


Inconsistency in Shoulder Arthrometers for Measuring Glenohumeral Joint Laxity: A Systematic Review

 , ,
, ,  ,
, 

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
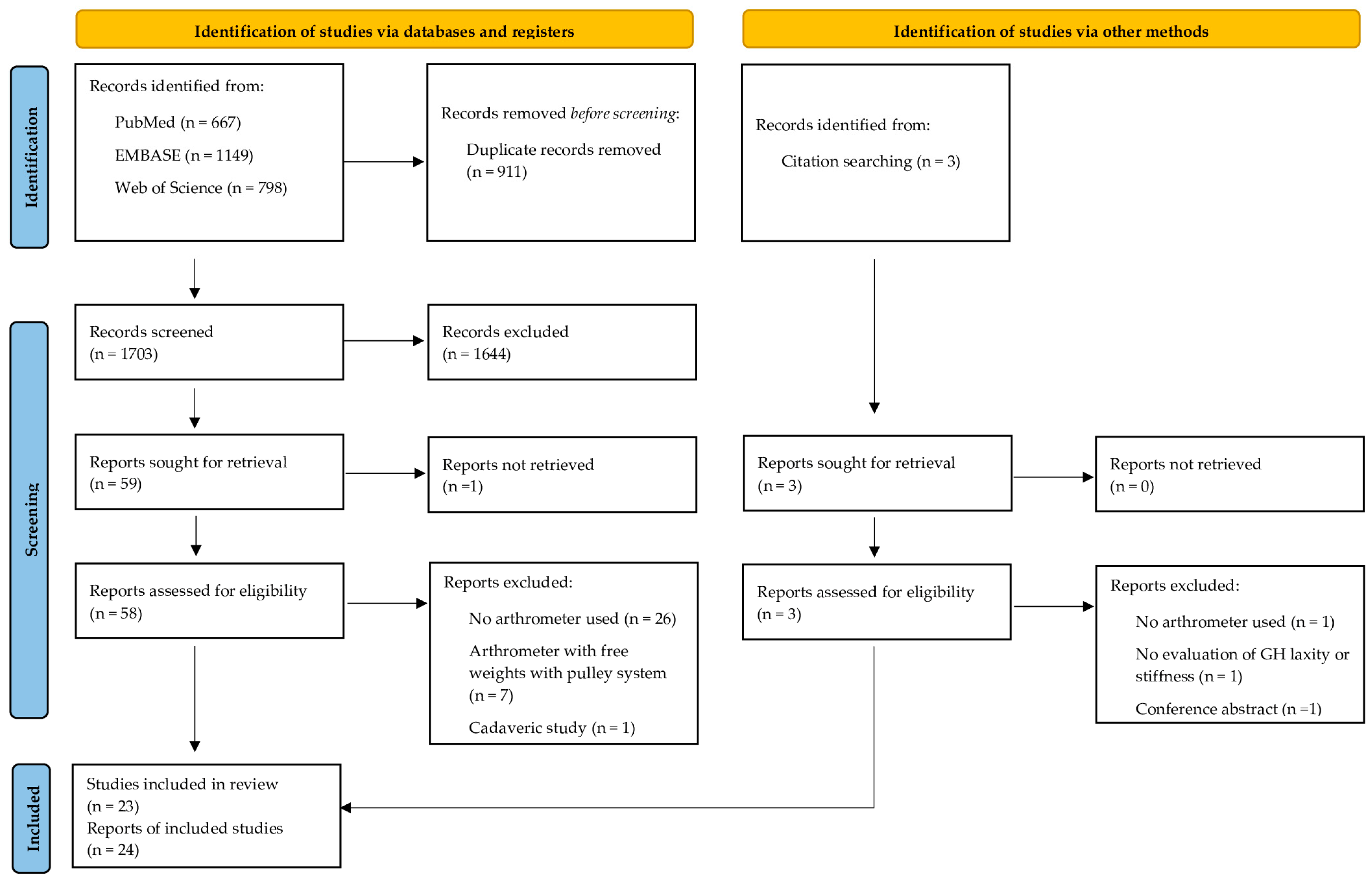
2.3. Study Selection
2.4. Data Collection and Extraction
2.5. Data Management
2.6. Risk of Bias
2.7. Data Synthesis
3. Results
3.1. Risk of Bias
3.2. Population Characteristics
3.3. Device Characteristics
3.4. Characteristics of Evaluation and Method of Measurement
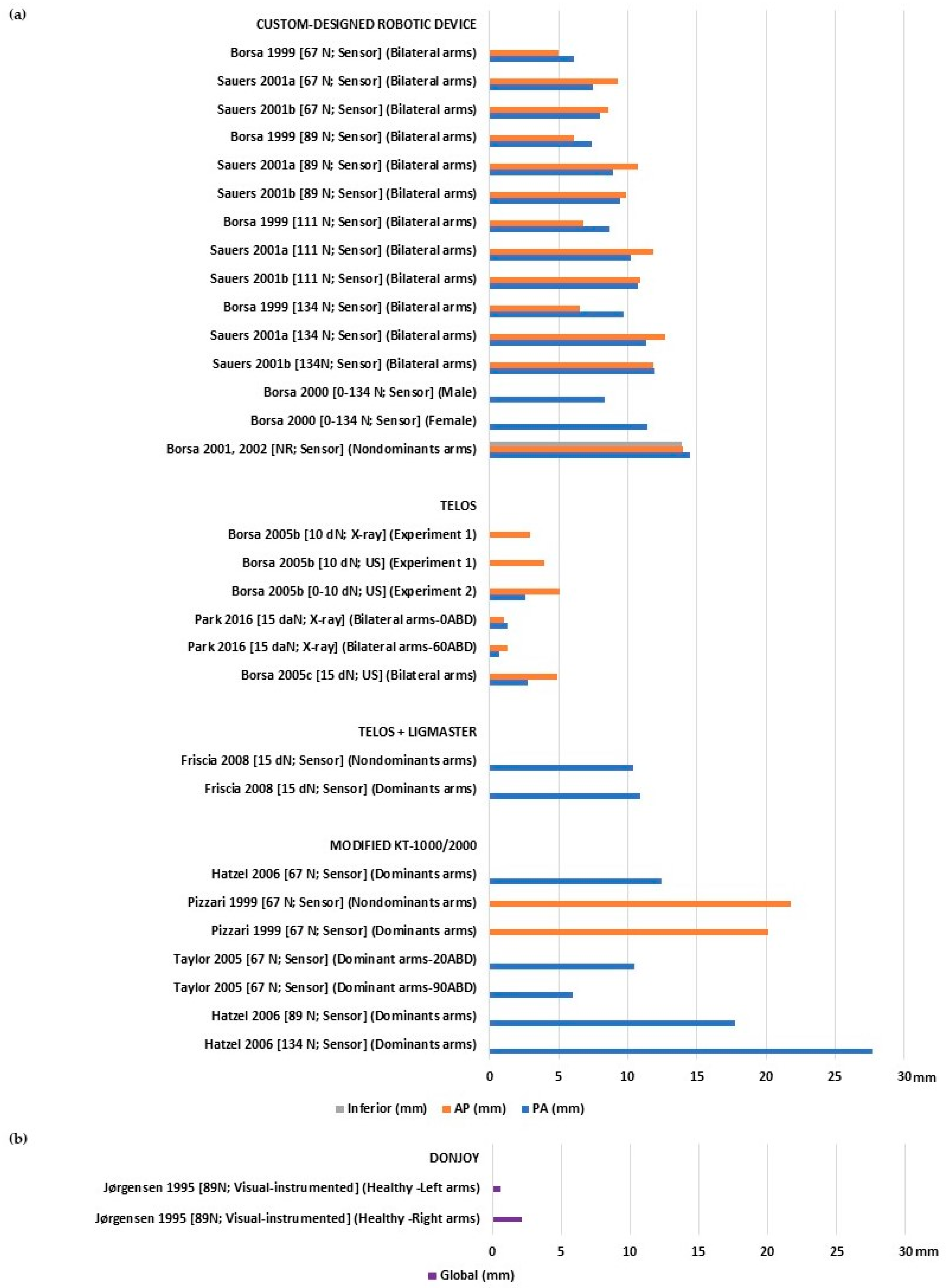
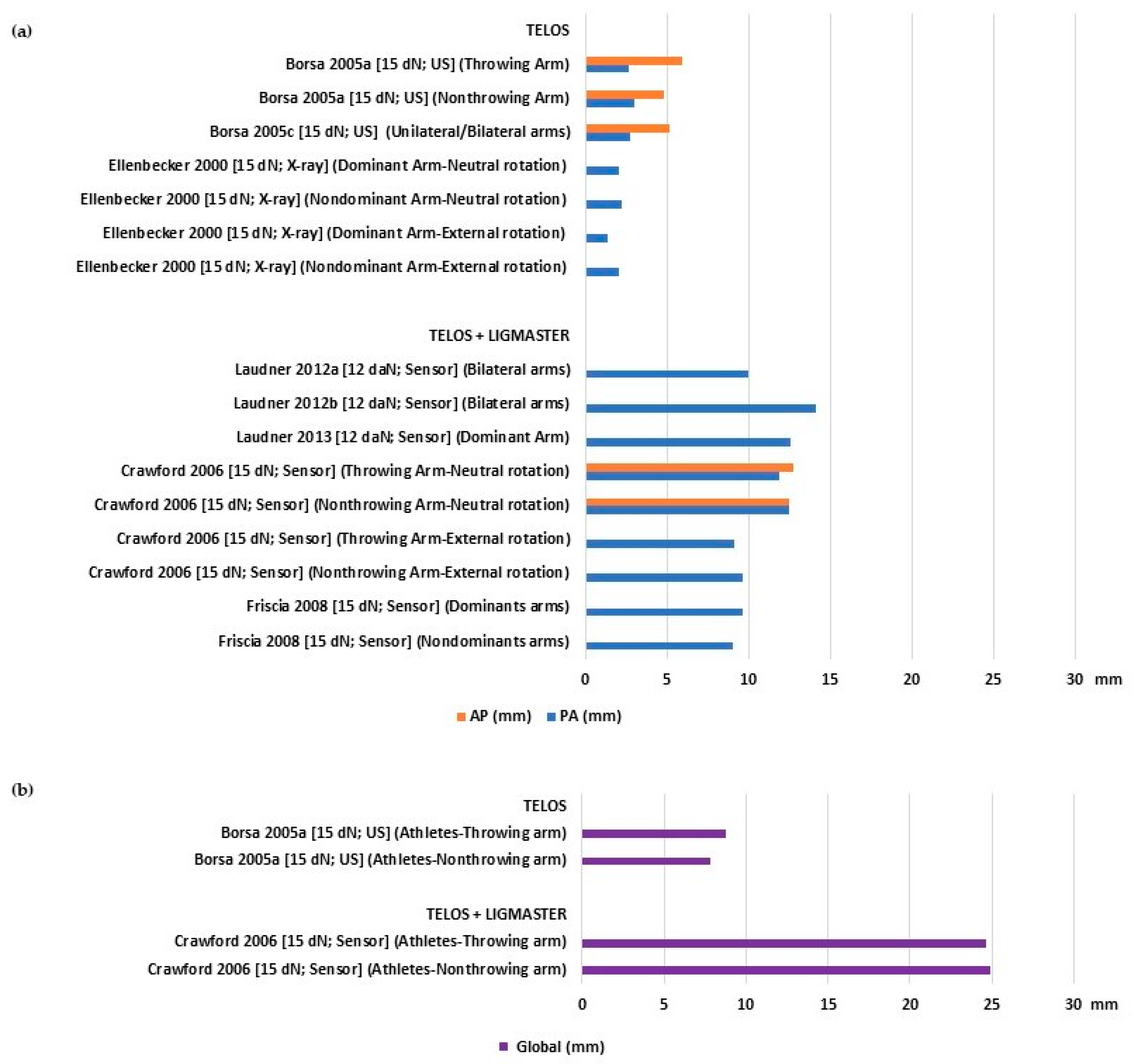
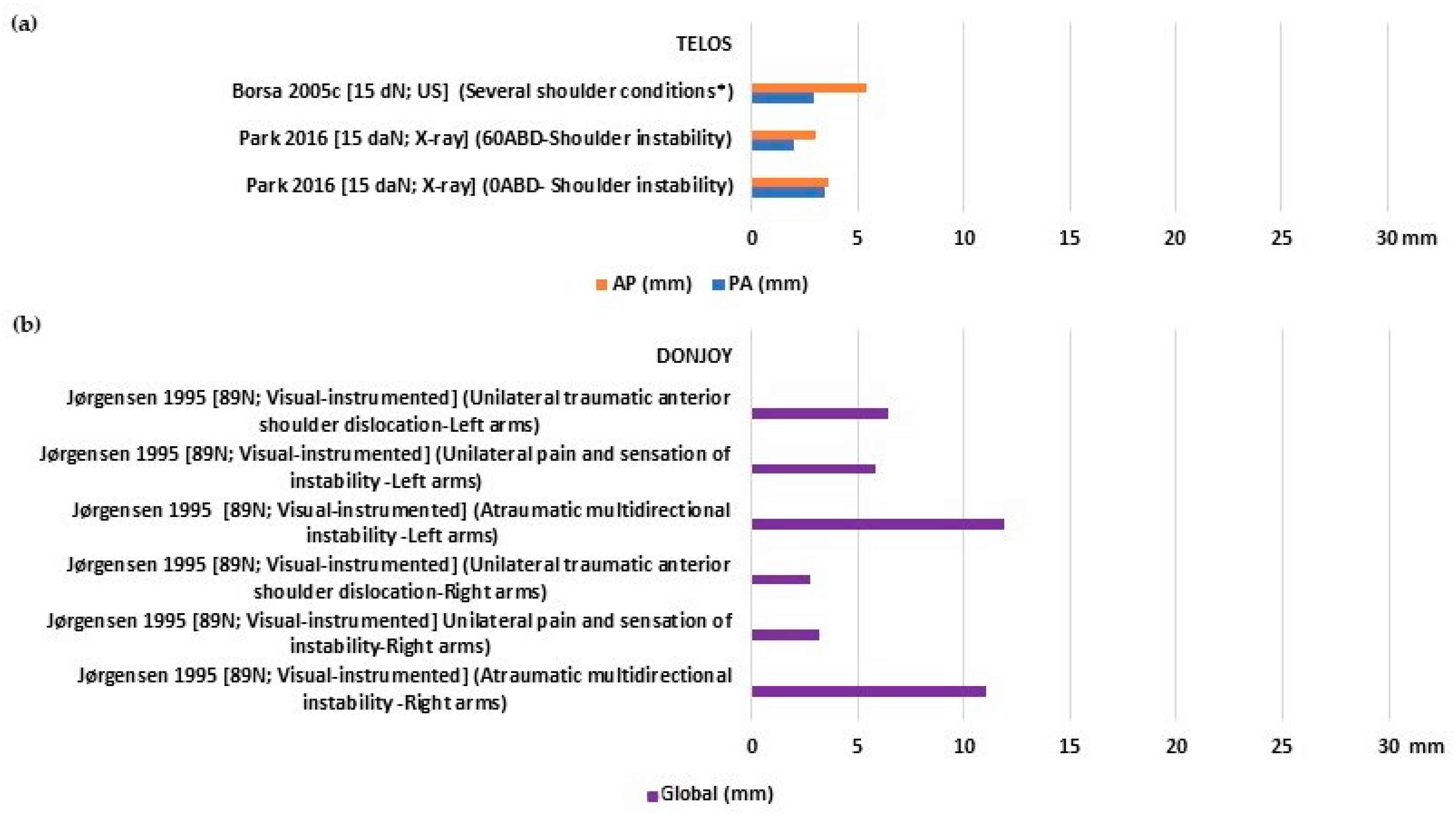
3.5. Laxity and Stiffness Values
4. Discussion
4.1. Why Are the Laxity Outcomes So Variable across Studies?
4.2. Is GH Laxity Symmetric and What Are the Differences between Symptomatic and Asymptomatic Shoulders?
4.3. Recommendations for Clinical Practice and Future Directions
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shah, A.; Judge, A.; Delmestri, A.; Edwards, K.; Arden, N.K.; Prieto-Alhambra, D.; Holt, T.A.; Pinedo-Villanueva, R.A.; Hopewell, S.; Lamb, S.E.; et al. Incidence of shoulder dislocations in the UK, 1995–2015: A population-based cohort study. BMJ Open 2017, 7, e016112. [Google Scholar] [CrossRef]
- Taş, M.; Canbora, M.K.; Kose, O.; Eğerci, F.; Gem, M. Demographic and clinical characteristics of traumatic shoulder dislocations in an urban city of Turkey: A retrospective analysis of 208 cases. Acta Orthop. Traumatol. Turc. 2013, 47, 147–152. [Google Scholar] [CrossRef]
- Szyluk, K.; Niemiec, P.; Sieroń, D.; Lukoszek, D.; Gierek, M.; Lorek, A.; Christe, A. Shoulder Dislocation Incidence and Risk Factors-Rural vs. Urban Populations of Poland. Int. J. Environ. Res. Public Health 2022, 19, 11857. [Google Scholar] [CrossRef]
- Shields, D.W.; Jefferies, J.G.; Brooksbank, A.J.; Millar, N.; Jenkins, P.J. Epidemiology of glenohumeral dislocation and subsequent instability in an urban population. J. Shoulder Elb. Surg. 2018, 27, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Zacchilli, M.A.; Owens, B.D. Epidemiology of Shoulder Dislocations Presenting to Emergency Departments in the United States. J. Bone Jt. Surg. 2010, 92, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Twomey-Kozak, J.; Whitlock, K.G.; O’donnell, J.A.; Anakwenze, O.A.; Klifto, C.S. Shoulder dislocations among high school–aged and college-aged athletes in the United States: An epidemiologic analysis. JSES Int. 2021, 5, 967–971. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.W.; Corlette, J.; Collins, C.L.; Comstock, R.D. Shoulder Injuries Among US High School Athletes, 2005/2006–2011/2012. Pediatrics 2014, 133, 272–279. [Google Scholar] [CrossRef]
- Owens, B.D.; Dawson, L.; Burks, R.; Cameron, K.L. Incidence of Shoulder Dislocation in the United States Military: Demographic Considerations from a High-Risk Population. J. Bone Jt. Surg. 2009, 91, 791–796. [Google Scholar] [CrossRef]
- Kardouni, J.R.; Mckinnon, C.J.; Seitz, A.L. Incidence of Shoulder Dislocations and the Rate of Recurrent Instability in Soldiers. Med. Sci. Sports Exerc. 2016, 48, 2150–2156. [Google Scholar] [CrossRef]
- Headey, J.; Brooks, J.H.M.; Kemp, S.P.T. The Epidemiology of Shoulder Injuries in English Professional Rugby Union. Am. J. Sports Med. 2007, 35, 1537–1543. [Google Scholar] [CrossRef]
- Szyluk, K.; Jasiński, A.; Niemiec, P.; Mielnik, M.; Koczy, B. Five-year prevalence of recurrent shoulder dislocation in the entire Polish population. Int. Orthop. 2018, 42, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.M.; Seah, M.; Akhtar, M.A. The Epidemiology, Risk of Recurrence, and Functional Outcome After an Acute Traumatic Posterior Dislocation of the Shoulder. J. Bone Jt. Surg. 2011, 93, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, E.J.; Goode, A.; Campbell, S.; Morin, A.; Tamaddoni, M.; Moorman, C.T.; Cook, C. Physical examination tests of the shoulder: A systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2008, 42, 80–92. [Google Scholar] [CrossRef]
- Santiago, F.R.; Martínez, A.M.; Muñoz, P.T.; Sánchez, J.P.; Pérez, A.Z. Imaging of shoulder instability. Quant. Imaging Med. Surg. 2017, 7, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Hegedus, E.J.; Goode, A.P.; Cook, C.E.; Michener, L.; Myer, C.A.; Myer, D.M.; Wright, A.A. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2012, 46, 964–978. [Google Scholar] [CrossRef] [PubMed]
- Bahk, M.; Keyurapan, E.; Tasaki, A.; Sauers, E.L.; McFarland, E.G. Laxity testing of the shoulder: A review. Am. J. Sports Med. 2007, 35, 131–144. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.-J.; Sheen, S.-S.; Hahn, S.; Jang, B.-H.; Son, H.-J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef]
- Azarsa, M.H.; Mirbagheri, A.; Hosseini, S.R.; Shadmehr, A.; Karimi, N. Objective measurement of Inferior-Directed stiffness in glenohumeral joint using a specially designed robotic device in healthy shoulders; Within- and Between-Session reliability. J. Biomech. 2021, 127, 110663. [Google Scholar] [CrossRef]
- Borsa, P.; Sauers, E.L.; Herling, D.E. In Vivo Assessment of AP Laxity in Healthy Shoulders Using an Instrumented Arthrometer. J. Sport Rehabil. 1999, 8, 157–170. [Google Scholar] [CrossRef]
- Borsa, P.A.; Sauers, E.L.; Herling, D.E. Patterns of glenohumeral joint laxity and stiffness in healthy men and women. Med. Sci. Sports Exerc. 2000, 32, 1685–1690. [Google Scholar] [CrossRef] [PubMed]
- Borsa, P.A.; Sauers, E.L.; Herling, D.E.; Manzour, W.F. In Vivo Quantification of Capsular End Point in the Nonimpaired Glenohumeral Joint Using an Instrumented Measurement System. J. Orthop. Sports Phys. Ther. 2001, 31, 419–426, discussion 427–431. [Google Scholar] [CrossRef] [PubMed]
- Borsa, P.A.; Sauers, E.L.; Herling, D.E. Glenohumeral Stiffness Response Between Men and Women for Anterior, Posterior, and Inferior Translation. J. Athl. Train. 2002, 37, 240–245. [Google Scholar]
- Borsa, P.A.; Wilk, K.E.; Jacobson, J.A.; Scibek, J.S.; Dover, G.C.; Reinold, M.M.; Andrews, J.R. Correlation of Range of Motion and Glenohumeral Translation in Professional Baseball Pitchers. Am. J. Sports Med. 2005, 33, 1392–1399. [Google Scholar] [CrossRef] [PubMed]
- Borsa, P.A.; Jacobson, J.A.; Scibek, J.S.; Dover, G.C. Comparison of Dynamic Sonography to Stress Radiography for Assessing Glenohumeral Laxity in Asymptomatic Shoulders. Am. J. Sports Med. 2005, 33, 734–741. [Google Scholar] [CrossRef]
- Borsa, P.A.; Scibek, J.S.; Jacobson, J.A.; Meister, K. Sonographic Stress Measurement of Glenohumeral Joint Laxity in Collegiate Swimmers and Age-Matched Controls. Am. J. Sports Med. 2005, 33, 1077–1084. [Google Scholar] [CrossRef]
- Borsa, P.A.; Dover, G.C.; Wilk, K.E.; Reinold, M.M. Glenohumeral Range of Motion and Stiffness in Professional Baseball Pitchers. Med. Sci. Sports Exerc. 2006, 38, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Crawford, S.D.; Sauers, E.L. Glenohumeral joint laxity and stiffness in the functional throwing position of high school baseball pitchers. J. Athl. Train. 2006, 41, 52–59. [Google Scholar]
- Ellenbecker, T.S.; Mattalino, A.J.; Elam, E.; Caplinger, R. Quantification of Anterior Translation of the Humeral Head in the Throwing Shoulder. Am. J. Sports Med. 2000, 28, 161–167. [Google Scholar] [CrossRef]
- Friscia, B.A.; Hammill, R.R.; McGuire, B.A.; Hertel, J.N.; Ingersoll, C.D. Anterior shoulder laxity is not correlated with medial elbow laxity in high school baseball players. J. Sport Rehabil. 2008, 17, 106–118. [Google Scholar] [CrossRef]
- Hatzel, B.; Horodyski, M.; Kaminski, T.W.; Meister, K.; Powers, M.; Brunt, D. Measurement of glenohumeral joint laxity using the KT-2000 knee ligament arthrometer: Reliability analysis. Phys. Ther. Sport 2006, 7, 137–143. [Google Scholar] [CrossRef]
- Jørgensen, U.; Bak, K. Shoulder instability Assessment of anterior-posterior translation with a knee laxity tester. Acta Orthop. 1995, 66, 398–400. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, U.; Svend-Hansen, H.; Bak, K.; Pedersen, I. Recurrent post-traumatic anterior shoulder dislocation—Open versus arthroscopic repair. Knee Surg. Sports Traumatol. Arthrosc. 1999, 7, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.; Meister, K.; Noel, B.; Deter, T. Anterior Glenohumeral Laxity Is Associated with Posterior Shoulder Tightness Among Professional Baseball Pitchers. Am. J. Sports Med. 2012, 40, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.G.; Meister, K.; Kajiyama, S.; Noel, B. The Relationship Between Anterior Glenohumeral Laxity and Proprioception in Collegiate Baseball Players. Clin. J. Sport Med. 2012, 22, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.G.; Metz, B.; Thomas, D.Q. Anterior Glenohumeral Laxity and Stiffness After a Shoulder-Strengthening Program in Collegiate Cheerleaders. J. Athl. Train. 2013, 48, 25–30. [Google Scholar] [CrossRef]
- Park, J.-Y.; Kim, Y.; Oh, K.-S.; Lim, H.-K.; Kim, J.-Y. Stress radiography for clinical evaluation of anterior shoulder instability. J. Shoulder Elb. Surg. 2016, 25, e339–e347. [Google Scholar] [CrossRef]
- Pizzari, T.; Kolt, G.S.; Remedios, L. Measurement of Anterior-to-Posterior Translation of the Glenohumeral Joint Using the KT-1000. J. Orthop. Sports Phys. Ther. 1999, 29, 602–608. [Google Scholar] [CrossRef]
- Sauers, E.L.; Borsa, P.A.; Herling, D.E.; Stanley, R.D. Instrumented measurement of glenohumeral joint laxity: Reliability and normative data. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 34–41. [Google Scholar] [CrossRef]
- Sauers, E.L.; Borsa, P.A.; Herling, D.E.; Stanley, R.D. Instrumented Measurement of Glenohumeral Joint Laxity and its Relationship to Passive Range of Motion and Generalized Joint Laxity. Am. J. Sports Med. 2001, 29, 143–150. [Google Scholar] [CrossRef]
- Taylor, J.D.; Bandy, W.D. Intrarater reliability of the KT1000 arthrometer in determining anterior translation of the glenohumeral joint. Arch. Phys. Med. Rehabil. 2005, 86, 826–829. [Google Scholar] [CrossRef]
- Hazmy, C.H.W.; Parwathi, A. The epidemiology of shoulder dislocation in a state-hospital: A review of 106 cases. Med. J. Malays. 2005, 60, 17–21. [Google Scholar]
- Mahaffey, B.L.; Smith, P.A. Shoulder instability in young athletes. Am. Fam. Physician 1999, 59, 2773–2782, 2787. [Google Scholar] [PubMed]
- Barnes, L.A.F.; Jobin, C.M.; Popkin, C.A.; Ahmad, C.S. Athletes With Anterior Shoulder Instability: A Prospective Study on Player Perceptions of Injury and Treatment. Orthop. J. Sports Med. 2021, 9, 23259671211032239. [Google Scholar]
- Bakshi, N.; Freehill, M.T. The Overhead Athletes Shoulder. Sports Med. Arthrosc. Rev. 2018, 26, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Rodeo, S.A.; Nguyen, J.T.; Cavanaugh, J.T.; Patel, Y.; Adler, R.S. Clinical and Ultrasonographic Evaluations of the Shoulders of Elite Swimmers. Am. J. Sports Med. 2016, 44, 3214–3221. [Google Scholar] [CrossRef]
- Kolber, M.J.; Corrao, M. Shoulder Joint and Muscle Characteristics Among Healthy Female Recreational Weight Training Participants. J. Strength Cond. Res. 2011, 25, 231–241. [Google Scholar] [CrossRef]
- Saremi, H.; Yavarikia, A.; Jafari, N. Generalized Ligamentous Laxity: An Important Predisposing Factor for Shoulder Injuries in Athletes. Iran. Red Crescent Med. J. 2016, 18, e38903. [Google Scholar] [CrossRef]
- Hill, L.; Collins, M.; Posthumus, M. Risk factors for shoulder pain and injury in swimmers: A critical systematic review. Physician Sportsmed. 2015, 43, 412–420. [Google Scholar] [CrossRef]
- De Martino, I.; Rodeo, S.A. The Swimmer’s Shoulder: Multi-directional Instability. Curr. Rev. Musculoskelet. Med. 2018, 11, 167–171. [Google Scholar] [CrossRef]
- Sugaya, H. Multidirectional Instability and Loose Shoulder in Athletes. In Sports Injuries to the Shoulder and Elbow; Park, J.-Y., Ed.; Springer Berlin Heidelberg: Berlin, Heidelberg, 2015; pp. 237–250. [Google Scholar]
- Burkhart, S.S.; Morgan, C.D. The peel-back mechanism: Its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthrosc. J. Arthrosc. Relat. Surg. 1998, 14, 637–640. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W.B. Shoulder Injuries in Overhead Athletes: The “Dead Arm” Revisited. Clin. Sports Med. 2000, 19, 125–158. [Google Scholar] [CrossRef]
- Burkhart, S.S.; Morgan, C.D.; Kibler, W. The disabled throwing shoulder: Spectrum of pathology part I: Pathoanatomy and biomechanics. Arthrosc. J. Arthrosc. Relat. Surg. 2003, 19, 404–420. [Google Scholar] [CrossRef] [PubMed]
- Barber, F.; Morgan, C.D.; Burkhart, S.S.; Jobe, C.M. Current Contraversies Point Counterpoint Labrum/Biceps/Cuff Dysfunction in the Throwing Athlete. Arthrosc. J. Arthrosc. Relat. Surg. 1999, 15, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Ji, J.H.; Petersen, S.A.; Freehill, M.T.; McFarland, E.G. An Analysis of Shoulder Laxity in Patients Undergoing Shoulder Surgery. J. Bone Jt. Surg. 2009, 91, 2144–2150. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, E. How reliable are measurements with arthrometers? Knee Surg. Sport. Traumatol. Arthrosc. 2000, 8, 131. [Google Scholar] [CrossRef]
- Levy, A.S.; Lintner, S.; Kenter, K.; Speer, K.P. Intra- and Interobserver Reproducibility of the Shoulder Laxity Examination. Am. J. Sports Med. 1999, 27, 460–463. [Google Scholar] [CrossRef]
- Guerra-Pinto, F.; Andrade, R.; Diniz, P.; Neto, A.L.; Espregueira-Mendes, J.; Consciência, J.G. Lack of Definition of Chronic Ankle Instability With Arthrometer-Assisted Ankle Joint Stress Testing: A Systematic Review of In Vivo Studies. J. Foot Ankle Surg. 2021, 60, 1241–1253. [Google Scholar] [CrossRef]
- Guth, J.J.; Brophy, R.H.; Matava, M.J.; Steinmetz, R.G.; Smith, M.V. Stress Radiography Is a Reliable Method to Quantify Posterior Cruciate Ligament Insufficiency: A Systematic Review. Arthrosc. Sports Med. Rehabil. 2022, 4, e1851–e1860. [Google Scholar] [CrossRef]
- James, E.W.; Williams, B.T.; LaPrade, R.F. Stress Radiography for the Diagnosis of Knee Ligament Injuries: A Systematic Review. Clin. Orthop. Relat. Res. 2014, 472, 2644–2657. [Google Scholar] [CrossRef]
- Espregueira-Mendes, J.; Pereira, H.; Sevivas, N.; Passos, C.; Vasconcelos, J.C.; Monteiro, A.; Oliveira, J.M.; Reis, R.L. Assessment of rotatory laxity in anterior cruciate ligament-deficient knees using magnetic resonance imaging with Porto-knee testing device. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Bastos, R.; Andrade, R.; Vasta, S.; Pereira, R.; Papalia, R.; van der Merwe, W.; Rodeo, S.; Espregueira-Mendes, J. Tibiofemoral bone bruise volume is not associated with meniscal injury and knee laxity in patients with anterior cruciate ligament rupture. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3318–3326. [Google Scholar] [CrossRef] [PubMed]
- Leal, A.; Andrade, R.; Flores, P.; Silva, F.S.; Fulkerson, J.; Neyret, P.; Arendt, E.; Espregueira-Mendes, J. Unilateral anterior knee pain is associated with increased patellar lateral position after stressed lateral translation. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Leal, A.; Andrade, R.; Hinckel, B.B.; Tompkins, M.; Flores, P.; Silva, F.; Espregueira-Mendes, J.; Arendt, E. A new device for patellofemoral instrumented stress-testing provides good reliability and validity. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 389–397. [Google Scholar] [CrossRef]
- Leal, A.; Andrade, R.; Hinckel, B.; Tompkins, M.; Bastos, R.; Flores, P.; Samuel, F.; Espregueira-Mendes, J.; Arendt, E. Patients with different patellofemoral disorders display a distinct ligament stiffness pattern under instrumented stress testing. J. ISAKOS Jt. Disord. Orthop. Sports Med. 2020, 5, 74–79. [Google Scholar] [CrossRef]
- Andrade, R.; Pereira, R.; Leal, A.; Pereira, B.; Boas, J.P.V.; van Dijk, C.N.; Espregueira-Mendes, J. Development of a medical device compatible with MRI/CT to measure ankle joint laxity: The Porto Ankle Testing Device. Porto Biomed. J. 2021, 6, e122. [Google Scholar] [CrossRef]
- Espregueira-Mendes, J.; Andrade, R.; Leal, A.; Pereira, H.; Skaf, A.; Rodrigues-Gomes, S.; Oliveira, J.M.; Reis, R.L.; Pereira, R. Global rotation has high sensitivity in ACL lesions within stress MRI. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 2993–3003. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Asymptomatic Shoulders | Injured Shoulders | Total Sample | |
|---|---|---|---|---|
| Healthy Individuals | Athletes | |||
| K (population) | 401 | 278 | 134 | 813 |
| N (shoulders) | 570 | 455 | 137 | 1162 |
| Sex (M/F) | 196/161 | 103/41 | 71/36 | 370/238 |
| Age (years) | 21.2 ± 7.2 | 21.5 ± 2.9 | 24.4 ± 7.7 | 23.0 ± 3.7 |
| Weight (kg) | 72.9 ± 6.1 | 83.6 ± 13.2 | NR | 79.3 ± 12.1 |
| Height (cm) | 171.7 ± 4.3 | 182.0 ± 7.7 | NR | 177.8 ± 8.5 |
| Population | Arthrometer | Studies | Amount of Load | Device | Evaluated Arms | PA | AP | Inferior |
|---|---|---|---|---|---|---|---|---|
| Healthy Individuals | Custom-designed robotic device | Azarsa et al. (2021) [19] | 10–80 N | Digital motion controller + software | Right arm | NR | NR | 1.51 |
| Customized instrumented shoulder arthrometer | Borsa et al. (2001,2002) [22,23] | NR | Sensor | Nondominant arms | 16.7 | 15.4 | 15.7 | |
| Borsa et al. (2000) [21] | 0–134 N | Sensor | Bilateral arms—male | 20.5 | NR | NR | ||
| Borsa et al. (2000) [21] | 0–134 N | Sensor | Bilateral arms—female | 16.3 | NR | NR | ||
| Healthy Athletes | Telos + Ligmaster | Crawford & Sauers (2006) [28] | 15 dN | Sensor | Throwing arm—neutral rotation | 8.05 | 8.00 | NR |
| Crawford & Sauers (2006) [28] | 15 dN | Sensor | Nonthrowing arm—neutral rotation | 7.77 | 8.05 | NR | ||
| Crawford & Sauers (2006) [28] | 15 dN | Sensor | Throwing arm—external rotation | 10.87 | NR | NR | ||
| Crawford & Sauers (2006) [28] | 15 dN | Sensor | Nonthrowing arm—external rotation | 10.24 | NR | NR | ||
| Borsa et al. (2006) [27] | 15 dN | Sensor | Throwing arm | 16.6 | 15.1 | NR | ||
| Borsa et al. (2006) [27] | 15 dN | Sensor | Nonthrowing arm | 16.2 | 15.3 | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, E.; Andrade, R.; Valente, C.; Santos, J.V.; Nunes, J.; Carvalho, Ó.; Correlo, V.M.; Silva, F.S.; Oliveira, J.M.; Reis, R.L.; et al. Inconsistency in Shoulder Arthrometers for Measuring Glenohumeral Joint Laxity: A Systematic Review. Bioengineering 2023, 10, 799. https://doi.org/10.3390/bioengineering10070799
Gomes E, Andrade R, Valente C, Santos JV, Nunes J, Carvalho Ó, Correlo VM, Silva FS, Oliveira JM, Reis RL, et al. Inconsistency in Shoulder Arthrometers for Measuring Glenohumeral Joint Laxity: A Systematic Review. Bioengineering. 2023; 10(7):799. https://doi.org/10.3390/bioengineering10070799
Chicago/Turabian StyleGomes, Eluana, Renato Andrade, Cristina Valente, J. Victor Santos, Jóni Nunes, Óscar Carvalho, Vitor M. Correlo, Filipe S. Silva, J. Miguel Oliveira, Rui L. Reis, and et al. 2023. "Inconsistency in Shoulder Arthrometers for Measuring Glenohumeral Joint Laxity: A Systematic Review" Bioengineering 10, no. 7: 799. https://doi.org/10.3390/bioengineering10070799
APA StyleGomes, E., Andrade, R., Valente, C., Santos, J. V., Nunes, J., Carvalho, Ó., Correlo, V. M., Silva, F. S., Oliveira, J. M., Reis, R. L., & Espregueira-Mendes, J. (2023). Inconsistency in Shoulder Arthrometers for Measuring Glenohumeral Joint Laxity: A Systematic Review. Bioengineering, 10(7), 799. https://doi.org/10.3390/bioengineering10070799