
Association Between Per- and Polyfluoroalkyl Substances and All-Cause Mortality in Diabetic Patients: Insights from a National Cohort Study and Toxicogenomic Analysis


Abstract
1. Introduction
2. Methods
2.1. Population-Based Cohort Study Analysis
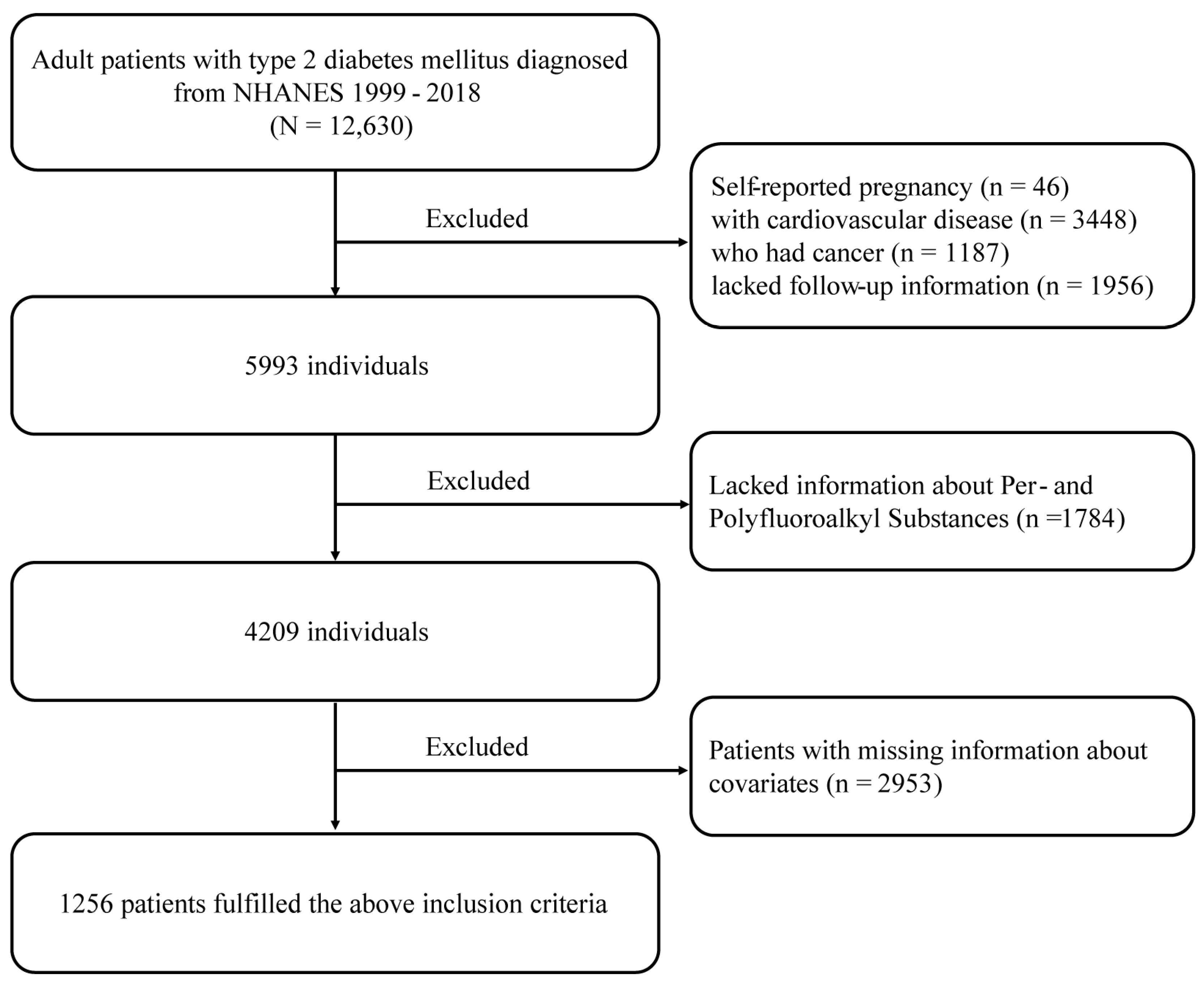
2.1.1. Research Population
2.1.2. Measurement of Serum PFAS Compounds
2.1.3. Definition of Outcome
2.1.4. The Use of Covariates
2.1.5. Statistical Analysis
2.2. Toxicogenomic Analysis
2.2.1. Identification of Potential Target Genes for PFAS Using Databases
2.2.2. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) Pathway Enrichment Analysis
2.2.3. Construction of PPI Network and Identification of Hub Genes
2.2.4. Chemical–Gene Interaction Patterns
3. Results
3.1. Baseline Characteristics
3.2. Logistic Regression Analysis of PFAS Compounds and Death in the DM Population
3.3. Assessing the Predictive Value of PFAS Compounds for All-Cause Mortality in DM Patients
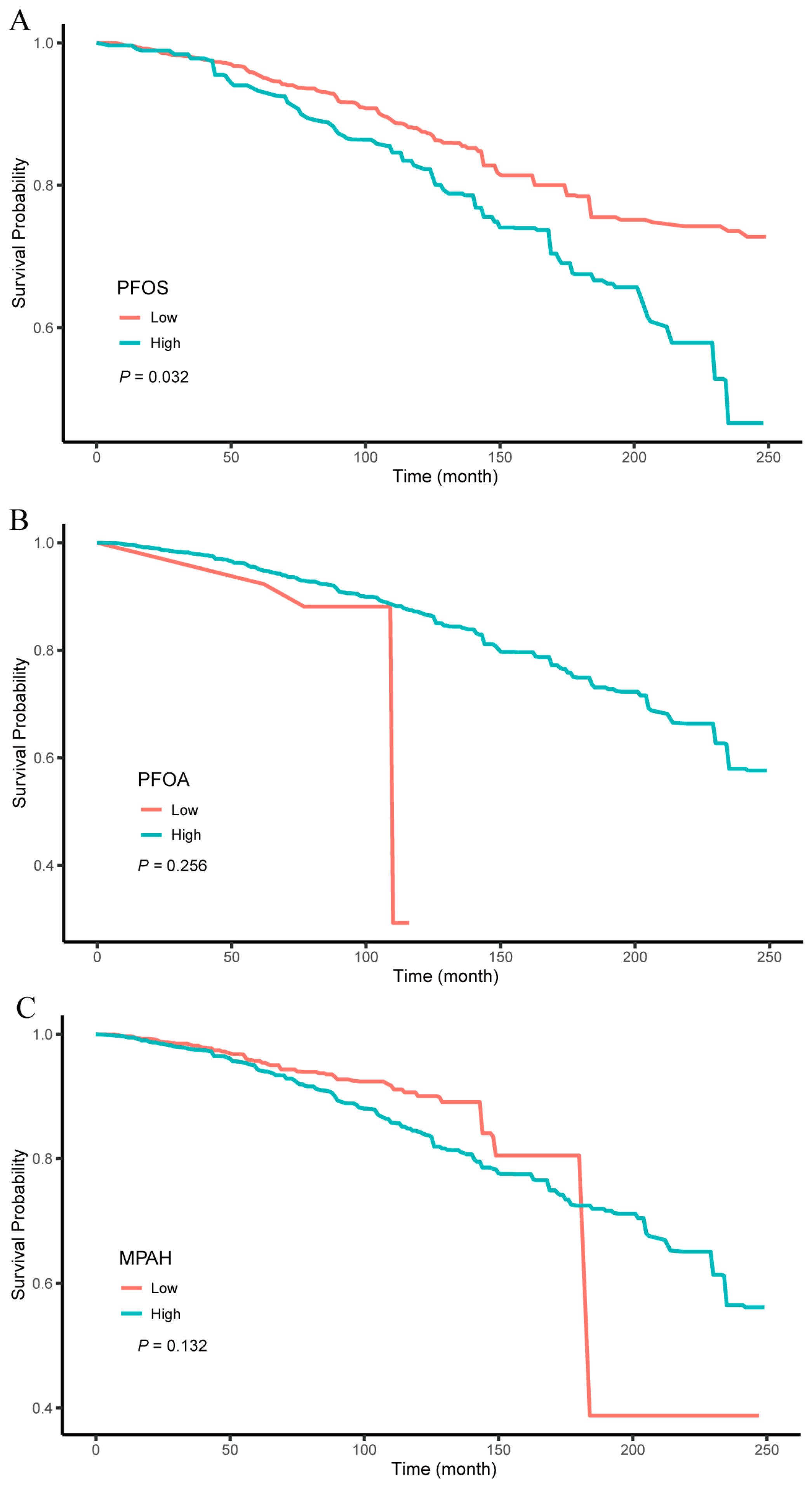
3.4. Investigating the Link Between Three PFAS Compounds and All-Cause Mortality in Diabetic Individuals
3.5. Results of Toxicogenomic Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Strain, W.D.; Paldanius, P.M. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc. Diabetol. 2018, 17, 57. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Ali, M.K.; Pearson-Stuttard, J.; Selvin, E.; Gregg, E.W. Interpreting global trends in type 2 diabetes complications and mortality. Diabetologia 2022, 65, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Zhu, Z.; Wan, R.; Xu, J. Exposure to per- and polyfluoroalkyl substance and metabolic syndrome: A nationally representative cross-sectional study from NHANES, 2003–2018. Environ. Pollut. 2024, 346, 123615. [Google Scholar] [CrossRef] [PubMed]
- Schymanski, E.L.; Zhang, J.; Thiessen, P.A.; Chirsir, P.; Kondic, T.; Bolton, E.E. Per- and Polyfluoroalkyl Substances (PFAS) in PubChem: 7 Million and Growing. Environ. Sci. Technol. 2023, 57, 16918–16928. [Google Scholar] [CrossRef] [PubMed]
- Jian, J.M.; Chen, D.; Han, F.J.; Guo, Y.; Zeng, L.; Lu, X.; Wang, F. A short review on human exposure to and tissue distribution of per- and polyfluoroalkyl substances (PFASs). Sci. Total Environ. 2018, 636, 1058–1069. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Herrera, V.; Field, J.A.; Luna-Velasco, A.; Sierra-Alvarez, R. Microbial toxicity and biodegradability of perfluorooctane sulfonate (PFOS) and shorter chain perfluoroalkyl and polyfluoroalkyl substances (PFASs). Environ. Sci. Process Impacts 2016, 18, 1236–1246. [Google Scholar] [CrossRef]
- Sunderland, E.M.; Hu, X.C.; Dassuncao, C.; Tokranov, A.K.; Wagner, C.C.; Allen, J.G. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects. J. Expo. Sci. Environ. Epidemiol. 2019, 29, 131–147. [Google Scholar] [CrossRef]
- Domingo, J.L.; Nadal, M. Human exposure to per- and polyfluoroalkyl substances (PFAS) through drinking water: A review of the recent scientific literature. Environ. Res. 2019, 177, 108648. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, L.; Barouki, R.; Blanc, E.; Coumoul, X.; Andreau, K. Per- and polyfluoroalkyl substances as persistent pollutants with metabolic and endocrine-disrupting impacts. Trends Endocrinol. Metab. 2024. online first. [Google Scholar] [CrossRef] [PubMed]
- Margolis, R.; Sant, K.E. Associations between Exposures to Perfluoroalkyl Substances and Diabetes, Hyperglycemia, or Insulin Resistance: A Scoping Review. J. Xenobiot. 2021, 11, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Donat-Vargas, C.; Bergdahl, I.A.; Tornevi, A.; Wennberg, M.; Sommar, J.; Kiviranta, H.; Koponen, J.; Rolandsson, O.; Akesson, A. Perfluoroalkyl substances and risk of type II diabetes: A prospective nested case-control study. Environ. Int. 2019, 123, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.C.; Goodrich, J.A.; Walker, D.I.; Liao, J.; Costello, E.; Alderete, T.L.; Valvi, D.; Hampson, H.; Li, S.; Baumert, B.O.; et al. Exposure to per- and polyfluoroalkyl substances and high-throughput proteomics in Hispanic youth. Environ. Int. 2024, 186, 108601. [Google Scholar] [CrossRef]
- Roth, K.; Yang, Z.; Agarwal, M.; Liu, W.; Peng, Z.; Long, Z.; Birbeck, J.; Westrick, J.; Liu, W.; Petriello, M.C. Exposure to a mixture of legacy, alternative, and replacement per- and polyfluoroalkyl substances (PFAS) results in sex-dependent modulation of cholesterol metabolism and liver injury. Environ. Int. 2021, 157, 106843. [Google Scholar] [CrossRef]
- Goodrich, J.A.; Walker, D.I.; He, J.; Lin, X.; Baumert, B.O.; Hu, X.; Alderete, T.L.; Chen, Z.; Valvi, D.; Fuentes, Z.C.; et al. Metabolic Signatures of Youth Exposure to Mixtures of Per- and Polyfluoroalkyl Substances: A Multi-Cohort Study. Environ. Health Perspect. 2023, 131, 27005. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Chen, L.; Hu, X.; Tan, T.; Yang, J.; Bao, W.; Rong, S. Association of Serum Uric Acid With All-Cause and Cardiovascular Mortality in Diabetes. Diabetes Care 2023, 46, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Bulka, C.M.; Avula, V.; Fry, R.C. Associations of exposure to perfluoroalkyl substances individually and in mixtures with persistent infections: Recent findings from NHANES 1999–2016. Environ. Pollut. 2021, 275, 116619. [Google Scholar] [CrossRef]
- Lin, P.D.; Cardenas, A.; Hauser, R.; Gold, D.R.; Kleinman, K.P.; Hivert, M.F.; Calafat, A.M.; Webster, T.F.; Horton, E.S.; Oken, E. Temporal trends of concentrations of per- and polyfluoroalkyl substances among adults with overweight and obesity in the United States: Results from the Diabetes Prevention Program and NHANES. Environ. Int. 2021, 157, 106789. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Lerman, J.L.; Krebs-Smith, S.M.; Kirkpatrick, S.I.; Pannucci, T.E.; Wilson, M.M.; Subar, A.F.; Kahle, L.L.; Tooze, J.A. Evaluation of the Healthy Eating Index-2015. J. Acad. Nutr. Diet. 2018, 118, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef]
- Davis, A.P.; Wiegers, T.C.; Johnson, R.J.; Sciaky, D.; Wiegers, J.; Mattingly, C.J. Comparative Toxicogenomics Database (CTD): Update 2023. Nucleic Acids Res. 2023, 51, D1257–D1262. [Google Scholar] [CrossRef]
- Fishilevich, S.; Zimmerman, S.; Kohn, A.; Iny Stein, T.; Olender, T.; Kolker, E.; Safran, M.; Lancet, D. Genic insights from integrated human proteomics in GeneCards. Database 2016, 2016, baw030. [Google Scholar] [CrossRef] [PubMed]
- Alsen, M.; Leung, A.M.; van Gerwen, M. Per- and Polyfluoroalkyl Substances (PFAS) in Community Water Systems (CWS) and the Risk of Thyroid Cancer: An Ecological Study. Toxics 2023, 11, 786. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.L.Y.; Co, V.A.; El-Nezami, H. Endocrine disrupting chemicals and breast cancer: A systematic review of epidemiological studies. Crit. Rev. Food Sci. Nutr. 2022, 62, 6549–6576. [Google Scholar] [CrossRef] [PubMed]
- Zota, A.R.; Geller, R.J.; Romano, L.E.; Coleman-Phox, K.; Adler, N.E.; Parry, E.; Wang, M.; Park, J.S.; Elmi, A.F.; Laraia, B.A.; et al. Association between persistent endocrine-disrupting chemicals (PBDEs, OH-PBDEs, PCBs, and PFASs) and biomarkers of inflammation and cellular aging during pregnancy and postpartum. Environ. Int. 2018, 115, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Wang, M.; Xu, X.; Li, T. Exposure to Per- and Polyfluoroalkyl Substances and Mortality in U.S. Adults: A Population-Based Cohort Study. Environ. Health Perspect. 2022, 130, 67007. [Google Scholar] [CrossRef]
- Biggeri, A.; Stoppa, G.; Facciolo, L.; Fin, G.; Mancini, S.; Manno, V.; Minelli, G.; Zamagni, F.; Zamboni, M.; Catelan, D.; et al. All-cause, cardiovascular disease and cancer mortality in the population of a large Italian area contaminated by perfluoroalkyl and polyfluoroalkyl substances (1980–2018). Environ. Health 2024, 23, 42. [Google Scholar] [CrossRef]
- Yang, W.; Ling, X.; He, S.; Cui, H.; Yang, Z.; An, H.; Wang, L.; Zou, P.; Chen, Q.; Liu, J.; et al. PPARalpha/ACOX1 as a novel target for hepatic lipid metabolism disorders induced by per- and polyfluoroalkyl substances: An integrated approach. Environ. Int. 2023, 178, 108138. [Google Scholar] [CrossRef]
- Qi, Q.; Niture, S.; Gadi, S.; Arthur, E.; Moore, J.; Levine, K.E.; Kumar, D. Per- and polyfluoroalkyl substances activate UPR pathway, induce steatosis and fibrosis in liver cells. Environ. Toxicol. 2023, 38, 225–242. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, B.; Hu, Y.; Rood, J.; Liang, L.; Qi, L.; Bray, G.A.; DeJonge, L.; Coull, B.; Grandjean, P.; et al. Associations of Perfluoroalkyl substances with blood lipids and Apolipoproteins in lipoprotein subspecies: The POUNDS-lost study. Environ. Health 2020, 19, 5. [Google Scholar] [CrossRef] [PubMed]
- Haug, M.; Dunder, L.; Lind, P.M.; Lind, L.; Salihovic, S. Associations of perfluoroalkyl substances (PFAS) with lipid and lipoprotein profiles. J. Expo. Sci. Environ. Epidemiol. 2023, 33, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Lu, Y.; Xie, S.; Wang, T.; Jones, K.C.; Sweetman, A.J. Exploring the fate, transport and risk of Perfluorooctane Sulfonate (PFOS) in a coastal region of China using a multimedia model. Environ. Int. 2015, 85, 15–26. [Google Scholar] [CrossRef]
- Song, X.; Ye, T.; Jing, D.; Wei, K.; Ge, Y.; Bei, X.; Qi, Y.; Wang, H.; Li, J.; Zhang, Y. Association Between Exposure to Per- and Polyfluoroalkyl Substances and Levels of Lipid Profile Based on Human Studies. Rev. Environ. Health 2024. Available online: https://www.degruyter.com/document/doi/10.1515/reveh-2023-0146/html (accessed on 1 September 2024). [CrossRef] [PubMed]
- Omoike, O.E.; Pack, R.P.; Mamudu, H.M.; Liu, Y.; Strasser, S.; Zheng, S.; Okoro, J.; Wang, L. Association between per and polyfluoroalkyl substances and markers of inflammation and oxidative stress. Environ. Res. 2021, 196, 110361. [Google Scholar] [CrossRef]
- Tan, Y.; Taibl, K.R.; Dunlop, A.L.; Barr, D.B.; Panuwet, P.; Yakimavets, V.; Kannan, K.; Corwin, E.J.; Ryan, P.B.; Eatman, J.A.; et al. Association between a Mixture of Per- and Polyfluoroalkyl Substances (PFAS) and Inflammatory Biomarkers in the Atlanta African American Maternal-Child Cohort. Environ. Sci. Technol. 2023, 57, 13419–13428. [Google Scholar] [CrossRef] [PubMed]
- Dagar, M.; Kumari, P.; Mirza, A.M.W.; Singh, S.; Ain, N.U.; Munir, Z.; Javed, T.; Virk, M.F.I.; Javed, S.; Qizilbash, F.H.; et al. The Hidden Threat: Endocrine Disruptors and Their Impact on Insulin Resistance. Cureus 2023, 15, e47282. [Google Scholar] [CrossRef] [PubMed]
- Qazi, M.R.; Bogdanska, J.; Butenhoff, J.L.; Nelson, B.D.; DePierre, J.W.; Abedi-Valugerdi, M. High-dose, short-term exposure of mice to perfluorooctanesulfonate (PFOS) or perfluorooctanoate (PFOA) affects the number of circulating neutrophils differently, but enhances the inflammatory responses of macrophages to lipopolysaccharide (LPS) in a similar fashion. Toxicology 2009, 262, 207–214. [Google Scholar]
- Wang, L.Q.; Liu, T.; Yang, S.; Sun, L.; Zhao, Z.Y.; Li, L.Y.; She, Y.C.; Zheng, Y.Y.; Ye, X.Y.; Bao, Q.; et al. Perfluoroalkyl substance pollutants activate the innate immune system through the AIM2 inflammasome. Nat. Commun. 2021, 12, 2915. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N = 1256) | Alive (N = 1044) | Death (N = 212) | p-Value |
|---|---|---|---|---|
| Age, n (%) | <0.0001 | |||
| 18–59 | 621 (61.685) | 572 (65.930) | 49 (34.308) | |
| ≥60 | 635 (38.315) | 472 (34.070) | 163 (65.692) | |
| Sex, n (%) | 0.14 | |||
| Male | 627 (49.053) | 507 (48.039) | 120 (55.598) | |
| Female | 629 (50.947) | 537 (51.961) | 92 (44.402) | |
| Race/Ethnicity, n (%) | 0.016 | |||
| White | 386 (57.654) | 285 (56.043) | 101 (68.044) | |
| Black | 324 (15.475) | 274 (15.495) | 50 (15.346) | |
| Other | 546 (26.872) | 485 (28.463) | 61 (16.610) | |
| PIR, n (%) | <0.0001 | |||
| <1.3 | 421 (24.454) | 344 (23.788) | 77 (28.748) | |
| 1.3–3.5 | 517 (40.072) | 412 (37.784) | 105 (54.830) | |
| >3.5 | 318 (35.473) | 288 (38.428) | 30 (16.422) | |
| Educational attainment, n (%) | 0.021 | |||
| Below high school | 235 (9.638) | 177 (8.699) | 58 (15.694) | |
| High school | 507 (40.107) | 415 (39.418) | 92 (44.553) | |
| Above high school | 514 (50.255) | 452 (51.884) | 62 (39.753) | |
| Smoking status, n (%) | 0.02 | |||
| Never | 677 (55.467) | 586 (57.263) | 91 (43.886) | |
| Former | 365 (27.707) | 286 (26.853) | 79 (33.212) | |
| Now | 214 (16.826) | 172 (15.884) | 42 (22.901) | |
| Alcohol consumption, n (%) | <0.0001 | |||
| Never | 225 (15.002) | 182 (14.296) | 43 (19.559) | |
| Moderate | 151 (14.672) | 142 (16.275) | 9 (4.335) | |
| Mild | 393 (37.568) | 347 (39.372) | 46 (25.938) | |
| Former | 302 (19.342) | 211 (16.207) | 91 (39.560) | |
| Heavy | 185 (13.416) | 162 (13.851) | 23 (10.608) | |
| BMI, n (%) | 0.02 | |||
| <18 | 169 (11.641) | 124 (10.641) | 45 (18.094) | |
| 18–25 | 363 (25.341) | 301 (24.985) | 62 (27.635) | |
| >25 | 724 (63.018) | 619 (64.374) | 105 (54.271) | |
| Hypertension, n (%) | 0.049 | |||
| No | 526 (41.110) | 448 (42.290) | 78 (33.503) | |
| Yes | 730 (58.890) | 596 (57.710) | 134 (66.497) | |
| Total cholesterol, (mean ± SD), mg/dl | 194.183 ± 1.782 | 193.331 ± 1.801 | 199.675 ± 5.020 | 0.215 |
| HEI-2015 score, (mean ± SD) | 50.129 ± 0.584 | 50.251 ± 0.633 | 49.341 ± 1.131 | 0.464 |
| Taking anti-diabetic medication | 0.55 | |||
| No | 552 (42.863) | 462 (43.243) | 90 (40.414) | |
| Yes | 704 (57.137) | 582 (56.757) | 122 (59.586) | |
| PFOS, median (IQR), ng/mL | 11.01 (5.40, 20.53) | 10.10 (5.00, 17.93) | 17.95 (10.10, 32.23) | <0.0001 |
| PFOA, median (IQR), ng/mL | 2.60 (1.57, 4.20) | 2.40 (1.47, 4.00) | 3.30 (2.3, 5.05) | 0.008 |
| PFNA, median (IQR), ng/mL | 0.91 (0.50, 1.40) | 0.90 (0.50, 1.40) | 0.91 (0.57, 1.48) | 0.53 |
| PFHS, median (IQR), ng/mL | 1.59 (0.90, 2.60) | 1.50 (0.80, 2.50) | 1.90 (1.19, 3.00) | 0.175 |
| PFDE, median (IQR), ng/mL | 0.20 (0.14, 0.40) | 0.19 (0.14, 0.40) | 0.20 (0.19, 0.33) | 0.472 |
| PFUA, median (IQR), ng/mL | 0.14 (0.07, 0.20) | 0.14 (0.07, 0.20) | 0.18 (0.14, 0.20) | 0.121 |
| MPAH, median (IQR), ng/mL | 0.20 (0.07, 0.40) | 0.20 (0.07, 0.37) | 0.37 (0.20, 0.63) | 0.003 |
| Crude Model | Model 1 | Model 2 | Model 3 | |||||
|---|---|---|---|---|---|---|---|---|
| PFAS | OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value |
| PFOS | 1.03 (1.02, 1.04) | <0.0001 | 1.03 (1.01, 1.04) | <0.001 | 1.03 (1.01, 1.04) | <0.001 | 1.03 (1.01, 1.04) | <0.001 |
| PFOA | 1.09 (1.03, 1.14) | 0.002 | 1.07 (1.00, 1.15) | 0.04 | 1.10 (1.02, 1.18) | 0.01 | 1.11 (1.03, 1.19) | 0.01 |
| PFNA | 1.05 (0.90, 1.23) | 0.52 | 1.03 (0.85, 1.25) | 0.75 | 1.07 (0.90, 1.27) | 0.45 | 1.07 (0.90, 1.26) | 0.44 |
| PFHS | 1.05 (0.98, 1.12) | 0.16 | 1.00 (0.93, 1.09) | 0.92 | 1.00 (0.93, 1.08) | 0.97 | 1.00 (0.93, 1.08) | 0.96 |
| PFDE | 1.26 (0.72, 2.20) | 0.41 | 1.24 (0.63, 2.42) | 0.53 | 1.33 (0.70, 2.50) | 0.38 | 1.23 (0.65, 2.33) | 0.52 |
| PFUA | 1.60 (0.89, 2.85) | 0.11 | 1.56 (0.83, 2.94) | 0.17 | 1.82 (0.98, 3.38) | 0.06 | 1.77 (0.96, 3.24) | 0.07 |
| MPAH | 2.51 (1.86, 3.39) | <0.0001 | 2.09 (1.55, 2.83) | <0.0001 | 2.13 (1.50, 3.02) | <0.0001 | 1.97 (1.39, 2.81) | <0.001 |
| Character | Se | p-Value | HR (95% CI) * |
|---|---|---|---|
| PFOS | |||
| Low level | ref | ref | ref |
| High level | 0.172 | 0.025 | 1.554 (1.056, 2.287) |
| Age | |||
| 18–59 | ref | ref | ref |
| ≥60 | 0.19 | <0.0001 | 3.639 (2.442, 5.424) |
| Sex | |||
| Male | ref | ref | ref |
| Female | 0.171 | 0.051 | 0.672 (0.450, 1.001) |
| Race/Ethnicity | |||
| White | ref | ref | ref |
| Black | 0.223 | 0.225 | 0.795 (0.548, 1.152) |
| Other | 0.239 | 0.022 | 0.530 (0.308, 0.912) |
| Education | |||
| Below high school | ref | ref | ref |
| High school | 0.25 | 0.227 | 0.715 (0.415, 1.232) |
| Above high school | 0.266 | 0.78 | 1.085 (0.614, 1.916) |
| PIR | |||
| <1.3 | ref | ref | ref |
| 1.3–3.5 | 0.19 | 0.935 | 1.016 (0.697, 1.479) |
| >3.5 | 0.268 | 0.011 | 0.467 (0.259, 0.842) |
| BMI | |||
| <18 | ref | ref | ref |
| 18–25 | 0.242 | 0.005 | 0.512 (0.322, 0.817) |
| >25 | 0.23 | 0.02 | 0.559 (0.342, 0.914) |
| Smoking status | |||
| never | ref | ref | ref |
| former | 0.199 | 0.613 | 1.116 (0.728, 1.711) |
| now | 0.228 | 0.049 | 1.688 (1.003, 2.840) |
| Alcohol consumption | |||
| never | ref | ref | ref |
| moderate | 0.426 | 0.005 | 0.255 (0.098, 0.663) |
| mild | 0.254 | 0.078 | 0.576 (0.312, 1.064) |
| former | 0.243 | 0.937 | 0.979 (0.576, 1.665) |
| heavy | 0.335 | 0.223 | 0.619 (0.286, 1.339) |
| HEI-2015 score | 0.006 | 0.014 | 0.984 (0.972, 0.997) |
| Hypertension | |||
| No | ref | ref | ref |
| Yes | 0.179 | 0.251 | 1.277 (0.841, 1.941) |
| Total cholesterol | 0.002 | 0.56 | 1.001 (0.998, 1.004) |
| Taking anti-diabetic medication | |||
| No | ref | ref | ref |
| Yes | 0.166 | 0.267 | 1.200 (0.870, 1.656) |
| Chemical–Gene Interaction | AKT1 | BCL2 | CASP3 | IL6 | TNF | PPARG | SIRT1 | INS | NFKB1 | EGFR | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PFOS | mRNA expression | - | ↓↓↓↓ | ↑ | ↑ | ↓ | ↑↑↑↑↓ | ↓ | - | ↓ | - |
| Protein expression | - | ↓↓↓ | - | - | - | - | ↓ | ↑ | - | - | |
| Protein activity | - | - | ↑↑ | - | - | ↑↑ | - | - | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Z.; Chen, J.; Mei, X.; Yu, Y. Association Between Per- and Polyfluoroalkyl Substances and All-Cause Mortality in Diabetic Patients: Insights from a National Cohort Study and Toxicogenomic Analysis. Toxics 2025, 13, 168. https://doi.org/10.3390/toxics13030168
Wei Z, Chen J, Mei X, Yu Y. Association Between Per- and Polyfluoroalkyl Substances and All-Cause Mortality in Diabetic Patients: Insights from a National Cohort Study and Toxicogenomic Analysis. Toxics. 2025; 13(3):168. https://doi.org/10.3390/toxics13030168
Chicago/Turabian StyleWei, Zhengxiao, Jinyu Chen, Xue Mei, and Yi Yu. 2025. "Association Between Per- and Polyfluoroalkyl Substances and All-Cause Mortality in Diabetic Patients: Insights from a National Cohort Study and Toxicogenomic Analysis" Toxics 13, no. 3: 168. https://doi.org/10.3390/toxics13030168
APA StyleWei, Z., Chen, J., Mei, X., & Yu, Y. (2025). Association Between Per- and Polyfluoroalkyl Substances and All-Cause Mortality in Diabetic Patients: Insights from a National Cohort Study and Toxicogenomic Analysis. Toxics, 13(3), 168. https://doi.org/10.3390/toxics13030168