
A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners

Abstract
:
1. Introduction
2. Materials and Methods
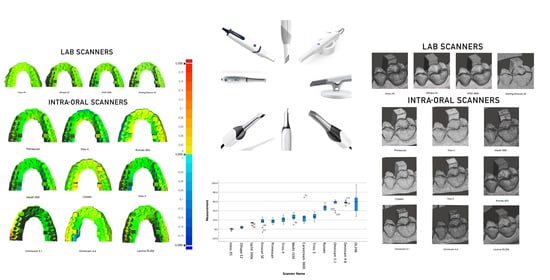
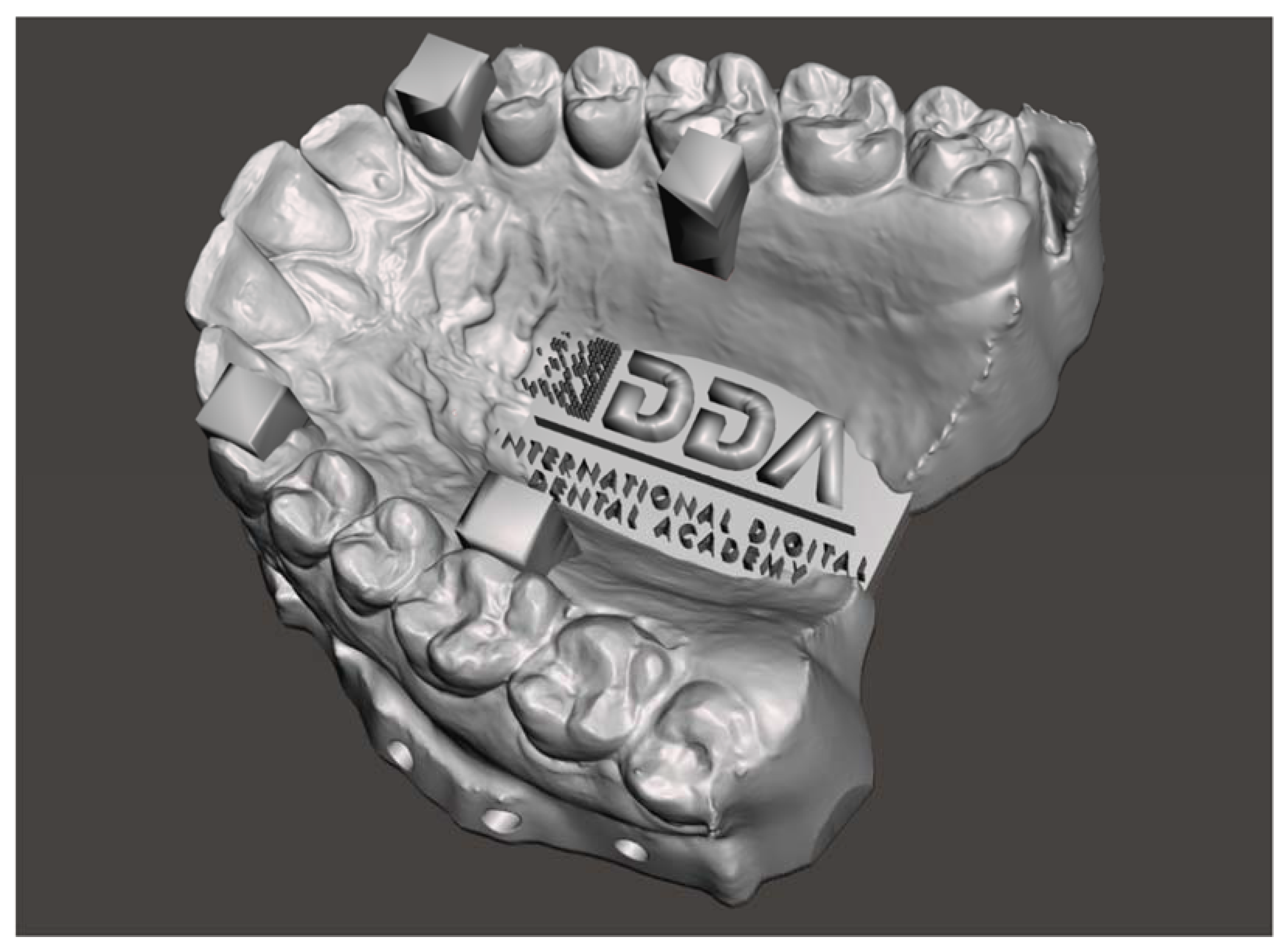
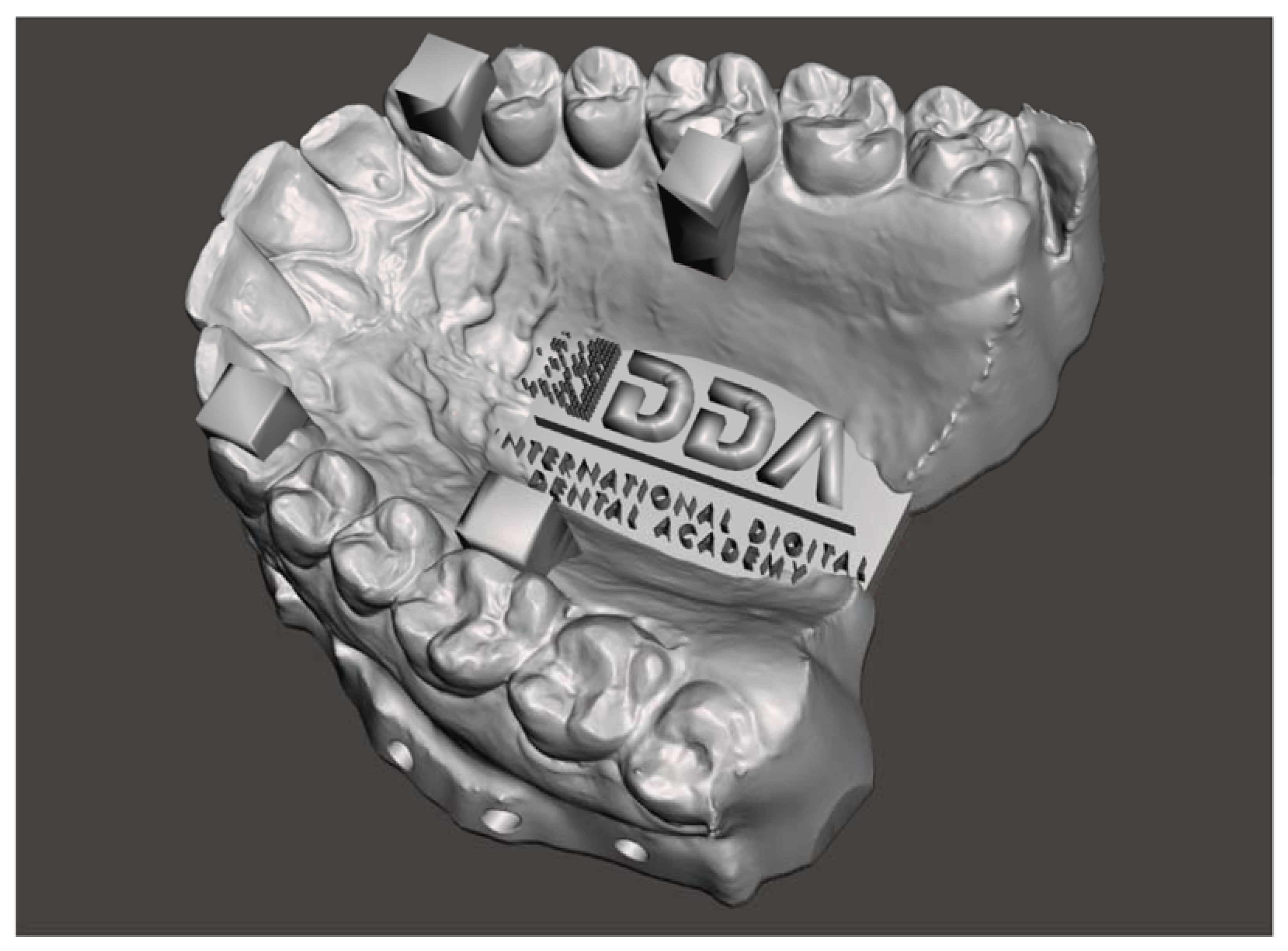
2.1. Study Model
- -
- a fully dentate arch;
- -
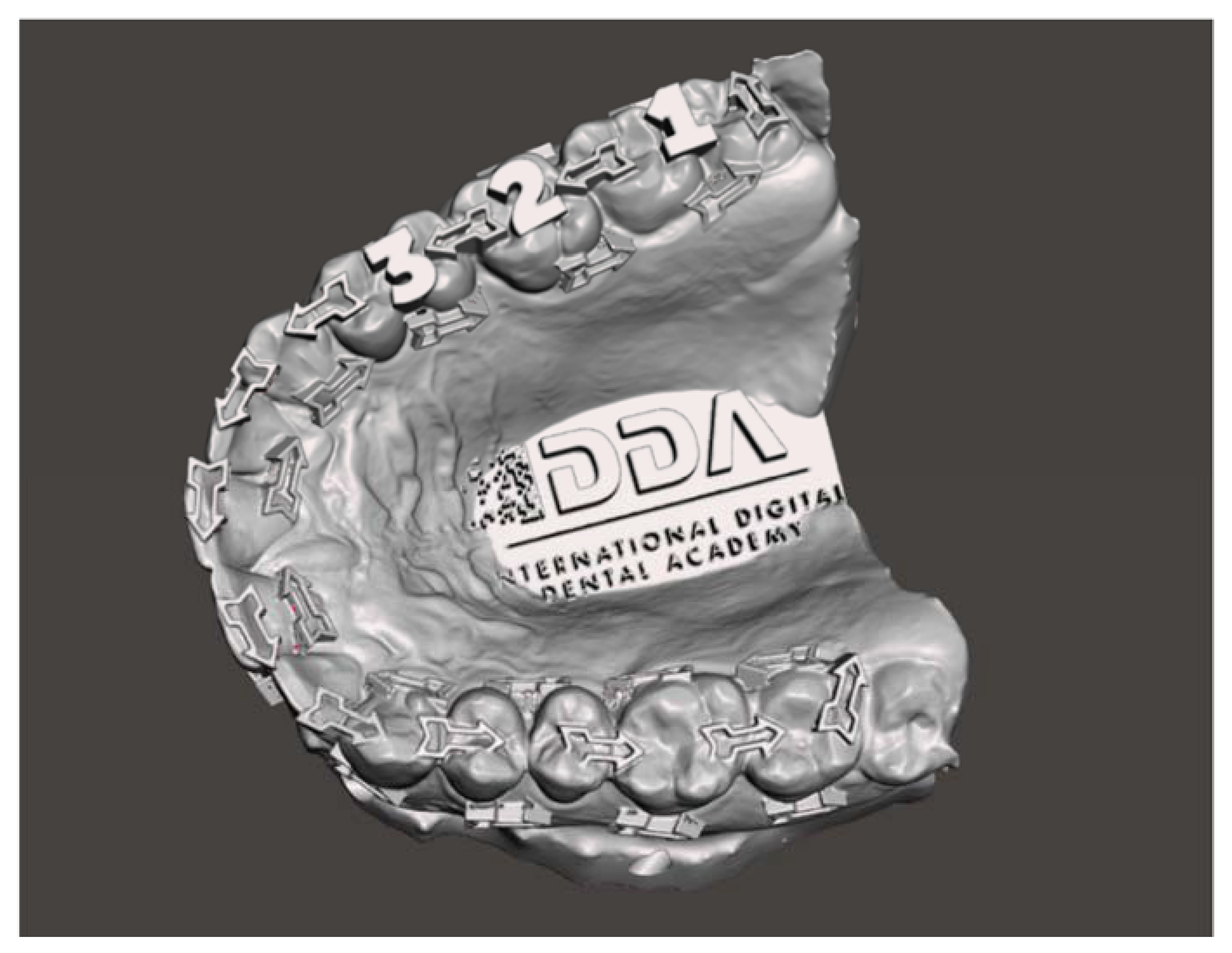
- four regular structures in the form of columns of known width and separation; and
- -
- a high degree of surface morphology.
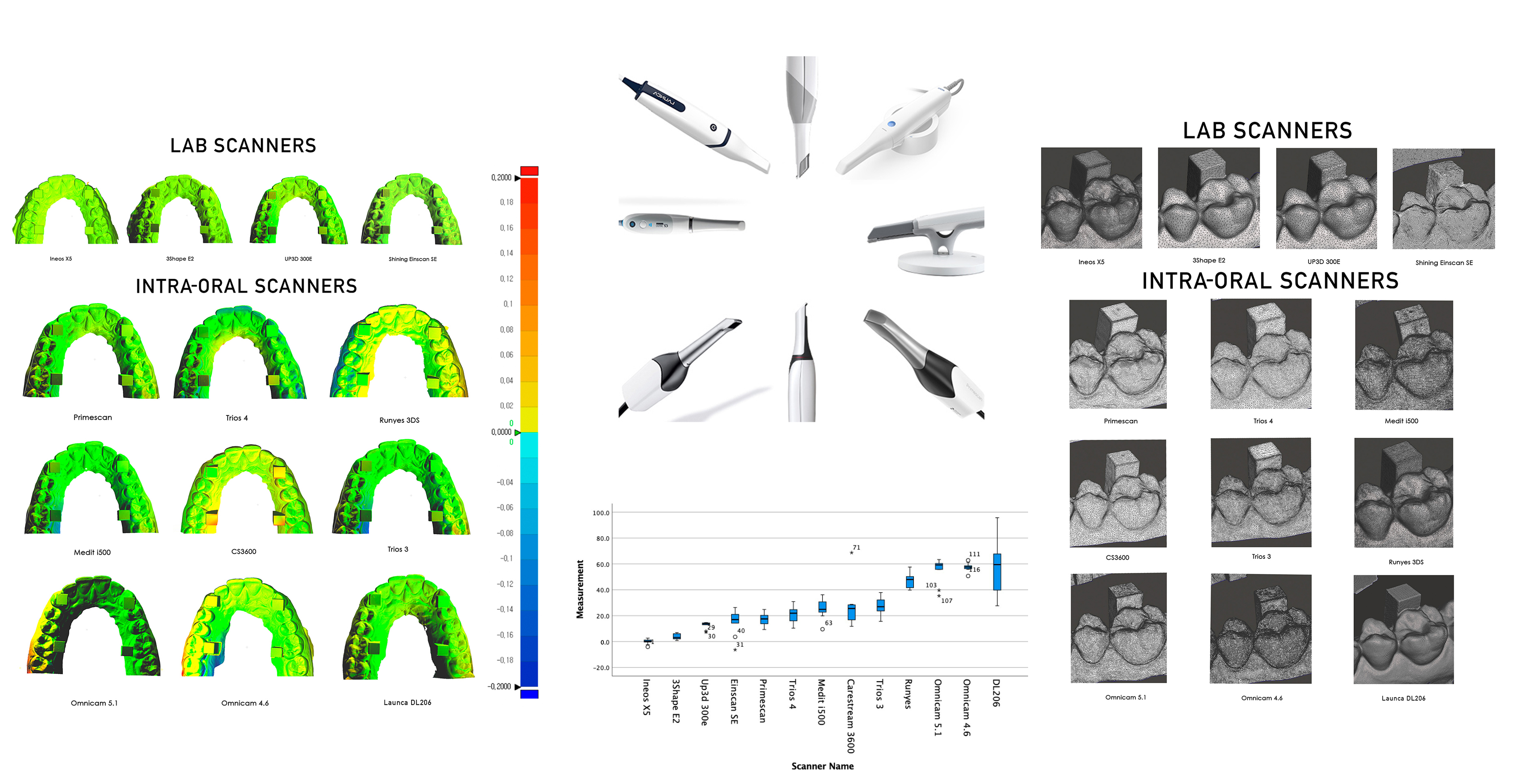
2.2. Scanners in the Study
2.3. Design of the Study
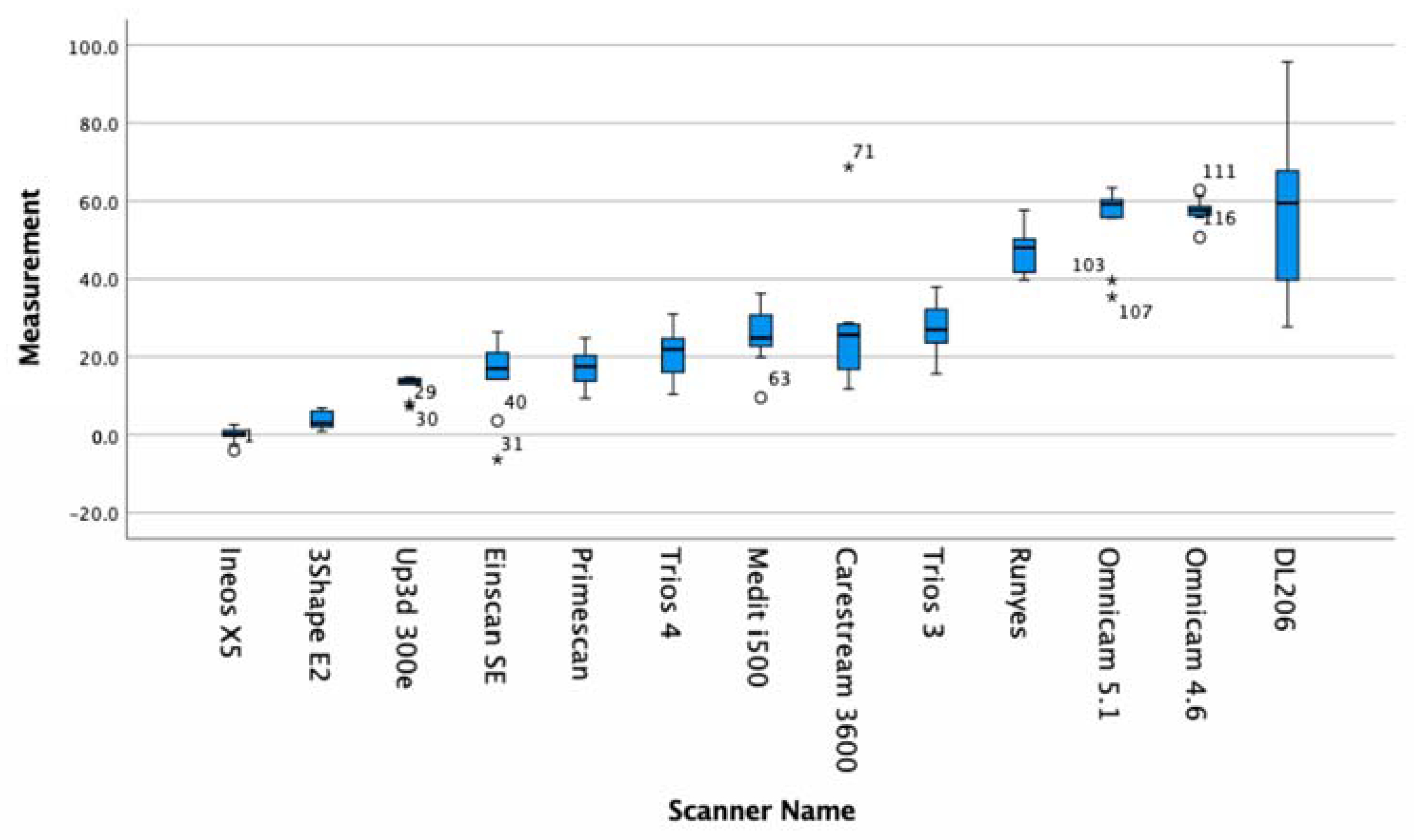
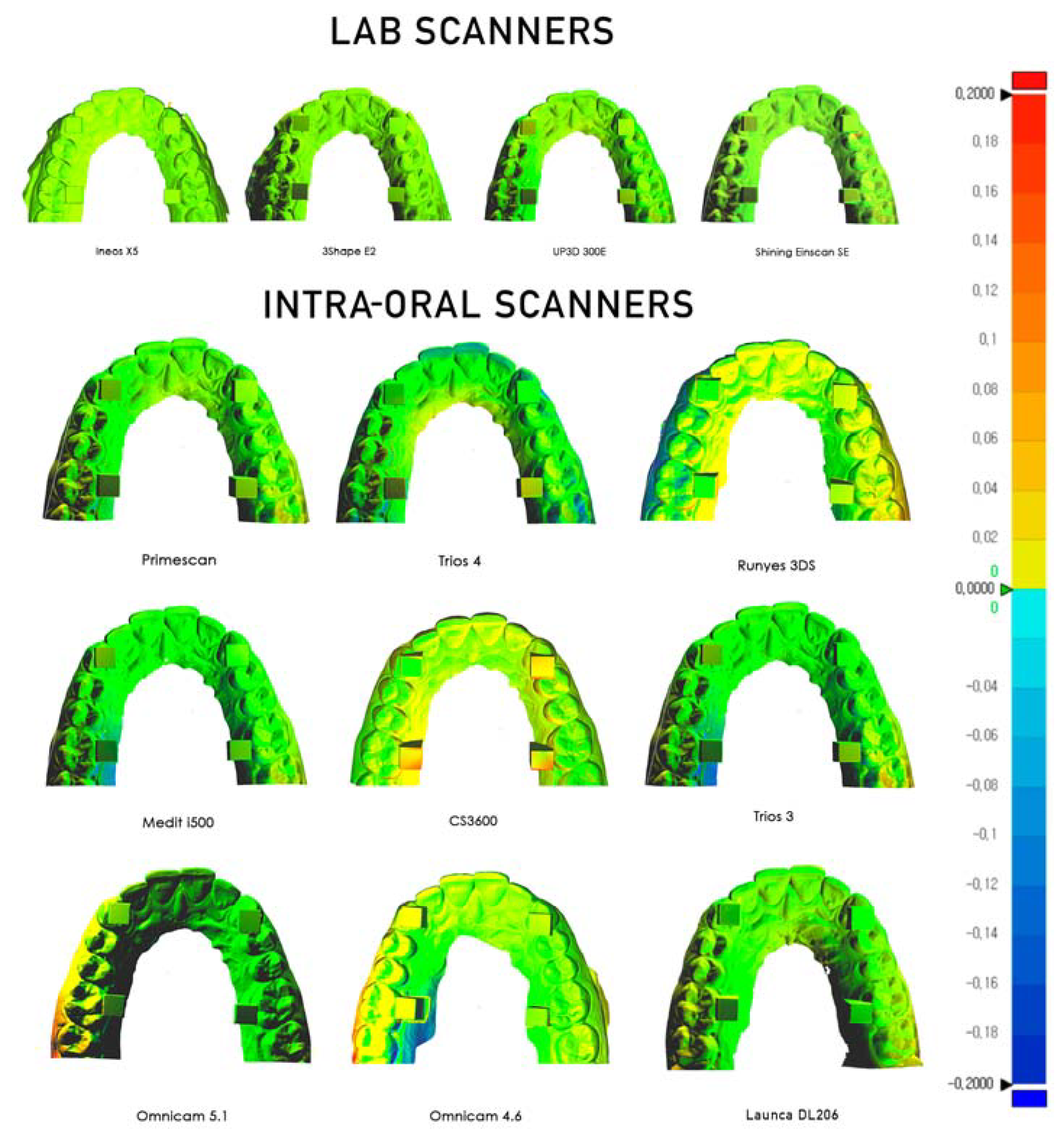
2.4. Evaluating Trueness
2.5. D Deviation
2.6. Evaluating Precision
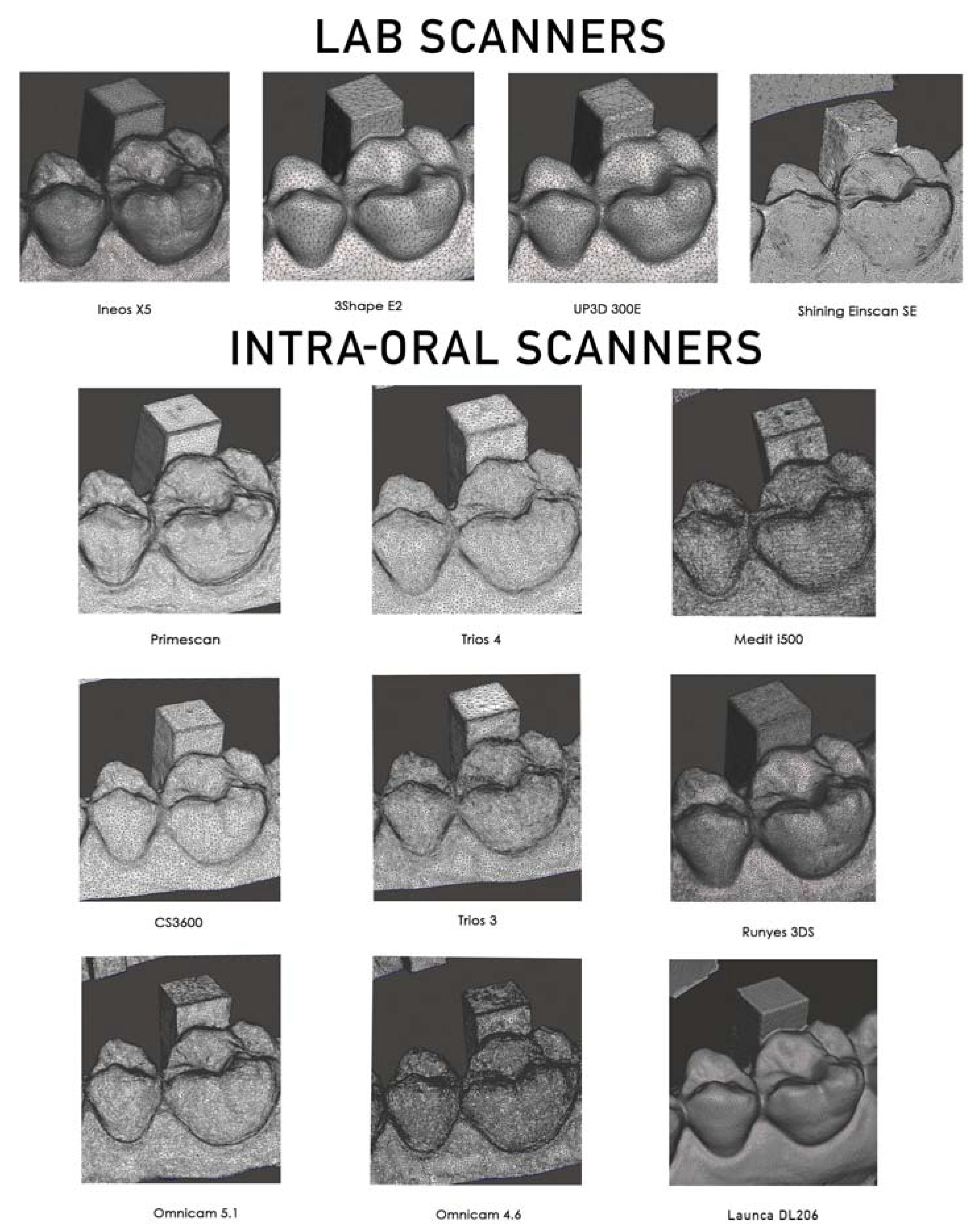
2.7. Surface Detail Observational Comparison
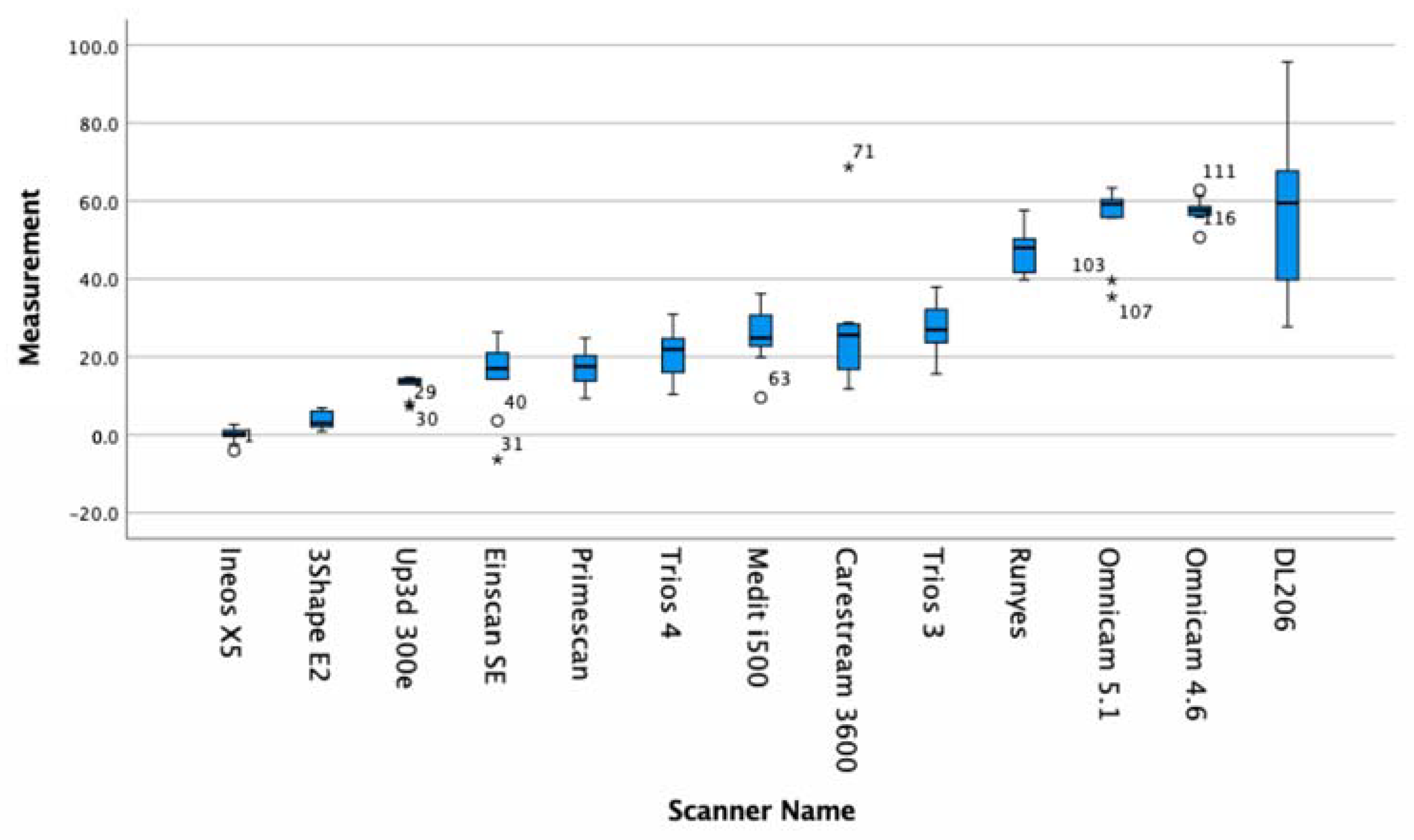
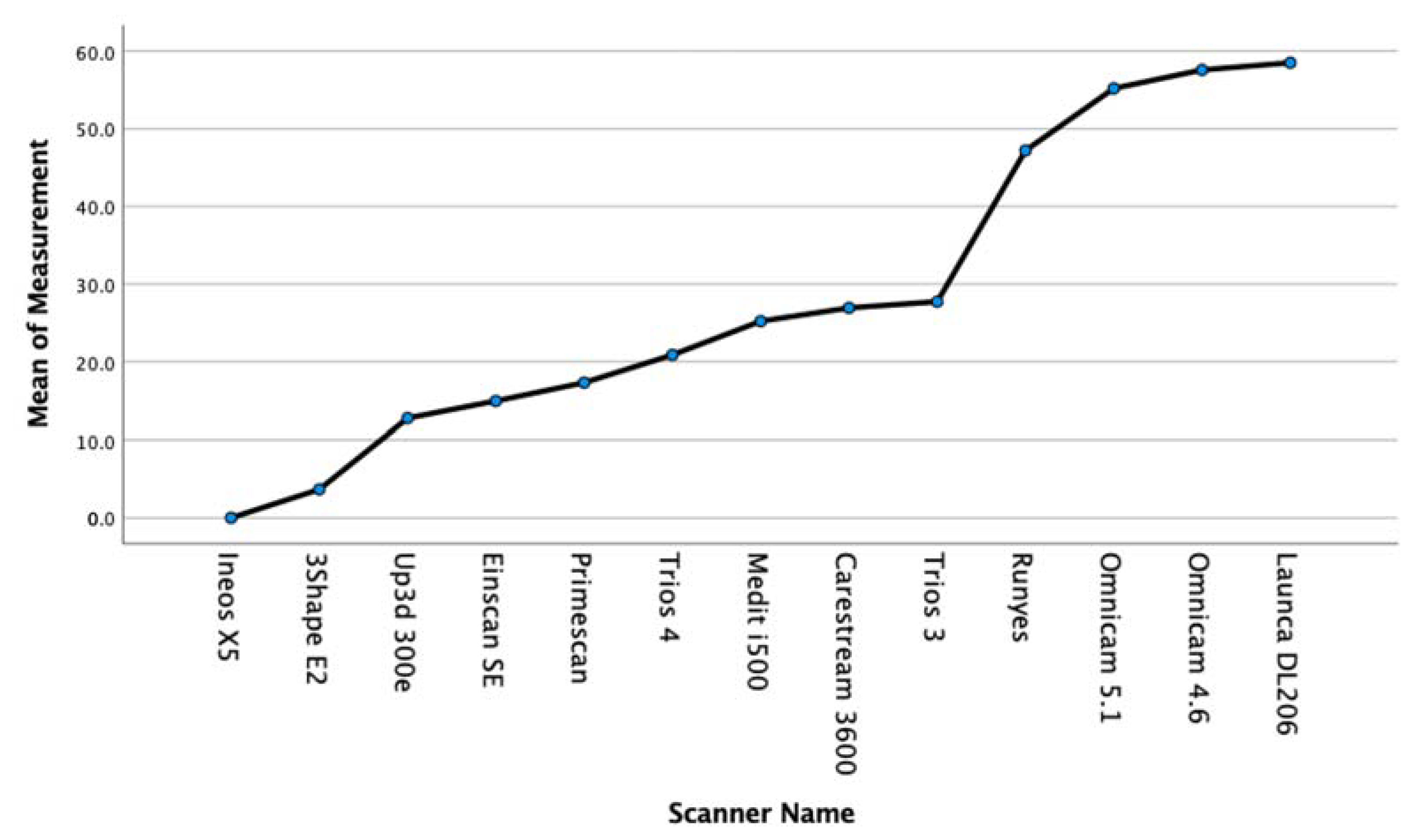
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mörmann, W.H. The evolution of the CEREC system. J. Am. Dent. Assoc. 2006, 137, 7S–13S. [Google Scholar] [CrossRef]
- Kim, R.J.Y.; Park, J.-M.; Shim, J.-S. Accuracy of 9 intraoral scanners for complete-arch image acquisition: A qualitative and quantitative evaluation. J. Prosthet. Dent. 2018, 120, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Yun, J.-H.; Han, J.-S.; Yeo, I.-S.L.; Yoon, H.-I. Repeatability of Intraoral Scanners for Complete Arch Scan of Partially Edentulous Dentitions: An In Vitro Study. J. Clin. Med. 2019, 8, 1187. [Google Scholar] [CrossRef] [Green Version]
- Chun, J.-H.; Tahk, J.H.; Chun, Y.-S.; Park, J.-M.; Kim, M. Analysis on the Accuracy of Intraoral Scanners: The Effects of Mandibular Anterior Interdental Space. Appl. Sci. 2017, 7, 719. [Google Scholar] [CrossRef]
- Braian, M.; Wennerberg, A. Trueness and precision of 5 intraoral scanners for scanning edentulous and dentate complete-arch mandibular casts: A comparative in vitro study. J. Prosthet. Dent. 2019, 122, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef]
- Jung, S.; Park, C.; Yang, H.-S.; Lim, H.-P.; Yun, K.-D.; Ying, Z.; Park, S.-W. Comparison of different impression techniques for edentulous jaws using three-dimensional analysis. J. Adv. Prosthodont. 2019, 11, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Fukazawa, S.; Odaira, C.; Kondo, H. Investigation of accuracy and reproducibility of abutment position by intraoral scanners. J. Prosthodont. Res. 2017, 61, 450–459. [Google Scholar] [CrossRef]
- Uhm, S.-H.; Kim, J.-H.; Jiang, H.B.; Woo, C.-W.; Chang, M.; Kim, K.-N.; Bae, J.-M.; Oh, S. Evaluation of the accuracy and precision of four intraoral scanners with 70% reduced inlay and four-unit bridge models of international standard. Dent. Mater. J. 2017, 36, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Park, G.-H.; Son, K.; Lee, K.-B. Feasibility of using an intraoral scanner for a complete-arch digital scan. J. Prosthet. Dent. 2019, 121, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kang, H.C.; Lee, J.; Shin, J.; Shin, Y.G. An enhanced method for reg- istration of dental surfaces partially scanned by a 3D dental laser scanning. Comput. Methods Programs Biomed. 2015, 118, 11–22. [Google Scholar] [CrossRef]
- Mao, Z.; Park, K.; Lee, K.; Li, X. Robust surface reconstruction of teeth from raw pointsets. Int. J. Numer. Methods Biomed. Eng. 2014, 30, 382–396. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, R.G.; Persson, A.S. Scanning accuracy and precision in 4 intraoral scanners: An in vitro comparison based on 3-dimensional analysis. J. Prosthet. Dent. 2014, 112, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; McDonagh, S. Simultaneous Registration of Multi-View Range Images with Adaptive Kernel Density Estimation. 2013. Available online: https://www.research.ed.ac.uk/en/publications/simultaneous-registration-of-multi-view-range-images-with-adaptiv (accessed on 3 February 2020).
- Zimmermann, M.; Mehl, A.; Mörmann, W.H.; Reich, S. Intraoral scanning systems—A current overview. Int. J. Comput. Dent. 2015, 18, 101–129. [Google Scholar]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.-C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 1–9. [Google Scholar] [CrossRef]
- International Organization for Standardization. Accuracy (Trueness and Precision) of Measurement Methods and Results e Part 1: General Principles and Definitions (ISO 5725e1:1994); Beuth Verlag GmbH: Berlin, Germany, 1997. [Google Scholar]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef] [Green Version]
- International Digital Dental Academy. Available online: www.idda.org (accessed on 2 December 2019).
- Ineos X5 Lab Scanner Information. Available online: https://www.dentsplysirona.com/en/explore/lab/cad-cam-equipment-dental-lab/scan.html (accessed on 14 January 2020).
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.H.; Son, K.; Lee, K.B. Accuracy of Five Intraoral Scanners and Two Laboratory Scanners for a Complete Arch: A Com-parative In Vitro Study. Appl. Sci. 2020, 10, 74. [Google Scholar] [CrossRef] [Green Version]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [Green Version]
- Meshlab. Available online: www.meshlab.net (accessed on 3 February 2020).
- SPSS 26. Available online: https://developer.ibm.com/predictiveanalytics/2019/04/09/whats-new-in-spss-statistics-26/ (accessed on 16 June 2020).
- Menini, M.; Setti, P.; Pera, F.; Pera, P.; Pesce, P. Accuracy of multi-unit implant impression: Traditional techniques versus a digital procedure. Clin. Oral Investig. 2018, 22, 1253–1262. [Google Scholar] [CrossRef]
- Sakornwimon, N.; Leevailoj, C. Clinical marginal fit of zirconia crowns and patients’ preferences for impression techniques using intraoral digital scanner versus polyvinyl siloxane material. J. Prosthet. Dent. 2017, 118, 386–391. [Google Scholar] [CrossRef]
- Rech-Ortega, C.; Fernández-Estevan, L.; Solá-Ruíz, M.F.; Agustín-Panadero, R.; Labaig-Rueda, C. Comparative in vitro study of the accuracy of impression techniques for dental implants: Direct technique with an elastomeric impression material versus in-traoral scanner. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e89. [Google Scholar] [CrossRef]
- Amin, S.; Weber, H.P.; Finkelman, M.; El Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impres-sions: A comparative study. Clin. Oral Implant. Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Emmanouilidi, A.; Stampf, S.; Strub, J.R.; Att, W. Accuracy of full-arch scans using intraoral scanners. Clin. Oral Investig. 2014, 18, 1687–1694. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Influence of scanning strategies on the accuracy of digital intraoral scanning systems. Int. J. Comput. Dent. 2013, 16, 11–21. [Google Scholar] [CrossRef]
- Lim, J.H.; Park, J.M.; Kim, M.; Heo, S.J.; Myung, J.Y. Comparison of digital intraoral scanner reproducibility and image trueness con-sidering repetitive experience. J. Prosthet. Dent. 2018, 119, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.A.; Simon, B.; Tóth, Z.; Vág, J. Evaluating the efficiency of the Dental Teacher system as a digital preclinical teaching tool. Eur. J. Dent. Educ. 2018, 22, e619–e623. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Weise, T.; Wismer, T.; Leibe, B.; Van Gool, L. Online loop closure for real-time interactive 3D scanning. Comput. Vis. Image Underst. 2011, 115, 635–648. [Google Scholar] [CrossRef] [Green Version]
- Arold, O.; Yang, Z.; Ettl, S.; Häusler, G. A new registration method to robustly align a series of sparse 3D data. DGaO Proc. 2009, 110, 20. [Google Scholar]
- Rehmann, P.; Sichwardt, V.; Wöstmann, B. Intraoral Scanning Systems: Need for Maintenance. Int. J. Prosthodont. 2017, 30, 27–29. [Google Scholar] [CrossRef] [Green Version]
- Andriessen, F.S.; Rijkens, D.R.; van der Meer, W.J.; Wismeijer, D.W. Applicability and accuracy of an intraoral scanner for scanning multiple implants in edentulous mandibles: A pilot study. J. Prosthet. Dent. 2014, 111, 186–194. [Google Scholar] [CrossRef]
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and Precision of Four Intraoral Scanners in Oral Implantology: A Comparative in Vitro Study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef]
- Ng, J.; Ruse, D.; Wyatt, C. A comparison of the marginal fit of crowns fabricated with digital and conventional methods. J. Prosthet. Dent. 2014, 112, 555–560. [Google Scholar] [CrossRef]
- Nedelcu, R.; Olsson, P.; Nyström, I.; Rydén, J.; Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 2018, 69, 110–118. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Manufacturer | Technology | STL Export | PLY/OBJ Colour Export |
|---|---|---|---|---|
| Omnicam 4.6 | Dentsply Sirona, York, PA, USA | Structured light—Optical triangulation and confocal microscopy | YES | NO |
| Omnicam 5.1 | Dentsply Sirona, York, PA, USA | Structured light—Optical triangulation and confocal microscopy | YES | NO |
| Primescan | Dentsply Sirona, York, PA, USA | Structured light—Confocal microscopy with Smart Pixel sensor. | YES | NO |
| CS3600 | Carestream Dental, Atlanta, GA, USA | Structured LED light—Active Speed 3D Video™ | YES | YES |
| Trios 3 | 3-Shape, Copenhagen, Denmark | Structured light—Confocal microscopy and Ultrafast Optical Scanning™ | YES | YES |
| Trios 4 | 3-Shape, Copenhagen, Denmark | Structured light—Confocal microscopy and Ultrafast Optical Scanning™ | YES | YES |
| Runyes | Ningbo Runyes Medical Instrument Co., Shenzhen, China | Structured light—Active Speed 3D Video™ | YES | YES |
| Launca DL206 | Guangdong Launca Medical Device Technology Co., Ltd., Dongguan, China | Structured light—Active Speed 3D Video™ | YES | YES |
| I500 | Medit, Seongbuk-gu, Seoul, Korea | Structured light—Active Speed 3D Video™ | YES | YES |
| Einscan SE | Shining 3D, Hangzhou, Zhejiang, China | Optical Blue Structured Light | YES | NO |
| UP3D 300E | Shenzhen UP3D Tech Co., Ltd., Shenzhen, China | Optical Blue Structured Light | YES | NO |
| E2 | 3-Shape, Copenhagen, Denmark | Optical Blue Structured Light | YES | NO |
| Ineos X5 | Dentsply Sirona, York, PA, USA | Optical Blue Structured Light | YES | NO |
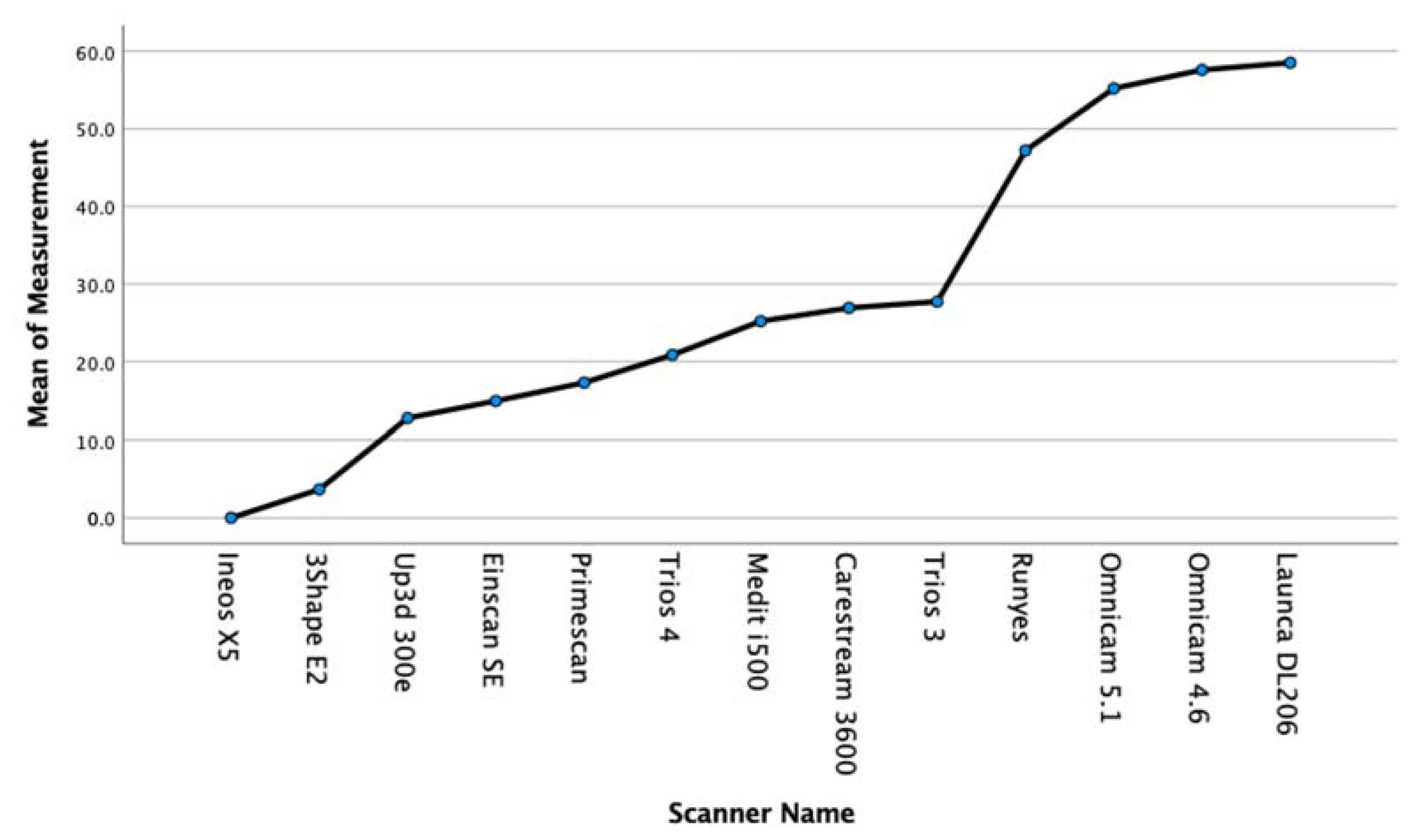
| Name | Mean (μm) | Std. Deviation (μm) | p Value |
|---|---|---|---|
| Ineos X5 | 0.0 | 1.9 | 1.000 |
| 3Shape E2 | 3.6 | 2.2 | 0.125 |
| UP3D 300E | 12.8 | 2.7 | 0.029 |
| Einscan SE | 14.9 | 9.5 | 0.004 |
| Primescan | 17.3 | 4.9 | <000.1 |
| Trios 4 | 20.8 | 6.2 | <000.1 |
| Medit i500 | 25.2 | 7.3 | <000.1 |
| CS3600 | 26.9 | 15.9 | <000.1 |
| Trios 3 | 27.7 | 6.8 | <000.1 |
| Runyes | 47.2 | 5.4 | <000.1 |
| Omnicam 5.1 | 55.1 | 9.5 | <000.1 |
| Omnicam 4.6 | 57.5 | 3.2 | <000.1 |
| Launca DL206 | 58.5 | 22.0 | <000.1 |
| Name | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Ineos X5 | 0.000 | ||||
| 3Shape E2 | 3.7 | 3.7 | |||
| UP3D 300E | 12.8 | 12.8 | 12.8 | ||
| Einscan SE | 15.0 | 15.0 | 15.0 | ||
| Primescan | 17.3 | 17.3 | 17.3 | ||
| Trios 4 | 20.9 | 20.9 | |||
| Medit i500 | 25.2 | 25.2 | |||
| CS3600 | 26.9 | 26.9 | |||
| Trios 3 | 27.7 | ||||
| Runyes | 47.2 | ||||
| Omnicam 5.1 | 55.2 | ||||
| Omnicam 4.6 | 57.6 | ||||
| Launca DL206 | 58.5 | ||||
| p Value (Sig) | 0.125 | 0.072 | 0.051 | 0.123 | 0.271 |
| Anova | |||||
|---|---|---|---|---|---|
| Measurement | Sum of Squares | Df | Mean Square | F | Sig. |
| Between Groups | 28,324.784639 | 8 | 3540.598080 | 29.235153 | 0.000 |
| Within Groups | 9809.712588 | 81 | 121.107563 | ||
| Total | 38,134.497226 | 89 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nulty, A.B. A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners. Dent. J. 2021, 9, 75. https://doi.org/10.3390/dj9070075
Nulty AB. A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners. Dentistry Journal. 2021; 9(7):75. https://doi.org/10.3390/dj9070075
Chicago/Turabian StyleNulty, Adam B. 2021. "A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners" Dentistry Journal 9, no. 7: 75. https://doi.org/10.3390/dj9070075
APA StyleNulty, A. B. (2021). A Comparison of Full Arch Trueness and Precision of Nine Intra-Oral Digital Scanners and Four Lab Digital Scanners. Dentistry Journal, 9(7), 75. https://doi.org/10.3390/dj9070075