
Efficacy and Safety of Iodixanol in Computed Coronary Tomographic Angiography and Cardiac Catheterization



Abstract
1. Introduction
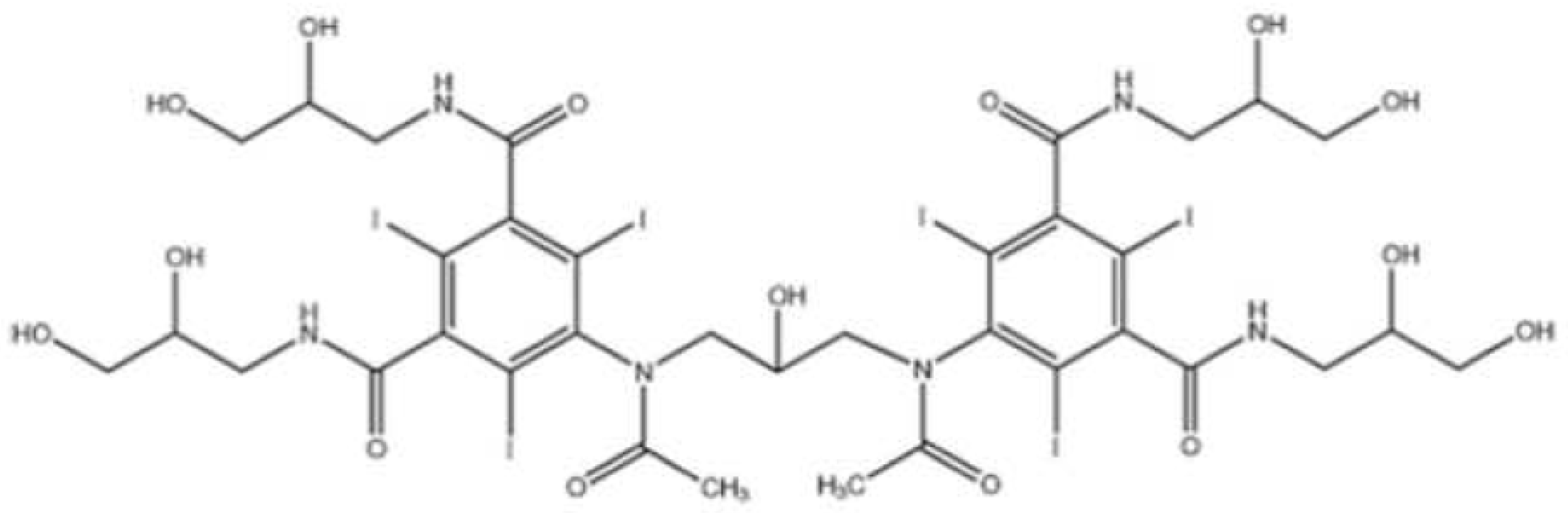
2. Pharmacological Properties
3. Image Quality
4. Tolerability and Safety
4.1. Pain and Discomfort
4.2. Flushing
4.3. Heart Rate Variability
5. Outcomes
5.1. Hemodynamic Changes and Cardiovascular Side Effects
5.2. Major Adverse Cardiovascular Event (MACE)
5.3. All-Cause Mortality
5.4. Contrast-Induced Nephropathy (CIN)
5.5. Hematological SDE
5.6. Neurological SDE
6. Cost-Effectiveness
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haschek, E.; Lindenthal, O.T. A contribution to the practical use of the photography according to Röntgen. Wien. Klin. Wochenschr. 1896, 9, 63. [Google Scholar]
- McClennan, B.L.; Stolberg, H.O. Intravascular contrast media. Ionic versus nonionic: Current status. Radiol. Clin. N. Am. 1991, 29, 437–454. [Google Scholar] [CrossRef] [PubMed]
- Spencer, C.M.; Goa, K.L. Iodixanol: A review of its pharmacodynamic and pharmacokinetic properties and diagnostic use as an x-ray contrast medium. Drugs 1996, 52, 899–927. [Google Scholar] [CrossRef] [PubMed]
- Binz-AaR, C. Uberbiochemische Eigenschaften von Derivaten des Pyridins und Chinolins. Biochem. Ztschr. 1928, 203, 218–222. [Google Scholar]
- Binz, A. The chemistry of uro-selectan. Br. J. Urol. 1930, 2, 348–351. [Google Scholar] [CrossRef]
- Pasternak, J.J.; Williamson, E.E. Clinical Pharmacology, Uses, and Adverse Reactions of Iodinated Contrast Agents: A Primer for the Non-radiologist. Mayo Clin. Proc. 2012, 87, 390–402. [Google Scholar] [CrossRef]
- Christensen, J.; Meyer, L.; Hurwitz, L.; Boll, D. Effects of iopamidol-370 versus iodixanol-320 on coronary contrast, branch depiction, and heart rate variability in dual-source coronary MDCT angiography. AJR Am. J. Roentgenol. 2011, 197, W445–W451. [Google Scholar] [CrossRef]
- Almén, T. Visipaque—A Step Forward: A historical review. Acta Radiol. 2016, 57, e47–e63. [Google Scholar] [CrossRef]
- Cademartiri, F.; Mollet, N.; van der Lugt, A.; McFadden, E.; Stijnen, T.; de Feyter, P.; Krestin, G. Intravenous contrast material administration at helical 16-detector row CT coronary angiography: Effect of iodine concentration on vascular attenuation. Radiology 2005, 236, 661–665. [Google Scholar] [CrossRef]
- Honoris, L.; Zhong, Y.; Chu, E.; Rosenthal, D.; Li, D.; Lam, F.; Budoff, M.J. Comparison of contrast enhancement, image quality and tolerability in Coronary CT angiography using 4 contrast agents: A prospective randomized trial. Int. J. Cardiol. 2015, 186, 126–128. [Google Scholar] [CrossRef]
- Lubbers, M.; Kock, M.; Niezen, A.; Galema, T.; Kofflard, M.; Bruning, T.; Kooij, H.; van Valen, H.; Dijkshoorn, M.; Booij, R.; et al. Iodixanol versus Iopromide at Coronary CT Angiography: Lumen Opacification and Effect on Heart Rhythm-the Randomized IsoCOR Trial. Radiology 2018, 286, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Huang, W.; Liu, W.; Zhu, Y.; Xu, Y.; Yang, G.; Tang, L.; Zhu, X. The Influence of Contrast Agent’s Osmolarity on Iodine Delivery Protocol in Coronary Computed Tomography Angiography: Comparison Between Iso-Osmolar Iodixanol-320 and Low-Osmolar Iomeprol-370. J. Comput. Assist. Tomogr. 2018, 42, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Tsai, I.C.; Lee, T.; Tsai, W.-L.; Chen, M.-C.; Wu, M.-J.; Lee, W.-L.; Ting, H.-J. Contrast enhancement in cardiac MDCT: Comparison of iodixanol 320 versus iohexol 350. AJR Am. J. Roentgenol. 2008, 190, W47–W53. [Google Scholar] [CrossRef] [PubMed]
- Pannu, H.K.; Thompson, R.E.; Phelps, J.; Magee, C.A.; Fishman, E.K. Optimal contrast agents for vascular imaging on computed tomography: Iodixanol versus iohexol. Acad. Radiol. 2005, 12, 576–584. [Google Scholar] [CrossRef]
- Choi, T.-Y.; Woo, V.; Gupta, M.; Sourayanezhad, S.; Li, D.; Mao, S.; Budoff, M. Comparison of iodixanol 320 and iohexol 350 in image quality during 64-slice multidetector computed tomography: Prospective randomized study. Int. J. Cardiol. 2012, 158, 134–138. [Google Scholar] [CrossRef]
- Budoff, M.; Bloom, S.; Chow, B.J.W.; Chandler, A.; Cole, J. Coronary computed tomography angiography predicts subsequent cardiac outcome events: Results of the Visipaque CCTA registry study. Coron. Artery Dis. 2015, 26, 301–307. [Google Scholar] [CrossRef]
- Budoff, M.; Dowe, D.; Jollis, J.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar]
- Budoff, M.; Li, D.; Kazerooni, E.; Thomas, G.; Mieres, J.; Shaw, L. Diagnostic Accuracy of Noninvasive 64-row Computed Tomographic Coronary Angiography (CCTA) Compared with Myocardial Perfusion Imaging (MPI): The PICTURE Study, A Prospective Multicenter Trial. Acad. Radiol. 2017, 24, 22–29. [Google Scholar] [CrossRef]
- Hill, J.A.; Cohen, M.B.; Kou, W.H.; Mancini, G.B.; Mansour, M.; Fountaine, H.; Brinker, J.A. Iodixanol, a new isosmotic nonionic contrast agent compared with iohexol in cardiac angiography. Am. J. Cardiol. 1994, 74, 57–63. [Google Scholar] [CrossRef]
- Andersen, P.E.; Bolstad, B.; Berg, K.J.; Justesen, P.; Thayssen, P.; Kloster, Y.F. Iodixanol and ioxaglate in cardioangiography: A double-blind randomized phase III study. Clin. Radiol. 1993, 48, 268–272. [Google Scholar] [CrossRef]
- Kløw, N.E.; Levorstad, K.; Berg, K.J.; Brodahl, U.; Endresen, K.; Kristoffersen, D.T.; Laake, B.; Simonsen, S.; Tofte, A.J.; Lundby, B. Iodixanol in cardioangiography in patients with coronary artery disease. Tolerability, cardiac and renal effects. Acta Radiol. 1993, 34, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, R.; Arsanjani, R.; Shalev, A.; Leipsic, J.; Gransar, H.; Lin, F.; Gomez, M.; Berman, D.; Min, J. Diagnostic Accuracy, Image Quality, and Patient Comfort for Coronary CT Angiography Performed Using Iso-Osmolar versus Low-Osmolar Iodinated Contrast: A Prospective International Multicenter Randomized Controlled Trial. Acad. Radiol. 2016, 23, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.W.; Barrett, B.J.; Parfrey, P.S. Contrast nephropathy. J. Am. Soc. Nephrol. 2000, 11, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Mao, S.S.; Zhuang, N.; Bakhsheshi, H.; Yamamoto, H.; Takasu, J.; Liu, S.C.; Budoff, M.J. Coronary artery motion during the cardiac cycle and optimal ECG triggering for coronary artery imaging. Investig. Radiol. 2001, 36, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Zhuang, N.; Mao, S.S.; Child, J.; Carson, S.; Budoff, M.J. Baseline heart rate-adjusted electrocardiographic triggering for coronary artery electron-beam CT angiography. Radiology 2004, 233, 590–595. [Google Scholar] [CrossRef]
- Flohr, T.G.; McCollough, C.H.; Bruder, H.; Petersilka, M.; Gruber, K.; Süss, C.; Grasruck, M.; Stierstorfer, K.; Krauss, B.; Raupach, R.; et al. First performance evaluation of a dual-source CT (DSCT) system. Eur. Radiol. 2006, 16, 256–268. [Google Scholar] [CrossRef]
- Giesler, T.; Baum, U.; Ropers, D.; Ulzheimer, S.; Wenkel, E.; Mennicke, M.; Bautz, W.; Kalender, W.A.; Daniel, W.G.; Achenbach, S. Noninvasive visualization of coronary arteries using contrast-enhanced multidetector CT: Influence of heart rate on image quality and stenosis detection. AJR Am. J. Roentgenol. 2002, 179, 911–916. [Google Scholar] [CrossRef]
- Hoffmann, M.H.; Shi, H.; Manzke, R.; Schmid, F.T.; De Vries, L.; Grass, M.; Brambs, H.J.; Aschoff, A.J. Noninvasive coronary angiography with 16-detector row CT: Effect of heart rate. Radiology 2005, 234, 86–97. [Google Scholar] [CrossRef]
- Chartrand Lefebvre, C.; White, C.; Bhalla, S.; Mayo Smith, W.; Prenovault, J.; Vydareny, K.; Soto, J.; Ozkan, O.; Chughtai, A.; Soulez, G. Comparison of the effect of low- and iso-osmolar contrast agents on heart rate during chest CT angiography: Results of a prospective randomized multicenter study. Radiology 2011, 258, 930–937. [Google Scholar] [CrossRef]
- Svensson, A.; Ripsweden, J.; Rück, A.; Aspelin, P.; Cederlund, K.; Brismar, B.T. Heart rate variability and heat sensation during CT coronary angiography: Low-osmolar versus iso-osmolar contrast media. Acta Radiol. 2010, 51, 722–726. [Google Scholar] [CrossRef]
- Roriz, R.; de Gevigney, G.; Finet, G.; Nantois-Collet, C.; Borch, K.W.; Amiel, M.; Beaune, J. Comparison of iodixanol (Visipaque) and ioxaglate (Hexabrix) in coronary angiography and ventriculography: A double-blind randomized study. J. Radiol. 1999, 80, 727–732. [Google Scholar] [PubMed]
- Schmid, I.; Didier, D.; Pfammatter, T.; Garachemani, A.; Fleisch, M.; Kirchin, M.; Meier, B. Effects of non-ionic iodinated contrast media on patient heart rate and pressures during intra-cardiac or intra-arterial injection. Int. J. Cardiol. 2007, 118, 389–396. [Google Scholar] [CrossRef]
- Tveit, K.; Bolz, K.D.; Bolstad, B.; Haugland, T.; Berg, K.J.; Skjaerpe, T.; Kloster, Y.F. Iodixanol in cardioangiography. A double-blind parallel comparison between iodixanol 320 mg I/mL and ioxaglate 320 mg I/mL. Acta Radiol. 1994, 35, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Juergens, C.P.; Winter, J.P.; Nguyen-Do, P.; Lo, S.; French, J.K.; Hallani, H.; Fernandes, C.; Jepson, N.; Leung, D.Y.C. Nephrotoxic effects of iodixanol and iopromide in patients with abnormal renal function receiving N-acetylcysteine and hydration before coronary angiography and intervention: A randomized trial. Intern. Med. J. 2008, 39, 25–31. [Google Scholar] [CrossRef]
- Bergstra, A.; van Dijk, R.B.; Brekke, O.; Buurma, A.E.; Orozco, L.; den Heijer, P.; Crijns, H.J. Hemodynamic effects of iodixanol and iohexol during ventriculography in patients with compromised left ventricular function. Catheter. Cardiovasc. Interv. 2000, 50, 314–321. [Google Scholar] [CrossRef]
- Xiao, Y.; Zeng, G.; Liu, X.; Peng, C.; Lai, C.; Zhou, P. Safety enhancement in adult body computed tomography scanning: Comparison of iodixanol versus iohexol. Springerplus 2016, 5, 148. [Google Scholar] [CrossRef]
- Qian, G.; Yang, Y.-Q.; Dong, W.; Cao, F.; Chen, Y.-D. Comparison of Iodixanol and Iopromide in Patients with Renal Insufficiency and Congestive Heart Failure Undergoing Coronary Angiography by Hemodynamic Monitoring. Angiology 2017, 68, 907–913. [Google Scholar] [CrossRef]
- Bertrand, M.E.; Esplugas, E.; Piessens, J.; Rasch, W. Influence of a nonionic, iso-osmolar contrast medium (iodixanol) versus an ionic, low-osmolar contrast medium (ioxaglate) on major adverse cardiac events in patients undergoing percutaneous transluminal coronary angioplasty: A multicenter, randomized, double-blind study. Visipaque in Percutaneous Transluminal Coronary Angioplasty [VIP] Trial Investigators. Circulation 2000, 101, 131–136. [Google Scholar]
- Davidson, C.J.; Laskey, W.K.; Hermiller, J.B.; Harrison, J.K.; Matthai, W.; Vlietstra, R.E.; Brinker, J.A.; Kereiakes, D.J.; Muhlestein, J.B.; Lansky, A.; et al. Randomized trial of contrast media utilization in high-risk PTCA: The COURT trial. Circulation 2000, 101, 2172–2177. [Google Scholar] [CrossRef]
- Giustino, G.; Baber, U.; Mastoris, I.; Vlachojannis, G.; Yu, J.; Teirstein, P.; Downey, W.; Batchelor, W.; Casterella, P.; Nikolsky, E.; et al. One-year results of the ICON (Ionic versus non-ionic Contrast to Obviate worsening Nephropathy after angioplasty in chronic renal failure patients) Study. Catheter. Cardiovasc. Interv. 2016, 87, 703–709. [Google Scholar] [CrossRef]
- Le Feuvre, C.; Batisse, A.; Collet, J.P.; Batisse, J.P.; Choussat, R.; Beygui, F.; Helft, G.; Montalescot, G.; Metzger, J.P. Cardiac events after low osmolar ionic or isosmolar nonionic contrast media utilization in the current era of coronary angioplasty. Catheter. Cardiovasc. Interv. 2006, 67, 852–858. [Google Scholar] [CrossRef] [PubMed]
- Bolognese, L.; Falsini, G.; Schwenke, C.; Grotti, S.; Limbruno, U.; Liistro, F.; Carrera, A.; Angioli, P.; Picchi, A.; Ducci, K.; et al. Impact of iso-osmolar versus low-osmolar contrast agents on contrast-induced nephropathy and tissue reperfusion in unselected patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention (from the Contrast Media and Nephrotoxicity Following Primary Angioplasty for Acute Myocardial Infarction [CONTRAST-AMI] Trial). Am. J. Cardiol. 2012, 109, 67–74. [Google Scholar] [PubMed]
- Harrison, J.B.H.; Vetrovec, G.W.; Smith, J.E.; Pulsipher, M.W.; Kern, M.J.; Conn, E.H.; Navetta, F.I.; She, L.; Pieper, K.; Sketch, M.H.; et al. A Randomized Study of 1276 Patients Undergoing PCI Using Iodixanol (Visipaque) vs Iopamidol (Isovue); Comparison of In-Hospital and 30 Day Major Adverse Cardiac Events. The Results of the VICC Trial. Circulation 2003, 108, 354–355. [Google Scholar]
- McCullough, P.; Bertrand, M.; Brinker, J.; Stacul, F. A meta-analysis of the renal safety of isosmolar iodixanol compared with low-osmolar contrast media. J. Am. Coll. Cardiol. 2006, 48, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Song, M.; Ge, Z.; Li, Y.; Shi, P.; Sun, M. Comparison of the nephrotoxic effects of iodixanol versus iohexol in patients with chronic heart failure undergoing coronary angiography or angioplasty. J. Interv. Cardiol. 2017, 30, 281–285. [Google Scholar] [CrossRef] [PubMed]
- From, A.M.; Bartholmai, B.J.; Williams, A.W.; McDonald, F.S. Iodixanol compared to iohexol for contrast procedures: A case-matched retrospective cohort study. Acta Radiol. 2008, 49, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Rudnick, M.R.; Goldfarb, S.; Wexler, L.; Ludbrook, P.A.; Murphy, M.J.; Halpern, E.F.; Hill, J.A.; Winniford, M.; Cohen, M.B.; VanFossen, D.B. Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: A randomized trial. The Iohexol Cooperative Study. Kidney Int. 1995, 47, 254–261. [Google Scholar] [CrossRef]
- Chalmers, N.; Jackson, R.W. Comparison of iodixanol and iohexol in renal impairment. Br. J. Radiol. 1999, 72, 701–703. [Google Scholar] [CrossRef]
- Aspelin, P.; Aubry, P.; Fransson, S.-G.; Strasser, R.; Willenbrock, R.; Berg, K. Nephrotoxic effects in high-risk patients undergoing angiography. N. Engl. J. Med. 2003, 348, 491–499. [Google Scholar] [CrossRef]
- Jo, S.-H.; Youn, T.-J.; Koo, B.-K.; Park, J.-S.; Kang, H.-J.; Cho, Y.-S.; Chung, W.-Y.; Joo, G.-W.; Chae, I.-H.; Choi, D.-J.; et al. Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: The RECOVER study: A randomized controlled trial. J. Am. Coll. Cardiol. 2006, 48, 924–930. [Google Scholar] [CrossRef]
- Mehran, R.; Nikolsky, E.; Kirtane, A.J.; Caixeta, A.; Wong, S.C.; Teirstein, P.S.; Downey, W.E.; Batchelor, W.B.; Casterella, P.J.; Kim, Y.H.; et al. Ionic low-osmolar versus nonionic iso-osmolar contrast media to obviate worsening nephropathy after angioplasty in chronic renal failure patients: The ICON (Ionic versus non-ionic Contrast to Obviate worsening Nephropathy after angioplasty in chronic renal failure patients) study. JACC Cardiovasc. Interv. 2009, 2, 415–421. [Google Scholar] [PubMed]
- Nie, B.; Cheng, W.-J.; Li, Y.-F.; Cao, Z.; Yang, Q.; Zhao, Y.-X.; Guo, Y.-H.; Zhou, Y.-J. A prospective, double-blind, randomized, controlled trial on the efficacy and cardiorenal safety of iodixanol vs. iopromide in patients with chronic kidney disease undergoing coronary angiography with or without percutaneous coronary intervention. Catheter. Cardiovasc. Interv. 2008, 72, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Hu, S.; Liu, Y.; Zhao, R.; Wang, L.; Fu, G.; He, Q.; Su, X.; Zheng, Y.; Qi, X.; et al. Renal tolerability of iopromide and iodixanol in 562 renally impaired patients undergoing cardiac catheterisation: The DIRECT study. EuroIntervention 2012, 8, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.J.; Natarajan, M.K.; Doucet, S.; Sharma, S.K.; Staniloae, C.S.; Katholi, R.E.; Gelormini, J.L.; Labinaz, M.; Moreyra, A.E. Cardiac Angiography in Renally Impaired Patients (CARE) study: A randomized double-blind trial of contrast-induced nephropathy in patients with chronic kidney disease. Circulation 2007, 115, 3189–3196. [Google Scholar] [CrossRef] [PubMed]
- Liss, P.; Persson, P.B.; Hansell, P.; Lagerqvist, B. Renal failure in 57 925 patients undergoing coronary procedures using iso-osmolar or low-osmolar contrast media. Kidney Int. 2006, 70, 1811–1817. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Choi, J.P.; Feghali, G.A.; Schussler, J.M.; Stoler, R.M.; Vallabahn, R.C.; Mehta, A. Contrast-Induced Acute Kidney Injury. J. Am. Coll. Cardiol. 2016, 68, 1465–1473. [Google Scholar] [CrossRef]
- Matschke, K.; Gerk, U.; Mrowietz, C.; Park, J.W.; Jung, F. Influence of radiographic contrast media on myocardial oxygen tension: A randomized, NaCl-controlled comparative study of iodixanol versus iomeprol in pigs. Acta Radiol. 2007, 48, 292–299. [Google Scholar] [CrossRef]
- Gerk, U.; Krüger, A.; Franke, R.P.; Jung, F. Effect of radiographic contrast media (Iodixanol, Iopromide) on hemolysis. Clin. Hemorheol. Microcirc. 2014, 58, 171–174. [Google Scholar] [CrossRef]
- Kerl, J.M.; Nguyen, S.A.; Lazarchick, J.; Powell, J.W.; Oswald, M.W.; Alvi, F.; Costello, P.; Vogl, T.J.; Schoepf, U.J. Iodinated contrast media: Effect of osmolarity and injection temperature on erythrocyte morphology in vitro. Acta Radiol. 2008, 49, 337–343. [Google Scholar] [CrossRef]
- Aulie Michelet, A. Effects of intravascular contrast media on blood-brain barrier. Comparison between iothalamate, iohexol, iopentol and iodixanol. Acta Radiol. 1987, 28, 329–333. [Google Scholar] [CrossRef]
- Iannazzo, S.; Vandekerckhove, S.; De Francesco, M.; Nayak, A.; Ronco, C.; Morana, G.; Valentino, M. Economic evaluation of intravenous iodinated contrast media in Italy. Int. J. Technol. Assess. Health Care 2014, 30, 69–77. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, M.; Ronco, C.; Wacinski, P.; Wessely, R.; Hernández, F.; Lamotte, M. Economic impact of contrast-induced acute kidney injury associated with invasive cardiology: Role of iso-osmolar contrast media in Germany, Italy, Poland, and Spain. J. Med Econ. 2016, 19, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K. Iodinated contrast media and contrast-induced nephropathy: Is there a preferred cost-effective agent? J. Invasive Cardiol. 2008, 20, 245–248. [Google Scholar] [PubMed]
- Keuffel, E.; McCullough, P.A.; Todoran, T.M.; Brilakis, E.S.; Palli, S.R.; Ryan, M.P.; Gunnarsson, C. The effect of major adverse renal cardiovascular event (MARCE) incidence, procedure volume, and unit cost on the hospital savings resulting from contrast media use in inpatient angioplasty. J. Med. Econ. 2018, 21, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Bottinor, W.; Polkampally, P.; Jovin, I. Adverse Reactions to Iodinated Contrast Media. Int. J. Angiol. 2013, 22, 149–154. [Google Scholar]
- Buttan, A.K.; Yang, E.H.; Budoff, M.J.; Vorobiof, G. Evaluation of valvular disease by cardiac computed tomography assessment. J. Cardiov. Comp. Tomo 2014, 6, 381–392. [Google Scholar] [CrossRef]
- Budoff, M.J.; Kalia, N.; Cole, J.; Nakanishi, R.; Nezarat, N.; Thomas, J.L. Diagnostic accuracy of Visipaque enhanced coronary computed tomographic angiography: A prospective multicenter trial. Coron. Artery Dis. 2017, 28, 52–56. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Randomized | Number of Patients | Mean Age | Contrast | Endpoints | Results |
|---|---|---|---|---|---|---|
| Lily Honoris et al., 2017 [10] | Yes | N = 513 | 57 ± 11 | Iodixanol Iohexol Iopamidol | Flushing | Iodixanol superior |
| Xiao et al., 2016 [36] | Yes | N = 2000 | 52 ± 13.3 | Iodixanol 320 Iohexol | Urticaria and nausea | Iodixanol superior |
| Carlartrand-Lefebvre et al., 2011 [29] | Yes | N = 130 | 52 ± 16 | Iopamido Iodixanol 320 | HR | No difference |
| Jared D. Christensen et al., 2011 [7] | Yes | N = 60 | 53.5 ± 15.1 | Iodixanol 320 Iopamidol 370 | HR | No difference |
| Ryo Nakazato, et al., 2016 [22] | Yes | N = 266 | 57.2 ± 11.7 | Iodixanol Iopamidol | HR Flushing | No difference No difference |
| Choi et al., 2012 [15] | Yes | N = 300 | 62 ± 11 | Iodixanol 320 Iohexol 350 | HR | Iodixanol superior |
| Study | Number of Pts | Mean Age | Contrast | Endpoint | Results |
|---|---|---|---|---|---|
| Qian et al., 2017 [37] | N = 90 | 62 ± 13 | Iodixanol Iopromide | 90-Day cardiac event Acute heart failure | Iodixanol superior No difference |
| Bertrand et al., 2000 [38] | N = 1411 | 61.6 ± 10.6 | Iodixanol Ioxaglate | Acute renal failure | No difference |
| Davidson et al., 2000 [39] | N = 810 | 61 ± 12 | Iodixanol Ioxaglate | During hospital stay 30-Day cardiac event | Iodixanol superior No difference |
| Harrison et al., 2003 [43] | N = 1276 | - | Iodixanol Iopamidol | In-hospital 30-Day cardiac event | Iodixanol superior No difference |
| Giustino et al., 2016 [40] | N = 146 | 71.6 ± 9.9 | Iodixanol Ioxaglate | ARF 30-Day events | No difference No difference |
| Song T2 et al., 2017 [45] | N = 220 | 54.1 ± 9.8 | Iodixanol Iohexanol | ARF | Iodixanol superior |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budoff, M.J.; Lee, H.S.; Roy, S.K.; Shekar, C. Efficacy and Safety of Iodixanol in Computed Coronary Tomographic Angiography and Cardiac Catheterization. J. Cardiovasc. Dev. Dis. 2023, 10, 449. https://doi.org/10.3390/jcdd10110449
Budoff MJ, Lee HS, Roy SK, Shekar C. Efficacy and Safety of Iodixanol in Computed Coronary Tomographic Angiography and Cardiac Catheterization. Journal of Cardiovascular Development and Disease. 2023; 10(11):449. https://doi.org/10.3390/jcdd10110449
Chicago/Turabian StyleBudoff, Matthew J., Hong Seok Lee, Sion K. Roy, and Chandana Shekar. 2023. "Efficacy and Safety of Iodixanol in Computed Coronary Tomographic Angiography and Cardiac Catheterization" Journal of Cardiovascular Development and Disease 10, no. 11: 449. https://doi.org/10.3390/jcdd10110449
APA StyleBudoff, M. J., Lee, H. S., Roy, S. K., & Shekar, C. (2023). Efficacy and Safety of Iodixanol in Computed Coronary Tomographic Angiography and Cardiac Catheterization. Journal of Cardiovascular Development and Disease, 10(11), 449. https://doi.org/10.3390/jcdd10110449