic cardiac control: Moderation by loneliness. Biol. Psychol. 2011, 86, 174–180. [Google Scholar] [CrossRef] [PubMed]
- de Geest, K.; Thiery, M.; Piron-Possuyt, G.; Vanden Driessche, R. Plasma oxytocin in human pregnancy and parturition. J. Perinat. Med. 1985, 13, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Kjerulff, K.H.; Brubaker, L.H. New mothers’ feelings of disappointment and failure after cesarean delivery. Birth 2018, 45, 19–27. [Google Scholar] [CrossRef]
- Akashi, Y.J.; Barbaro, G.; Sakurai, T.; Nakazawa, K.; Miyake, F. Cardiac autonomic imbalance in patients with reversible ventricular dysfunction takotsubo cardiomyopathy. J. Assoc. Physicians 2007, 100, 335–343. [Google Scholar] [CrossRef]
- Norcliffe-Kaufmann, L.; Kaufmann, H.; Martinez, J.; Katz, S.D.; Tully, L.; Reynolds, H.R. Autonomic findings in takotsubo cardiomyopathy. Am. J. Cardiol. 2016, 117, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Pauza, D.H.; Skripka, V.; Pauziene, N.; Stropus, R. Morphology, distribution, and variability of the epicardiac neural ganglionated subplexuses in the human heart. Anat. Rec. 2000, 259, 353–382. [Google Scholar] [CrossRef]
- Landzberg, J.S.; Parker, J.D.; Gauthier, D.F.; Colucci, W.S. Effects of intracoronary acetylcholine and atropine on basal and dobutamine-stimulated left ventricular contractility. Circulation 1994, 89, 164–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastitskaya, S.; Marina, N.; Gourine, A.; Gilbey, M.P.; Spyer, K.M.; Teschemacher, A.G.; Kasparov, S.; Trapp, S.; Ackland, G.L.; Gourine, A.V. Cardioprotection evoked by remote ischaemic preconditioning is critically dependent on the activity of vagal pre-ganglionic neurones. Cardiovasc. Res. 2012, 95, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Kawada, T.; Yamazaki, T.; Akiyama, T.; Li, M.; Ariumi, H.; Mori, H.; Sunagawa, K.; Sugimachi, M. Vagal stimulation suppresses ischemia-induced myocardial interstitial norepinephrine release. Life Sci. 2006, 78, 882–887. [Google Scholar] [CrossRef] [PubMed]
- L’Ecuyer, E.; Codsi, E.; Mongeon, F.P.; Dore, A.; Morin, F.; Leduc, L. Perinatal and cardiac outcomes of women with hypertrophic cardiomyopathy. J. Matern. Fetal Neonatal Med. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tsiaras, S.; Poppas, A. Mitral valve disease in pregnancy: Outcomes and management. Obstet. Med. 2009, 2, 6–10. [Google Scholar] [CrossRef]
- Amariles, P. A comprehensive literature search: Drugs as possible triggers of Takotsubo cardiomyopathy. Curr. Clin. Pharm. 2011, 6, 1–11. [Google Scholar] [CrossRef]
- Littlejohn, F.C.; Syed, O.; Ornstein, E.; Connolly, E.S.; Heyer, E.J. Takotsubo cardiomyopathy associated with anesthesia: Three case reports. Cases J. 2008, 1, 227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lederman, R.P.; McCann, D.S.; Work, B., Jr.; Huber, M.J. Endogenous plasma epinephrine and norepinephrine in last-trimester pregnancy and labor. Am. J. Obstet. Gynecol. 1977, 129, 5–8. [Google Scholar] [CrossRef]
- Hawkins, J.L.; Chang, J.; Palmer, S.K.; Gibbs, C.P.; Callaghan, W.M. Anesthesia-related maternal mortality in the United States: 1979–2002. Obs. Gynecol. 2011, 117, 69–74. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoulos, G.E.; Evaggelou, T.I.; Moulias, E.K.; Tsonis, O.; Zekios, K.C.; Nikas, D.N.; Tzimas, P.; Paschopoulos, M.; Kolettis, T.M. Autonomic Responses during Labor: Potential Implications for Takotsubo Syndrome. J. Cardiovasc. Dev. Dis. 2021, 8, 152. https://doi.org/10.3390/jcdd8110152
Papadopoulos GE, Evaggelou TI, Moulias EK, Tsonis O, Zekios KC, Nikas DN, Tzimas P, Paschopoulos M, Kolettis TM. Autonomic Responses during Labor: Potential Implications for Takotsubo Syndrome. Journal of Cardiovascular Development and Disease. 2021; 8(11):152. https://doi.org/10.3390/jcdd8110152
Chicago/Turabian StylePapadopoulos, Georgios E., Theoxaris I. Evaggelou, Errikos K. Moulias, Orestis Tsonis, Konstantinos C. Zekios, Dimitrios N. Nikas, Petros Tzimas, Minas Paschopoulos, and Theofilos M. Kolettis. 2021. "Autonomic Responses during Labor: Potential Implications for Takotsubo Syndrome" Journal of Cardiovascular Development and Disease 8, no. 11: 152. https://doi.org/10.3390/jcdd8110152
APA StylePapadopoulos, G. E., Evaggelou, T. I., Moulias, E. K., Tsonis, O., Zekios, K. C., Nikas, D. N., Tzimas, P., Paschopoulos, M., & Kolettis, T. M. (2021). Autonomic Responses during Labor: Potential Implications for Takotsubo Syndrome. Journal of Cardiovascular Development and Disease, 8(11), 152. https://doi.org/10.3390/jcdd8110152