
The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
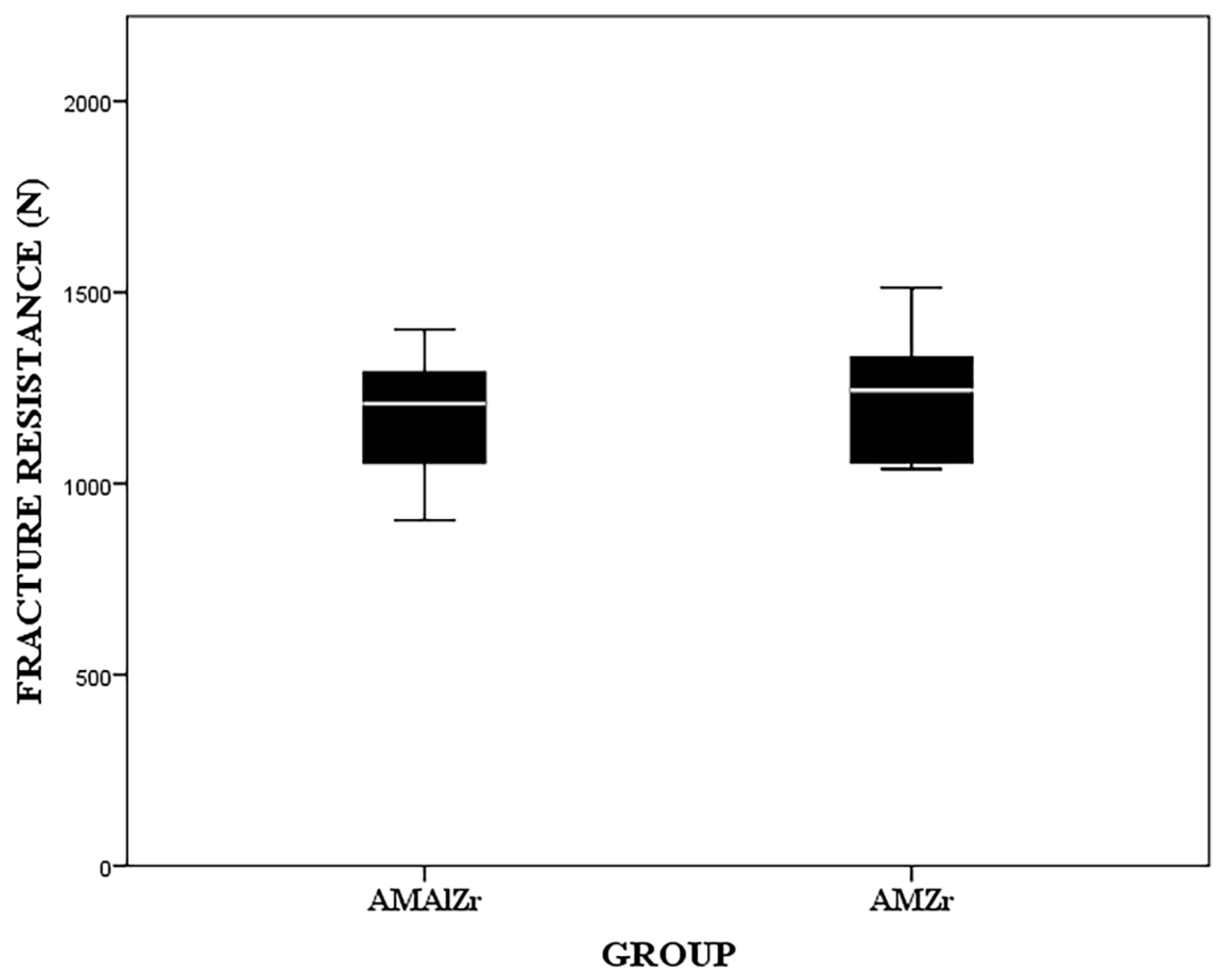
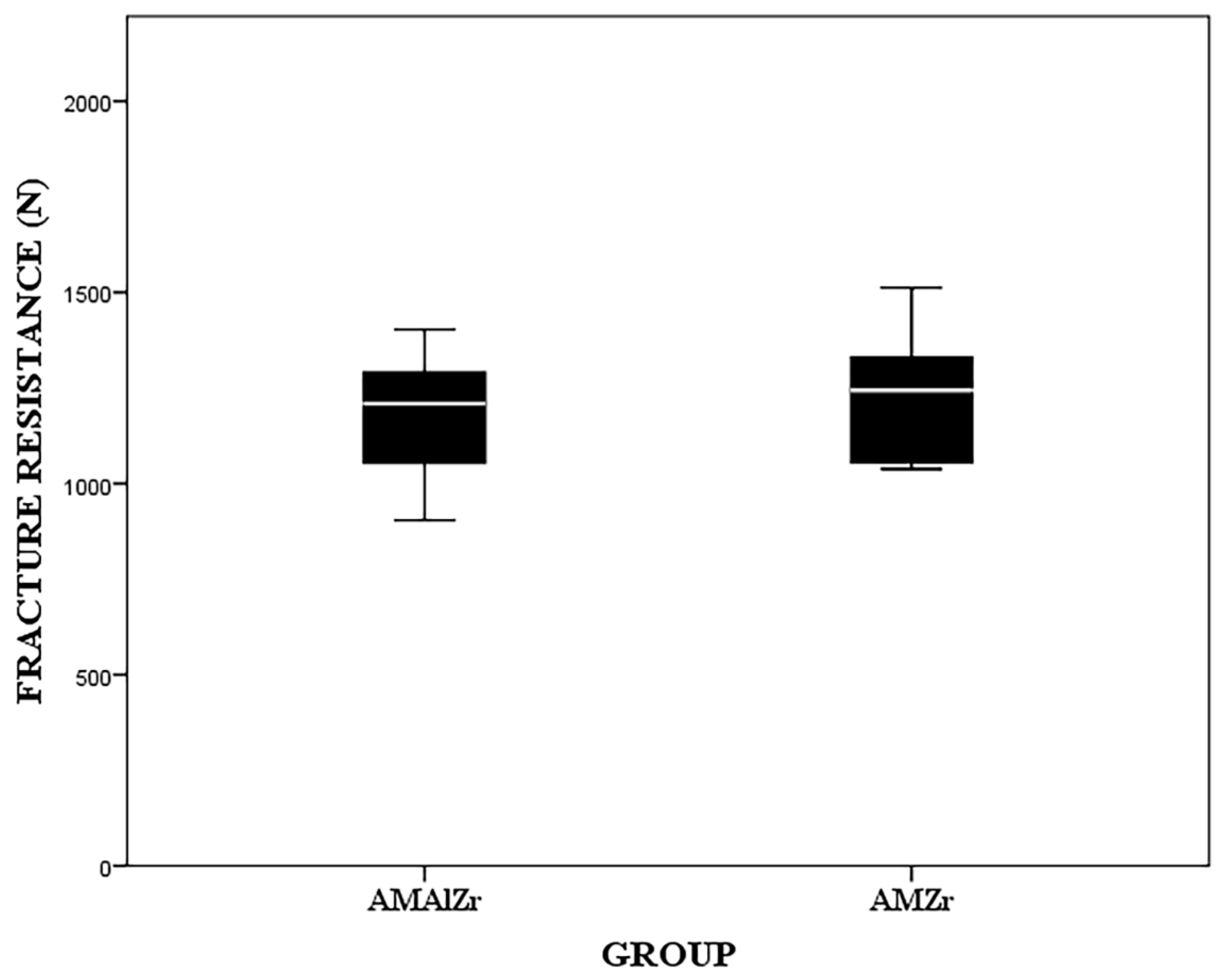
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anusavice, K.J.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials, 12th ed.; Saunders: Philadelphia, PA, USA, 2013; pp. 418–474. [Google Scholar]
- Zarone, F.; Russo, S.; Sorrentino, R. From porcelain-fused-to-metal to zirconia: Clinical and experimental considerations. Dent. Mater. 2011, 27, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.; Shenoy, N. Dental ceramics: An update. J. Conserv. Dent. 2010, 13, 195–203. [Google Scholar] [CrossRef]
- Conrad, H.J.; Seong, W.J.; Pesun, I.J. Current ceramic materials and systems with clinical recommendations: A systematic review. J. Prosthet. Dent. 2007, 98, 389–404. [Google Scholar] [CrossRef]
- Zhang, Y.; Kelly, J.R. Dental Ceramics for Restoration and Metal Veneering. Dent. Clin. North Am. 2017, 61, 797–819. [Google Scholar] [CrossRef] [PubMed]
- Simonis, P.; Dufour, T.; Tenenbaum, H. Long-term implant survival and success: A 10-16-year follow-up of non-submerged dental implants. Clin. Oral Implant. Res. 2010, 21, 772–777. [Google Scholar] [CrossRef]
- den Hartog, L.; Slater, J.J.; Vissink, A.; Meijer, H.J.; Raghoebar, G.M. Treatment outcome of immediate, early and conventional single-tooth implants in the esthetic zone: A systematic review to survival, bone level, soft-tissue, esthetics and patient satisfaction. J. Clin. Periodontol. 2008, 35, 1073–1086. [Google Scholar] [CrossRef]
- Tan, P.L.; Dunne, J.T., Jr. An esthetic comparison of a metal ceramic crown and cast metal abutment with an all-ceramic crown and zirconia abutment: A clinical report. J. Prosthet. Dent. 2004, 91, 215–218. [Google Scholar] [CrossRef]
- Nakamura, K.; Kanno, T.; Milleding, P.; Ortengren, U. Zirconia as a dental implant abutment material: A systematic review. Int. J. Prosthodont. 2010, 23, 299–309. [Google Scholar]
- Ferrari, M.; Vichi, A.; Zarone, F. Zirconia abutments and restorations: From laboratory to clinical investigations. Dent. Mater. 2015, 31, 63–76. [Google Scholar] [CrossRef]
- Mitsias, M.E.; Silva, N.R.; Pines, M.; Stappert, C.; Thompson, V.P. Reliability and fatigue damage modes of zirconia and titanium abutments. Int. J. Prosthodont. 2010, 23, 56–59. [Google Scholar]
- Rammelsberg, P.; Meyer, A.; Lorenzo-Bermejo, J.; Kappel, S.; Zenthöfer, A. Long-term chipping and failure rates of implant-supported and combined tooth–implant-supported metal-ceramic and ceramic fixed dental prostheses: A cohort study. J. Prosthet. Dent. 2021, 126, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.H.; Raffelt, C.; Pfeiffer, H.; Bizhang, M.; Saul, G.; Blunck, U.; Roulet, J.F. Restoring strength of incisors with veneers and full ceramic crowns. J. Adhes. Dent. 2010, 12, 45–54. [Google Scholar]
- Corsalini, M.; Di Venere, D.; Carossa, M.; Ripa, M.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Di Santantonio, G.; Lenoci, G.; Barile, G.; et al. Comparative clinical study between zirconium-ceramic and metal-ceramic fixed rehabilitations. Oral Implantol. 2018, 11, 150–160. [Google Scholar]
- Zisis, T.; Kordolemis, A.; Giannakopoulos, A.E. Development of Strong Surfaces Using Functionally Graded Composites Inspired by Natural Teeth—Finite Element and Experimental Verification. J. Eng. Mater. Technol. 2009, 132, 011010. [Google Scholar] [CrossRef]
- Huang, M.; Rahbar, N.; Wang, R.; Thompson, V.; Rekow, D.; Soboyejo, W.O. Bioinspired design of dental multilayers. J. Mater. Sci. Mater. Med. 2007, 464, 315–320. [Google Scholar]
- Marshall, G.W., Jr.; Balooch, M.; Gallagher, R.R.; Gansky, S.A.; Marshall, S.J. Mechanical properties of the dentinoenamel junction: AFM studies of nanohardness, elastic modulus, and fracture. J. Biomed. Mater. Res. 2001, 54, 87–95. [Google Scholar] [CrossRef]
- Niu, X.; Rahbar, N.; Farias, S.; Soboyejo, W. Bio-inspired design of dental multilayers: Experiments and model. J. Mech. Behav. Biomed. Mater. 2009, 2, 596–602. [Google Scholar] [CrossRef]
- He, L.H.; Yin, Z.H.; van Vuuren, L.J.; Carter, E.A.; Liang, X.W. A natural functionally graded biocomposite coating—Human enamel. Acta. Biomater. 2013, 9, 6330–6337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chai, H.; Lawn, B.R. Graded structures for all-ceramic restorations. J. Dent. Res. 2010, 89, 417–421. [Google Scholar] [CrossRef] [Green Version]
- Silva, N.R.; Witek, L.; Coelho, P.G.; Thompson, V.P.; Rekow, E.D.; Smay, J. Additive CAD/CAM process for dental prostheses. J. Prosthodont. 2011, 20, 93–96. [Google Scholar] [CrossRef]
- Strub, J.R.; Rekow, E.D.; Witkowski, S. Computer-aided design and fabrication of dental restorations: Current systems and future possibilities. J. Am. Dent. Assoc. 2006, 137, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Huang, H. Machining characteristics and surface integrity of yttria stabilized tetragonal zirconia in high speed deep grinding. J. Mater. Sci. Eng. A 2003, 345, 155–163. [Google Scholar] [CrossRef]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Zhang, Y.; Liu, Z.; Wei, B. Effects of repeated firing on the marginal accuracy of Co-Cr copings fabricated by selective laser melting. J. Prosthet. Dent. 2015, 113, 135–139. [Google Scholar] [CrossRef]
- Hoang, L.N.; Thompson, G.A.; Cho, S.H.; Berzins, D.W.; Ahn, K.W. Die spacer thickness reproduction for central incisor crown fabrication with combined computer-aided design and 3D printing technology: An in vitro study. J. Prosthet. Dent. 2015, 113, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehurtevent, M.; Robberecht, L.; Hornez, J.C.; Thuault, A.; Deveaux, E.; Behin, P. Stereolithography: A new method for processing dental ceramics by additive computer-aided manufacturing. Dent. Mater. 2017, 33, 477–485. [Google Scholar] [CrossRef]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef]
- Ebert, J.; Ozkol, E.; Zeichner, A.; Uibel, K.; Weiss, O.; Koops, U.; Telle, R.; Fischer, H. Direct inkjet printing of dental prostheses made of zirconia. J. Dent. Res. 2009, 88, 673–676. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- ASTM. Standard Terminology for Additive Manufacturing—General Principles and Terminology. ISO/ASTM52900-15. Available online: https://www.astm.org/Standards/ISOASTM52900.htm (accessed on 10 August 2021).
- Stamp, R.; Fox, P.; O’Neill, W.; Jones, E.; Sutcliffe, C. The development of a scanning strategy for the manufacture of porous biomaterials by selective laser melting. J. Mater. Sci. Mater. Med. 2009, 20, 1839–1848. [Google Scholar] [CrossRef]
- Deckard, C.; Beaman, J.J. Process and control issues in selective laser sintering. ASME Prod. Eng. Div. PED 1988, 33, 191–197. [Google Scholar]
- Traini, T.; Mangano, C.; Sammons, R.L.; Mangano, F.; Macchi, A.; Piattelli, A. Direct laser metal sintering as a new approach to fabrication of an isoelastic functionally graded material for manufacture of porous titanium dental implants. Dent. Mater. 2008, 24, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.S.; Starr, T.L.; Harris, B.T.; Zandinejad, A.; Morton, D. Additive manufacturing technology (direct metal laser sintering) as a novel approach to fabricate functionally graded titanium implants: Preliminary investigation of fabrication parameters. Int. J. Oral. Maxillofac. Implants. 2013, 28, 1490–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.S.; Zandinejad, A.; Morton, D. Methods for Fabricating Dental Prostheses. U.S. Patent 10045839 B2, 14 August 2018. [Google Scholar]
- Zandinejad, A.; Lin, W.S.; Morton, D. Method for Fabricating Dental Restorations. U.S. Patent 10716648 B2, 21 July 2020. [Google Scholar]
- Zandinejad, A.; Methani, M.M.; Schneiderman, E.D.; Revilla-Leon, M.; Morton, D. Fracture Resistance of Additively Manufactured Zirconia Crowns when Cemented to Implant Supported Zirconia Abutments: An in vitro Study. J. Prosthodont. 2019, 28, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Att, W.; Kurun, S.; Gerds, T.; Strub, J.R. Fracture resistance of single-tooth implant-supported all-ceramic restorations: An in vitro study. J. Prosthet. Dent. 2006, 95, 111–116. [Google Scholar] [CrossRef]
- Klotz, M.W.; Taylor, T.D.; Goldberg, A.J. Wear at the Titanium-Zirconia Implant-Abutment Interface: A Pilot Study. Int. J. Oral. Maxillofac. Implants. 2011, 26, 970–975. [Google Scholar] [PubMed]
- Bidra, A.S.; Rungruanganunt, P. Clinical outcomes of implant abutments in the anterior region: A systematic review. J. Esthet. Restor. Dent. 2013, 25, 159–176. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, G.; Fradeani, M.; Dellificorelli, G.; De Lorenzi, M.; Zarone, F.; Sorrentino, R. Clinical Evaluation of the Influence of Connection Type and Restoration Height on the Reliability of Zirconia Abutments: A Retrospective Study on 965 Abutments with a Mean 6-Year Follow-Up. Int. J. Periodontics Restor. Dent. 2017, 37, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Rus, F.; Ferreiroa, A.; Özcan, M.; Bartolomé, J.F.; Pradíes, G. Fracture resistance of crowns cemented on titanium and zirconia implant abutments: A comparison of monolithic versus manually veneered all-ceramic systems. Int. J. Oral Maxillofac. Implants 2012, 27, 1448–1455. [Google Scholar]
- Jang, Y.; Sim, J.Y.; Park, J.K.; Kim, J.H.; Kim, H.Y. Evaluation of the marginal and internal fit of a single crown fabricated based on a three-dimensional printed model. J. Adv. Prosthodont. 2018, 10, 367–373. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical/Mechanical Properties | 3DMix ZrO2 3D CERAM | 3DMix ATZ 3D CERAM |
|---|---|---|
| Grade | 700 | NP * |
| Particle size (μm) | 0.1–0.8 | >5.2 |
| Density (g/cm3) | 5.97 | >5.2 |
| Vickers Hardness (GPa) | 12.6 | NP* |
| Young’s modulus (GPa) | 209.4 | 220 |
| Weibull modulus | NP * | 5.8 |
| Shear modulus (GPa) | 79.8 | NP * |
| Flexural strength (MPa) | 1088 | 1094 |
| Compressive strength (MPa) | 2070 | NP * |
| Coefficient thermal expansion (K−1) | 12.4 | 7.50 to 8.33 |
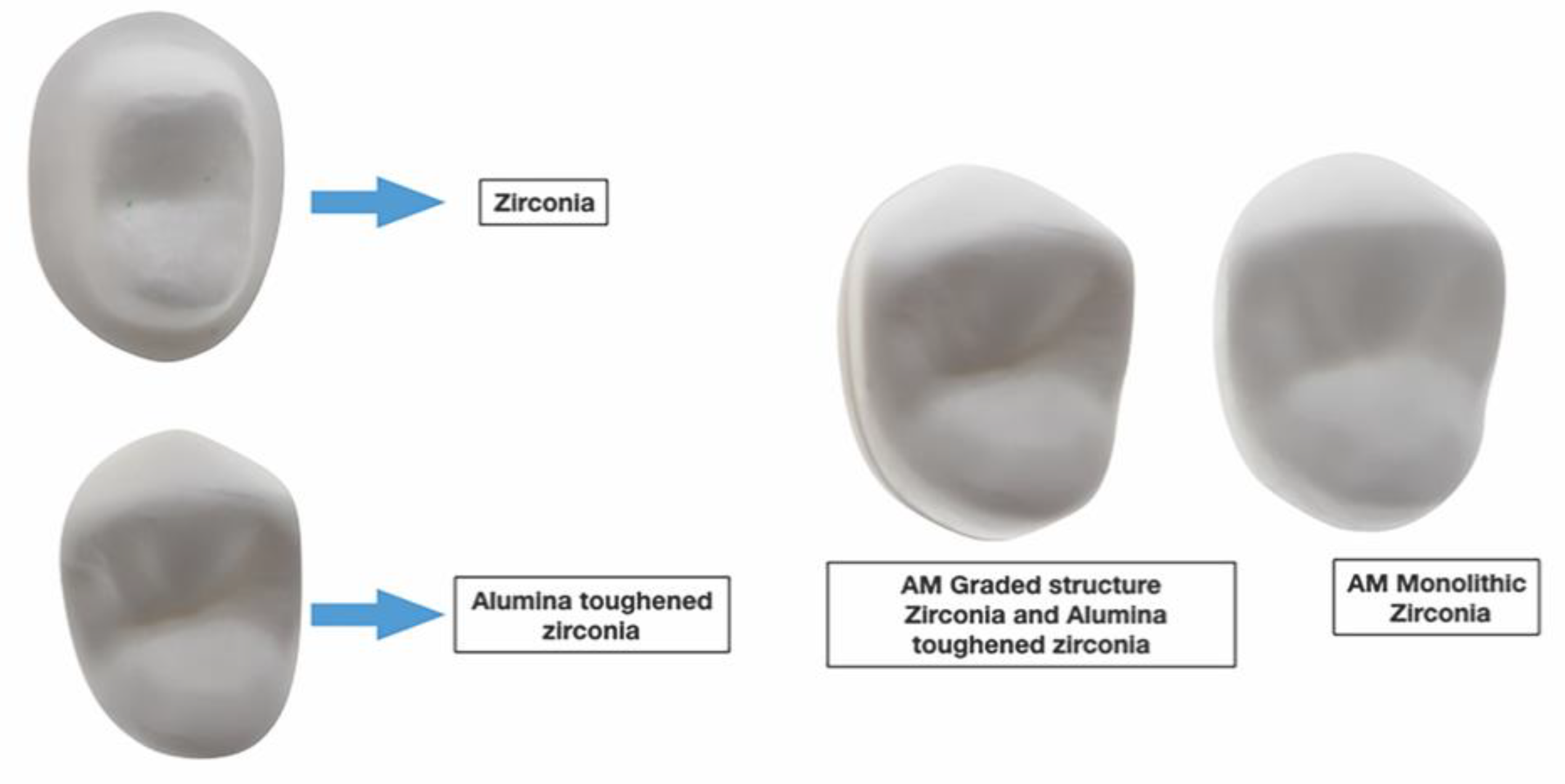
| Group | Material | Fabrication Technique | Composition |
|---|---|---|---|
| AMZr | 3DMix ZrO2 (3D Ceram) | Laser Stereolithography (SLA) | Zirconia stabilized with 3% yttria |
| AMAlZr | 3DMix ATZ (3DCeram) | Laser Stereolithography (SLA) | The ceramic ATZ combines both Alumina (20%) and Zirconia (80%) ceramics in one |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zandinejad, A.; Revilla-León, M.; Methani, M.M.; Nasiry Khanlar, L.; Morton, D. The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study. Dent. J. 2021, 9, 115. https://doi.org/10.3390/dj9100115
Zandinejad A, Revilla-León M, Methani MM, Nasiry Khanlar L, Morton D. The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study. Dentistry Journal. 2021; 9(10):115. https://doi.org/10.3390/dj9100115
Chicago/Turabian StyleZandinejad, Amirali, Marta Revilla-León, Mohammad Mujtaba Methani, Leila Nasiry Khanlar, and Dean Morton. 2021. "The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study" Dentistry Journal 9, no. 10: 115. https://doi.org/10.3390/dj9100115
APA StyleZandinejad, A., Revilla-León, M., Methani, M. M., Nasiry Khanlar, L., & Morton, D. (2021). The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study. Dentistry Journal, 9(10), 115. https://doi.org/10.3390/dj9100115