
Stroke and Falls—Clash of the Two Titans in Geriatrics


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Epidemiology of Falls in Stroke
4. Risk Factors
4.1. Stroke-Related Deficits
4.1.1. Motor Deficits
4.1.2. Mobility and Dependency Level Post-Stroke
4.1.3. Sensory
4.1.4. Visual
4.1.5. Perception/Abstract Thinking
4.1.6. Cognitive Function
4.1.7. Cerebellar and Vestibular Function
4.2. Cardiovascular Risk factors
4.2.1. Atrial Fibrillation
4.2.2. Hypotensive Disorders
4.3. Psychological Risk Factors
4.4. Medications
4.4.1. Blood Pressure Lowering Therapy
4.4.2. Anticholinergic Burden
4.4.3. Falls Risk Increasing Drugs
4.4.4. Anticoagulation
4.5. Epilepsy
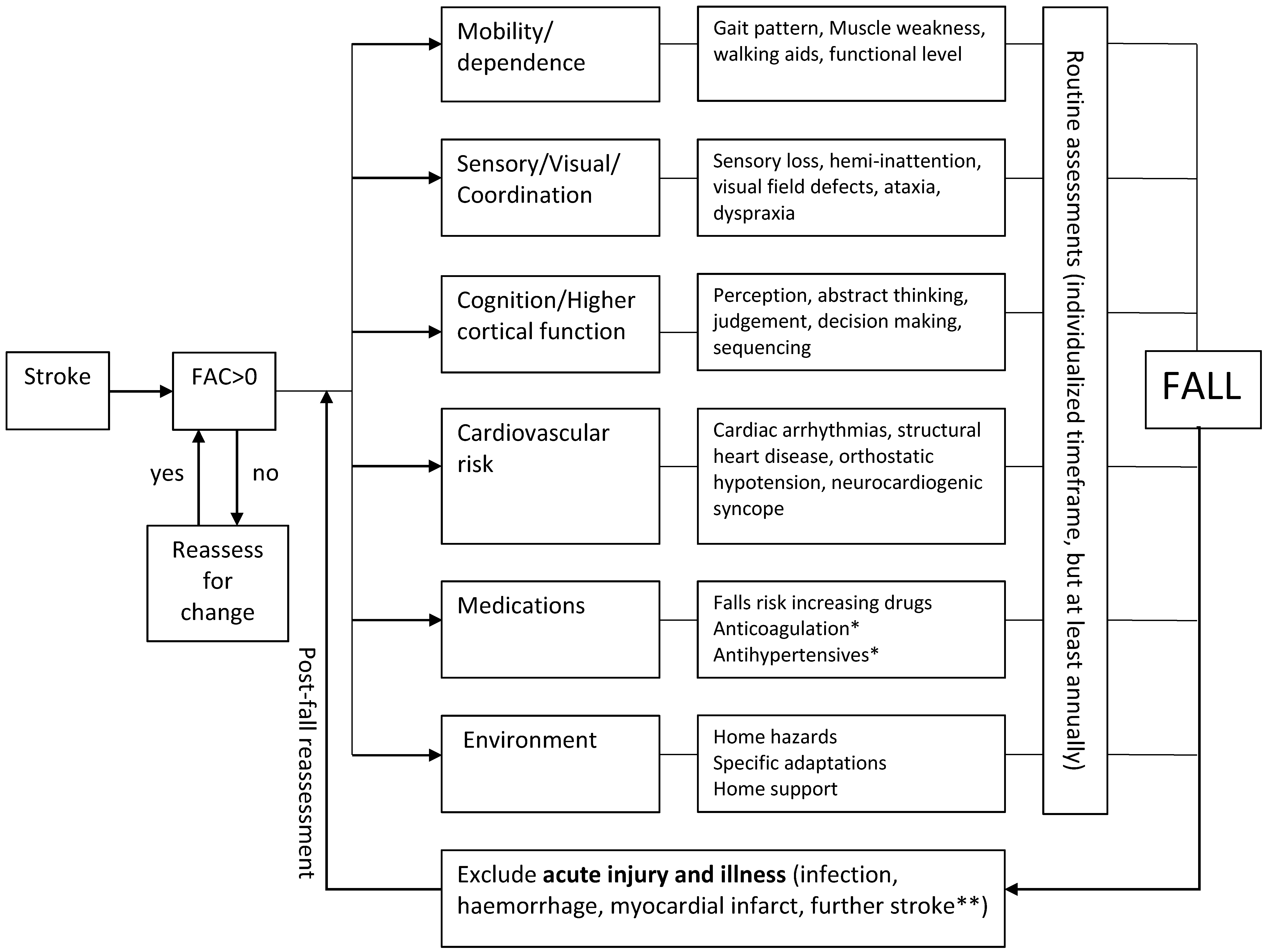
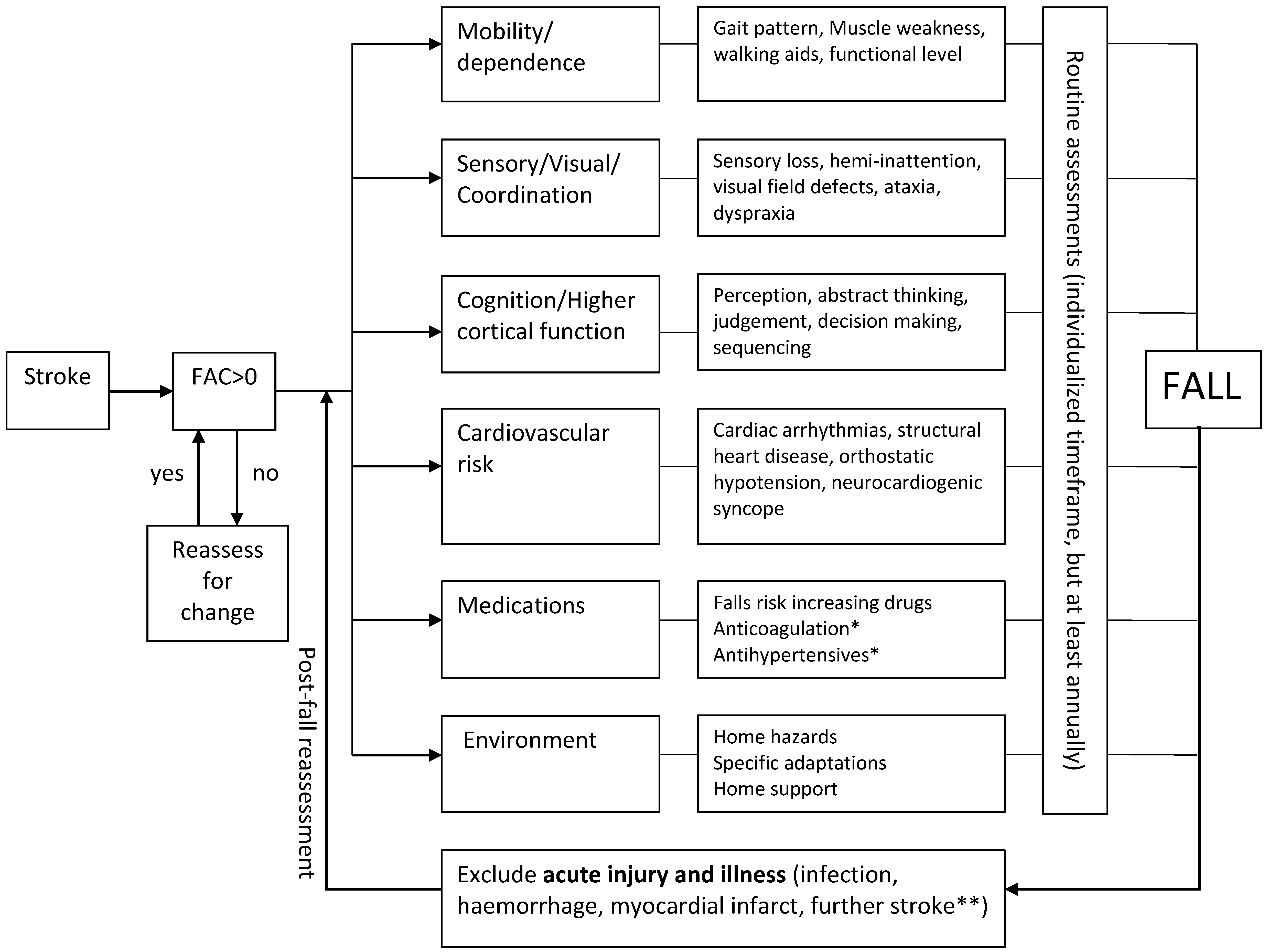
5. Investigative Strategy
5.1. Post-Stroke Falls Prediction
5.2. Investigation of Falls Post-Stroke
5.3. Baseline Investigations
5.4. Gait and Balance
5.5. Home Hazards
5.6. Cardiovascular Assessment
5.7. Imaging
5.8. Other Investigations
6. Management
6.1. Physical Therapy
6.2. Medication Management
6.3. Environmental Modification and Assistive Devices
6.4. Cardiovascular Interventions
6.5. Visual Interventions
6.6. Vitamin D and Osteoporosis Management
6.7. Multifaceted Interventions
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kerse, N.; Parag, V.; Feigin, V.L.; McNaughton, H.; Hackett, M.L.; Bennett, D.A.; Anderson, C.S. Auckland Regional Community Stroke (ARCOS) Study Group. Falls after stroke: Results from the Auckland Regional Community Stroke (ARCOS) Study, 2002 to 2003. Stroke 2008, 39, 1890–1893. [Google Scholar] [CrossRef] [PubMed]
- Goh, H.T.; Nadarajah, M.; Hamzah, N.B.; Varadan, P.; Tan, M.P. Falls and Fear of Falling After Stroke: A Case-Control Study. PM & R 2016. [Google Scholar] [CrossRef]
- Callaly, E.L.; Ni Chroinin, D.; Hannon, N.; Sheehan, O.; Marnane, M.; Merwick, A.; Kelly, L.A.; Horgan, G.; Williams, E.; Harris, D.; et al. Falls and fractures 2 years after acute stroke: The North Dublin Population Stroke Study. Age Ageing 2015, 44, 882–886. [Google Scholar] [PubMed]
- Teasell, R.; McRae, M.; Foley, N.; Bhardwaj, A. The incidence and consequences of falls in stroke patients during inpatient rehabilitation: Factors associated with high risk. Arch. Phys. Med. Rehabil. 2002, 83, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Jalayondeja, C.; Sullivan, P.E.; Pichaiyongwongdee, S. Six-month prospective study of fall risk factors identification in patients post-stroke. Geriatr. Gerontol. Int. 2014, 14, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Park, G.-D.; Choi, J.-U.; Kim, Y.-M. The effects of multidirectional stepping training on balance, gait ability, and falls efficacy following stroke. J. Phys. Ther. Sci. 2016, 28, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Yates, J.S.; Lai, S.M.; Duncan, P.W.; Studenski, S. Falls in community-dwelling stroke survivors: An accumulated impairments model. J. Rehabil. Res. Dev. 2002, 39, 385–394. [Google Scholar] [PubMed]
- Jorgensen, L.; Engstad, T.; Jacobsen, B.K. Higher incidence of falls in long-term stroke survivors than in population controls: Depressive symptoms predict falls after stroke. Stroke 2002, 33, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, S.F.; Goldie, P.; Hill, K. Falls incidence and factors associated with falling in older, community-dwelling, chronic stroke survivors (>1 year after stroke) and matched controls. Aging Clin. Exp. Res. 2005, 17, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Urabe, Y.; Fujii, E.; Moriyama, N.; Iwata, S.; Sasadai, J. The effect of different stretching techniques on ankle joint range of motion and dynamic postural stability after landing. J. Sports Med. Phys. Fitness 2016, 56, 692–698. [Google Scholar] [PubMed]
- Liu-Ambrose, T.; Pang, M.Y.; Eng, J.J. Executive function is independently associated with performances of balance and mobility in community-dwelling older adults after mild stroke: Implications for falls prevention. Cerebrovasc. Dis. 2007, 23, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ashburn, A.; Hyndman, D.; Pickering, R.; Yardley, L.; Harris, S. Predicting people with stroke at risk of falls. Age Ageing 2008, 37, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Hyndman, D.; Ashburn, A.; Stack, E. Fall events among people with stroke living in the community: Circumstances of falls and characteristics of fallers. Arch. Phys. Med. Rehabil. 2002, 83, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.Y.; Liu, W.M.; Chen, S.W.; Yang, C.A.; Tung, Y.C.; Chou, L.W.; Lin, L.C. Anosognosia, neglect and quality of life of right hemisphere stroke survivors. Eur. J. Neurol. 2014, 21, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Beatriz Pinto, E.; Nascimento, C.; Marinho, C.; Oliveira, I.; Monteiro, M.; Castro, M.; Myllane-Fernandes, P.; Ventura, L.M.; Maso, I.; Lopes, A.A.; et al. Risk factors associated with falls in adult patients after stroke living in the community: Baseline data from a stroke cohort in Brazil. Top. Stroke Rehabil. 2014, 21, 220–227. [Google Scholar] [CrossRef]
- Jones, S.A.; Shinton, R.A. Improving outcome in stroke patients with visual problems. Age Ageing 2006, 35, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.W.; Hornby, T.G.; Schmit, B.D. Perception of lower extremity loads in stroke survivors. Clin. Neurophysiology 2015, 126, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Morone, G.; Iosa, M.; Pratesi, L.; Paolucci, S. Can overestimation of walking ability increase the risk of falls in people in the subacute stage after stroke on their return home? Gait Posture 2014, 39, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Kearney, F.C.; Harwood, R.H.; Gladman, J.R.F.; Lincoln, N.; Masud, T. The relationship between executive function and falls and gait abnormalities in older adults: A systematic review. Dement. Geriatr. Cogn. Disord. 2013, 36, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Alemdaroglu, E.; Ucan, H.; Topcuoglu, A.M.; Sivas, F. In-hospital predictors of falls in community-dwelling individuals after stroke in the first 6 months after a baseline evaluation: A prospective cohort study. Arch. Phys. Med. Rehabil. 2012, 93, 2244–2250. [Google Scholar] [CrossRef] [PubMed]
- Wada, N.; Sohmiya, M.; Shimizu, T.; Okamoto, K.; Shirakura, K. Clinical analysis of risk factors for falls in home-living stroke patients using functional evaluation tools. Arch. Phys. Med. Rehabil. 2007, 88, 1601–1605. [Google Scholar] [CrossRef] [PubMed]
- Bultmann, U.; Pierscianek, D.; Gizewski, E.R.; Schoch, B.; Fritsche, N.; Timmann, D.; Maschke, M.; Frings, M. Functional recovery and rehabilitation of postural impairment and gait ataxia in patients with acute cerebellar stroke. Gait Posture 2014, 39, 563–569. [Google Scholar] [CrossRef]
- Sanna, T.; Diener, H.-.C.; Passman, R.S.; Di Lazzaro, V.; Bernstein, R.A.; Morillo, C.A.; Rymer, M.M.; Thijs, V.; Rogers, T.; Beckers, F.; et al. Cryptogenic Stroke and Underlying Atrial Fibrillation. N. Engl. J. Med. 2014, 370, 2478–2486. [Google Scholar] [CrossRef]
- Chang, H.Y.; Lin, Y.J.; Lo, L.W.; Chang, S.L.; Hu, Y.F.; Li, C.H.; Chao, T.F.; Yin, W.H.; Chen, S.A. Sinus node dysfunction in atrial fibrillation patients: The evidence of regional atrial substrate remodelling. Europace 2013, 15, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Stroke Prevention in Atrial Fibrillation Investigators. Warfarin versus aspirin for prevention of thromboembolism in atrial fibrillation: Stroke Prevention in Atrial Fibrillation II Study. Lancet 1994, 343, 687–691. [Google Scholar]
- Richardson, D.A.; Bexton, R.S.; Shaw, F.E.; Kenny, R.A. Prevalence of Cardioinhibitory Carotid Sinus Hypersensitivity in Patients 50 Years or over Presenting to the Accident and Emergency Department with “Unexplained” or “Recurrent” Falls. Pacing Clin. Electrophysiol. 1997, 20, 820–823. [Google Scholar] [CrossRef] [PubMed]
- McLaren, A.; Kerr, S.; Allan, L.; Steen, I.N.; Ballard, C.; Allen, J.; Murray, A.; Kenny, R.A. Autonomic function is impaired in elderly stroke survivors. Stroke 2005, 36, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.P.; Chadwick, T.J.; Kerr, S.R.; Parry, S.W. Symptomatic presentation of carotid sinus hypersensitivity is associated with impaired cerebral autoregulation. J. Am. Heart Assoc. 2014, 3, e000514. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, C.; Bennett, K.; Langan, Y.; Fan, C.W.; Kenny, R.A. Amnesia for loss of consciousness is common in vasovagal syncope. Europace 2011, 13, 1040–1045. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.W.; Steen, I.N.; Baptist, M.; Kenny, R.A. Amnesia for loss of consciousness in carotid sinus syndrome: Implications for presentation with falls. J. Am. Coll. Cardiol. 2005, 45, 1840–1843. [Google Scholar] [CrossRef] [PubMed]
- Saedon, N.I.; Zainal-Abidin, I.; Chee, K.H.; Khor, H.M.; Tan, K.M.; Kamaruzzaman, S.K.; Chin, A.V.; Poi, P.J.; Tan, M.P. Postural blood pressure electrocardiographic changes are associated with falls in older people. Clin. Auton. Res. 2016, 26, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Andersson, Å.G.; Kamwendo, K.; Appelros, P. Fear of falling in stroke patients: Relationship with previous falls and functional characteristics. Int. J. Rehabil. Res. 2008, 31, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Belgen, B.; Beninato, M.; Sullivan, P.E.; Narielwalla, K. The Association of Balance Capacity and Falls Self-Efficacy with History of Falling in Community-Dwelling People with Chronic Stroke. Arch. Phys. Med. Rehabil. 2006, 87, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Kernan, W.N.; Ovbiagele, B.; Black, H.R.; Bravata, D.M.; Chimowitz, M.I.; Ezekowitz, M.D.; Fang, M.C.; Fisher, M.; Furie, K.L.; Heck, D.V.; et al. Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 2160–2236. [Google Scholar] [CrossRef] [PubMed]
- Van der Velde, N.; Stricker, B.H.; Pols, H.A.; van der Cammen, T.J. Risk of falls after withdrawal of fall-risk-increasing drugs: A prospective cohort study. Br. J. Clin. Pharmacol. 2007, 63, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Marcum, Z.A.; Perera, S.; Newman, A.B.; Thorpe, J.M.; Switzer, G.E.; Gray, S.L.; Simonsick, E.M.; Shorr, R.I.; Bauer, D.C.; Castle, N.G.; et al. Antihypertensive Use and Recurrent Falls in Community-Dwelling Older Adults: Findings From the Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Medi. Sci. 2015. [Google Scholar] [CrossRef] [PubMed]
- Callisaya, M.L.; Sharman, J.E.; Close, J.; Lord, S.R.; Srikanth, V.K. Greater Daily Defined Dose of Antihypertensive Medication Increases the Risk of Falls in Older People—A Population-Based Study. J. Am. Geriatr. Soc. 2014, 62, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Marcum, Z.A.; Wirtz, H.S.; Pettinger, M.; LaCroix, A.Z.; Carnahan, R.; Cauley, J.A.; Bea, J.W.; Gray, S.L. Anticholinergic medication use and falls in postmenopausal women: Findings from the women’s health initiative cohort study. BMC Geriatr. 2016, 16, 76. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Fox, C.; Kwok, C.S.; Luben, R.N.; Wareham, N.J.; Khaw, K.-T. Total anticholinergic burden and risk of mortality and cardiovascular disease over 10 years in 21,636 middle-aged and older men and women of EPIC-Norfolk prospective population study. Age Ageing 2015, 44, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Richardson, K.; Bennett, K.; Maidment, I.D.; Fox, C.; Smithard, D.; Kenny, R.A. Use of medications with anticholinergic activity and self-reported injurious falls in older community-dwelling adults. J. Am. Geriatr. Soc. 2015, 63, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Zia, A.; Kamaruzzaman, S.; Myint, P.K.; Tan, M.P. Anticholinergic burden is associated with recurrent and injurious falls in older individuals. Maturitas 2016, 84, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Milos, V.; Bondesson, Å.; Magnusson, M.; Jakobsson, U.; Westerlund, T.; Midlöv, P. Fall risk-increasing drugs and falls: A cross-sectional study among elderly patients in primary care. BMC Geriatr. 2014, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Shiek Ahmad, B.; Hill, K.D.; O’Brien, T.J.; Gorelik, A.; Habib, N.; Wark, J.D. Falls and fractures in patients chronically treated with antiepileptic drugs. Neurology 2012, 79, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Quach, L.; Yang, F.M.; Berry, S.D.; Newton, E.; Jones, R.N.; Burr, J.A.; Lipsitz, L.A. Depression, antidepressants, and falls among community-dwelling elderly people: The MOBILIZE Boston study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Pieracci, F.M.; Eachempati, S.R.; Shou, J.; Hydo, L.J.; Barie, P.S. Use of long-term anticoagulation is associated with traumatic intracranial hemorrhage and subsequent mortality in elderly patients hospitalized after falls: Analysis of the new york state administrative database. J. Trauma Acute Care Surg. 2007, 63, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Donzé, J.; Clair, C.; Hug, B.; Rodondi, N.; Waeber, G.; Cornuz, J.; Aujesky, D. Risk of falls and major bleeds in patients on oral anticoagulation therapy. Am. J. Med. 2012, 125, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Garwood, C.L.; Corbett, T.L. Use of anticoagulation in elderly patients with atrial fibrillation who are at risk for falls. Ann. Pharmacother. 2008, 42, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y.H. A novel user-friendly score (has-bled) to assess 1-year risk of major bleeding in patients with atrial fibrillation: Euro heart survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Graham, N.S.; Crichton, S.; Koutroumanidis, M.; Wolfe, C.D.; Rudd, A.G. Incidence and associations of poststroke epilepsy: The prospective South London Stroke Register. Stroke 2013, 44, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Walsh, M.E.; Horgan, N.F.; Walsh, C.D.; Galvin, R. Systematic review of risk prediction models for falls after stroke. J. Epidemiol. Commun. Health 2016. [Google Scholar] [CrossRef] [PubMed]
- AGS/BGS PoPoFiOP. Updated American Geriatrics Society/British Geriatrics Society Clinical Practice Guideline for Prevention of Falls in Older Persons and Recommendations: American Geriatrics Society. Available online: http://geriatricscareonline.org/ProductAbstract/updated-american-geriatrics-societybritish-geriatrics-society-clinical-practice-guideline-for-prevention-of-falls-in-older-persons-and-recommendations/CL014 (accessed on 22 November 2016).
- Freeman, R.; Wieling, W.; Axelrod, F.B.; Benditt, D.G.; Benarroch, E.; Biaggioni, I.; Cheshire, W.P.; Chelimsky, T.; Cortelli, P.; Gibbons, C.H.; et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin. Auton. Res. 2011, 21, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Zia, A.; Kamaruzzaman, S.B.; Myint, P.K.; Tan, M.P. The association of antihypertensives with postural blood pressure and falls among seniors residing in the community: A case-control study. Eur. J. Clin. Invest. 2015, 45, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meiβner, D.; Pohl, M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-oriented assessment of mobility problems in elderly patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; Williams, J. The Balance Scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehabil. Med. 1995, 27, 27–36. [Google Scholar] [PubMed]
- Tiedemann, A.; Shimada, H.; Sherrington, C.; Murray, S.; Lord, S. The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people. Age Ageing 2008, 37, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Pighills, A.; Ballinger, C.; Pickering, R.; Chari, S. A critical review of the effectiveness of environmental assessment and modification in the prevention of falls amongst community dwelling older people. Br. J. Occup. Ther. 2016, 79, 133–143. [Google Scholar] [CrossRef]
- Said, C.M.; Batchelor, F.; Shaw, K.; Blennerhassett, J. Preparing patients at high risk of falls for discharge home after rehabilitation: Do we meet the guidelines? Geriatr. Gerontol. Int. 2016, 16, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Alboni, P.; Brignole, M.; Menozzi, C.; Raviele, A.; Del Rosso, A.; Dinelli, M.; Solano, A.; Bottoni, N. Diagnostic value of history in patients with syncope with or without heart disease. J. Am. Coll. Cardiol. 2001, 37, 1921–1928. [Google Scholar] [CrossRef]
- Bhangu, J.; McMahon, C.G.; Hall, P.; Bennett, K.; Rice, C.; Crean, P.; Sutton, R.; Kenny, R.A. Long-term cardiac monitoring in older adults with unexplained falls and syncope. Heart 2016, 102, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Moya, A.; Sutton, R.; Ammirati, F.; Blanc, J.-.J.; Brignole, M.; Dahm, J.B.; Deharo, J.C.; Gajek, J.; Gjesdal, K.; Krahn, A.; et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur. Heart J. 2009, 30, 2631–2671. [Google Scholar] [PubMed]
- Ungar, A.; Rivasi, G.; Rafanelli, M.; Toffanello, G.; Mussi, C.; Ceccofiglio, A.; McDonagh, R.; Drumm, B.; Marchionni, N.; Alboni, P.; et al. Safety and tolerability of Tilt Testing and Carotid Sinus Massage in the octogenarians. Age Ageing 2016, 45, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.W.; Reeve, P.; Lawson, J.; Shaw, F.E.; Davison, J.; Norton, M.; Frearson, R.; Kerr, S.; Newton, J.L. The Newcastle protocols 2008: An update on head-up tilt table testing and the management of vasovagal syncope and related disorders. Heart 2009, 95, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.M.; Nehus, N.R.; Astin, M.R.; Brown, C.K.; Johnson, R.; Brewer, K.L. Use of Cranial Computed Tomography (CT) in Elderly Patients Presenting After a Fall: Can We Predict Those Having Abnormal Head CT Scans. Br. J. Med. Med. Res. 2015, 6, 342–350. [Google Scholar] [CrossRef]
- Watson, P.; Conroy, A.; Moran, G.; Duncan, S. Retrospective study of sensitivity and specificity of EEG in the elderly compared with younger age groups. Epilepsy Behav. 2012, 25, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, G.S.; Weerdesteyn, V.; Pickering, R.M.; Kunkel, D.; Lennon, S.; Geurts, A.C.; Ashburn, A. Interventions for preventing falls in people after stroke. Cochrane Database Syst Rev. 2013, 5, Cd008728. [Google Scholar]
- Batchelor, F.; Hill, K.; Mackintosh, S.; Said, C. What works in falls prevention after stroke? A systematic review and meta-analysis. Stroke 2010, 41, 1715–1722. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar]
- Zia, A.; Kamaruzzaman, S.B.; Tan, M.P. Polypharmacy and falls in older people: Balancing evidence-based medicine against falls risk. Postgrad. Med. 2015, 127, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Robertson, M.C.; Gardner, M.M.; Norton, R.N.; Buchner, D.M. Psychotropic medication withdrawal and a home-based exercise program to prevent falls: A randomized, controlled trial. J. Am. Geriatr. Soc. 1999, 47, 850–853. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Piliae, R.E.; Mohler, M.J.; Najafi, B.; Coull, B.M. Objective fall risk detection in stroke survivors using wearable sensor technology: A feasibility study. Top. Stroke Rehabil. 2016, 23, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Parry, S.W.; Matthews, I.G. Update on the role of pacemaker therapy in vasovagal syncope and carotid sinus syndrome. Prog. Cardiovasc. Dis. 2013, 55, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R.H.; Foss, A.; Osborn, F.; Gregson, R.; Zaman, A.; Masud, T. Falls and health status in elderly women following first eye cataract surgery: A randomised controlled trial. Br. J. Ophthalmol. 2005, 89, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Rossi, P.W.; Kheyfets, S.; Reding, M.J. Fresnel prisms improve visual perception in stroke patients with homonymous hemianopia or unilateral visual neglect. Neurology 1990, 40, 1597–1599. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Iwamoto, J.; Kanoko, T.; Satoh, K. Low-dose vitamin D prevents muscular atrophy and reduces falls and hip fractures in women after stroke: A randomized controlled trial. Cerebrovasc. Dis. 2005, 20, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Iwamoto, J.; Honda, Y. An open-label trial comparing alendronate and alphacalcidol in reducing falls and hip fractures in disabled stroke patients. J. Stroke Cerebrovasc. Dis. 2011, 20, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Luan, L.; Li, R.; Wang, Z.; Hou, X.; Gu, W.; Wang, X.; Yan, S.; Xu, D. Stroke increases the risk of hip fracture: A systematic review and meta-analysis. Osteoporos. Int. 2016, 27, 3149–3154. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.-C.; Mo, H.; Guan, J.; He, J.-L.; Wu, Z.-J. Risk of hip fracture following stroke, a meta-analysis of 13 cohort studies. Osteoporos. Int. 2016, 27, 3673–3679. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsen, B.; Grove, E.; Vestergaard, P. Nationwide registry-based analysis of cardiovascular risk factors and adverse outcomes in patients treated with strontium ranelate. Osteoporos. Int. 2014, 25, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.; Kern, S.; Blennow, K.; Zetterberg, H.; Waern, M.; Guo, X.; Börjesson-Hanson, A.; Skoog, I.; Östling, S. Calcium supplementation and risk of dementia in women with cerebrovascular disease. Neurology 2016, 87, 1674–1680. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, F.A.; Hill, K.D.; Mackintosh, S.F.; Said, C.M.; Whitehead, C.H. Effects of a Multifactorial Falls Prevention Program for People with Stroke Returning Home After Rehabilitation: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2012, 93, 1648–1655. [Google Scholar] [CrossRef] [PubMed]

© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, K.M.; Tan, M.P. Stroke and Falls—Clash of the Two Titans in Geriatrics. Geriatrics 2016, 1, 31. https://doi.org/10.3390/geriatrics1040031
Tan KM, Tan MP. Stroke and Falls—Clash of the Two Titans in Geriatrics. Geriatrics. 2016; 1(4):31. https://doi.org/10.3390/geriatrics1040031
Chicago/Turabian StyleTan, Kit Mun, and Maw Pin Tan. 2016. "Stroke and Falls—Clash of the Two Titans in Geriatrics" Geriatrics 1, no. 4: 31. https://doi.org/10.3390/geriatrics1040031
APA StyleTan, K. M., & Tan, M. P. (2016). Stroke and Falls—Clash of the Two Titans in Geriatrics. Geriatrics, 1(4), 31. https://doi.org/10.3390/geriatrics1040031