
Body Weight, BMI, Percent Fat and Associations with Mortality and Incident Mobility Limitation in Older Men

 , , ,
, , ,
Abstract
1. Introduction
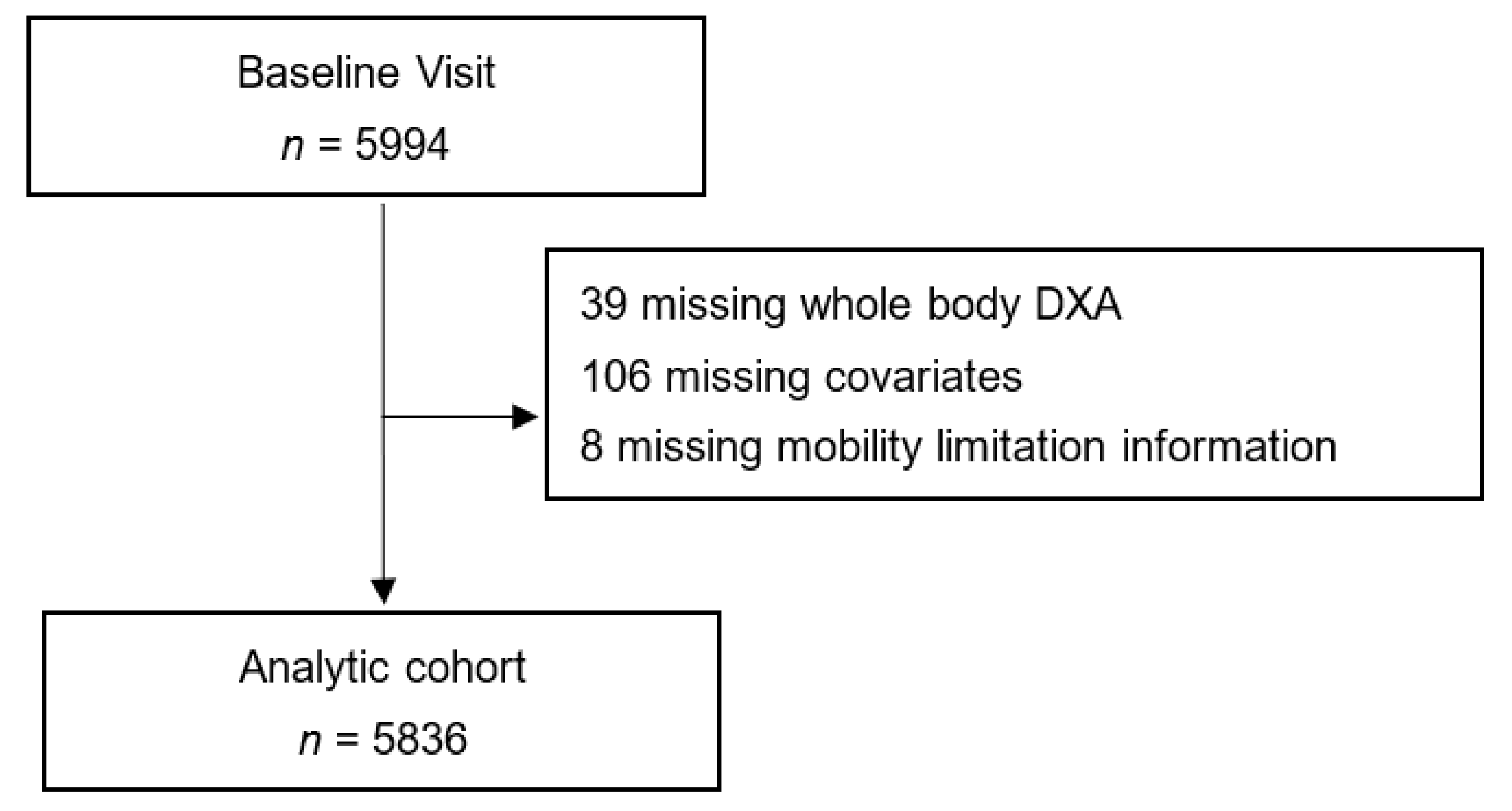
2. Materials and Methods
2.1. BMI, Weight, Percent Fat and Total Energy Intake
2.2. Mobility Limitation
2.3. Mortality
2.4. Clinical Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Participants
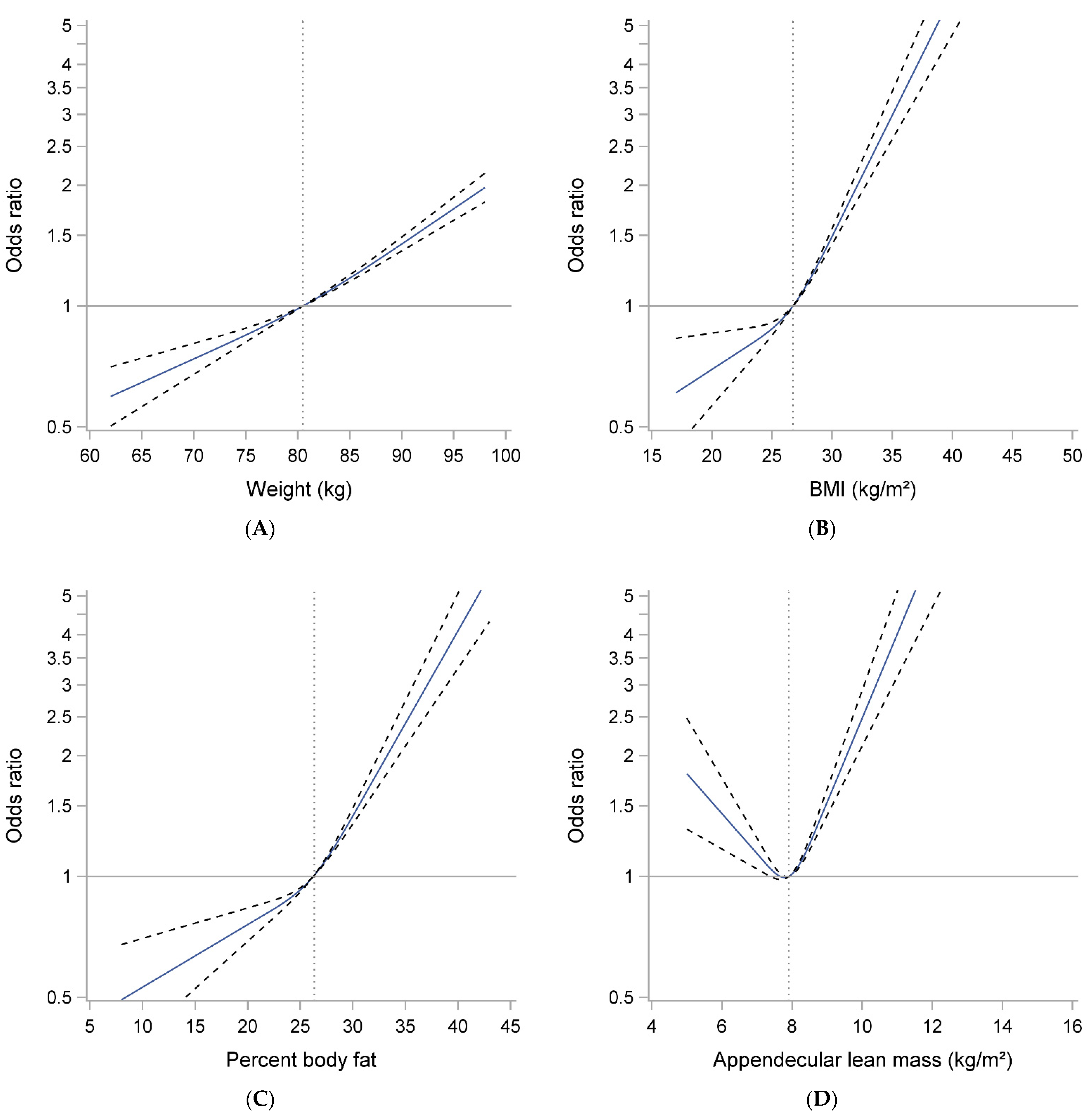
3.2. Weight, BMI, Percent Body Fat, ALM/ht2 and Likelihood of Mobility Limitation
3.3. Weight, BMI, Percent Body Fat, ALM/ht2 and Risk of Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of Obesity among Adults and Youth: United States, 2011–2014; NCHS Data Brief; National Center for Health Statistics: Hyattsville, MD, USA, 2015; pp. 1–8. [Google Scholar]
- Peeters, A.; Bonneux, L.; Nusselder, W.J.; De Laet, C.; Barendregt, J.J. Adult obesity and the burden of disability throughout life. Obes. Res. 2004, 12, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Zaslavsky, O.; Rillamas-Sun, E.; LaCroix, A.Z.; Woods, N.F.; Tinker, L.F.; Zisberg, A.; Shadmi, E.; Cochrane, B.; Edward, B.J.; Kritchevsky, S.; et al. Association Between Anthropometric Measures and Long-Term Survival in Frail Older Women: Observations from the Women’s Health Initiative Study. J. Am. Geriatr. Soc. 2016, 64, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Pischon, T.; Boeing, H.; Hoffmann, K.; Bergmann, M.; Schulze, M.B.; Overvad, K.; van der Schouw, Y.T.; Spencer, E.; Moons, K.G.; Tjonneland, A.; et al. General and abdominal adiposity and risk of death in Europe. N. Engl. J. Med. 2008, 359, 2105–2120. [Google Scholar] [CrossRef]
- Bea, J.W.; Thomson, C.A.; Wertheim, B.C.; Nicholas, J.S.; Ernst, K.C.; Hu, C.; Jackson, R.D.; Cauley, J.A.; Lewis, C.E.; Caan, B.; et al. Risk of Mortality According to Body Mass Index and Body Composition Among Postmenopausal Women. Am. J. Epidemiol. 2015, 182, 585–596. [Google Scholar] [CrossRef]
- Janssen, I.; Mark, A.E. Elevated body mass index and mortality risk in the elderly. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2007, 8, 41–59. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and all-cause mortality in older adults: A meta-analysis. Am. J. Clin. Nutr. 2014, 99, 875–890. [Google Scholar] [CrossRef]
- Bowman, K.; Atkins, J.L.; Delgado, J.; Kos, K.; Kuchel, G.A.; Ble, A.; Ferrucci, L.; Melzer, D. Central adiposity and the overweight risk paradox in aging: Follow-up of 130,473 UK Biobank participants. Am. J. Clin. Nutr. 2017, 106, 130–135. [Google Scholar] [CrossRef]
- Bowman, K.; Delgado, J.; Henley, W.E.; Masoli, J.A.; Kos, K.; Brayne, C.; Thokala, P.; Lafortune, L.; Kuchel, G.A.; Ble, A.; et al. Obesity in Older People with and Without Conditions Associated with Weight Loss: Follow-up of 955,000 Primary Care Patients. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G.; Lennon, L. Reasons for intentional weight loss, unintentional weight loss, and mortality in older men. Arch. Intern. Med. 2005, 165, 1035–1040. [Google Scholar] [CrossRef]
- Newman, A.B.; Yanez, D.; Harris, T.; Duxbury, A.; Enright, P.L.; Fried, L.P. Weight change in old age and its association with mortality. J. Am. Geriatr. Soc. 2001, 49, 1309–1318. [Google Scholar] [CrossRef]
- Payette, H.; Coulombe, C.; Boutier, V.; Gray-Donald, K. Weight loss and mortality among free-living frail elders: A prospective study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1999, 54, M440–M445. [Google Scholar] [CrossRef]
- Kritchevsky, S.B.; Beavers, K.M.; Miller, M.E.; Shea, M.K.; Houston, D.K.; Kitzman, D.W.; Nicklas, B.J. Intentional weight loss and all-cause mortality: A meta-analysis of randomized clinical trials. PLoS ONE 2015, 10, e0121993. [Google Scholar] [CrossRef]
- Brown, C.J.; Flood, K.L. Mobility limitation in the older patient: A clinical review. JAMA 2013, 310, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Hillier, T.A.; Lui, L.Y.; Kado, D.M.; Leblanc, E.; Vesco, K.K.; Bauer, D.C.; Cauley, J.A.; Ensrud, K.E.; Black, D.M.; Hochberg, M.C.; et al. Height loss in older women: Risk of hip fracture and mortality independent of vertebral fractures. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2011. [Google Scholar] [CrossRef]
- Snijder, M.B.; van Dam, R.M.; Visser, M.; Seidell, J.C. What aspects of body fat are particularly hazardous and how do we measure them? Int. J. Epidemiol. 2006, 35, 83–92. [Google Scholar] [CrossRef]
- Visser, M.; Harris, T.B.; Langlois, J.; Hannan, M.T.; Roubenoff, R.; Felson, D.T.; Wilson, P.W.; Kiel, D.P. Body fat and skeletal muscle mass in relation to physical disability in very old men and women of the Framingham Heart Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1998, 53, M214–221. [Google Scholar] [CrossRef] [PubMed]
- Koster, A.; Patel, K.V.; Visser, M.; van Eijk, J.T.; Kanaya, A.M.; de Rekeneire, N.; Newman, A.B.; Tylavsky, F.A.; Kritchevsky, S.B.; Harris, T.B. Joint effects of adiposity and physical activity on incident mobility limitation in older adults. J. Am. Geriatr. Soc. 2008, 56, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.K.; Velkoff, V.A. The Next Four Decades, the Older Population in the United States: 2010 to 2050; Current Population Reports; U.S. Census Bureau: Washington, DC, USA, 2010; pp. 25–1138.
- Batsis, J.A.; Mackenzie, T.A.; Barre, L.K.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity and mortality in older adults: Results from the National Health and Nutrition Examination Survey III. Eur. J. Clin. Nutr. 2014. [Google Scholar] [CrossRef]
- Batsis, J.A.; Mackenzie, T.A.; Emeny, R.T.; Lopez-Jimenez, F.; Bartels, S.J. Low Lean Mass with and without Obesity, and Mortality: Results From the 1999-2004 National Health and Nutrition Examination Survey. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Padwal, R.; Leslie, W.D.; Lix, L.M.; Majumdar, S.R. Relationship Among Body Fat Percentage, Body Mass Index, and All-Cause Mortality: A Cohort Study. Ann. Intern. Med. 2016, 164, 532–541. [Google Scholar] [CrossRef]
- Androga, L.; Sharma, D.; Amodu, A.; Abramowitz, M.K. Sarcopenia, obesity, and mortality in US adults with and without chronic kidney disease. Kidney Int. Rep. 2017, 2, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Hao, Q.; Hai, S.; Wang, H.; Cao, L.; Dong, B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas 2017, 103, 16–22. [Google Scholar] [CrossRef]
- Blank, J.B.; Cawthon, P.M.; Carrion-Petersen, M.L.; Harper, L.; Johnson, J.P.; Mitson, E.; Delay, R.R. Overview of recruitment for the osteoporotic fractures in men study (MrOS). Contemp. Clin. Trials 2005, 26, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Orwoll, E.; Blank, J.B.; Barrett-Connor, E.; Cauley, J.; Cummings, S.; Ensrud, K.; Lewis, C.; Cawthon, P.M.; Marcus, R.; Marshall, L.M.; et al. Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study—A large observational study of the determinants of fracture in older men. Contemp. Clin. Trials 2005, 26, 569–585. [Google Scholar] [CrossRef] [PubMed]
- Boucher, B.; Cotterchio, M.; Kreiger, N.; Nadalin, V.; Block, T.; Block, G. Validity and reliability of the Block98 food-frequency questionnaire in a sample of Canadian women. Public Health Nutr. 2006, 9, 84–93. [Google Scholar] [CrossRef]
- Johnson, B.A.; Herring, A.H.; Ibrahim, J.G.; Siega-Riz, A.M. Structured measurement error in nutritional epidemiology: Applications in the Pregnancy, Infection, and Nutrition (PIN) Study. J. Am. Stat. Assoc. 2007, 102, 856–866. [Google Scholar] [CrossRef]
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The Physical Activity Scale for the Elderly (PASE): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Fullman, R.L.; Marshall, L.; Mackey, D.C.; Fink, H.A.; Cauley, J.A.; Cummings, S.R.; Orwoll, E.S.; Ensrud, K.E. Physical performance and risk of hip fractures in older men. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2008, 23, 1037–1044. [Google Scholar] [CrossRef]
- Abramowitz, M.K.; Hall, C.B.; Amodu, A.; Sharma, D.; Androga, L.; Hawkins, M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study. PLoS ONE 2018, 13, e0194697. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fieding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. The Authors reply: "Dual energy X-ray absorptiometry: Gold standard for muscle mass?" by Scafoglieri et al. J. Cachexia Sarcopenia Muscle 2018. [Google Scholar] [CrossRef]
- Scafoglieri, A.; Clarys, J.P. Dual energy X-ray absorptiometry: Gold standard for muscle mass? J. Cachexia Sarcopenia Muscle 2018. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Orwoll, E.S.; Peters, K.E.; Ensrud, K.E.; Cauley, J.A.; Kado, D.M.; Stefanick, M.L.; Shikany, J.M.; Strotmeyer, E.S.; Glynn, N.W.; et al. Strong Relation Between Muscle Mass Determined by D3-creatine Dilution, Physical Performance, and Incidence of Falls and Mobility Limitations in a Prospective Cohort of Older Men. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 844–852. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| N (%), or Mean ± SD | Baseline Weight (kg) Quintiles | p-Value | ||||
|---|---|---|---|---|---|---|
| Q1: | Q2: | Q3: | Q4: | Q5: | ||
| N = 1150 | N = 1156 | N = 1192 | N = 1156 | N = 1187 | ||
| Age, years | 76.0 ± 6.5 | 74.5 ± 5.8 | 73.3 ± 5.6 | 72.7 ± 5.4 | 71.6 ± 4.9 | <0.001 |
| Non-Hispanic White | 956 (83.1) | 1054 (91.2) | 1089 (91.4) | 1060 (91.7) | 1083 (91.2) | <0.001 |
| Married (vs. not) | 920 (80.0) | 961 (83.1) | 1003 (84.1) | 951 (82.3) | 972 (81.9) | 0.105 |
| College educated (vs. < college) | 905 (78.7) | 908 (78.6) | 910 (76.3) | 864 (74.7) | 871 (73.4) | 0.007 |
| Ever smoker (vs. never) | 636 (55.3) | 684 (59.2) | 765 (64.2) | 765 (66.2) | 800 (67.4) | <0.001 |
| Drinks per day, >2 (vs ≤2) | 127 (11.1) | 126 (10.9) | 151 (12.7) | 135 (11.7) | 138 (11.7) | 0.685 |
| Height, m | 1.69 ± 0.1 | 1.72 ± 0.1 | 1.74 ± 0.1 | 1.77 ± 0.1 | 1.79 ± 0.1 | <0.001 |
| Weight, kg | 66.5 ± 4.4 | 75.3 ± 1.9 | 81.7 ± 1.9 | 88.9 ± 2.4 | 102.9 ± 8.5 | <0.001 |
| Body mass index, kg/m2 | 23.3 ± 1.9 | 25.4 ± 1.7 | 27.0 ± 1.8 | 28.6 ± 2.0 | 32.4 ± 3.4 | <0.001 |
| Percent body fat | 21.9 ± 4.8 | 24.5 ± 4.3 | 25.9 ± 4.3 | 27.7 ± 4.3 | 31.0 ± 4.5 | <0.001 |
| ALM/height2 (kg/m2) | 7.2 ± 0.7 | 7.6 ± 0.7 | 8.0 ± 0.7 | 8.2 ± 0.7 | 8.9 ± 0.9 | <0.001 |
| Comorbidities | 0.003 | |||||
| 0 | 340 (29.6) | 343 (30.0) | 336 (28.2) | 308 (26.6) | 293 (24.7) | |
| 1 | 396 (34.3) | 405 (35.0) | 386 (32.4) | 432 (37.4) | 394 (33.2) | |
| 2+ | 414 (36.0) | 408 (35.3) | 470 (39.4) | 416 (35.9) | 500 (42.1) | |
| PASE score | 144.6 ± 70.4 | 145.7 ± 65.1 | 152.3 ± 68.9 | 148.0 ± 66.4 | 143.8 ± 69.1 | 0.019 |
| Walk speed (m/s) | 1.18 ± 0.2 | 1.22 ± 0.2 | 1.22 ± 0.2 | 1.21 ± 0.2 | 1.18 ± 0.2 | <0.001 |
| Total energy intake (kcal) | 1545 ± 574 | 1553 ± 546 | 1611 ± 611 | 1685 ± 674 | 1746 ± 723 | <0.001 |
| Incident obility limitation | 435 (37.8) | 511 (44.2) | 547 (47.3) | 591 (51.1) | 718 (60.5) | 0.003 |
| Died during follow-up | 427 (37.1) | 321 (27.8) | 280 (23.5) | 293 (25.4) | 303 (25.5) | <0.001 |
| Mobility Limitation (N = 2802 of 5841) | Mortality (N = 1630 of 5849) | |
|---|---|---|
| Weight (kg) | ||
| Quintile 1 (<70.7 kg) | 1.00 (referent) | 1.45 (1.23, 1.70) |
| Quintile 2 (70.7–77.3 kg) | 1.48 (1.27, 1.72) | 1.11 (0.94, 1.70) |
| Quintile 3 (77.3–84.0 kg) | 1.61 (1.38, 1.87) | 1.00 (referent) |
| Quintile 4 (84.0–92.4 kg) | 2.15 (1.83, 2.51) | 1.15 (0.98, 1.35) |
| Quintile 5 (>92.4 kg) | 3.60 (3.04, 4.25) | 1.29 (1.09, 1.53) |
| BMI (kg/m2) | ||
| Quintile 1 (<24.0 kg/m2) | 1.00 (referent) | 1.32 (1.13, 1.540) |
| Quintile 2 (24.0–<25.9 kg/m2) | 1.23 (1.06, 1.42) | 1.03 (0.88, 1.20) |
| Quintile 3 (25.9–<27.8 kg/m2) | 1.31 (1.13, 1.52) | 1.00 (referent) |
| Quintile 4 (27.8–<30.2 kg/m2) | 1.68 (1.46, 1.94) | 0.95 (0.81, 1.13) |
| Quintile 5 (≥30.2 kg/m2) | 2.83 (2.45, 3.27) | 1.30 (1.12, 1.53) |
| % body fat | ||
| Quintile 1 (<21.8) | 1.00 (referent) | 1.07 (0.92, 1.25) |
| Quintile 2 (21.8–<24.9) | 1.07 (0.93, 1.25) | 0.94 (0.80, 1.10) |
| Quintile 3 (24.9–<27.6) | 1.19 (1.03, 1.38) | 1.00 (referent) |
| Quintile 4 (27.6–<30.7) | 1.34 (1.15, 1.56) | 0.92 (0.79, 1.07) |
| Quintile 5 (≥30.7) | 1.86 (1.57, 2.20) | 1.03 (0.88, 1.19) |
| ALM/ht2 | ||
| Quintile 1 (<7.21 kg/ht2) | 1.00 (referent) | 1.38 (1.18, 1.60) |
| Quintile 2 (7.21–<7.70 kg/ht2) | 0.95 (0.82, 1.10) | 1.04 (0.88, 1.22) |
| Quintile 3 (7.70–<8.13 kg/ht2) | 0.93 (0.81, 1.08) | 1.00 (referent) |
| Quintile 4 (8.13–<8.71 kg/ht2) | 1.05 (0.90, 1.21) | 1.01 (0.85, 1.19) |
| Quintile 5 (≥8.71 kg/ht2) | 1.56 (1.35, 1.81) | 1.15 (0.97, 1.36) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cawthon, P.M.; Harrison, S.L.; Rogers-Soeder, T.; Webber, K.; Jonnalagadda, S.; Pereira, S.L.; Lane, N.; Cauley, J.A.; Shikany, J.M.; Farsijani, S.; et al. Body Weight, BMI, Percent Fat and Associations with Mortality and Incident Mobility Limitation in Older Men. Geriatrics 2021, 6, 53. https://doi.org/10.3390/geriatrics6020053
Cawthon PM, Harrison SL, Rogers-Soeder T, Webber K, Jonnalagadda S, Pereira SL, Lane N, Cauley JA, Shikany JM, Farsijani S, et al. Body Weight, BMI, Percent Fat and Associations with Mortality and Incident Mobility Limitation in Older Men. Geriatrics. 2021; 6(2):53. https://doi.org/10.3390/geriatrics6020053
Chicago/Turabian StyleCawthon, Peggy M., Stephanie L. Harrison, Tara Rogers-Soeder, Katey Webber, Satya Jonnalagadda, Suzette L. Pereira, Nancy Lane, Jane A. Cauley, James M. Shikany, Samaneh Farsijani, and et al. 2021. "Body Weight, BMI, Percent Fat and Associations with Mortality and Incident Mobility Limitation in Older Men" Geriatrics 6, no. 2: 53. https://doi.org/10.3390/geriatrics6020053
APA StyleCawthon, P. M., Harrison, S. L., Rogers-Soeder, T., Webber, K., Jonnalagadda, S., Pereira, S. L., Lane, N., Cauley, J. A., Shikany, J. M., Farsijani, S., & Langsetmo, L. (2021). Body Weight, BMI, Percent Fat and Associations with Mortality and Incident Mobility Limitation in Older Men. Geriatrics, 6(2), 53. https://doi.org/10.3390/geriatrics6020053