
An Innovative Artificial Intelligence Classification Model for Non-Ischemic Cardiomyopathy Utilizing Cardiac Biomechanics Derived from Magnetic Resonance Imaging



Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset and Cohorts
2.1.1. Training Set (n = 1196)
- Chinese PLA General Hospital (Beijing);
- Xiangya Hospital, Central South University (Changsha);
- West China Hospital, Sichuan University (Chengdu);
- Beijing Anzhen Hospital, Capital Medical University (Beijing).
- Dilated Cardiomyopathy (DCM): 474 cases;
- Hypertrophic Cardiomyopathy (HCM): 358 cases;
- Cardiac Amyloidosis (CA): 132 cases;
- Hypertensive Cardiomyopathy (HTCM): 106 cases;
- Healthy Controls (HC): 126 individuals.
2.1.2. External Validation Set (n = 137)
- Dilated Cardiomyopathy (DCM): 45 cases;
- Hypertrophic Cardiomyopathy (HCM): 35 cases;
- Cardiac Amyloidosis (CA): 22 cases;
- Hypertensive Cardiomyopathy (HTCM): 15 cases;
- Healthy Controls (HC): 20 individuals.
2.2. CMR Acquisition and Analysis
2.2.1. CMR Image Collection
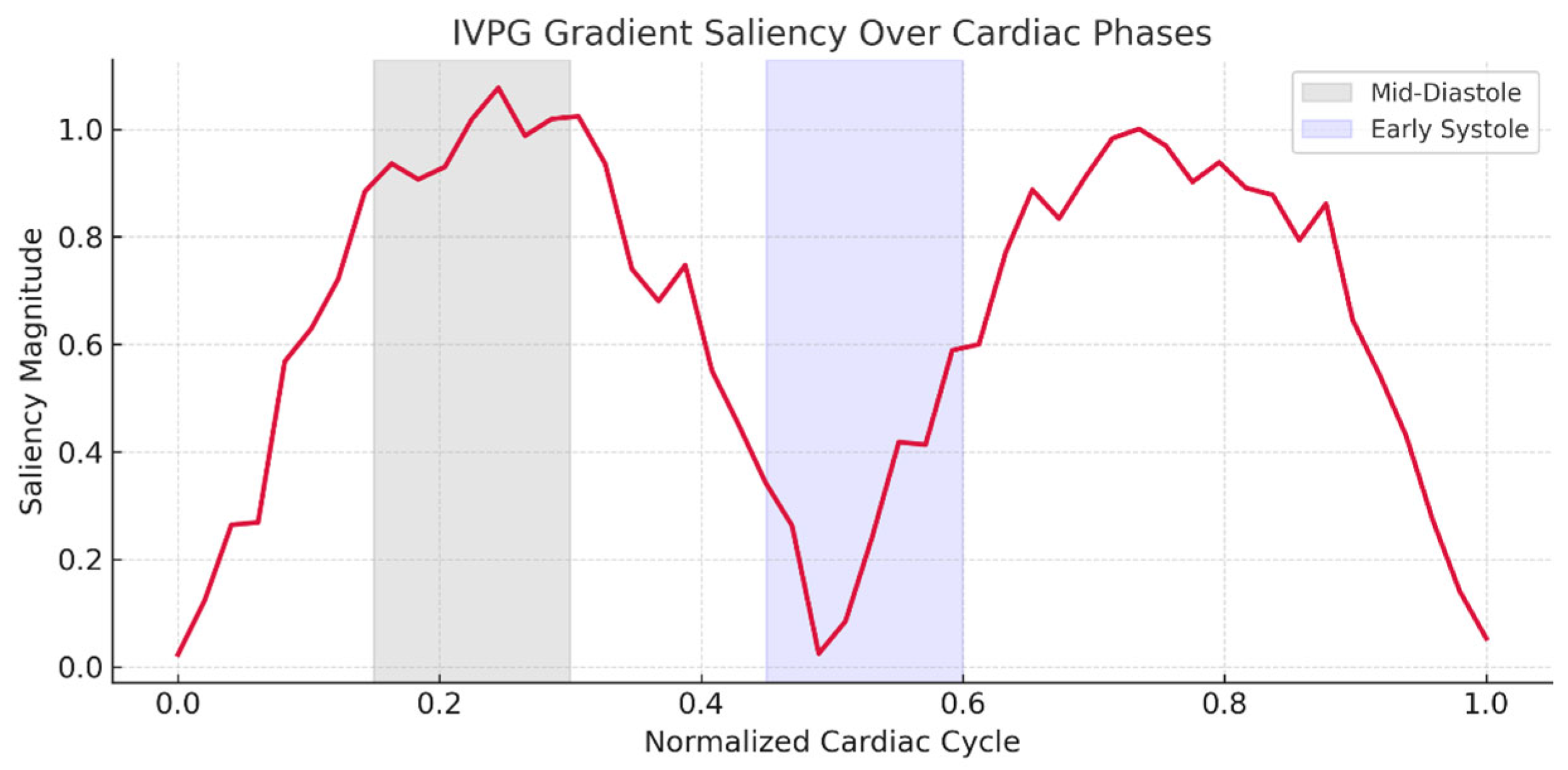
2.2.2. IVPG Extraction from Cine CMR
- Feature-tracked endocardial borders and valve annuli were used to derive myocardial velocities.
- Spline-based interpolation generated a smooth 3D left ventricular (LV) geometry per frame.
- Inflow/outflow velocities across the mitral and aortic valve planes were also tracked.
- A-wave: Systolic ejection;
- B-wave: Early diastolic suction (recoil);
- C-wave: Passive filling;
- D-wave: Atrial contraction.
2.3. Artificial Intelligence Methodology
2.3.1. Mathematical Formulation
2.3.2. Objective Functions
- –
- : Multi-frame CMR sequence for subject ;
- –
- : Time-series IVPG vectors for subject ;
- –
- : True diagnostic label (NICM subtype);
- –
- : Temporal length, height, width, and channel count of CMR data;
- –
- : Deep classification model with learnable parameters ;
- –
- : Gradient operator biomechanical input ;
- –
- : Regularization coefficients;
- –
- : Kullback–Leibler divergence;
- –
- : Weight regularization function.
2.3.3. Dual-Stream AI Architecture
- CNN (ResNet-50): Extracts spatial features frame-wise from .
- LSTM: Two-layer LSTM encodes cardiac motion dynamics over time:
- Dense (64) ReLU;
- Dense (32) ReLU;
- Dense (16) Embedding output.
- Dense (128) → ReLU;
- Dense (64) → ReLU;
- Dropout (0.4);
- Softmax output for 5-class NICM prediction.
- : Categorical cross-entropy;
- : IVPG sensitivity regularization;
- : L2 weight decay.
2.4. Ethical Compliance and Data Handling
3. Results
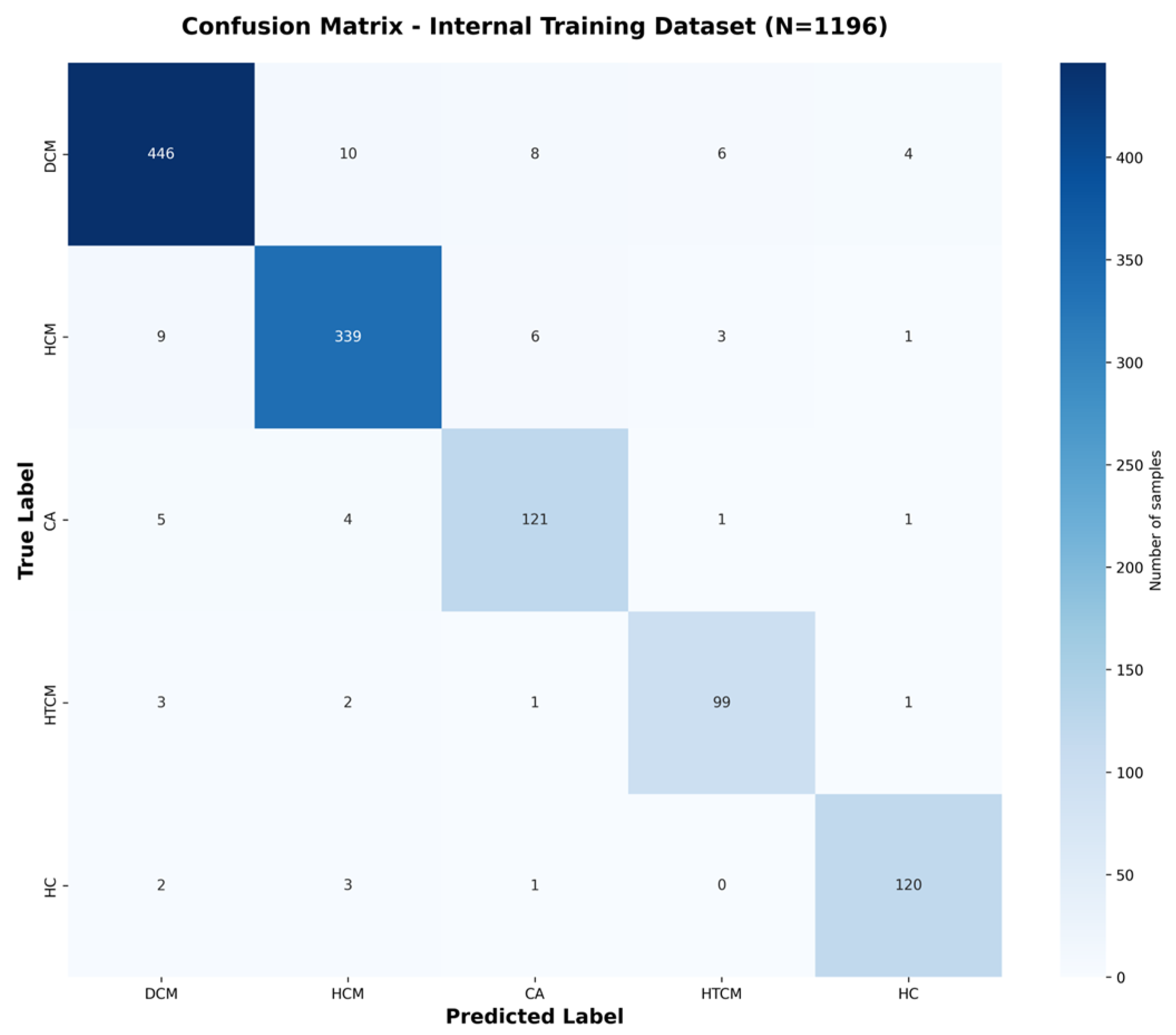
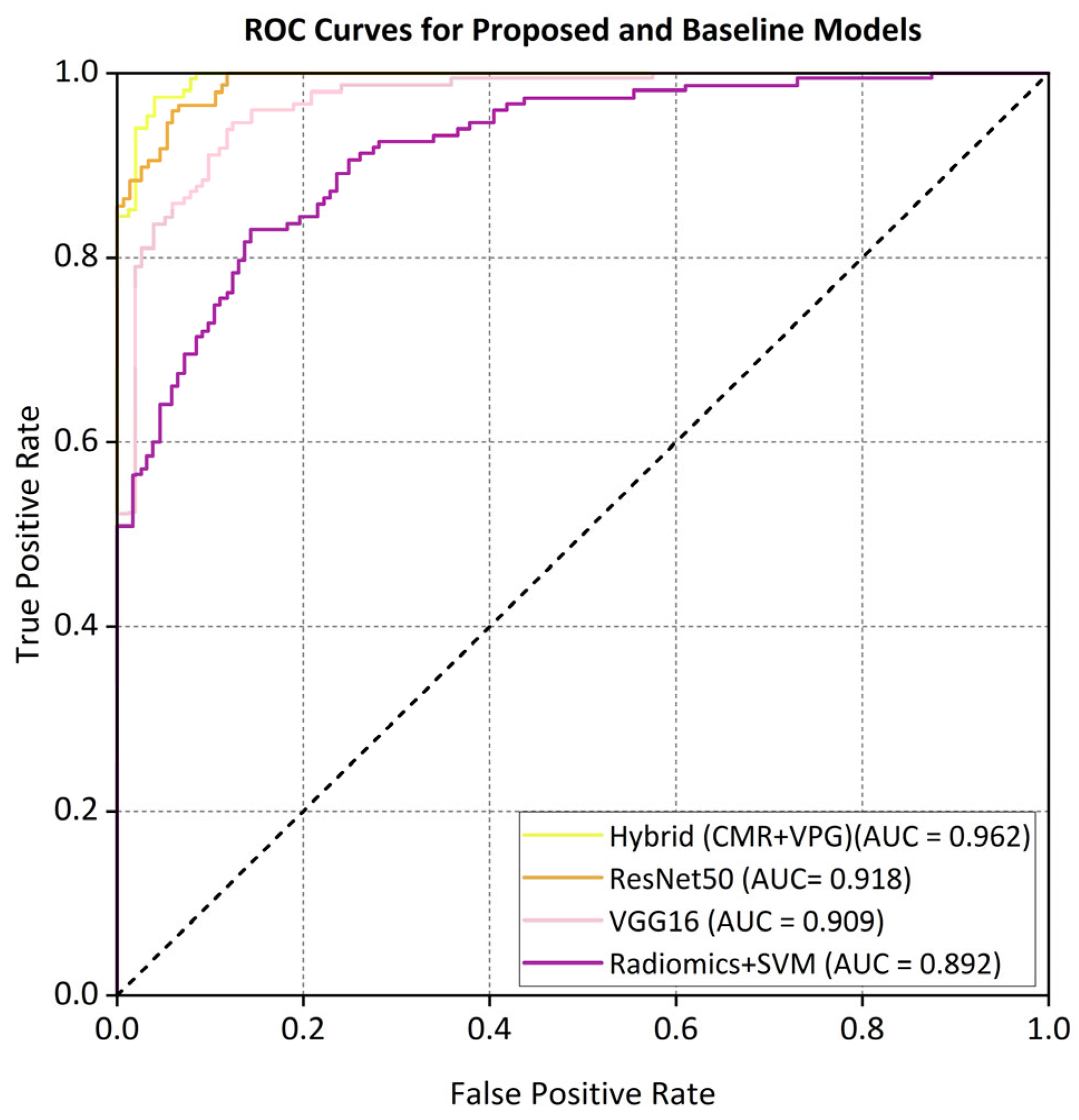
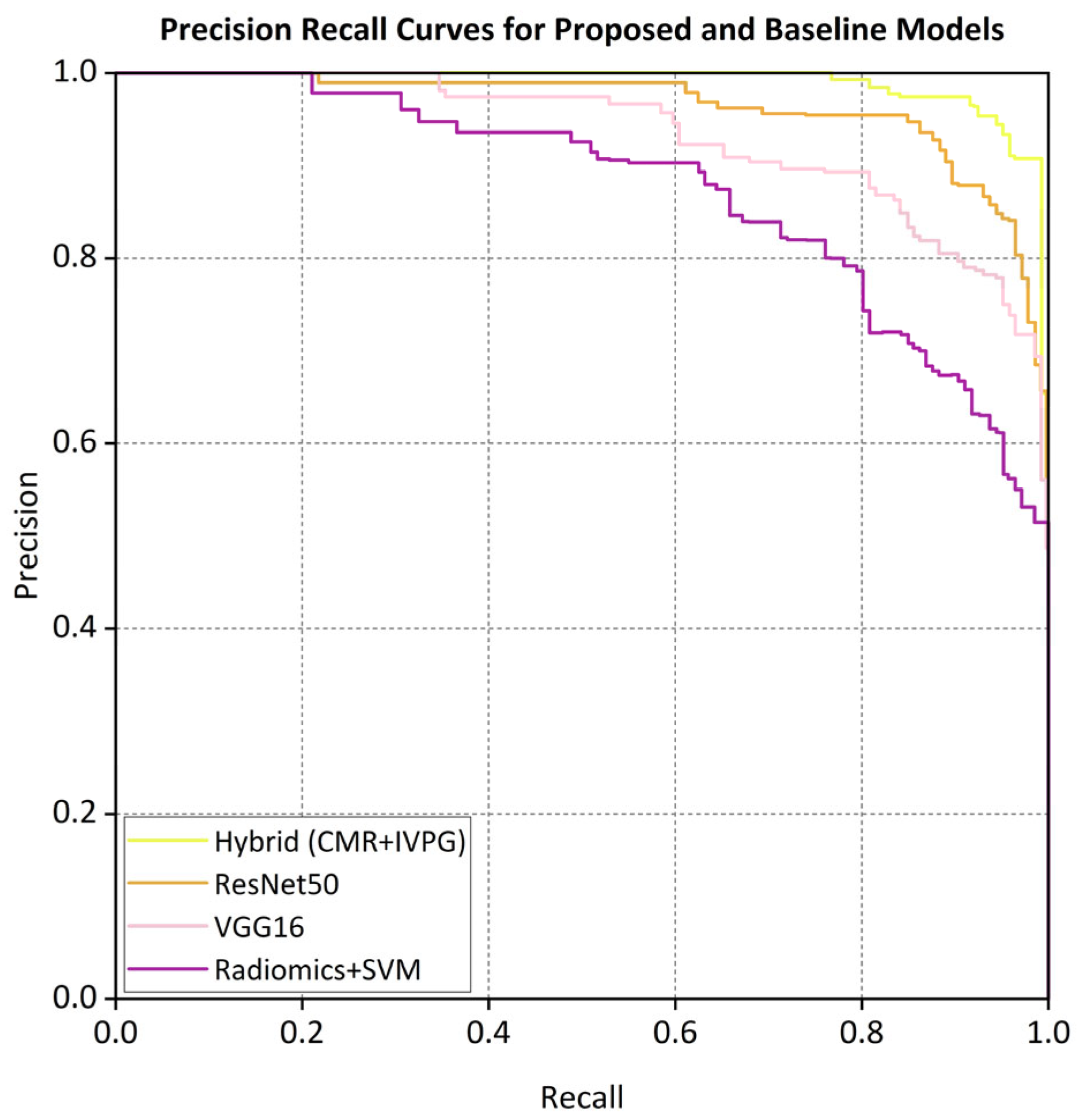
3.1. Quantitative Performance Evaluation
3.2. Contribution of IVPG Features
3.3. Generalizability and External Validation
3.4. Model Interpretability and Clinical Relevance
3.5. Comparative Analysis of Model Variants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NICMs | Non-ischemic cardiomyopathies |
| IVPGs | Intraventricular pressure gradients |
| CMR | Cardiac magnetic resonance |
| DCM | Dilated cardiomyopathy |
| HCM | Hypertrophic cardiomyopathy |
| HTCM | Hypertensive cardiomyopathy |
| CA | Cardiac amyloidosis |
| CNNs | Convolutional neural networks |
| GAN | Generative adversarial network |
| MLP | Multi-layer perception |
| DL | Deep learning |
| SVMs | Support vector machines |
| Grad-CAM | Gradient-weighted class activation mapping |
References
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis. A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. J. Heart Fail. 2021, 23, 512–526. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Oh, J.; Hong, Y.J.; Kim, D.; Yu, H.T.; Lee, C.J.; Kim, T.H.; Uhm, J.S.; Joung, B.; Pak, H.N.; et al. Tissue characterization using cardiac magnetic resonance imaging and response to cardiac resynchronization therapy. EP Eur. 2025, 27, euaf043. [Google Scholar] [CrossRef]
- Berberoğlu, E.; Stoeck, C.T.; Kozerke, S.; Genet, M. Quantification of left ventricular strain and torsion by joint analysis of 3D tagging and cine MR images. Med. Image Anal. 2022, 82, 102598. [Google Scholar] [CrossRef]
- Taylor, R.J.; Moody, W.E.; Umar, F.; Edwards, N.C.; Taylor, T.J.; Stegemann, B.; Townend, J.N.; Hor, K.N.; Steeds, R.P.; Mazur, W.; et al. Myocardial strain measurement with feature-tracking cardiovascular magnetic resonance: Normal values. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 871–881. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Rev. Esp. Cardiol. 2016, 69, 1167. [Google Scholar] [CrossRef] [PubMed]
- Merlo, M.; Gagno, G.; Baritussio, A.; Bauce, B.; Biagini, E.; Canepa, M.; Cipriani, A.; Castelletti, S.; Dellegrottaglie, S.; Guaricci, A.I.; et al. Clinical application of CMR in cardiomyopathies: Evolving concepts and techniques. Heart Fail. Rev. 2023, 28, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Ibrahim, E.H.; Parwani, P.; Bhave, N.; Stojanovska, J. Practical Guide to Evaluating Myocardial Disease by Cardiac MRI. AJR Am. J. Roentgenol. 2020, 214, 546–556. [Google Scholar] [CrossRef]
- Bhaskaran, A.; De Silva, K.; Kumar, S. Contemporary updates on ventricular arrhythmias: From mechanisms to management. Intern. Med. J. 2023, 53, 892–906. [Google Scholar] [CrossRef]
- Pan, J.A.; Patel, A.R. The role of multimodality imaging in cardiomyopathy. Curr. Cardiol. Rep. 2024, 26, 689–703. [Google Scholar] [CrossRef]
- Nakashima, M.; Chen, D.; Basnet, R.; Benovoy, M.; Hwang, T.H.; Geschke, R.; Grimm, R.A.; Kapadia, S.R.; Svensson, L.G.; Griffin, B.P.; et al. Comparison of deep learning and radiomic features to differentiate non-ischemic and ischemic cardiomyopathy using cardiac MRI cine imaging. Circulation 2021, 144, A12691. [Google Scholar] [CrossRef]
- Nakashima, M.; Cockrum, J.; Salam, D.; Mazumder, S.; Sreedhara, K.; Kapadia, S.R.; Svensson, L.G.; Grimm, R.A.; Nguyen, C.; Tang, W.H.W.; et al. Segmentation improves deep learning accuracy for differentiating non-ischemic and ischemic cardiomyopathy using cardiac MRI cine imaging. Circulation 2022, 146, A15522. [Google Scholar] [CrossRef]
- Cau, R.; Pisu, F.; Pintus, A.; Palmisano, V.; Montisci, R.; Suri, J.S.; Salgado, R.; Saba, L. Cine-cardiac magnetic resonance to distinguish between ischemic and non-ischemic cardiomyopathies: A machine learning approach. Eur. Radiol. 2024, 34, 5691–5704. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Zhang, L.; Wang, J.; Li, X.; Hu, S.; Fu, Y.; Wang, X.; Hao, S.; Hu, C. Differentiating between cardiac amyloidosis and hypertrophic cardiomyopathy on non-contrast cine-magnetic resonance images using machine learning-based radiomics. Front. Cardiovasc. Med. 2022, 9, 1001269. [Google Scholar] [CrossRef]
- Avard, E.; Shiri, I.; Hajianfar, G.; Abdollahi, H.; Kalantari, K.R.; Houshmand, G.; Kasani, K.; Bitarafan-Rajabi, A.; Deevband, M.R.; Oveisi, M.; et al. Non-contrast cine cardiac magnetic resonance image radiomics features and machine learning algorithms for myocardial infarction detection. Comput. Biol. Med. 2022, 141, 105145. [Google Scholar] [CrossRef]
- Miller, R.; Kerfoot, E.; Mauger, C.; Ismail, T.F.; Young, A.A.; Nordsletten, D.A. An implementation of patient-specific biventricular mechanics simulations with a deep learning and computational pipeline. Front. Physiol. 2021, 12, 716597. [Google Scholar] [CrossRef]
- Abdulkareem, M.; Kenawy, A.A.; Rauseo, E.; Lee, A.M.; Sojoudi, A.; Amir-Khalili, A.; Lekadir, K.; Young, A.A.; Barnes, M.R.; Barckow, P.; et al. Predicting post-contrast information from contrast agent free cardiac MRI using machine learning: Challenges and methods. Front. Cardiovasc. Med. 2022, 9, 894503. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Janardhanan, R. Role of cardiac MRI in nonischemic cardiomyopathies. Indian Heart J. 2016, 68, 405–409. [Google Scholar] [CrossRef]
- Wang, Y.; Jia, H.; Song, J. Accurate classification of non-ischemic cardiomyopathy. Curr. Cardiol. Rep. 2023, 25, 1299–1317. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, L.; Liao, B.; Cai, Q.; Luo, G.; Zhou, H.; Tang, H. Challenges in clinical translation of cardiac magnetic resonance imaging radiomics in non-ischemic cardiomyopathy: A narrative review. Cardiovasc. Diagn. Ther. 2024, 14, 1210–1227. [Google Scholar] [CrossRef]
- El-Husseiny, H.M.; Mady, E.A.; Ma, D.; Hamabe, L.; Takahashi, K.; Tanaka, R. Intraventricular pressure gradient: A novel tool to assess the post-infarction chronic congestive heart failure. Front. Cardiovasc. Med. 2022, 9, 944171. [Google Scholar] [CrossRef]
- Konijnenberg, L.S.; Beijnink, C.W.; van Lieshout, M.; Vos, J.L.; Rodwell, L.; Bodi, V.; Ortiz-Pérez, J.T.; van Royen, N.; Rodriguez Palomares, J.; Nijveldt, R. Cardiovascular magnetic resonance imaging-derived intraventricular pressure gradients in ST-segment elevation myocardial infarction: A long-term follow-up study. Eur. Heart J. Imaging Methods Pract. 2024, 2, qyae009. [Google Scholar] [CrossRef] [PubMed]
- Hirose, M.; Ma, D.; Shimada, K.; Yoshida, T.; Matsuura, K.; Kitpipatkun, P.; Hatanaka, A.; Zhao, Y.; Takahashi, K.; Tanaka, R.; et al. Effects of trans-mitral flow patterns and heart rate on intraventricular pressure gradients and E/E’ in the early stage of a rat model of hypertensive cardiomyopathy. Front. Vet. Sci. 2025, 12, 1507817. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Ma, X.; Dong, Z.; Chen, X.; Yang, S.; Chen, X.; Yang, K.; Zhao, S. Cardiac magnetic resonance visualization of the myocardial microstructure in non-ischemic cardiomyopathies. Cardiovasc. Innov. Appl. 2024, 9, e939. [Google Scholar] [CrossRef]
- Jumadilova, D.; Rakhmanov, Y.; Khissamutdinov, N.; Zhankorazova, A.; Toktarbay, B.; Khamitova, Z.; Zholshybek, N.; Bekbossynova, M.; Dautov, T.; Gaipov, A.; et al. Differences in cardiac mechanics assessed by left ventricular hemodynamic forces in athletes and patients with hypertension. Sci. Rep. 2024, 14, 27402. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.S.; Chan, W.X.; Mao, W.; Yap, C.H. 3D velocity and pressure field reconstruction in the cardiac left ventricle via physics-informed neural network from echocardiography guided by 3D colour Doppler. Comput. Methods Programs Biomed. 2025, 263, 108671. [Google Scholar] [CrossRef]
- Meyers, B.A. Methods for Echocardiographic Biomechanical Measurements. Ph.D. Dissertation, Purdue University, West Lafayette, IN, USA, 2021. [Google Scholar]
- Fatehi Hassanabad, A.; Garcia, J. Intra-cardiac kinetic energy and ventricular flow analysis in bicuspid aortic valve: Impact on left ventricular function, dilation severity, and surgical referral. Fluids 2024, 10, 5. [Google Scholar] [CrossRef]
- Sugiura, T.; Nawaz, S.; Shahannaz, D.C.; Ferrell, B.E.; Yoshida, T. From injury to repair: The therapeutic potential of induced pluripotent stem cells in heart failure. Regener. Med. Rep. 2025, 2, 22–30. [Google Scholar] [CrossRef]
- Hu, Y.; Zou, Y.; Qiao, L.; Lin, L. Integrative proteomic and metabolomic elucidation of cardiomyopathy with in vivo and in vitro models and clinical samples. Mol. Ther. 2024, 32, 3288–3312. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Accuracy | Precision | Recall | F1-Score | AUC | Kappa |
|---|---|---|---|---|---|---|
| Internal (n = 1196) | 94.2% | 93.8% | 94.2% | 93.4% | 0.974 | 0.925 |
| External (n = 137) | 92.1% | 92.3% | 92.1% | 91.7% | 0.962 | 0.884 |
| Model | Accuracy | F1-Score | AUC | Kappa |
|---|---|---|---|---|
| Proposed hybrid (CMR + IVPG) | 92.1% | 91.7% | 0.962 | 0.884 |
| ResNet50 (CMR only) | 86.4% | 86.1% | 0.918 | 0.812 |
| VGG16 (CMR only) | 85.3% | 84.9% | 0.909 | 0.799 |
| Radiomics + SVM | 82.1% | 81.6% | 0.892 | 0.752 |
| Model Variant | Accuracy | F1-Score | AUC |
|---|---|---|---|
| CMR + IVPG (full model) | 92.1% | 91.7% | 0.962 |
| CMR only | 86.4% | 86.1% | 0.918 |
| IVPG only | 78.1% | 77.6% | 0.852 |
| Subset | Accuracy | F1-Score | AUC |
|---|---|---|---|
| 2019–2020 | 92.3% | 91.8% | 0.961 |
| 2021–2023 | 91.9% | 91.5% | 0.963 |
| 2024–2025 | 92.0% | 91.6% | 0.964 |
| Cangzhou (overall) | 92.1% | 91.7% | 0.962 |
| Model | Accuracy | F1-Score | AUC | Kappa |
|---|---|---|---|---|
| Hybrid (CMR + IVPG) | 92.1% | 91.7% | 0.962 | 0.884 |
| ResNet50 (CMR only) | 86.4% | 86.1% | 0.918 | 0.812 |
| VGG16 (CMR only) | 85.3% | 84.9% | 0.909 | 0.799 |
| Radiomics + SVM | 82.1% | 81.6% | 0.892 | 0.752 |
| CMR + IVPG (ablation test) | 92.1% | 91.7% | 0.962 | 0.884 |
| CMR only (ablation test) | 86.4% | 86.1% | 0.918 | 0.812 |
| IVPG only (ablation test) | 78.1% | 77.6% | 0.852 | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, L.; Zhang, P.; Cheng, L.; Zhi, P.; Xu, J.; Liu, X.; Zhang, Y.; Xu, Z.; He, K. An Innovative Artificial Intelligence Classification Model for Non-Ischemic Cardiomyopathy Utilizing Cardiac Biomechanics Derived from Magnetic Resonance Imaging. Bioengineering 2025, 12, 670. https://doi.org/10.3390/bioengineering12060670
Fu L, Zhang P, Cheng L, Zhi P, Xu J, Liu X, Zhang Y, Xu Z, He K. An Innovative Artificial Intelligence Classification Model for Non-Ischemic Cardiomyopathy Utilizing Cardiac Biomechanics Derived from Magnetic Resonance Imaging. Bioengineering. 2025; 12(6):670. https://doi.org/10.3390/bioengineering12060670
Chicago/Turabian StyleFu, Liqiang, Peifang Zhang, Liuquan Cheng, Peng Zhi, Jiayu Xu, Xiaolei Liu, Yang Zhang, Ziwen Xu, and Kunlun He. 2025. "An Innovative Artificial Intelligence Classification Model for Non-Ischemic Cardiomyopathy Utilizing Cardiac Biomechanics Derived from Magnetic Resonance Imaging" Bioengineering 12, no. 6: 670. https://doi.org/10.3390/bioengineering12060670
APA StyleFu, L., Zhang, P., Cheng, L., Zhi, P., Xu, J., Liu, X., Zhang, Y., Xu, Z., & He, K. (2025). An Innovative Artificial Intelligence Classification Model for Non-Ischemic Cardiomyopathy Utilizing Cardiac Biomechanics Derived from Magnetic Resonance Imaging. Bioengineering, 12(6), 670. https://doi.org/10.3390/bioengineering12060670