Uprighting Impacted Mandibular Second Molar Using a Skeletal Anchorage: A Case Report

 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
- to show an innovative combined orthodontic-surgical procedure to solve a moderately mesially-impacted mandibular second molar (MM2) using an orthodontic miniscrew with an elastic chain;
- to evaluate the impact of this procedure on the Oral health–related quality of life (OHRQoL).
2. Materials and Methods
2.1. Case Presentation
2.2. Treatment Plan
- maxillary canines impaction (1.3 and 2.3);
- MM2 impaction (3.7 and 4.7)
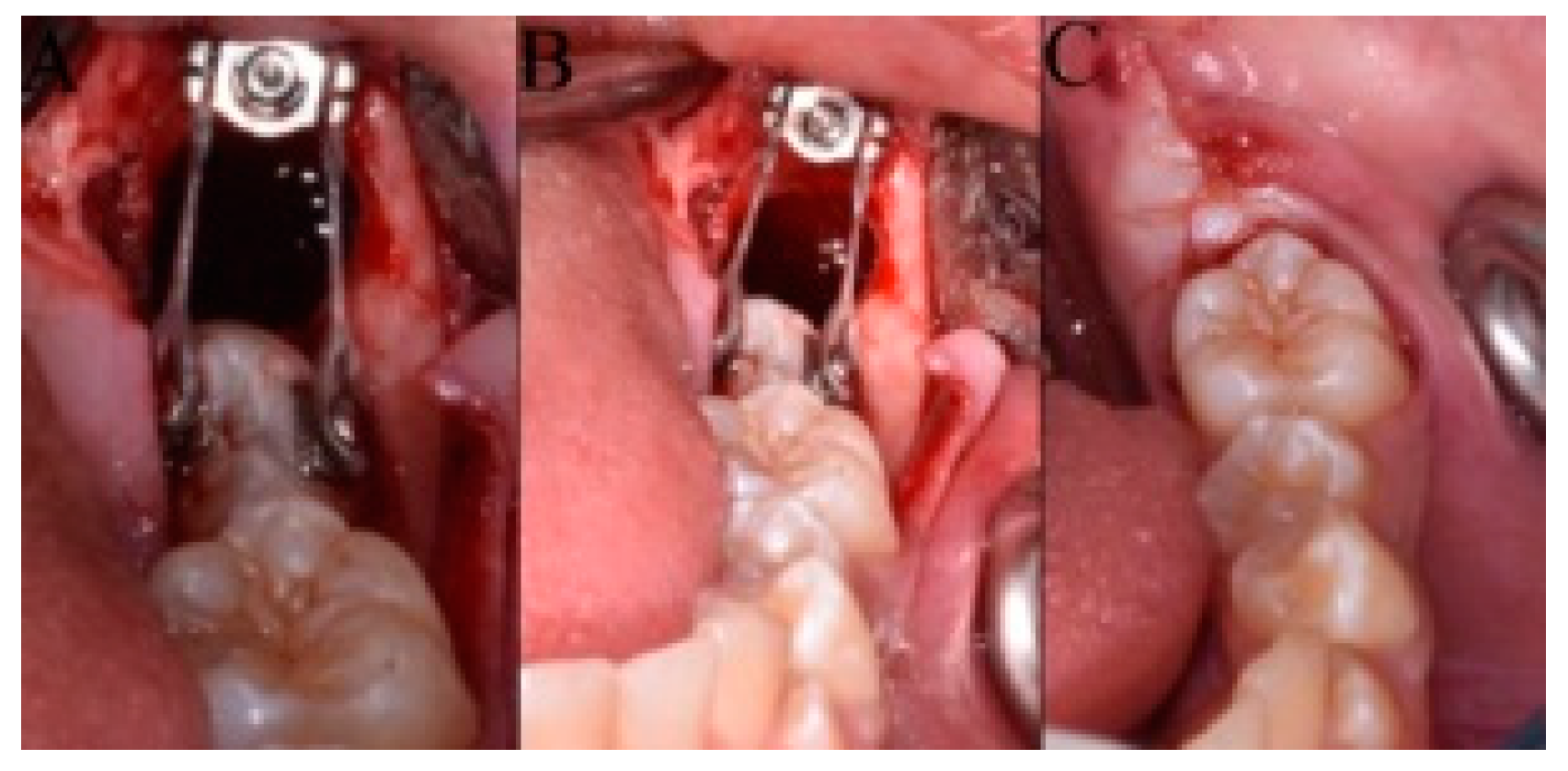
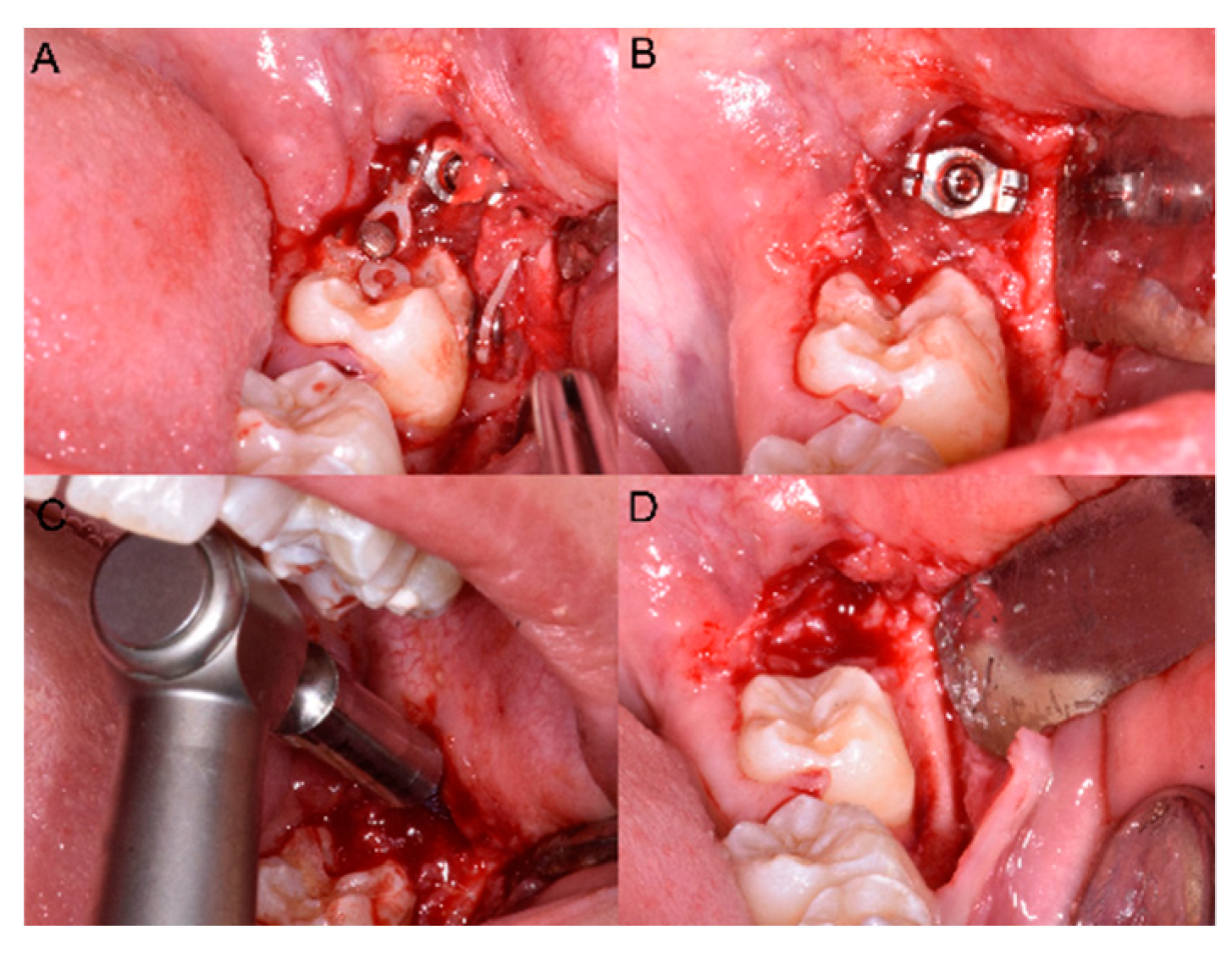
2.3. Surgical-Orthodontic Treatment of an Impacted MM2
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fu, P.S.; Wang, J.C.; Wu, Y.M.; Huang, T.K.; Chen, W.C.; Tseng, Y.C.; Tseng, C.H.; Hung, C.C. Impacted mandibular second molars. Angle Orthod. 2012, 82, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Guarnieri, R.; Padalino, G.; Di Giorgio, R.; Barbato, E. Maxillary canine impaction and the association with dental and skeletal anomalies: A retrospective study|[Inclusione del canino mascellare e anomalie dentali e scheletriche associate: Uno studio retrospettivo]. Dent. Cadmos 2018, 86, 603–610. [Google Scholar] [CrossRef]
- Cassetta, M.; Guarnieri, R.; Altieri, F.; Brandetti, G.; Padalino, G.; Di Giorgio, R.; Barbato, E. Relationship between upper lateral incisors anomalies and palatal displaced canine: A case-control retrospective study. Minerva Stomatol. 2020, 69, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Giordano, A. Mirror imaging of impacted and supernumerary teeth in dizygotic twins: A case report. J. Clin. Exp. Dent. 2015, 7, e167–e169. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cassetta, M.; Altieri, F.; Di Mambro, A.; Giansanti, M.; Barbato, E.; Galluccio, G. Impaction of permanent mandibular second molar: A retrospective study. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e564–e568. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Calasso, S. Etiological factors in second mandibular molar impaction. J. Clin. Exp. Dent. 2014, 6, e150–e154. [Google Scholar] [CrossRef] [PubMed]
- Sawicka, M.; Racka-Pilszak, B.; Rosnowska-Mazurkiewicz, A. Uprighting partially impacted permanent second molars. Angle Orthod. 2007, 77, 148–154. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F. The treatment of impacted mandibular second molars using brass wire: A prospective clinical study. [La disinclusione del secondo molare mandibolare con l’utilizzo del filo di ottone: Uno studio clinico prospettico]. Dent. Cadmos 2017, 85, 475–482. [Google Scholar] [CrossRef]
- Kupietzky, A. Correction of eruption of permanent molars utilizing the brass wire technique. Pediatr. Dent. 2000, 22, 408–412. [Google Scholar]
- Cassetta, M.; Altieri, F. The influence of mandibular third molar germectomy on the treatment time of impacted mandibular second molars using brass wire: A prospective clinical pilot study. Int. J. Oral Maxillofac. Surg. 2017, 46, 905–911. [Google Scholar] [CrossRef]
- Pogrel, M.A. The surgical uprighting of mandibular second molars. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 180–183. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Di Mambro, A.; Giansanti, M.; Galluccio, G.; Barbato, E. A retrospective study on impaction of mandibular second molar. Dent. Cadmos 2013, 81, 603–611. [Google Scholar] [CrossRef]
- Papadopoulos, M.A.; Tarawneh, F. The use of miniscrew implants for temporary skeletal anchorage in orthodontics: A comprehensive review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, e6–e15. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Altieri, F.; Di Giorgio, R.; Barbato, E. Palatal orthodontic miniscrew insertion using a CAD-CAM surgical guide: Description of a technique. Int. J. Oral Maxillofac. Surg. 2018, 47, 1195–1198. [Google Scholar] [CrossRef] [PubMed]
- Altieri, F.; Padalino, G.; Guarnieri, R.; Barbato, E.; Cassetta, M. Computer-guided palatal canine disimpaction: A technical note. Int. J. Comput. Dent. 2020, 23, 219–224. [Google Scholar] [PubMed]
- Cassetta, M.; Brandetti, G.; Altieri, F. Miniscrew-supported distal jet versus conventional distal jet appliance: A pilot study. J. Clin. Exp. Dent. 2019, 11, e650–e658. [Google Scholar] [CrossRef]
- Evans, R. Incidence of lower second permanent molar impaction. Br. J. Orthod. 1988, 15, 199–203. [Google Scholar] [CrossRef]
- Franchignoni, M.; Giordano, A.; Brigatti, E.; Migliario, M.; Levrini, L.; Ferriero, G. Psychometric properties of the Italian version of the reduced form of the Oral Health Impact Profile (OHIP-14). G. Ital. Med. Lav. Ergon. 2010, 32, B71–B78. [Google Scholar]
- Altieri, F.; Cassetta, M. The impact of tooth-borne vs computer-guided bone-borne rapid maxillary expansion on pain and oral health–related quality of life: A parallel cohort study. Am. J. Orthod. Dentofac. Orthop. 2020, 158, e83–e90. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Di Giorgio, R.; Silvestri, A. Two-dimensional and three-dimensional cephalometry using cone beam computed tomography scans. J. Craniofac. Surg. 2005, 26, e311–e315. [Google Scholar]
- Lau, C.K.; Whang, C.Z.; Bister, D. Orthodontic uprighting of severely impacted mandibular second molars. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 116–124. [Google Scholar] [CrossRef] [PubMed]
- McAboy, C.P.; Grumet, J.T.; Siegel, E.B.; Iacopino, A.M. Surgical uprighting and repositioning of severely impacted mandibular second molars. J. Am. Dent. Assoc. 2003, 134, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Giancotti, A.; Arcuri, C.; Barlattani, A. Treatment of ectopic mandibular second molar with titanium miniscrews. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 113–117. [Google Scholar] [CrossRef]
- Miyahira, Y.I.; Maltagliati, L.A.; Siqueira, D.F.; Romanoc, R. Miniplates as skeletal anchorage for treating mandibular second molar impactions. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Zhen, J.; Liu, C.H.; Zhang, W.X.; Zhou, L.S.; He, H.X.; Qin, X.; Lan, Z.D. Uprigting deeply impacted mandibular second molars with miniscrew anchorage. J. Clin. Orthod. 2019, 53, 405–413. [Google Scholar] [PubMed]
- Finotti, M.; Del Torre, M.; Roberto, M.; Miotti, F.A. Could the distalization of the mandibular molars be facilitated? A new therapeutic method. Orthod. Fr. 2009, 80, 371–378. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Giansanti, M.; Bellardini, M.; Brandetti, G.; Piccoli, L. Is there a learning curve in static computer-assisted surgery? A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020, 49, 1335–1342. [Google Scholar] [CrossRef]
- Iezzi, G.; Perrotti, V.; Piattelli, A.; D’Arcangelo, C.; Altieri, F.; Cassetta, M. Split crest technique for implant treatment of agenesis of upper lateral incisors: Results of a randomized pilot histological and clinical study at 24-mont follow-up. Braz. Oral Res. 2020, 34, e118. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, F.; Guarnieri, R.; Mezio, M.; Padalino, G.; Cipollone, A.; Barbato, E.; Cassetta, M. Uprighting Impacted Mandibular Second Molar Using a Skeletal Anchorage: A Case Report. Dent. J. 2020, 8, 129. https://doi.org/10.3390/dj8040129
Altieri F, Guarnieri R, Mezio M, Padalino G, Cipollone A, Barbato E, Cassetta M. Uprighting Impacted Mandibular Second Molar Using a Skeletal Anchorage: A Case Report. Dentistry Journal. 2020; 8(4):129. https://doi.org/10.3390/dj8040129
Chicago/Turabian StyleAltieri, Federica, Rosanna Guarnieri, Martina Mezio, Gabriella Padalino, Angela Cipollone, Ersilia Barbato, and Michele Cassetta. 2020. "Uprighting Impacted Mandibular Second Molar Using a Skeletal Anchorage: A Case Report" Dentistry Journal 8, no. 4: 129. https://doi.org/10.3390/dj8040129
APA StyleAltieri, F., Guarnieri, R., Mezio, M., Padalino, G., Cipollone, A., Barbato, E., & Cassetta, M. (2020). Uprighting Impacted Mandibular Second Molar Using a Skeletal Anchorage: A Case Report. Dentistry Journal, 8(4), 129. https://doi.org/10.3390/dj8040129