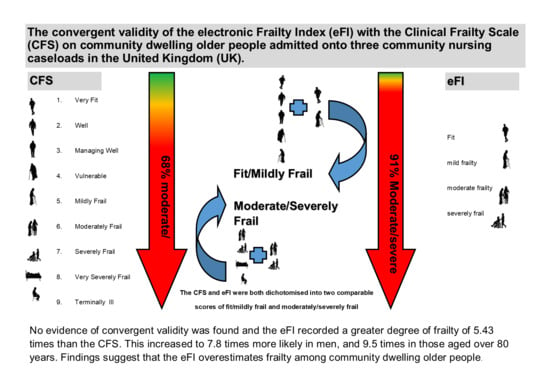
The Convergent Validity of the electronic Frailty Index (eFI) with the Clinical Frailty Scale (CFS)


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Measures
2.4. Scoring Frailty
2.4.1. eFI
2.4.2. CFS
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Clegg, A.; Rogers, L.; Young, J. Diagnostic test accuracy of simple instruments for identifying frailty in community-dwelling older people: A systematic review. Age Ageing 2014, 44, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Gan, P.; How, C.H. Approach to frailty in the elderly in primary care and the community. Singap. Med. J. 2018, 59, 240–245. [Google Scholar] [CrossRef] [PubMed]
- John, P.D.S.; McClement, S.S.; Swift, A.U.; Tate, R.B. Older Men’s Definitions of Frailty—The Manitoba Follow-up Study. Can. J. Aging 2018, 38, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Gilardi, F.; Capanna, A.; Ferraro, M.; Scarcella, P.; Marazzi, M.C.; Palombi, L.; Liotta, G. Frailty screening and assessment tools: A review of characteristics and use in Public Health. Ann. Ig. 2018, 30, 128–139. [Google Scholar] [PubMed]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur. J. Intern. Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- British Geriatric Society (BGS). Comprehensive Geriatric Assessment Toolkit for Primary Care Practitioners (online). 2019. Available online: https://www.bgs.org.uk/resources/resource-series/comprehensive-geriatric-assessment-toolkit-for-primary-care-practitioners (accessed on 10 July 2020).
- NHS England. NHS Long Term Plan (online). 2019. Available online: https://www.longtermplan.nhs.uk/online-version/ (accessed on 4 July 2020).
- NHS England. Supporting Routine Frailty Identification and Frailty through the GP Contract 2017/2018 (online). 2019. Available online: https://www.england.nhs.uk/publication/supporting-routine-frailty-identification-and-frailty-through-the-gp-contract-20172018/ (accessed on 7 July 2020).
- Stow, D.; Matthews, F.E.; Barclay, S.; Iliffe, S.; Clegg, A.; De Biase, S.; Robinson, L.; Hanratty, B. Evaluating frailty scores to predict mortality in older adults using data from population based electronic health records: Case control study. Age Ageing 2018, 47, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Long, S.; Jelley, B.; Martin, R.; Suter-Jones, V.E. Underestimation of frailty using the 7-point Clinical Frailty Scale: An evaluation of geriatric registrar scoring accuracy. Age Ageing 2018, 47, ii25–ii39. [Google Scholar] [CrossRef]
- Clegg, A.P.; Bates, C.; Young, J.; Ryan, R.; Nichols, L.; Teale, E.A.; Mohammed, M.A.; Parry, J.; Marshall, T. Development and validation of an electronic frailty index using routine primary care electronic health record data. Age Ageing 2016, 45, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; Macknight, C.; Bergman, H.; Hogan, D.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. Can. Med Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Ozsurekci, C.; Balcı, C.; Kızılarslanoğlu, M.C.; Çalışkan, H.; Doğrul, R.T.; Ayçiçek, G. Şengül; Sümer, F.; Karabulut, E.; Yavuz, B.B.; Cankurtaran, M.; et al. An important problem in an aging country: Identifying the frailty via 9 Point Clinical Frailty Scale. Acta Clin. Belg. 2019, 75, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Owen, R.K.; Conroy, S.P.; Taub, N.; Jones, W.; Bryden, D.; Pareek, M.; Faull, C.; Abrams, K.R.; Davis, D.; Banerjee, J. OUP accepted manuscript. Age Ageing 2020. [Google Scholar] [CrossRef]
- Aw, D.; Woodrow, L.; Ogliari, G.; Harwood, R. Association of frailty with mortality in older inpatients with Covid-19: A cohort study. Age Ageing 2020. [Google Scholar] [CrossRef] [PubMed]
- Upton, G.J.; Cook, I. A Dictionary of Statistics; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Brundle, C.; Heaven, A.; Brown, L.; Teale, E.; Young, J.; West, R.; Clegg, A. Convergent validity of the electronic frailty index. Age Ageing 2018, 48, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, M.; Khera, S.; Dabravolskaj, J.; Vandermeer, B.; Theou, O.; Rolfson, D.; Clegg, A. A cross-sectional study examining convergent validityof a frailty index based on electronic medical records in a Canadian primary care program. BMC Geriatr. 2019, 19, 109. [Google Scholar]
- Lansbury, L.N.; Roberts, H.C.; Clift, E.; Herklots, A.; Robinson, N.; Sayer, A.A. Use of the electronic Frailty Index to identify vulnerable patients: A pilot study in primary care. Br. J. Gen. Pr. 2017, 67, e751–e756. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef]
- Elliott, A.; Phelps, K.; Regen, E.; Conroy, S.P. Identifying frailty in the Emergency Department—Feasibility study. Age Ageing 2017, 46, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Hale, M.D.; Santorelli, G.; Brundle, C.; Clegg, A. A cross-sectional study assessing agreement between self-reported and general practice-recorded health conditions among community dwelling older adults. Age Ageing 2019, 49, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Dean, M.; Liu, T.; George, L.; Gann, M.; Cohen, J.; Bruce, M.L. Physical and mental health of homebound older adults: An overlooked population. J. Am. Geriatr. Soc. 2010, 58, 2423–2428. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Category of frailty | eFI | CFS | ||
|---|---|---|---|---|
| Fit/Mild | Moderate/Severe | Fit/Mild | Moderate/Severe | |
| Total patients | 23 (9%) | 242 (91%) | 85 (32%) | 180 (68%) |
| Age (mean) | 80.7 | 86 | 84.8 | 85.95 |
| Male | 10 (43%) | 105 (43%) | 43 (51%) | 72 (40%) |
| Female | 13 (57%) | 137 (57%) | 42 (49%) | 108 (60%) |
| CFS | ||||
|---|---|---|---|---|
| eFI | Category of frailty | Fit to Mild | Moderate to Severe | Total |
| Fit to Mild | 9 | 14 | 23 | |
| Moderate to severe | 76 | 166 | 242 | |
| Total | 85 | 180 | 265 | |
| ≤80 years | CFS | ||
|---|---|---|---|
| eFI | Mild/fit | Moderate/severe | Total |
| Mild/fit | 4 (a) | 8 (b) | 12 (a + b) |
| Moderate/severe | 19 (c) | 39 (d) | 58 (c + d) |
| total | 23 (a + c) | 47 (b + d) | 70 |
| >80 years | CFS | ||
| eFI | Mild/fit | Moderate/severe | Total |
| Mild/fit | 5 (a) | 6 (b) | 11 (a + b) |
| Moderate/severe | 57 (c) | 127 (d) | 184 (c + d) |
| total | 62 (a + c) | 133 (b + d) | 195 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Broad, A.; Carter, B.; Mckelvie, S.; Hewitt, J. The Convergent Validity of the electronic Frailty Index (eFI) with the Clinical Frailty Scale (CFS). Geriatrics 2020, 5, 88. https://doi.org/10.3390/geriatrics5040088
Broad A, Carter B, Mckelvie S, Hewitt J. The Convergent Validity of the electronic Frailty Index (eFI) with the Clinical Frailty Scale (CFS). Geriatrics. 2020; 5(4):88. https://doi.org/10.3390/geriatrics5040088
Chicago/Turabian StyleBroad, Antoinette, Ben Carter, Sara Mckelvie, and Jonathan Hewitt. 2020. "The Convergent Validity of the electronic Frailty Index (eFI) with the Clinical Frailty Scale (CFS)" Geriatrics 5, no. 4: 88. https://doi.org/10.3390/geriatrics5040088
APA StyleBroad, A., Carter, B., Mckelvie, S., & Hewitt, J. (2020). The Convergent Validity of the electronic Frailty Index (eFI) with the Clinical Frailty Scale (CFS). Geriatrics, 5(4), 88. https://doi.org/10.3390/geriatrics5040088