Left Ventricular Noncompaction Is More Prevalent in Ventricular Septal Defect Than Other Congenital Heart Defects: A Morphological Study





Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Both Short and Long Axis of the Heart Can Be Used for Noncompaction Measurements
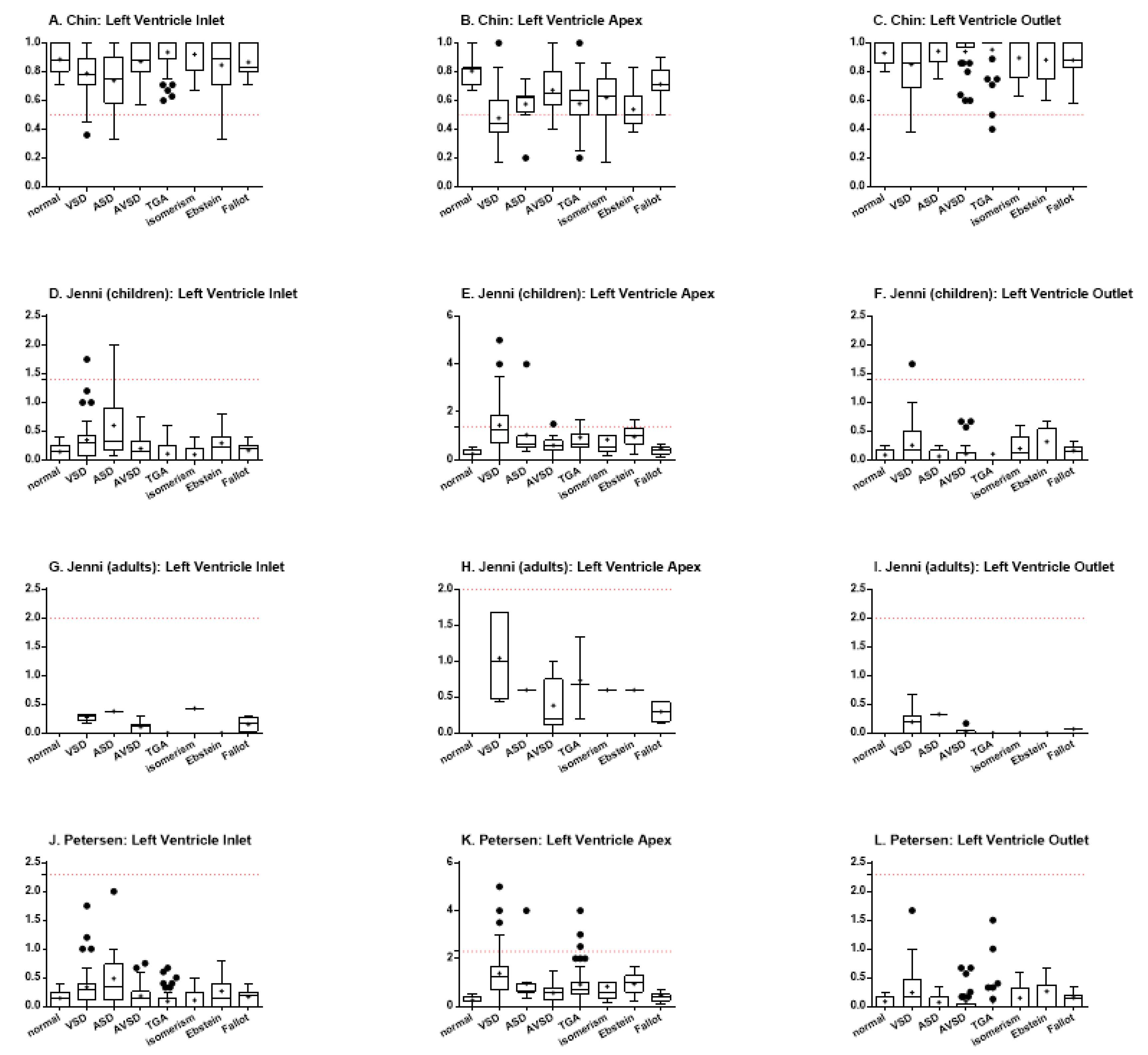
3.3. Different Ventricular Walls Present Different Degrees of LVNC
3.4. LVNC Is More Often Associated with Ventricular Septal Defect than Other Congenital Heart Diseases
3.5. Different LVNC Diagnostic Criteria Lead to Important Differences in Outcomes
3.6. Prevalence of LVCN According to Age
3.7. Sex Influence on the Prevalence of LVCN
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Engberding, R.; Bender, F. Identification of a rare congenital anomaly of the myocardium by twodimensional echocardiography: Persistence of isolated myocardial sinusoids. Am. J. Cardiol. 1984, 53, 1733–1734. [Google Scholar] [CrossRef]
- Lofiego, C.; Biagini, E.; Pasquale, F.; Ferlito, M.; Rocchi, G.; Perugini, E.; Bacchi-Reggiani, M.L.; Boriani, G.; Leone, O.; Caliskan, K.; et al. Wide spectrum of presentation and variable outcomes of isolated left ventricular non-compaction. Heart 2007, 93, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.G.; Pinto, F. Non-compaction cardiomyopathy. Heart 2013, 99, 1535–1542. [Google Scholar] [CrossRef]
- Chin, T.K.; Perloff, J.K.; Williams, R.G.; Jue, K.; Mohrmann, R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation 1990, 82, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Jenni, R.; Oechslin, E.; Schneider, J.; Attenhofer, C.; Kaufmann, P.A. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: A step towards classification as a distinct cardiomyopathy. Heart 2001, 86, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Stöllberger, C.; Finsterer, J.; Blazek, G. Left ventricular hypertrabeculation/noncompaction and association with additional cardiac abnormalities and neuromuscular disorders. Am. J. Cardiol. 2002, 90, 899–902. [Google Scholar] [CrossRef]
- Petersen, S.E.; Selvanayagam, J.B.; Wiesmann, F.; Robson, M.D.; Francis, J.M.; Anderson, R.H.; Watkins, H.; Neubauer, S. Left Ventricular Non-Compaction. J. Am. Coll. Cardiol. 2005, 46, 101–105. [Google Scholar] [CrossRef]
- Jacquier, A.; Thuny, F.; Jop, B.; Giorgi, R.; Cohen, F.; Gaubert, J.-Y.; Vidal, V.; Bartoli, J.M.; Habib, G.; Moulin, G. Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur. Hear. J. 2010, 31, 1098–1104. [Google Scholar] [CrossRef]
- Ritter, M.; Oechslin, E.; Sütsch, G.; Attenhofer, C.; Schneider, J.; Jenni, R. Isolated Noncompaction of the Myocardium in Adults. Mayo Clin. Proc. 1997, 72, 26–31. [Google Scholar] [CrossRef]
- Xu, L.; Yang, J.; Yang, Y. Acute Kidney Infarction Due to Left Ventricular Thrombus Embolization In Patient with Isolated Left Ventricular Noncompaction: A Case Report. Hear. Surg. Forum. 2017, 20, 252–255. [Google Scholar] [CrossRef][Green Version]
- Papadopoulos, K.; Petrou, P.M.; Michaelides, D. Left Ventricular Noncompaction Cardiomyopathy Presenting with Heart Failure in a 35-Year-Old Man. Tex. Hear. Inst. J. 2017, 44, 260–263. [Google Scholar] [CrossRef]
- Oechslin, E.N.; Jost, C.H.A.; Rojas, J.R.; A Kaufmann, P.; Jenni, R. Long-term follow-up of 34 adults with isolated left ventricular noncompaction: A distinct cardiomyopathy with poor prognosis. J. Am. Coll. Cardiol. 2000, 36, 493–500. [Google Scholar] [CrossRef]
- Ramachandran, P.; Woo, J.G.; Ryan, T.D.; Bryant, R.; Heydarian, H.C.; Jefferies, J.L.; Towbin, J.A.; Lorts, A. The Impact of Concomitant Left Ventricular Non-compaction with Congenital Heart Disease on Perioperative Outcomes. Pediatr. Cardiol. 2016, 37, 1307–1312. [Google Scholar] [CrossRef]
- Sedmera, D.; Pexieder, T.; Vuillemin, M.; Thompson, R.P.; Anderson, R.H. Developmental patterning of the myocardium. Anat. Rec. 2000, 258, 319–337. [Google Scholar] [CrossRef]
- Anderson, R.H.; Jensen, B.; Mohun, T.J.; Petersen, S.E.; Aung, N.; Zemrak, F.; Planken, R.N.; Maciver, D.H. Key Questions Relating to Left Ventricular Noncompaction Cardiomyopathy: Is the Emperor Still Wearing Any Clothes? Can. J. Cardiol. 2017, 33, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Attenhofer Jost, C.H.; Connolly, H.M.; O’Leary, P.W.; Warnes, C.A.; Tajik, A.J.; Seward, J.B. Left heart lesions in patients with Ebstein anomaly. Mayo Clin. Proc. 2005, 80, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Aga, P.; Singh, R.; Tiwari, B. Non-compaction of the left ventricular myocardium with Cor-triatriatum and associated anomalies. BMJ Case Rep. 2013, 2013, bcr2012008104. [Google Scholar] [CrossRef] [PubMed]
- Fazio, G.; Visconti, C.; D’Angelo, L.; Grassedonio, E.; Re, G.L.; D’Amico, T.; Sutera, L.; Novo, G.; Ferrara, F.; Midiri, M.; et al. Diagnosis and definition of biventricular non-compaction associated to Ebstein’s anomaly. Int. J. Cardiol. 2011, 150, e20–e24. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Song, H.; Jiang, S.; Li, T. Congenital Atresia of the Left Main Coronary Artery with Noncompaction of the Ventricular Myocardium in an Asymptomatic Young Child. Pediatr. Cardiol. 2012, 34, 1998–2002. [Google Scholar] [CrossRef] [PubMed]
- Nimeri, N.A.; Nahia, F.F.A.; Ibrahim, A.S.; Khella, A.Y. The first reported case of non-compacted cardiomyopathy in a preterm infant with Ebstein’s anomaly. BMJ Case Rep. 2012, 2012, bcr0220125861. [Google Scholar] [CrossRef] [PubMed]
- Calzolari, M.; Gaddi, O.; Ilari, B.; Iotti, R.; Tortorella, G.; Muià, N.; Guiducci, U. Association of non-compacted myocardium and patent ductus arteriosus in a young asymptomatic male patient: Findings in screening for contact sport eligibility. Ital. Hear. J. Suppl. Off. J. Ital. Fed. Cardiol. 2002, 3, 659–664. [Google Scholar]
- Vermeer, A.M.C.; Van Engelen, K.; Postma, A.V.; Baars, M.J.; Christiaans, I.; De Haij, S.; Klaassen, S.; Mulder, B.J.; Keavney, B. Ebstein anomaly associated with left ventricular noncompaction: An autosomal dominant condition that can be caused by mutations in MYH7. Am. J. Med. Genet. Part C Semin. Med. Genet. 2013, 163, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.S.; Madureira, A.J.; Almeida, P.B.; Goncalves, A.; Araújo, V. Double-chambered left ventricle plus left ventricular non-compaction: Report of an abnormal association. Eur. Hear. J. Cardiovasc. Imaging 2012, 14, 127. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Laghari, A.H.; Tai, J.M.; Saleem, S. Non-compaction of the left ventricle and associated ventricular septal defect. BMJ Case Rep. 2012, bcr2012006614. [Google Scholar] [CrossRef] [PubMed]
- Stähli, B.E.; Gebhard, C.; Biaggi, P.; Klaassen, S.; Buechel, E.V.; Jost, C.H.A.; Jenni, R.; Tanner, F.; Greutmann, M. Left ventricular non-compaction: Prevalence in congenital heart disease. Int. J. Cardiol. 2013, 167, 2477–2481. [Google Scholar] [CrossRef]
- Zuckerman, W.A.; Richmond, M.E.; Singh, R.K.; Carroll, S.J.; Starc, T.J.; Addonizio, L.J. Left-ventricular noncompaction in a pediatric population: Predictors of survival. Pediatr. Cardiol. 2011, 32, 406–412. [Google Scholar] [CrossRef]
- Punn, R.; Silverman, N.H. Cardiac Segmental Analysis in Left Ventricular Noncompaction: Experience in a Pediatric Population. J. Am. Soc. Echocardiogr. 2010, 23, 46–53. [Google Scholar] [CrossRef]
- Tsai, S.F.; Ebenroth, E.S.; Hurwitz, R.A.; Cordes, T.M.; Schamberger, M.S.; Batra, A.S. Is Left Ventricular Noncompaction in Children Truly an Isolated Lesion? Pediatr. Cardiol. 2009, 30, 597–602. [Google Scholar] [CrossRef]
- Partridge, J.B.; Anderson, R.H. Left ventricular anatomy: Its nomenclature, segmentation, and planes of imaging. Clin. Anat. 2009, 22, 77–84. [Google Scholar] [CrossRef]
- Van Der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; A Helbing, W.; Takkenberg, J.J.M.; Roos-Hesselink, J.W. Birth Prevalence of Congenital Heart Disease Worldwide. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef]
- Zemrak, F.; Ahlman, M.A.; Captur, G.; Mohiddin, S.A.; Kawel-Boehm, N.; Prince, M.R.; Moon, J.C.; Hundley, W.G.; Lima, J.A.; Bluemke, D.A.; et al. The relationship of left ventricular trabeculation to ventricular function and structure over a 9.5-year follow-up: The MESA study. J. Am. Coll. Cardiol. 2014, 64, 1971–1980. [Google Scholar] [CrossRef] [PubMed]
- Arbustini, E.; Favalli, V.; Narula, N.; Serio, A.; Grasso, M. Left Ventricular Noncompaction. J. Am. Coll. Cardiol. 2016, 68, 949–966. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Sample Size | Criteria | Total of CHD | Congenital Heart Defect (n) |
|---|---|---|---|---|
| Stähli (2013) [25] | 202 | Jenni | 40 (19.8%) | Uni-or bicuspid aortic valves (7) Ebstein Anomaly (6) Tetralogy of Fallot (3) Aortic Coarctation (2) |
| Zuckerman (2010) [26] | 50 | Jenni | 13 (26.0%) | VSD (7) ASD (4) PAPVC (1) Pulmonary atresia with intact ventricular septum (1) |
| Punn (2010) [27] | 44 | Jenni | 13 (29.5%) | Ebstein Anomaly (7) AVSD (3) VSD (3) Tetralogy of Fallot (2) Pulmonary valve stenosis (2) |
| Tsai (2009) [28] | 46 | Chin | 38 (82.6%) | VSD (17) ASD (16) PDA (14) Ebstein Anomaly (5) |
| Criterium | Method | Acquisition | Moment | LVNC Threshold |
|---|---|---|---|---|
| Chin et al. | Echocardiography | Short axis | End-diastolic | C/T < 0.5 |
| Jenni et al. | Echocardiography | Short axis | End-systolic | NC/C > 1.4 (or >2.0 in adults) |
| Petersen et al. | CMR | Long axis | End-diastolic | NC/C > 2.3 |
| CHD | Sex | Age | ||||
|---|---|---|---|---|---|---|
| Male | Female | NA | Children | Adult | NA | |
| normal | 4 (36.4%) | 6 (54.5%) | 1 (9.1%) | 11 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| VSD | 25 (49.0%) | 24 (47.0%) | 2 (4.0%) | 43 (84.3%) | 7 (13.7%) | 1 (2.0%) |
| ASD | 5 (31.3%) | 8 (50%) | 3 (18.7%) | 11 (68.8%) | 2 (12.5%) | 3 (18.7%) |
| AVSD | 17 (41.5%) | 24 (58.6%) | 0 (0.0%) | 33 (80.5%) | 8 (19.5%) | 0 (0.0%) |
| TGA | 33 (61.1%) | 20 (37.0%) | 1 (1.9%) | 51 (94.5%) | 3 (5.5%) | 0 (0%) |
| Isomerism | 10 (34.5%) | 18 (62.1%) | 1 (3.4%) | 26 (89.7%) | 1 (3.4%) | 2 (6.9%) |
| Ebstein | 7 (30.4%) | 16 (69.6%) | 0 (0.0%) | 21 (91.3%) | 2 (8.7%) | 0 (0.0%) |
| Fallot | 18 (52.9%) | 16 (47.1%) | 0 (0.0%) | 30 (88.2%) | 4 (11.8%) | 0 (0.0%) |
| TOTAL | 119 (45.9%) | 132 (51.0%) | 8 (3.1%) | 226 (87.3%) | 27 (10.4%) | 6 (2.3%) |
| Chin | Jenni | Petersen | |||||||
|---|---|---|---|---|---|---|---|---|---|
| % (n) | OR * (95% CI) | p-value | % (n) | OR * (95% CI) | p-Value | % (n) | OR * (95% CI) | p-Value | |
| normal | 0.0% (0/11) | - | - | 0.0% (0/11) | - | - | 0.0% (0/11) | - | - |
| VSD | 54.2% (26/48) | 27.09 (1.51–486.10) | 0.0013 | 35.4% (17/48) | 12.78 (0.71–230.3) | 0.0241 | 12.5% (6/48) | 3.52 (0.18–67.21) | 0.5820 |
| ASD | 8.3% (1/12) | 3.00 (0.11–81.68) | 1.0000 | 8.3% (1/12) | 3.00 (0.11–81.68) | 1.0000 | 8.3% (1/12) | 3.00 (0.11–81.68) | 1.0000 |
| AVSD | 2.9% (1/34) | 1.03 (0.04–27.12) | 1.0000 | 2.9% (1/34) | 1.03 (0.04–27.12) | 1.000 | 0.0% (0/34) | 0.33 (0.01–17.79) | 1.0000 |
| TGA | 22.6% (12/53) | 6.93 (0.38–126.1) | 0.1064 | 17.0% (9/53) | 4.91 (0.27–90.81) | 0.3382 | 5.7% (3/53) | 1.59 (0.08–33.07) | 1.0000 |
| Isomerism | 7.1% (2/28) | 2.17 (0.96–48.89) | 1.0000 | 7.1% (2/28) | 2.17 (0.096–48.89) | 1.000 | 7.1% (2/28) | 2.17 (0.096–48.89) | 1.0000 |
| Ebstein | 28.6% (6/21) | 9.65 (0.49–189.20) | 0.0711 | 9.5% (2/21) | 2.95 (0.13–67.00) | 0.5343 | 0.0% (0/21) | 0.53 (0.01–28.79) | 1.0000 |
| Fallot | 5.9% (2/34) | 1.77 (0.08–39.70) | 1.0000 | 2.9% (1/34) | 1.030 (0.04–27.12) | 1.0000 | 2.9% (1/34) | 1.030 (0.04–27.12) | 1.0000 |
| Chin | Jenni | Petersen | |
|---|---|---|---|
| 1 | VSD | VSD | VSD |
| 2 | Ebstein | TGA | ASD |
| 3 | TGA | Ebstein | Isomerism |
| 4 | ASD | ASD | TGA |
| 5 | Isomerism | Isomerism | Fallot |
| 6 | Fallot | AVSD/Fallot | AVSD/Ebstein |
| 7 | AVSD | - | - |
| Chin | Jenni | Petersen | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CHD | % (n) | OR * (95% CI) | p-Value | % (n) | OR * (95% CI) | p-Value | % (n) | OR * (95% CI) | p-Value |
| isolated TGA | 22.2% (4/18) | - | - | 11.1% (2/18) | - | - | 5.6% (1/18) | - | - |
| TGA + ASD | 6.7% (1/15) | 0.25 (0.02–2.53) | 0.3457 | 6.7% (1/15) | 0.57 (0.05–7.0) | 1.000 | 0.0% (0/15) | 0.38 (0.01–9.94) | 1.0000 |
| TGA + ASD + VSD | 57.1% (4/7) | 4.67 (0.72–30.12) | 0.1563 | 57.1% (4/7) | 10.67 (1.30–86.98) | 0.0324 | 28.6% (2/7) | 6.8 (0.51–91.55) | 0.1796 |
| TGA + VSD | 23.1% (3/13) | 1.05 (0.19–5.77) | 1.0000 | 15.4% (2/13) | 1.46 (0.18–11.94) | 1.0000 | 0.0% (0/13) | 0.43 (0.02–11.47) | 1.0000 |
| Chin | Jenni | Petersen | |||||||
|---|---|---|---|---|---|---|---|---|---|
| CHD | % (n) | OR * (95% CI) | p-Value | % (n) | OR * (95% CI) | p-Value | % (n) | OR * (95% CI) | p-Value |
| isolated isomerism | 0.0% (0/3) | - | - | 0.0% (0/3) | - | - | 0.0% (0/3) | - | - |
| isomerism + ASD | 0.0% (0/4) | 0.78 (0.01–49.95) | 1.0000 | 0.0% (0/4) | 0.78 (0.01–49.95) | 1.0000 | 0.0% (0/4) | 0.78 (0.01–49.95) | 1.0000 |
| isomerism + ASD + VSD | 20.0% (1/5) | 2.33 (0.70–76.73) | 1.0000 | 20.0% (1/5) | 2.33 (0.70–76.73) | 1.0000 | 20.0% (1/5) | 2.33 (0.70–76.73) | 1.0000 |
| isomerism + AVSD | 0.0% (0/8) | 0.41 (0.01–25.19) | 1.0000 | 0.0% (0/8) | 0.41 (0.01–25.19) | 1.000 | 0.0% (0/8) | 0.41 (0.01–25.19) | 1.0000 |
| other combinations | 11.1% (1/9) | 1.23 (0.04–38.33) | 1.0000 | 11.1% (1/9) | 1.23 (0.04–38.33) | 1.0000 | 11.1% (1/9) | 1.23 (0.04–38.33) | 1.0000 |
| CHD | Chin | Jenni | Petersen | |||
|---|---|---|---|---|---|---|
| Children (≤18 y) | Adults (>18 y) | Children (≤18 y) | Adults (>18 y) | Children (≤18 y) | Adults (>18 y) | |
| VSD | 57.1% (24/42) | 40% (2/5) | 40.5% (17/42) | 0.0% (0/5) | 14.3% (6/42) | 0.0% (0/5) |
| ASD | 11.1% (1/9) | 0.0% (0/1) | 11.1% (1/9) | 0.0% (0/1) | 11.1% (1/9) | 0.0% (0/1) |
| AVSD | 3.6% (1/28) | 0.0% (0/6) | 3.6% (1/28) | 0.0% (0/6) | 0.0% (0/28) | 0.0% (0/6) |
| TGA | 22% (11/50) | 33.3% (1/3) | 18% (9/50) | 0.0% (0/3) | 6% (3/50) | 0.0% (0/3) |
| Isomerism | 8% (2/25) | 0.0% (0/2) | 8% (2/25) | 0.0% (0/2) | 8% (2/25) | 0.0% (0/2) |
| Ebstein | 31.6% (6/19) | 0.0% (0/2) | 10.5% (2/19) | 0.0% (0/2) | 0.0% (0/19) | 0.0% (0/2) |
| Fallot | 6.7% (2/30) | 0.0% (0/4) | 3.3% (1/30) | 0.0% (0/4) | 3.3% (1/30) | 0.0% (0/4) |
| TOTAL | 23.2% (47/203) | 13.0% (3/23) | 16.3% (33/203) | 0.0% (0/23) | 6.4% (13/203) | 0.0% (0/23) |
| CHD | Chin | Jenni | Petersen | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | OR (95% CI) | p-Value | Male | Female | OR (95% CI) | p-Value | Male | Female | OR (95% CI) | p-Value | |
| VSD | 41.7% (10/24) | 68.2% (15/22) | 3.00 (0.89–10.06) | 0.0852 | 25.0% (6/24) | 45.5% (10/22) | 2.50 (0.72–8.71) | 0.2167 | 0.0% (0/24) | 22.7% (5/22) | 15.40 (0.80–297.2) | 0.0192 |
| ASD | 25.0% (1/4) | 0.0% (0/6) | 0.17 (0.01–5.68) | 0.4000 | 25.0% (1/4) | 0.0% (0/6) | 0.18 (0.01–5.68) | 0.4000 | 25.0% (1/4) | 0.0% (0/6) | 0.18 (0.01–5.68) | 0.4000 |
| AVSD | 7.1% (1/14) | 0.0% (0/20) | 0.22 (0.01–5.80) | 0.4118 | 7.1% (1/14) | 0.0% (0/20) | 0.22 (0.01–5.80) | 0.4118 | 0.0% (0/14) | 0.0% (0/20) | 0.70 (0.01–37.79) | 1.0000 |
| TGA | 18.8% (6/32) | 25.0% (5/20) | 1.44 (0.38–5.55) | 0.7300 | 15.6% (5/32) | 15% (3/20) | 0.95 (0.20–4.51) | 1.0000 | 3.1% (1/32) | 10% (2/20) | 3.44 (0.29–40.74) | 0.5511 |
| Isomerism | 10.0% (1/10) | 5.9% (1/17) | 0.56 (0.03–10.12) | 1.0000 | 10.0% (1/10) | 5.9% (1/17) | 0.56 (0.03–10.12) | 1.0000 | 10.0% (1/10) | 5.9% (1/17) | 0.56 (0.03–10.12) | 1.0000 |
| Ebstein | 14.3% (1/7) | 35.7% (5/14) | 3.33 (0.31–36.13) | 0.6126 | 0.0% (0/7) | 14.3% (2/14) | 3.00 (0.13–71.37) | 0.5333 | 0.0% (0/7) | 0.0% (0/14) | 0.52 (0.01–28.78) | 1.0000 |
| Fallot | 11.1% (2/18) | 0.0% (0/16) | 0.20 (0.01–4.50) | 0.8889 | 15.6% (1/18) | 0.0% (0/16) | 0.35 (0.01–9.31) | 1.0000 | 15.6% (1/18) | 0.0% (0/16) | 0.35 (0.01–9.31) | 1.0000 |
| TOTAL | 20.2% (22/109) | 22.6% (26/115) | 1.06 (0.90–1.24) | 0.7551 | 13.8% (15/109) | 13.9% (16/115) | 1.01 (0.47–2.16) | 1.0000 | 3.7% (4/109) | 7.0% (8/115) | 1.963 (0.57–6.71) | 0.3766 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marques, L.C.; Liguori, G.R.; Amarante Souza, A.C.; Aiello, V.D. Left Ventricular Noncompaction Is More Prevalent in Ventricular Septal Defect Than Other Congenital Heart Defects: A Morphological Study. J. Cardiovasc. Dev. Dis. 2020, 7, 39. https://doi.org/10.3390/jcdd7040039
Marques LC, Liguori GR, Amarante Souza AC, Aiello VD. Left Ventricular Noncompaction Is More Prevalent in Ventricular Septal Defect Than Other Congenital Heart Defects: A Morphological Study. Journal of Cardiovascular Development and Disease. 2020; 7(4):39. https://doi.org/10.3390/jcdd7040039
Chicago/Turabian StyleMarques, Laís Costa, Gabriel Romero Liguori, Ana Carolina Amarante Souza, and Vera Demarchi Aiello. 2020. "Left Ventricular Noncompaction Is More Prevalent in Ventricular Septal Defect Than Other Congenital Heart Defects: A Morphological Study" Journal of Cardiovascular Development and Disease 7, no. 4: 39. https://doi.org/10.3390/jcdd7040039
APA StyleMarques, L. C., Liguori, G. R., Amarante Souza, A. C., & Aiello, V. D. (2020). Left Ventricular Noncompaction Is More Prevalent in Ventricular Septal Defect Than Other Congenital Heart Defects: A Morphological Study. Journal of Cardiovascular Development and Disease, 7(4), 39. https://doi.org/10.3390/jcdd7040039