

Machine Learning and Optical-Coherence-Tomography-Derived Radiomics Analysis to Predict the Postoperative Anatomical Outcome of Full-Thickness Macular Hole

 ,
,
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. OCT Image Acquisition
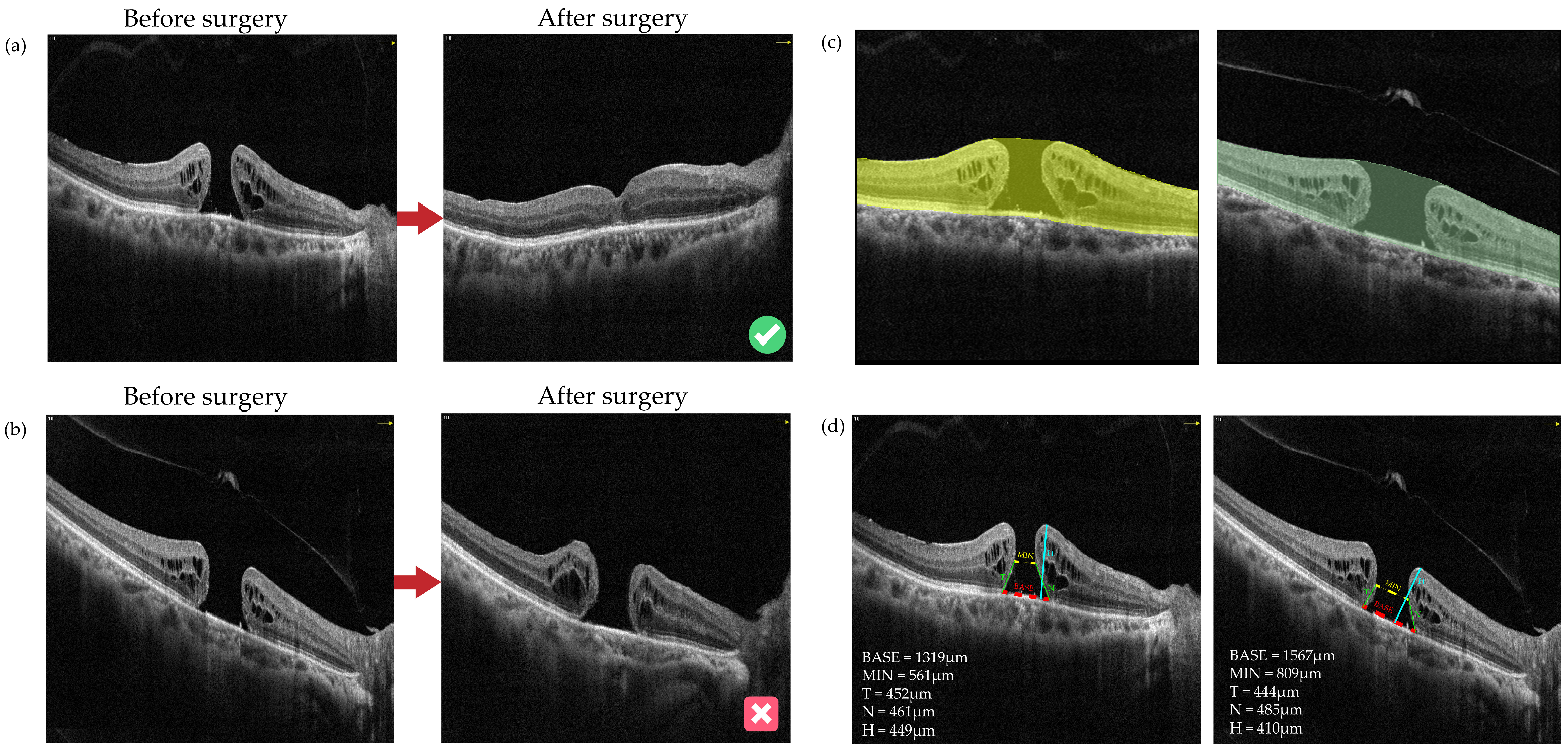
2.3. Region of Interest Segmentation and Parameter Measurement
2.4. Feature Extraction and Selection
2.5. Development of OCT-Omics Models
- sampling_strategy = “auto”,
- random_state = None,
- k_neighbors = 5,
- n_jobs = None
2.6. Training and Validation of Machine Learning Models
- SVM: penalty factor C = 1; kernel function, linear; maximum of iterations = 1000; 5-fold cross-validation;
- BPNN: activation function, rectified linear unit (ReLU); solver, Limited-memory Broyden–Fletche–Goldfarb–Shanno (LBFGS); L2 regularization term = 1; number of iterations = 1000; 5-fold cross-validation.
2.7. Statistical Analysis
3. Results
3.1. Summary of Study Design and Baseline Characteristics
3.2. OCT-Omics Model Development and Clinical Implication Evaluation
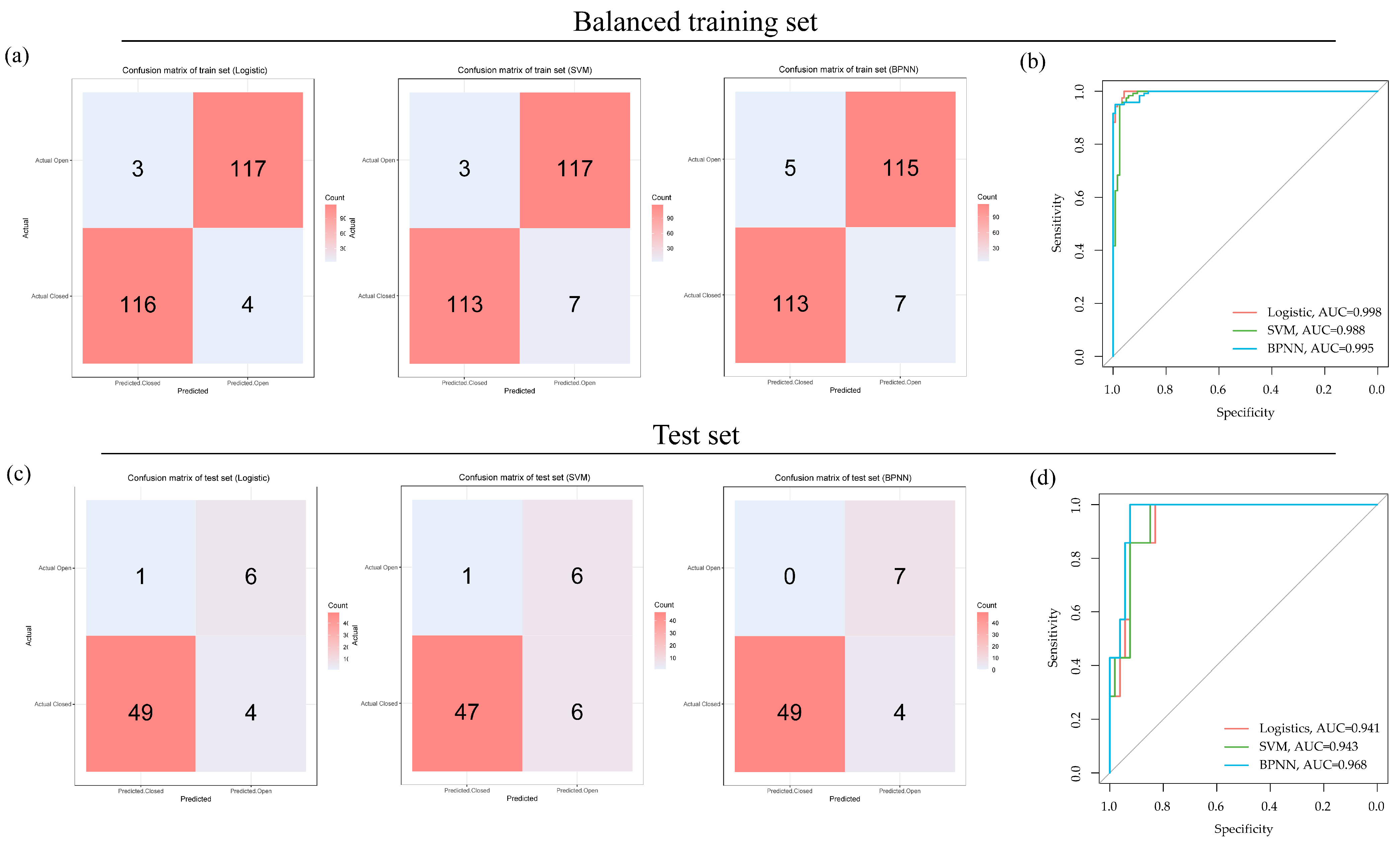
3.3. Evaluation of Overall Performance in Multiple Models
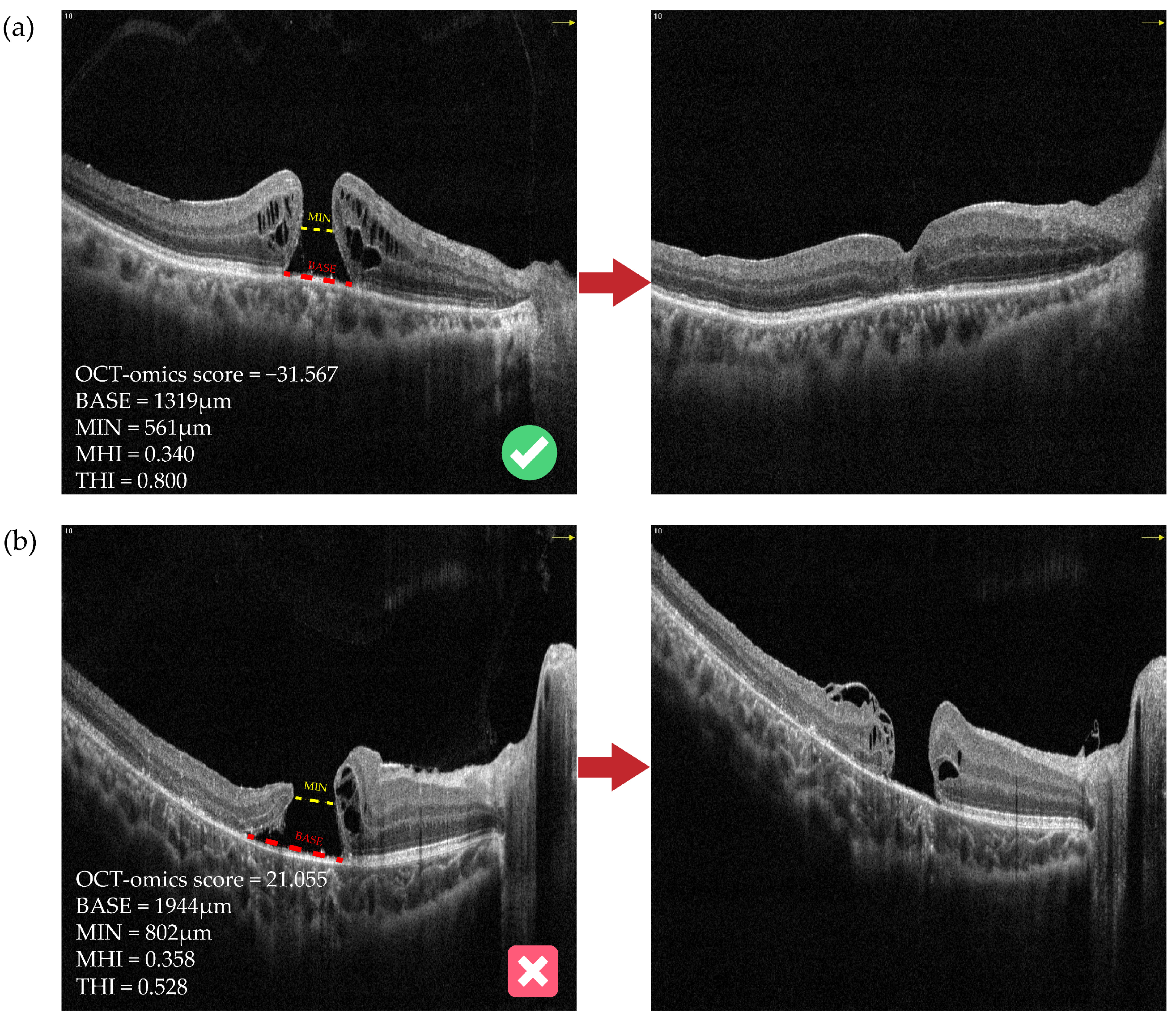
3.4. Clinical Implications of the OCT-Omics Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BASE | MIN | N | T | H | HFF | MHI | DHI | THI | OCT-Omics | |
|---|---|---|---|---|---|---|---|---|---|---|
| BASE | 1 *** | 0.653 *** | 0.719 *** | 0.766 *** | 0.324 *** | −0.131 | −0.805 *** | −0.2 ** | −0.442 *** | 0.217 *** |
| MIN | 0.653 *** | 1 *** | 0.141 * | 0.22 *** | −0.04 | −0.658 *** | −0.718 *** | 0.518 *** | −0.904 *** | 0.255 *** |
| N | 0.719 *** | 0.141 * | 1 *** | 0.865 *** | 0.52 *** | 0.46 *** | −0.411 *** | −0.591 *** | 0.074 | 0.153 * |
| T | 0.766 *** | 0.22 *** | 0.865 *** | 1 *** | 0.557 *** | 0.398 *** | −0.437 *** | −0.532 *** | 0.016 | 0.137 |
| H | 0.324 *** | −0.04 | 0.52 *** | 0.557 *** | 1 *** | 0.442 *** | 0.208 ** | −0.384 *** | 0.39 *** | 0.103 |
| HFF | −0.131 | −0.658 *** | 0.46 *** | 0.398 *** | 0.442 *** | 1 *** | 0.436 *** | −0.733 *** | 0.787 *** | −0.103 |
| MHI | −0.805 *** | −0.718 *** | −0.411 *** | −0.437 *** | 0.208 ** | 0.436 *** | 1 *** | −0.067 | 0.737 *** | −0.2 ** |
| DHI | −0.2 ** | 0.518 *** | −0.591 *** | −0.532 *** | −0.384 *** | −0.733 *** | −0.067 | 1 *** | −0.646 *** | 0.055 |
| THI | −0.442 *** | −0.904 *** | 0.074 | 0.016 | 0.39 *** | 0.787 *** | 0.737 *** | −0.646 *** | 1 *** | −0.215 ** |
| OCT-omics | 0.217 *** | 0.255 *** | 0.153 * | 0.137 | 0.103 | −0.103 | −0.2 ** | 0.055 | −0.215 ** | 1 *** |
| Variables | Total (n = 200) | ILM Peeling (n = 136) | ILM Flap (n = 64) | Statistic | p |
|---|---|---|---|---|---|
| BASE, M (IQR) | 965.50 (591) | 914.00 (565) | 1029.00 (574) | Z = −2.10 | 0.035 ** |
References
- Duker, J.S.; Kaiser, P.K.; Binder, S.; de Smet, M.D.; Gaudric, A.; Reichel, E.; Sadda, S.R.; Sebag, J.; Spaide, R.F.; Stalmans, P. The International Vitreomacular Traction Study Group Classification of Vitreomacular Adhesion, Traction, and Macular Hole. Ophthalmology 2013, 120, 2611–2619. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xu, L.; Jonas, J.B. Prevalence of Full-Thickness Macular Holes in Urban and Rural Adult Chinese: The Beijing Eye Study. Am. J. Ophthalmol. 2006, 141, 589–591. [Google Scholar] [CrossRef]
- Nangia, V.; Jonas, J.B.; Khare, A.; Lambat, S. Prevalence of Macular Holes in Rural Central India. The Central India Eye and Medical Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2012, 250, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- McCannel, C.A.; Ensminger, J.L.; Diehl, N.N.; Hodge, D.N. Population-Based Incidence of Macular Holes. Ophthalmology 2009, 116, 1366–1369. [Google Scholar] [CrossRef]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G. Idiopathic Macular Hole Preferred Practice Pattern®. Ophthalmology 2020, 127, P184–P222. [Google Scholar] [CrossRef]
- GASS, J.D.M. Reappraisal of Biomicroscopic Classification of Stages of Development of a Macular Hole. Am. J. Ophthalmol. 1995, 119, 752–759. [Google Scholar] [CrossRef]
- Spiteri Cornish, K.; Lois, N.; Scott, N.; Burr, J.; Cook, J.; Boachie, C.; Tadayoni, R.; la Cour, M.; Christensen, U.; Kwok, A. Vitrectomy with Internal Limiting Membrane (ILM) Peeling versus Vitrectomy with No Peeling for Idiopathic Full-Thickness Macular Hole (FTMH). Cochrane Database Syst. Rev. 2013, CD009306. [Google Scholar] [CrossRef] [PubMed]
- Ternent, L.; Vale, L.; Boachie, C.; Burr, J.M.; Lois, N. Full-Thickness Macular Hole and Internal Limiting Membrane Peeling Study (FILMS) Group Cost-Effectiveness of Internal Limiting Membrane Peeling versus No Peeling for Patients with an Idiopathic Full-Thickness Macular Hole: Results from a Randomised Controlled Trial. Br. J. Ophthalmol. 2012, 96, 438–443. [Google Scholar] [CrossRef]
- Ghoraba, H.; Rittiphairoj, T.; Akhavanrezayat, A.; Karaca, I.; Matsumiya, W.; Pham, B.; Mishra, K.; Yasar, C.; Mobasserian, A.; Abdelkarem, A.A.; et al. Pars Plana Vitrectomy with Internal Limiting Membrane Flap versus Pars Plana Vitrectomy with Conventional Internal Limiting Membrane Peeling for Large Macular Hole. Cochrane Database Syst. Rev. 2023, 2023, CD015031. [Google Scholar] [CrossRef]
- Cundy, O.; Lange, C.A.; Bunce, C.; Bainbridge, J.W.; Solebo, A.L. Face-down Positioning or Posturing after Macular Hole Surgery. Cochrane Database Syst. Rev. 2023, 2023, CD008228. [Google Scholar] [CrossRef]
- Elhusseiny, A.M.; Schwartz, S.G.; Flynn, H.W.; Smiddy, W.E. Long-Term Outcomes after Macular Hole Surgery. Ophthalmol. Retin. 2020, 4, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Ip, M.S. Anatomical Outcomes of Surgery for Idiopathic Macular Hole as Determined by Optical Coherence Tomography. Arch. Ophthalmol. 2002, 120, 29. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Tartaro, R.; Barca, F.; Caporossi, T.; Bacherini, D.; Giansanti, F. Internal limiting membrane peeling versus inverted flap technique for treatment of full-thickness macular holes. Retina 2018, 38, S73–S78. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Machairoudia, G.; Kazantzis, D.; Theodossiadis, G.; Theodossiadis, P. Inverted Internal Limiting Membrane Flap Technique for Myopic Macular Hole: A Meta-Analysis. Surv. Ophthalmol. 2021, 66, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Ramtohul, P.; Parrat, E.; Denis, D.; Lorenzi, U. Inverted Internal Limiting Membrane Flap Technique versus Complete Internal Limiting Membrane Peeling in Large Macular Hole Surgery: A Comparative Study. BMC Ophthalmol. 2020, 20, 11. [Google Scholar] [CrossRef]
- Tam, A.L.C.; Yan, P.; Gan, N.Y.; Lam, W.-C. The current surgical management of large, recurrent, or persistent macular holes. Retina 2018, 38, 1263–1275. [Google Scholar] [CrossRef]
- Ullrich, S. Macular Hole Size as a Prognostic Factor in Macular Hole Surgery. Br. J. Ophthalmol. 2002, 86, 390–393. [Google Scholar] [CrossRef]
- Kusuhara, S.; Teraoka Escaño, M.F.; Fujii, S.; Nakanishi, Y.; Tamura, Y.; Nagai, A.; Yamamoto, H.; Tsukahara, Y.; Negi, A. Prediction of Postoperative Visual Outcome Based on Hole Configuration by Optical Coherence Tomography in Eyes with Idiopathic Macular Holes. Am. J. Ophthalmol. 2004, 138, 709–716. [Google Scholar] [CrossRef]
- Ruiz-Moreno, J.M.; Staicu, C.; Pinero, D.P.; Montero, J.; Lugo, F.; Amat, P. Optical Coherence Tomography Predictive Factors for Macular Hole Surgery Outcome. Br. J. Ophthalmol. 2008, 92, 640–644. [Google Scholar] [CrossRef]
- Antonopoulou, P.G.; Baumann, C.; Jalil, A.; Dhawahir-Scala, F.; Muñoz-Sanz, N.; Lu, V.H.J.; Park, D.; Patton, N. How Big Is the Hole? Measuring Intra- and Inter-Individual Agreement in Macular Hole Size Measurements. Curr. Eye Res. 2020, 45, 1000–1004. [Google Scholar] [CrossRef]
- Karn, P.K.; Abdulla, W.H. On Machine Learning in Clinical Interpretation of Retinal Diseases Using OCT Images. Bioengineering 2023, 10, 407. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Chen, Y.; Li, H.; Zhang, Y.; Yao, X.; Meng, Y.; Shi, W.; Liang, Y.; Hu, Y.; Liu, D.; et al. Machine Learning and Optical Coherence Tomography-Derived Radiomics Analysis to Predict Persistent Diabetic Macular Edema in Patients Undergoing Anti-VEGF Intravitreal Therapy. J. Transl. Med. 2024, 22, 358. [Google Scholar] [CrossRef] [PubMed]
- Balyen, L.; Peto, T. Promising Artificial Intelligence-Machine Learning-Deep Learning Algorithms in Ophthalmology. Asia Pac. J. Ophthalmol. 2019, 8, 264–272. [Google Scholar] [CrossRef]
- Lu, W.; Tong, Y.; Yu, Y.; Xing, Y.; Chen, C.; Shen, Y. Applications of Artificial Intelligence in Ophthalmology: General Overview. J. Ophthalmol. 2018, 2018, 1–15. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic Minority Over-Sampling Technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Shen, W.; Song, Z.; Zhong, X.; Huang, M.; Shen, D.; Gao, P.; Qian, X.; Wang, M.; He, X.; Wang, T.; et al. Sangerbox: A Comprehensive, Interaction-friendly Clinical Bioinformatics Analysis Platform. iMeta 2022, 1, e36. [Google Scholar] [CrossRef]
- Yao, Y.; Qu, J.; Dong, C.; Li, X.; Liang, J.; Yin, H.; Huang, L.; Li, Y.; Liu, P.; Pan, C.; et al. The Impact of Extent of Internal Limiting Membrane Peeling on Anatomical Outcomes of Macular Hole Surgery: Results of a 54-week Randomized Clinical Trial. Acta Ophthalmol. 2019, 97, 303–312. [Google Scholar] [CrossRef]
- Chhablani, J.; Khodani, M.; Hussein, A.; Bondalapati, S.; Rao, H.B.; Narayanan, R.; Sudhalkar, A. Role of Macular Hole Angle in Macular Hole Closure. Br. J. Ophthalmol. 2015, 99, 1634–1638. [Google Scholar] [CrossRef] [PubMed]
- Bajdik, B.; Vajas, A.; Kemenes, G.; Fodor, M.; Surányi, É.; Takács, L. Prediction of Long-Term Visual Outcome of Idiopathic Full-Thickness Macular Hole Surgery Using Optical Coherence Tomography Parameters That Estimate Potential Preoperative Photoreceptor Damage. Graefe’s Arch. Clin. Exp. Ophthalmol. 2024. [Google Scholar] [CrossRef]
- Xiao, Y.; Hu, Y.; Quan, W.; Yang, Y.; Lai, W.; Wang, X.; Zhang, X.; Zhang, B.; Wu, Y.; Wu, Q.; et al. Development and Validation of a Deep Learning System to Classify Aetiology and Predict Anatomical Outcomes of Macular Hole. Br. J. Ophthalmol. 2023, 107, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Zgolli, H.; El Zarrug, H.H.k.; Meddeb, M.; Mabrouk, S.; Khlifa, N. Anatomical Prognosis after Idiopathic Macular Hole Surgery: Machine Learning Based-Predection. Libyan J. Med. 2022, 17, 2034334. [Google Scholar] [CrossRef]
- Xiao, Y.; Hu, Y.; Quan, W.; Zhang, B.; Wu, Y.; Wu, Q.; Liu, B.; Zeng, X.; Lin, Z.; Fang, Y.; et al. Machine Learning-Based Prediction of Anatomical Outcome after Idiopathic Macular Hole Surgery. Ann. Transl. Med. 2021, 9, 830. [Google Scholar] [CrossRef]
- Lachance, A.; Godbout, M.; Antaki, F.; Hébert, M.; Bourgault, S.; Caissie, M.; Tourville, É.; Durand, A.; Dirani, A. Predicting Visual Improvement After Macular Hole Surgery: A Combined Model Using Deep Learning and Clinical Features. Trans. Vis. Sci. Tech. 2022, 11, 6. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Xie, P.; Ding, Y.; Zheng, X.; Yuan, D.; Liu, Q. Face-down or No Face-down Posturing Following Macular Hole Surgery: A Meta-analysis. Acta Ophthalmol. 2016, 94, 326–333. [Google Scholar] [CrossRef]
- Yuksel, K.; Goker, Y.S.; Yazici, A.T.; Ozkaya, A.; Cosar, G. Can Perifoveal Pseudocyst Area Be a Prognostic Factor in Macular Hole Surgery? Medicine 2014, 93, e182. [Google Scholar] [CrossRef]


| Variables | Total (n = 200) | Training Set (n = 140) | Test Set (n = 60) | p |
|---|---|---|---|---|
| Age, years, M (IQR) | 61.00 (12.00) | 61.00 (13.25) | 61.00 (10.00) | 0.393 f |
| Age groups, n (%) | 0.086 g | |||
| <40 | 17 (8.50) | 2 (2.33) | 15 (10.71) | |
| ≥40 | 183 (91.50) | 58 (96.67) | 125 (89.29) | |
| Sex, n (%) | 0.492 g | |||
| Female | 133 (66.50) | 91 (65.00) | 42 (70.00) | |
| Male | 67 (33.50) | 49 (35.00) | 18 (30.00) | |
| Laterality, n (%) | 0.951 g | |||
| Right | 106 (53.00) | 74 (52.86) | 32 (53.33) | |
| Left | 94 (47.00) | 66 (47.14) | 28 (46.67) | |
| Outcome, n (%) | 0.619 g | |||
| Closed | 173 (86.50) | 53 (88.33) | 120 (85.71) | |
| Open | 27 (13.50) | 20 (14.29) | 7 (11.67) | |
| High myopia, n (%) | 0.387 g | |||
| No | 170 (85.00) | 121 (86.43) | 49 (81.67) | |
| Yes | 30 (15.00) | 19 (13.57) | 11 (18.33) | |
| Surgery, n (%) | 0.055 g | |||
| ILM peeling a | 136 (68.00) | 101 (72.14) | 35 (58.33) | |
| ILM flap b | 64 (32.00) | 39 (27.86) | 25 (41.67) | |
| Size of FTMH c, n (%) | 0.947 g | |||
| Large | 122 (61.00) | 36 (60.00) | 86 (61.43) | |
| Medium | 43 (17.00) | 11 (18.33) | 23 (16.43) | |
| Small | 44 (22.00) | 13 (21.67) | 31 (2214) | |
| Examination interval d, day, M (IQR) | 59.00 (194.25) | 70.50 (230.75) | 55.50 (168.5) | 0.156 f |
| BCVA (logMAR) e, M (IQR) | 1.00 (0.57) | 1.00 (0.60) | 0.92 (0.40) | 0.895 f |
| BASE, μm, M (IQR) | 965.50 (591.00) | 953.00 (546.5) | 1059.50 (598.5) | 0.570 f |
| MIN, μm, M (IQR) | 478.00 (377.75) | 478.00 (318.50) | 486.00 427.75) | 0.657 f |
| N, μm, M (IQR) | 330.50 (198.00) | 334.00 (195.25) | 327.00 (215.75) | 0.915 f |
| T, μm, M (IQR) | 325.00 (196.75) | 327.00 (195.25) | 318.00 (214.25) | 0.832 f |
| H, μm, M (IQR) | 428.50 (108.50) | 428.00 (106.00) | 430.50 (126.25) | 0.719 f |
| HFF, M (IQR) | 0.73 (0.27) | 0.72 (0.26) | 0.74 (0.27) | 0.897 f |
| MHI, M (IQR) | 0.44 (0.24) | 0.45 (0.23) | 0.43 (0.24) | 0.617 f |
| DHI, M (IQR) | 0.51 (0.27) | 0.51 (0.26) | 0.47 (0.28) | 0.542 f |
| THI, M (IQR) | 0.92 (0.90) | 0.88 (0.86) | 0.95 (0.96) | 0.996 f |
| Training Set | Test Set | |||||
|---|---|---|---|---|---|---|
| Logistic | SVM | BPNN | Logistic | SVM | BPNN | |
| SEN | 0.967 | 0.942 | 0.942 | 0.925 | 0.887 | 0.925 |
| SPE | 0.975 | 0.975 | 0.958 | 0.857 | 0.857 | 1.000 |
| ACC | 0.971 | 0.958 | 0.950 | 0.917 | 0.883 | 0.933 |
| PPV | 0.975 | 0.974 | 0.958 | 0.980 | 0.979 | 1.000 |
| NPV | 0.967 | 0.944 | 0.943 | 0.600 | 0.500 | 0.636 |
| F1 | 0.971 | 0.958 | 0.950 | 0.951 | 0.931 | 0.961 |
| AUC | 0.998 | 0.988 | 0.995 | 0.941 | 0.943 | 0.968 |
| Algorithm | MH | Surgery Type | Eyes (Patients) (n) | Country | SEN | SPE | ACC | AUC | |
|---|---|---|---|---|---|---|---|---|---|
| Xiao (2021) [33] | Random forest | Full-thickness IMH | ILM peeling | 288 | China | 0.973 | 0.904 | 0.892 | 0.951 |
| ZGOLLI (2022) [34] | MDSS | Full-thickness IMH | IML flap | 120 (114) | Tunis | \ | \ | \ | 0.967 |
| Xiao (2023) [35] | MDFN | Full-thickness IMH | ILM peeling | 209 | China | 0.979 | 0.815 | 0.875 | 0.947 |
| Xiao (2023) [35] | MDFN | FTMH | ILM peeling | 330 | China | 0.766 | 0.977 | 0.825 | 0.904 |
| Our models | Logistic | FTMH | ILM peeling or IML flap | 200 (193) | China | 0.925 | 0.857 | 0.917 | 0.941 |
| SVM | 0.887 | 0.857 | 0.883 | 0.943 | |||||
| BPNN | 0.925 | 1 | 0.933 | 0.968 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Meng, Y.; Liang, Y.; Zhang, Y.; Chen, B.; Qiu, J.; Meng, Z.; Luo, J. Machine Learning and Optical-Coherence-Tomography-Derived Radiomics Analysis to Predict the Postoperative Anatomical Outcome of Full-Thickness Macular Hole. Bioengineering 2024, 11, 949. https://doi.org/10.3390/bioengineering11090949
Hu Y, Meng Y, Liang Y, Zhang Y, Chen B, Qiu J, Meng Z, Luo J. Machine Learning and Optical-Coherence-Tomography-Derived Radiomics Analysis to Predict the Postoperative Anatomical Outcome of Full-Thickness Macular Hole. Bioengineering. 2024; 11(9):949. https://doi.org/10.3390/bioengineering11090949
Chicago/Turabian StyleHu, Yuqian, Yongan Meng, Youling Liang, Yiwei Zhang, Biying Chen, Jianing Qiu, Zhishang Meng, and Jing Luo. 2024. "Machine Learning and Optical-Coherence-Tomography-Derived Radiomics Analysis to Predict the Postoperative Anatomical Outcome of Full-Thickness Macular Hole" Bioengineering 11, no. 9: 949. https://doi.org/10.3390/bioengineering11090949
APA StyleHu, Y., Meng, Y., Liang, Y., Zhang, Y., Chen, B., Qiu, J., Meng, Z., & Luo, J. (2024). Machine Learning and Optical-Coherence-Tomography-Derived Radiomics Analysis to Predict the Postoperative Anatomical Outcome of Full-Thickness Macular Hole. Bioengineering, 11(9), 949. https://doi.org/10.3390/bioengineering11090949