




In Vivo Assessment of Skin Surface Pattern: Exploring Its Potential as an Indicator of Bone Biomechanical Properties

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Osteogenesis Imperfecta and Non-Pathological Population
2.2. Senior Women Population
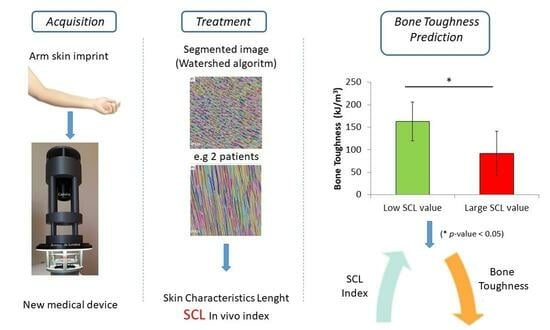
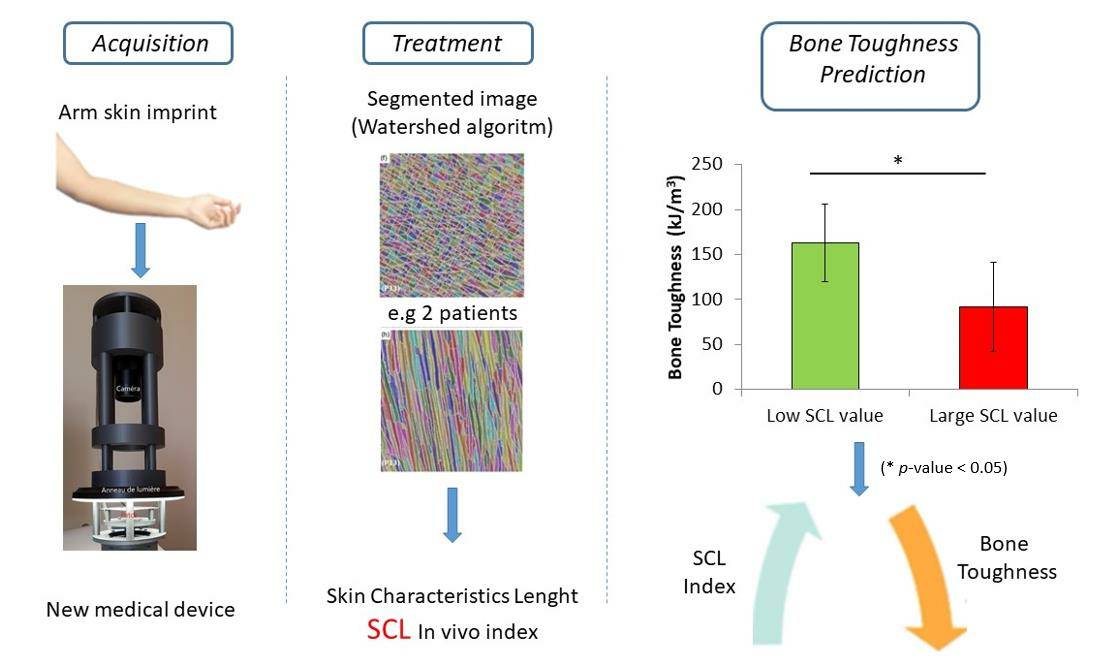
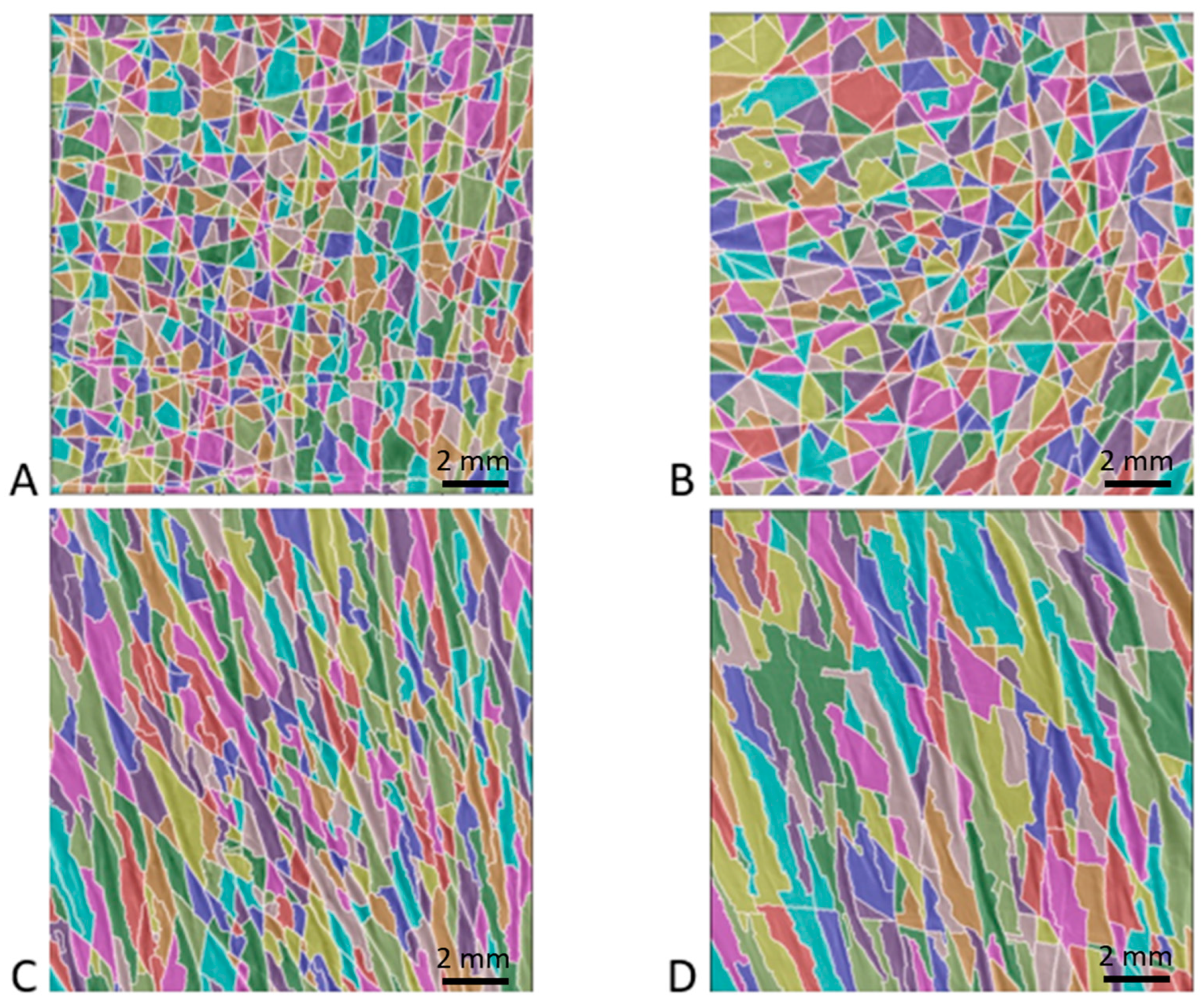
2.3. Skin Characteristic Length (SCL)
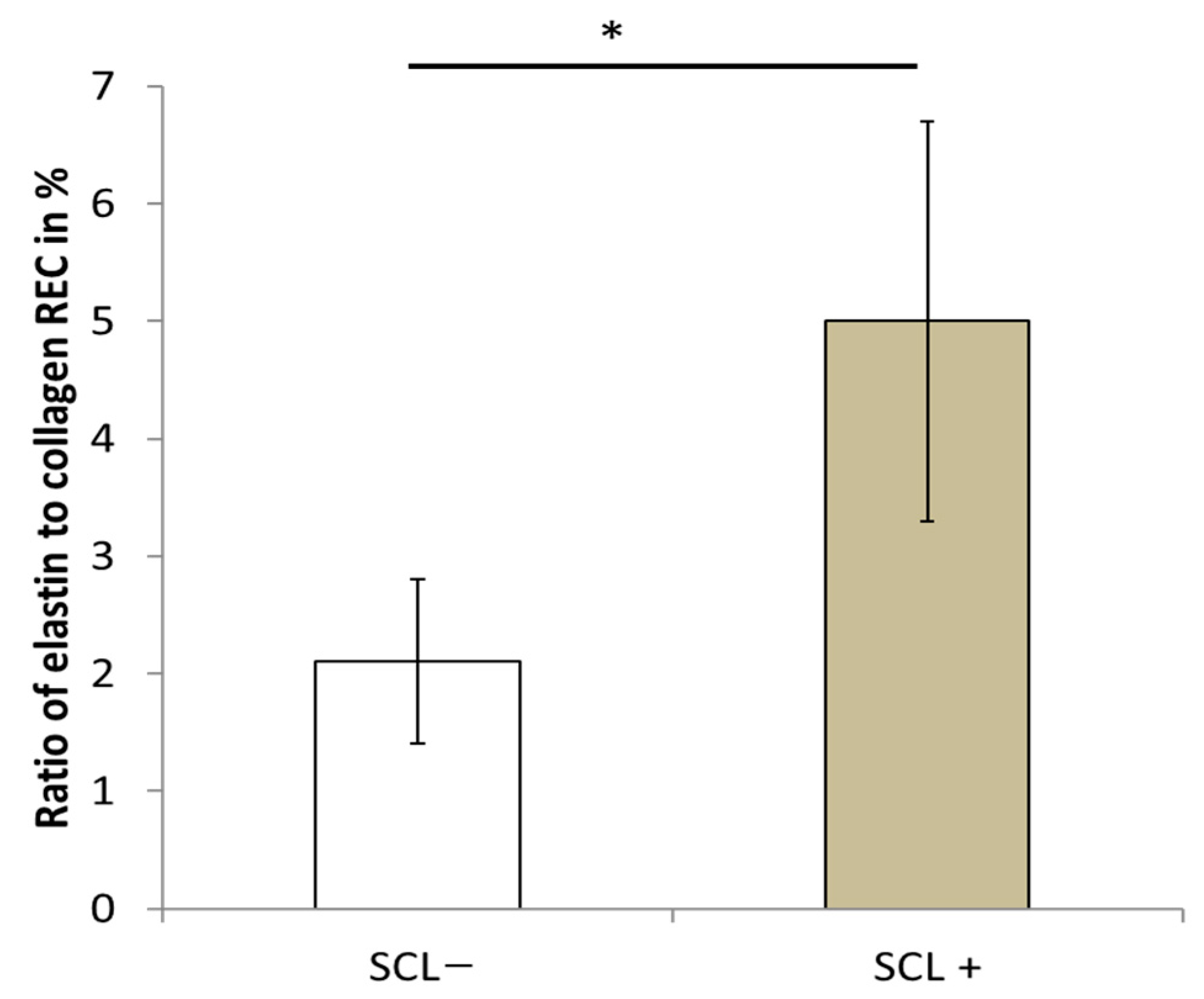
2.4. Ratio of Elastin to Collagen in the Dermis of Senior Women (REC)
2.5. Bone Volume Fraction of Trabecular Bone of Senior Women
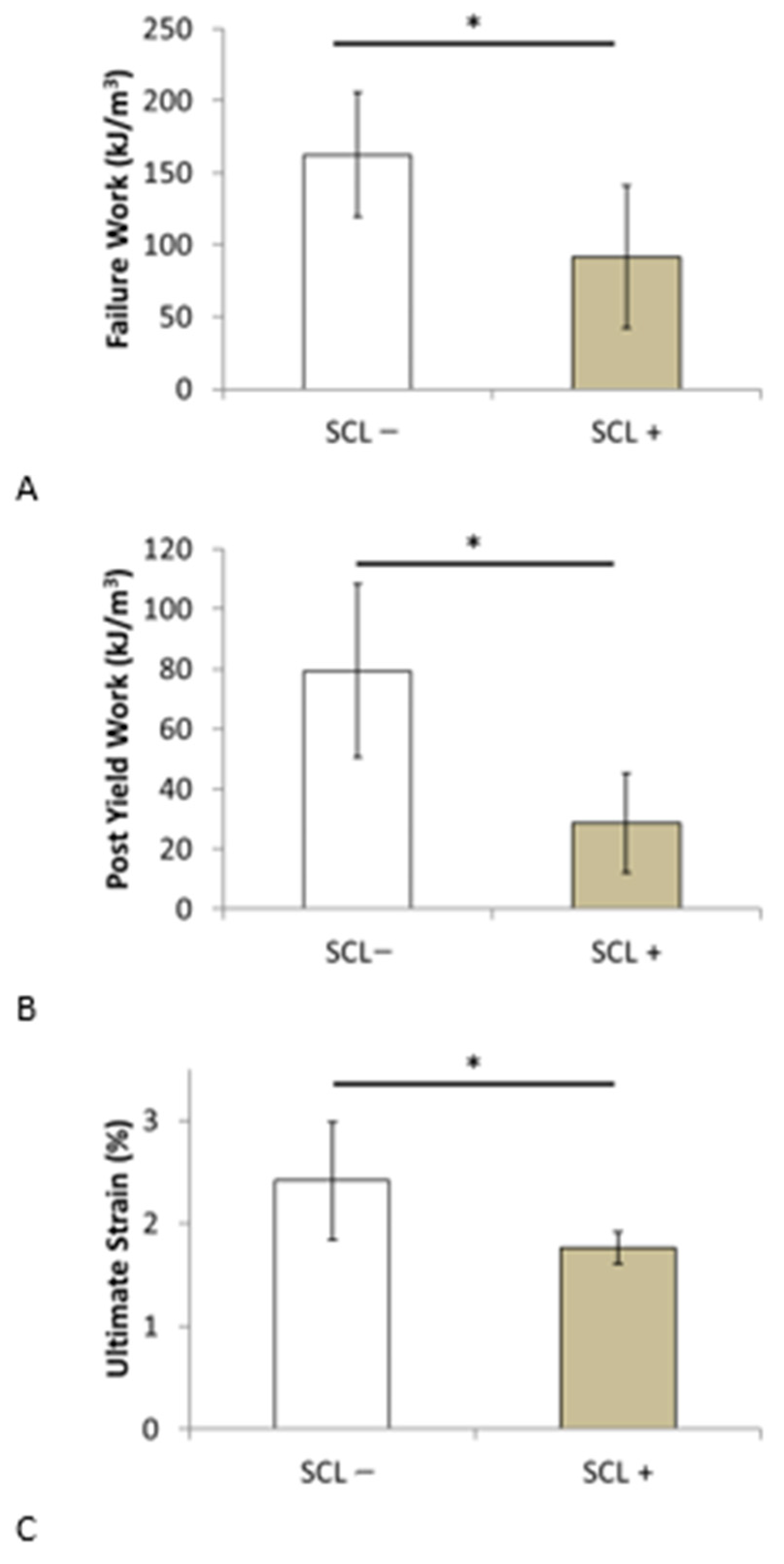
2.6. Uniaxial Mechanical Properties of Trabecular Bone
2.7. Statistical Analysis
3. Results
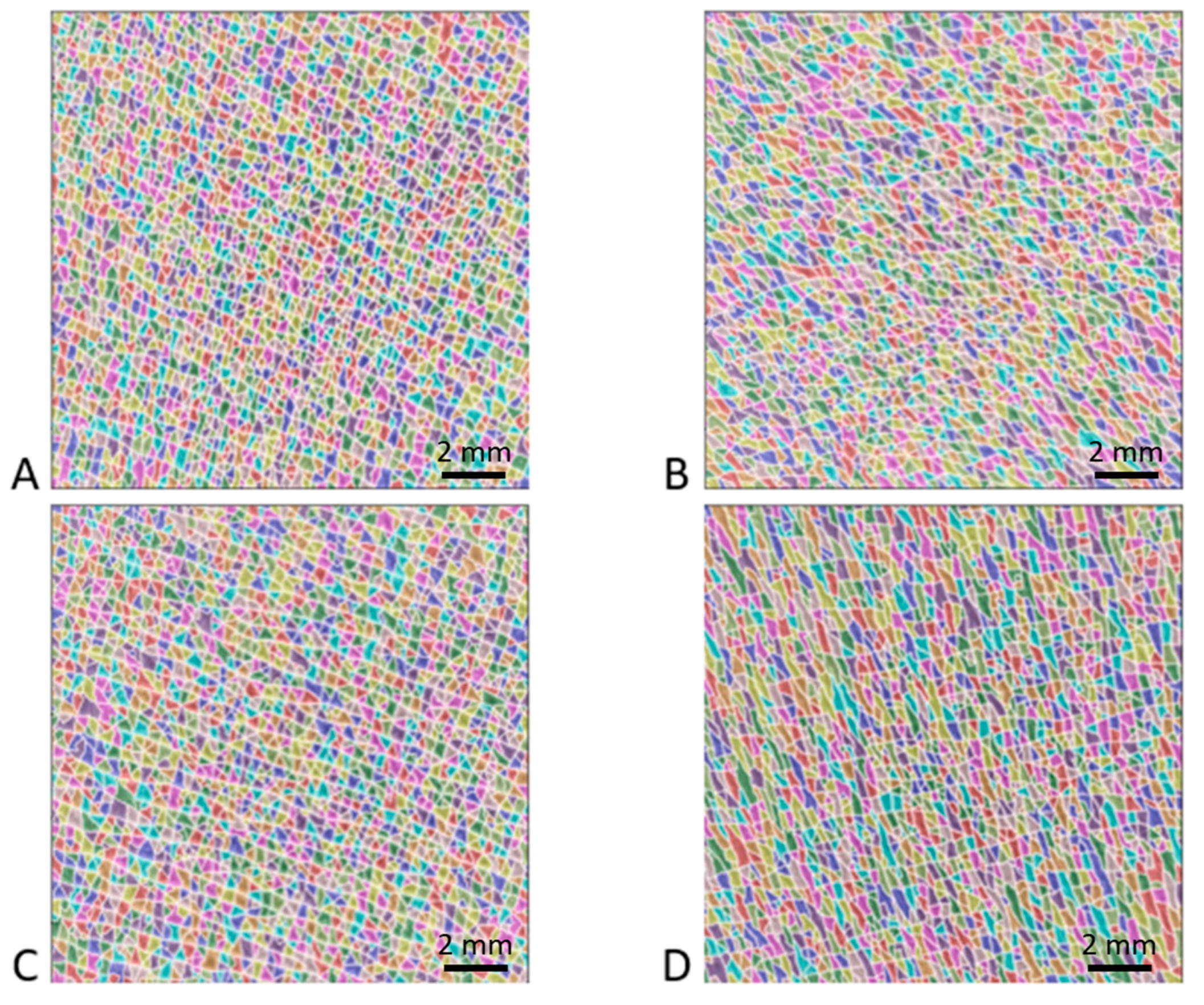
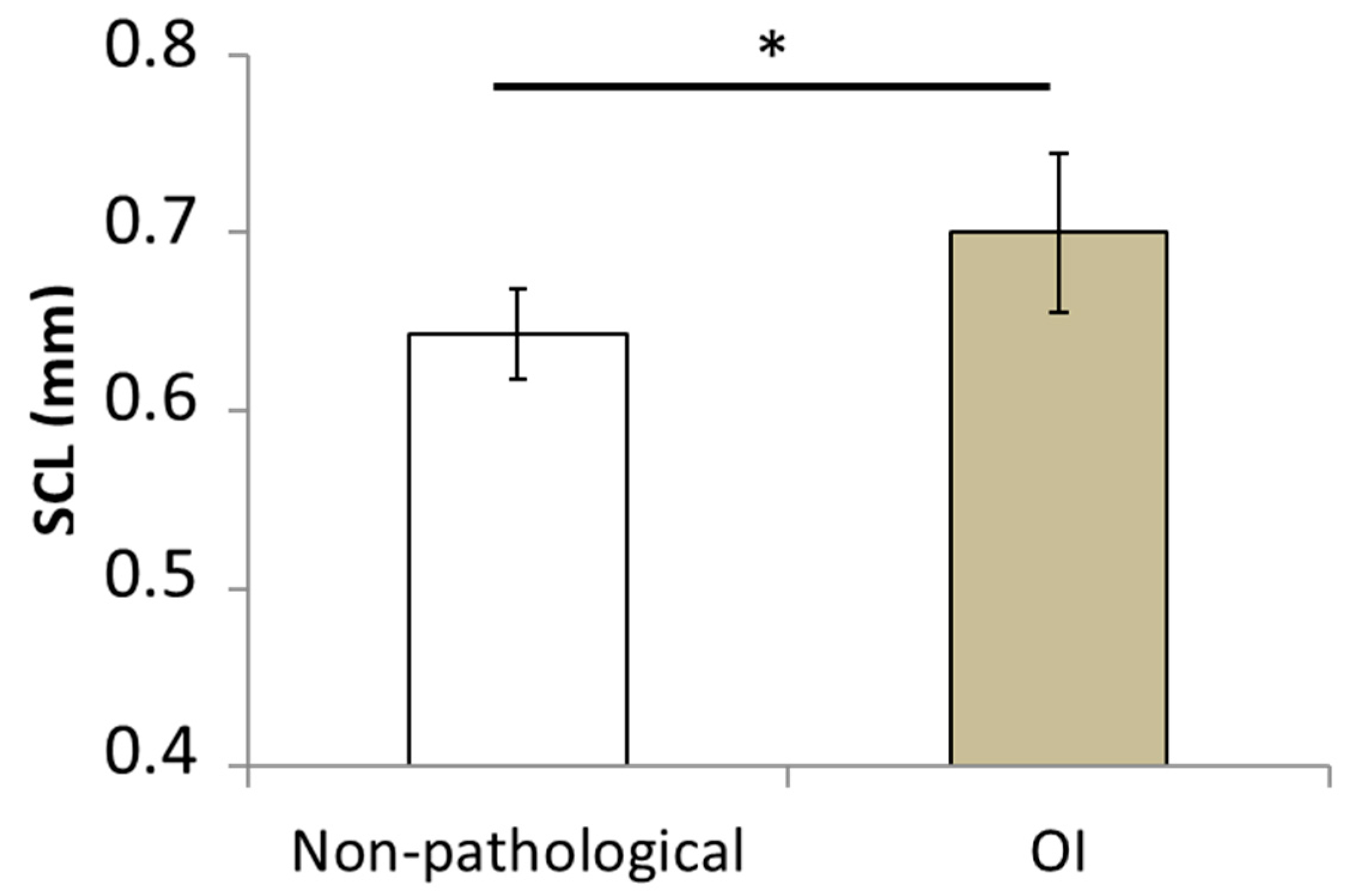
3.1. Effect of Osteogenesis Imperfecta on Skin Surface Morphology
3.2. Effect of Aging
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koons, G.L.; Diba, M.; Mikos, A.G. Materials design for bone-tissue engineering. Nat. Rev. Mater. 2020, 5, 584–603. [Google Scholar] [CrossRef]
- Akhavan, O.; Ghaderi, E.; Shahsavar, M. Graphene nanogrids for selective and fast osteogenic differentiation of human mesenchymal stem cells. Carbon 2013, 59, 200–211. [Google Scholar] [CrossRef]
- Bose, S.; Li, S.; Mele, E.; Silberschmidt, V.V. Fracture behaviour and toughening mechanisms of dry and wet collagen. Acta Biomater. 2022, 142, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.F.; Unnikrisnan, G.U.; Hussein, A.I. Bone Mechanical Properties in Healthy and Diseased States. Annu. Rev. Biomed. Eng. 2018, 20, 119–143. [Google Scholar] [CrossRef] [PubMed]
- Osterhoff, G.; Morgan, E.F.; Shefelbine, S.J.; Karim, L.; McNamara, L.M.; Augat, P. Bone mechanical properties and changes with osteoporosis. Injury 2016, 47, S11–S20. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Eastell, R.; Lui, L.-Y.; Wu, L.A.; de Papp, A.E.; Grauer, A.; Marin, F.; Cauley, J.A.; Bauer, D.C.; Black, D.M.; et al. Change in Bone Density and Reduction in Fracture Risk: A Meta-Regression of Published Trials. J. Bone Miner. Res. 2019, 34, 632–642. [Google Scholar] [CrossRef]
- Cosman, F.; de Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef]
- Heaney, R.P. Is the paradigm shifting? Bone 2003, 33, 457–465. [Google Scholar] [CrossRef]
- Hernandez, C.J.; van der Meulen, M.C. Understanding Bone Strength Is Not Enough. J. Bone Miner. Res. 2017, 32, 1157–1162. [Google Scholar] [CrossRef]
- Viguet-Carrin, S.; Garnero, P.; Delmas, P.D. The role of collagen in bone strength. Osteoporos. Int. 2006, 17, 319–336. [Google Scholar] [CrossRef]
- Fantner, G.E.; Birkedal, H.; Kindt, J.H.; Hassenkam, T.; Weaver, J.C.; Cutroni, J.A.; Bosma, B.L.; Bawazer, L.; Finch, M.M.; Cidade, G.A.G.; et al. Influence of the degradation of the organic matrix on the microscopic fracture behavior of trabecular bone. Bone 2004, 35, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Fratzl, P.; Weinkamer, R. Nature’s hierarchical materials. Prog. Mater. Sci. 2007, 52, 1263–1334. [Google Scholar] [CrossRef]
- Reznikov, N.; Bilton, M.; Lari, L.; Stevens, M.M.; Kröger, R. Fractal-like hierarchical organization of bone begins at the nanoscale. Science 2018, 360, eaao2189. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Meyers, M.A.; Ritchie, R.O. Structural architectures with toughening mechanisms in Nature: A review of the materials science of Type-I collagenous materials. Prog. Mater. Sci. 2019, 103, 425–483. [Google Scholar] [CrossRef]
- Boskey, A.L.; Coleman, R. Critical reviews in oral biology & medicine: Aging and bone. J. Dent. Res. 2010, 89, 1333–1348. [Google Scholar]
- Burr, D.B. Changes in bone matrix properties with aging. Bone 2019, 120, 85–93. [Google Scholar] [CrossRef]
- Xiong, Z.; Rouquier, L.; Chappard, C.; Bachy, M.; Huang, X.; Potier, E.; Bensidhoum, M.; Hoc, T. A New Microarchitecture-Based Parameter to Predict the Micromechanical Properties of Bone Allografts. Materials 2023, 16, 3349. [Google Scholar] [CrossRef]
- Nyman, J.S.; Roy, A.; Acuna, R.L.; Gayle, H.J.; Reyes, M.J.; Tyler, J.H.; Dean, D.D.; Wang, X. Age-related effect on the concentration of collagen crosslinks in human osteonal and interstitial bone tissue. Bone 2006, 39, 1210–1217. [Google Scholar] [CrossRef]
- Saito, M.; Marumo, K. Collagen cross-links as a determinant of bone quality: A possible explanation for bone fragility in aging, osteoporosis, and diabetes mellitus. Osteoporos. Int. 2010, 21, 195–214. [Google Scholar] [CrossRef]
- Bosser, C.; Ogier, A.; Imbert, L.; Hoc, T. Raman Spectroscopy as a Biomarker-Investigative Tool in Bone Metabolism. In Biomarkers in Bone Disease; Preedy, V.R., Ed.; Springer: Dordrecht, The Netherlands, 2016; pp. 1–27. ISBN 978-94-007-7745-3. [Google Scholar]
- Carretta, R.; Stüssi, E.; Müller, R.; Lorenzetti, S. Within subject heterogeneity in tissue-level post-yield mechanical and material properties in human trabecular bone. J. Mech. Behav. Biomed. Mater. 2013, 24, 64–73. [Google Scholar] [CrossRef]
- Chatzipanagis, K.; Baumann, C.G.; Sandri, M.; Sprio, S.; Tampieri, A.; Kröger, R. In situ mechanical and molecular investigations of collagen/apatite biomimetic composites combining Raman spectroscopy and stress-strain analysis. Acta Biomater. 2016, 46, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Fantner, G.E.; Hassenkam, T.; Kindt, J.H.; Weaver, J.C.; Birkedal, H.; Pechenik, L.; Cutroni, J.A.; Cidade, G.A.G.; Stucky, G.D.; Morse, D.E.; et al. Sacrificial bonds and hidden length dissipate energy as mineralized fibrils separate during bone fracture. Nat. Mater. 2005, 4, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Licini, C.; Notarstefano, V.; Marchi, S.; Cerqueni, G.; Ciapetti, G.; Vitale-Brovarone, C.; Giorgini, E.; Mattioli-Belmonte, M. Altered type I collagen networking in osteoporotic human femoral head revealed by histomorphometric and Fourier transform infrared imaging correlated analyses. BioFactors 2022, 48, 1089–1110. [Google Scholar] [CrossRef]
- Schwiedrzik, J.; Raghavan, R.; Bürki, A.; LeNader, V.; Wolfram, U.; Michler, J.; Zysset, P. In situ micropillar compression reveals superior strength and ductility but an absence of damage in lamellar bone. Nat. Mater. 2014, 13, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Buehler, M.J. Nature designs tough collagen: Explaining the nanostructure of collagen fibrils. Proc. Natl. Acad. Sci. USA 2006, 103, 12285–12290. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.K.; Gautieri, A.; Chang, S.-W.; Buehler, M.J. Molecular mechanics of mineralized collagen fibrils in bone. Nat. Commun. 2013, 4, 1724. [Google Scholar] [CrossRef]
- Wang, X.; Bank, R.A.; Tekoppele, J.M.; Agrawal, C.M. The role of collagen in determining bone mechanical properties. J. Orthop. Res. 2001, 19, 1021–1026. [Google Scholar] [CrossRef]
- Poundarik, A.A.; Wu, P.-C.; Evis, Z.; Sroga, G.E.; Ural, A.; Rubin, M.; Vashishth, D. A direct role of collagen glycation in bone fracture. J. Mech. Behav. Biomed. Mater. 2015, 52, 120–130. [Google Scholar] [CrossRef]
- Saito, M.; Marumo, K. Effects of Collagen Crosslinking on Bone Material Properties in Health and Disease. Calcif. Tissue Int. 2015, 97, 242–261. [Google Scholar] [CrossRef]
- Hans, D.; Goertzen, A.L.; Krieg, M.-A.; Leslie, W.D. Bone microarchitecture assessed by TBS predicts osteoporotic fractures independent of bone density: The manitoba study. J. Bone Miner. Res. 2011, 26, 2762–2769. [Google Scholar] [CrossRef]
- Ulivieri, F.M.; Rinaudo, L. Beyond Bone Mineral Density: A New Dual X-Ray Absorptiometry Index of Bone Strength to Predict Fragility Fractures, the Bone Strain Index. Front. Med. 2021, 7. [Google Scholar] [CrossRef] [PubMed]
- Hart, N.H.; Nimphius, S.; Rantalainen, T.; Ireland, A.; Siafarikas, A.; Newton, R.U. Mechanical basis of bone strength: Influence of bone material, bone structure and muscle action. J. Musculoskelet. Neuronal Interact. 2017, 17, 114–139. [Google Scholar] [PubMed]
- Shuster, S. Osteoporosis, a unitary hypothesis of collagen loss in skin and bone. Med. Hypotheses 2005, 65, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Shuster, S. Osteoporosis, like skin ageing, is caused by collagen loss which is reversible. J R Soc Med 2020, 113, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Cicchi, R.; Kapsokalyvas, D.; De Giorgi, V.; Maio, V.; Van Wiechen, A.; Massi, D.; Lotti, T.; Pavone, F.S. Scoring of collagen organization in healthy and diseased human dermis by multiphoton microscopy. J. Biophotonics 2010, 3, 34–43. [Google Scholar] [CrossRef]
- Koehler, M.J.; Hahn, S.; Preller, A.; Elsner, P.; Ziemer, M.; Bauer, A.; König, K.; Bückle, R.; Fluhr, J.W.; Kaatz, M. Morphological skin ageing criteria by multiphoton laser scanning tomography: Non-invasive in vivo scoring of the dermal fibre network. Exp. Dermatol. 2008, 17, 519–523. [Google Scholar] [CrossRef]
- Krueger, N.; Luebberding, S.; Oltmer, M.; Streker, M.; Kerscher, M. Age-related changes in skin mechanical properties: A quantitative evaluation of 120 female subjects. Ski. Res. Technol. 2011, 17, 141–148. [Google Scholar] [CrossRef]
- Trojahn, C.; Dobos, G.; Schario, M.; Ludriksone, L.; Blume-Peytavi, U.; Kottner, J. Relation between skin micro-topography, roughness, and skin age. Ski. Res. Technol. 2015, 21, 69–75. [Google Scholar] [CrossRef]
- Russell-Goldman, E.; Murphy, G.F. The Pathobiology of Skin Aging: New Insights into an Old Dilemma. Am. J. Pathol. 2020, 190, 1356–1369. [Google Scholar] [CrossRef]
- Wang, H.; Shyr, T.; Fevola, M.J.; Cula, G.O.; Stamatas, G.N. Age-related morphological changes of the dermal matrix in human skin documented in vivo by multiphoton microscopy. J. Biomed. Opt. 2018, 23. [Google Scholar] [CrossRef]
- Bachy, M.; Bosser, C.; Villain, B.; Aurégan, J.-C. Quantification of Microstructural Changes in the Dermis of Elderly Women Using Morphometric Indices of the Skin Surface. Materials 2022, 15, 8258. [Google Scholar] [CrossRef] [PubMed]
- Grafe, I.; Yang, T.; Alexander, S.; Homan, E.P.; Lietman, C.; Jiang, M.M.; Bertin, T.; Munivez, E.; Chen, Y.; Dawson, B.; et al. Excessive transforming growth factor-β signaling is a common mechanism in osteogenesis imperfecta. Nat. Med. 2014, 20, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Carriero, A.; Zimmermann, E.A.; Paluszny, A.; Tang, S.Y.; Bale, H.; Busse, B.; Alliston, T.; Kazakia, G.; Ritchie, R.O.; Shefelbine, S.J. How Tough Is Brittle Bone? Investigating Osteogenesis Imperfecta in Mouse Bone. J. Bone Miner. Res. 2014, 29, 1392–1401. [Google Scholar] [CrossRef]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Oden, A.; Ström, O.; Borgström, F. Development and use of FRAX® in osteoporosis. Osteoporos. Int. 2010, 21, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K. New methods for surface ultrastructure: Comparative studies of scanning electron microscopy, transmission electron microscopy and replica method. Int. J. Dermatol. 1974, 13, 357–381. [Google Scholar] [CrossRef]
- Sampson, J. A Method of replicating Dry or Moist Surfaces for Examination by Light Microscopy. Nature 1961, 191, 932–933. [Google Scholar] [CrossRef]
- Tang, S.Y.; Zeenath, U.; Vashishth, D. Effects of non-enzymatic glycation on cancellous bone fragility. Bone 2007, 40, 1144–1151. [Google Scholar] [CrossRef]
- Shuster, S.; Black, M.M.; McVitie, E. The influence of age and sex on skin thickness, skin collagen and density. Br. J. Dermatol. 1975, 93, 639–643. [Google Scholar] [CrossRef]
- Waller, J.M.; Maibach, H.I. Age and skin structure and function, a quantitative approach (II): Protein, glycosaminoglycan, water, and lipid content and structure. Ski. Res. Technol. 2006, 12, 145–154. [Google Scholar] [CrossRef]
- Lagarde, J.M.; Rouvrais, C.; Black, D. Topography and anisotropy of the skin surface with ageing. Ski. Res. Technol. 2005, 11, 110–119. [Google Scholar] [CrossRef]
- Mcconkey, B.; Fraser, G.M.; Bligh, A.S.; Whiteley, H. Transparent skin and osteoporosis. Lancet 1963, 281, 693–695. [Google Scholar] [CrossRef]
- Aurégan, J.-C.; Bosser, C.; Bensidhoum, M.; Bégué, T.; Hoc, T. Correlation between skin and bone parameters in women with postmenopausal osteoporosis: A systematic review. EFORT Open Rev. 2018, 3, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Castelo-Branco, C.; Pons, F.; Gratacós, E.; Fortuny, A.; Vanrell, J.A.; González-Merlo, J. Relationship between skin collagen and bone changes during aging. Maturitas 1994, 18, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Chappard, D.; Alexandre, C.; Robert, J.-M.; Riffat, G. Relationships between Bone and Skin Atrophies during Aging. Cells Tissues Organs 1991, 141, 239–244. [Google Scholar] [CrossRef]
- Patel, R.; Blake, G.M.; Fogelman, I. Evaluation of Osteoporosis Using Skin Thickness Measurements. Calcif. Tissue Int. 2007, 81, 442–449. [Google Scholar] [CrossRef]
- Haffer, H.; Chiapparelli, E.; Moser, M.; Muellner, M.; Dodo, Y.; Adl Amini, D.; Zhu, J.; Miller, T.T.; Han, Y.X.; Donnelly, E.; et al. Dermal ultrasound measurements for bone quality assessment: An investigation of advanced glycation endproducts derived from confocal fluorescence microscopy. J. Orthop. Res. 2023, 41, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Mortier, G.R.; Cohn, D.H.; Cormier-Daire, V.; Hall, C.; Krakow, D.; Mundlos, S.; Nishimura, G.; Robertson, S.; Sangiorgi, L.; Savarirayan, R.; et al. Nosology and classification of genetic skeletal disorders: 2019 revision. Am. J. Med. Genet. Part A 2019, 179, 2393–2419. [Google Scholar] [CrossRef]
- Sillence, D.O.; Senn, A.; Danks, D.M. Genetic heterogeneity in osteogenesis imperfecta. J. Med. Genet. 1979, 16, 101. [Google Scholar] [CrossRef]
- Holbrook, K.A.; Byers, P.H. Structural abnormalities in the dermal collagen and elastic matrix from the skin of patients with inherited connective tissue disorders. J. Investig. Dermatol. 1982, 79, 7–16. [Google Scholar] [CrossRef]
- Marini, J.C.; Forlino, A.; Bächinger, H.P.; Bishop, N.J.; Byers, P.H.; Paepe, A.D.; Fassier, F.; Fratzl-Zelman, N.; Kozloff, K.M.; Krakow, D.; et al. Osteogenesis imperfecta. Nat. Rev. Dis. Primers 2017, 3, 17052. [Google Scholar] [CrossRef]
- Pragnère, S.; Auregan, J.-C.; Bosser, C.; Linglart, A.; Bensidhoum, M.; Hoc, T.; Nouguier-Lehon, C.; Chaussain, C. Human dentin characteristics of patients with osteogenesis imperfecta: Insights into collagen-based biomaterials. Acta Biomater. 2021, 119, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Boskey, A.L.; Doty, S.B. Chapter 4—Mineralized Tissue: Histology, Biology and Biochemistry. In Osteogenesis Imperfecta; Shapiro, J.R., Byers, P.H., Glorieux, F.H., Sponseller, P.D., Eds.; Academic Press: San Diego, CA, USA, 2014; pp. 31–43. Available online: https://www.sciencedirect.com/science/article/pii/B9780123971654000046 (accessed on 22 October 2023).
- Cassella, J.P.; Barber, P.; Catterall, A.C.; Ali, S.Y. A Morphometric analysis of osteoid collagen fibril diameter in osteogenesis imperfecta. Bone 1994, 15, 329–334. [Google Scholar] [CrossRef]
- Fratzl, P.; Paris, O.; Klaushofer, K.; Landis, W.J. Bone mineralization in an osteogenesis imperfecta mouse model studied by small-angle x-ray scattering. J. Clin. Investig. 1996, 97, 396–402. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Imbert, L.; Aurégan, J.-C.; Pernelle, K.; Hoc, T. Mechanical and mineral properties of osteogenesis imperfecta human bones at the tissue level. Bone 2014, 65, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.A. The mechanical properties of trabecular bone: Dependence on anatomic location and function. J. Biomech. 1987, 20, 1055–1061. [Google Scholar] [CrossRef]
- Hunt, H.B.; Torres, A.M.; Palomino, P.M.; Marty, E.; Saiyed, R.; Cohn, M.; Jo, J.; Warner, S.; Sroga, G.E.; King, K.B.; et al. Altered Tissue Composition, Microarchitecture, and Mechanical Performance in Cancellous Bone From Men With Type 2 Diabetes Mellitus. J. Bone Miner. Res. 2019, 34, 1191–1206. [Google Scholar] [CrossRef] [PubMed]
- Kopperdahl, D.L.; Keaveny, T.M. Yield strain behavior of trabecular bone. J. Biomech. 1998, 31, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Røhl, L.; Larsen, E.; Linde, F.; Odgaard, A.; Jørgensen, J. Tensile and compressive properties of cancellous bone. J. Biomech. 1991, 24, 1143–1149. [Google Scholar] [CrossRef]
- Wang, X.; Shen, X.; Li, X.; Mauli Agrawal, C. Age-related changes in the collagen network and toughness of bone. Bone 2002, 31, 1–7. [Google Scholar] [CrossRef]
- Zioupos, P.; Currey, J.D. Changes in the Stiffness, Strength, and Toughness of Human Cortical Bone With Age. Bone 1998, 22, 57–66. [Google Scholar] [CrossRef]
- Vashishth, D.; Gibson, G.J.; Khoury, J.I.; Schaffler, M.B.; Kimura, J.; Fyhrie, D.P. Influence of nonenzymatic glycation on biomechanical properties of cortical bone. Bone 2001, 28, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Vörös, E.; Robert, C.; Robert, A.M. Age-Related Changes of the Human Skin Surface Microrelief. Gerontology 2009, 36, 276–285. [Google Scholar] [CrossRef]
- Gkogkolou, P.; Böhm, M. Advanced glycation end products: Key players in skin aging? Dermato-Endocrinology 2012, 4, 259–270. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OI N° | Sex | Age (Year) | Height (cm) | Weight (kg) | Non-Pathological N° | Sex | Age (Year) | Height (cm) | Weight (kg) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 8 | 119 | 24 | 1 | F | 10 | 134 | 23 |
| 2 | F | 10 | 106 | 20 | 2 | M | 13 | 158 | 46 |
| 3 | M | 12 | 147 | 52 | 3 | M | 15 | 175 | 60 |
| 4 | M | 12 | 147 | 38 | 4 | M | 15 | 181 | 80 |
| 5 | F | 13 | 148 | 37 | 5 | M | 15 | 172 | 60 |
| 6 | M | 13 | 159 | 43 | 6 | F | 15 | 170 | 60 |
| 7 | M | 13 | 125 | 30 | 7 | F | 17 | 163 | 53 |
| 8 | F | 14 | 152 | 35 | 8 | F | 17 | 170 | 52 |
| 9 | M | 14 | 155 | 55 | 9 | M | 17 | 180 | 75 |
| 10 | M | 14 | 152 | 34 | 10 | M | 17 | 182 | 78 |
| 11 | F | 15 | 159 | 59 | 11 | F | 20 | 170 | 50 |
| 12 | F | 16 | 127 | 31 | |||||
| 13 | M | 18 | 130 | 38 | |||||
| Mean value | 13.3 (±2.4) | 140 (±16) | 38.2 (±11) | 15.5 (±2.4) | 168 (±13) | 57.9 (±15.6) |
| Age (Years Old) | Weight (kg) | Height (in cm) | BMI | |
|---|---|---|---|---|
| 1 | 61 | 65 | 165 | 23.8 |
| 2 | 95 | 55 | 160 | 21.45 |
| 3 | 68 | 64 | 165 | 23.5 |
| 4 | 76 | 69 | 168 | 24.4 |
| 5 | 89 | 74 | 160 | 28.9 |
| 6 | 85 | 59 | 164 | 27.7 |
| 7 | 79 | 52 | 162 | 19.8 |
| 8 | 96 | 40 | 150 | 17.8 |
| 9 | 87 | 56 | 156 | 23. |
| 10 | 74 | 64 | 165 | 23.5 |
| 11 | 94 | 49 | 162 | 18.7 |
| 12 | 80 | 70 | 165 | 25.7 |
| 13 | 89 | 50 | 160 | 19.5 |
| 14 | 75 | 60 | 171 | 20.5 |
| 15 | 89 | 55 | 147 | 25.5 |
| 16 | 91 | 46 | 158 | 18.4 |
| 17 | 85 | 60 | 169 | 21. |
| 18 | 81 | 70 | 160 | 27.3 |
| 19 | 82 | 54 | 160 | 21.1 |
| 20 | 73 | 61 | 166 | 22.1 |
| 21 | 67 | 65 | 160 | 25.4 |
| 22 | 86 | 73 | 165 | 26.8 |
| Mean value | 81.9 (±9.3) | 59.6 (±8.8) | 161 (±.6.4) | 23 (±3.1) |
| OI N° | Mean Polygon Area (mm2) | Mean Perimeter Length (mm) | SCL (mm) | Non-Pathological N° | Mean Polygon Area (mm2) | Mean Perimeter Length (mm) | SCL (mm) |
|---|---|---|---|---|---|---|---|
| 1 | 0.092 | 1.42 | 0.65 | 1 | 0.078 | 1.31 | 0.60 |
| 2 | 0.086 | 1.4 | 0.64 | 2 | 0.079 | 1.31 | 0.6 |
| 3 | 0.11 | 1.71 | 0.75 | 3 | 0.085 | 1.37 | 0.63 |
| 4 | 0.11 | 1.54 | 0.71 | 4 | 0.085 | 1.44 | 0.65 |
| 5 | 0.12 | 1.64 | 0.75 | 5 | 0.093 | 1.44 | 0.66 |
| 6 | 0.096 | 1.45 | 0.67 | 6 | 0.09 | 1.39 | 0.64 |
| 7 | 0.107 | 1.52 | 0.7 | 7 | 0.1 | 1.51 | 0.69 |
| 8 | 0.12 | 1.67 | 0.76 | 8 | 0.09 | 1.43 | 0.65 |
| 9 | 0.093 | 1.47 | 0.67 | 9 | 0.098 | 1.48 | 0.68 |
| 10 | 0.1 | 1.44 | 0.67 | 10 | 0.095 | 1.44 | 0.66 |
| 11 | 0.11 | 1.59 | 0.72 | 11 | 0.092 | 1.43 | 0.66 |
| 12 | 0.135 | 1.73 | |||||
| 13 | 0.106 | 1.53 | |||||
| Mean value | 0.11 (±0.01) | 1.57 (±0.1) | 0.71 (±0.04) | 0.09 (±0.007) | 1.4 (±0.06) | 0.65 (±0.02) |
| Mean Value | Standard Deviation | Median Value | |
|---|---|---|---|
| E (MPa) | 710 | 322 | 678 |
| σy (MPa) | 9.43 | 4.3 | 9.4 |
| εy (%) | 1.51 | 0.31 | 1.44 |
| σm (MPa) | 10.2 | 4.59 | 10.8 |
| εu (%) | 2.08 | 0.53 | 1.88 |
| PYW (kJ/m3) | 54 | 34.6 | 53.6 |
| Wf (kJ/m3) | 127 | 58.3 | 133 |
| BV/TV (%) | 23.75 | 6.4 | 24.6 |
| SCL (mm) | 1.71 | 0.55 | 1.6 |
| N° | Mean Polygon Area (mm2) | Mean Perimeter Length (mm) | SCL (mm) | REC (%) |
|---|---|---|---|---|
| Group SCL− | ||||
| 21 | 0.16 | 2.0 | 0.90 | 1.25 |
| 7 | 0.22 | 2.3 | 1.05 | 2.30 |
| 15 | 0.21 | 2.4 | 1.06 | 1.45 |
| 20 | 0.24 | 2.4 | 1.10 | 2.19 |
| 19 | 0.27 | 2.6 | 1.18 | 2.21 |
| 16 | 0.32 | 2.8 | 1.29 | 1.22 |
| 22 | 0.34 | 3.0 | 1.35 | 2.70 |
| 17 | 0.37 | 3.0 | 1.36 | 0,60 |
| 2 | 0.36 | 3.0 | 1.37 | 3.00 |
| 18 | 0.39 | 3.3 | 1.46 | 1.40 |
| 12 | 0.47 | 3.5 | 1.56 | 3.08 |
| Group SCL+ | ||||
| 14 | 0.45 | 3.7 | 1.62 | 2.66 |
| 10 | 0.43 | 4.0 | 1.66 | 3.87 |
| 1 | 0.53 | 4.4 | 1.84 | 3.63 |
| 4 | 0.64 | 4.1 | 1.85 | 3.46 |
| 11 | 0.74 | 5.2 | 2.17 | 4.36 |
| 3 | 0.61 | 5.6 | 2.19 | 5.00 |
| 5 | 0.87 | 5.2 | 2.25 | 4.94 |
| 13 | 0.96 | 5.3 | 2.31 | 5.18 |
| 9 | 0.74 | 6.6 | 2.52 | 5.56 |
| 6 | 1.04 | 6.5 | 2.65 | 8.43 |
| 8 | 1.39 | 6.6 | 2.8 | 7.85 |
| SCL− (n = 11) | SCL+ (n = 11) | p Value | |
|---|---|---|---|
| Demographic Data | |||
| Age (Years) | 82.54 ± 7.6 | 81.27 ± 10.7 | 0.97 |
| Height (cm) | 161.1 ± 5.5 | 160.7 ± 7.2 | 0.97 |
| Weight (kg) | 60.1 ± 8.2 | 59.1 ± 9.3 | 0.89 |
| BMI (kg/m2) | 23.15 ± 2.9 | 22.85 ± 3.4 | 0.79 |
| Bone Parameters | |||
| E (MPa) | 729 ± 277.2 | 691 ± 360.5 | 0.56 |
| σy (MPa) | 10.52 ± 3.6 | 8.34 ± 4.6 | 0.29 |
| εy (%) | 1.61 ± 0.4 | 1.41 ± 0.14 | 0.49 |
| σm (MPa) | 11.34 ± 3.8 | 9.05 ± 4.89 | 0.37 |
| εu (%) | 2.41 ± 0.57 | 1.75 ± 0.15 | <0.05 |
| PYW (kJ/m3) | 79.3 ± 28.9 | 28.6 ± 16.6 | <0.05 |
| Wf (kJ/m3) | 162.6 ± 42.9 | 91.6 ± 49.4 | <0.05 |
| BV/TV (%) | 25.9 ± 5.4 | 21.5 ± 6.5 | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aurégan, J.-C.; Bosser, C.; Bachy-Razzouk, M.; Bensidhoum, M.; Hoc, T. In Vivo Assessment of Skin Surface Pattern: Exploring Its Potential as an Indicator of Bone Biomechanical Properties. Bioengineering 2023, 10, 1338. https://doi.org/10.3390/bioengineering10121338
Aurégan J-C, Bosser C, Bachy-Razzouk M, Bensidhoum M, Hoc T. In Vivo Assessment of Skin Surface Pattern: Exploring Its Potential as an Indicator of Bone Biomechanical Properties. Bioengineering. 2023; 10(12):1338. https://doi.org/10.3390/bioengineering10121338
Chicago/Turabian StyleAurégan, Jean-Charles, Catherine Bosser, Manon Bachy-Razzouk, Morad Bensidhoum, and Thierry Hoc. 2023. "In Vivo Assessment of Skin Surface Pattern: Exploring Its Potential as an Indicator of Bone Biomechanical Properties" Bioengineering 10, no. 12: 1338. https://doi.org/10.3390/bioengineering10121338
APA StyleAurégan, J.-C., Bosser, C., Bachy-Razzouk, M., Bensidhoum, M., & Hoc, T. (2023). In Vivo Assessment of Skin Surface Pattern: Exploring Its Potential as an Indicator of Bone Biomechanical Properties. Bioengineering, 10(12), 1338. https://doi.org/10.3390/bioengineering10121338