
Histomorphometric Evaluation of Gingival Phenotypic Characteristics: A Cross-Sectional Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Assessments
- (a)
- Probe Visibility (PV): Participants were categorized into thin and thick PV groups based on the visibility of a periodontal probe through the gingiva after its insertion into the gingival sulcus (Figure 1). Intra-examiner reproducibility was evaluated prior to the study through duplicate assessments of thirty maxillary incisors performed 15 days apart, yielding a high Cohen’s kappa coefficient of 0.870.
- (b)
- Keratinized Tissue Width (KTW): This was measured as the distance between the mucogingival junction (MGJ) defined using the wrinkling method and the zenith of the free gingiva of one maxillary central incisor. A periodontal probe was positioned parallel to the sagittal plane, and a standardized photograph was taken with a camera aligned to the participant’s frontal plane. The image was subsequently analyzed using specialized image analysis software (ImageJ) and KTW was digitally measured following calibration (Figure 1).
2.2. Histological Assessments
- (a)
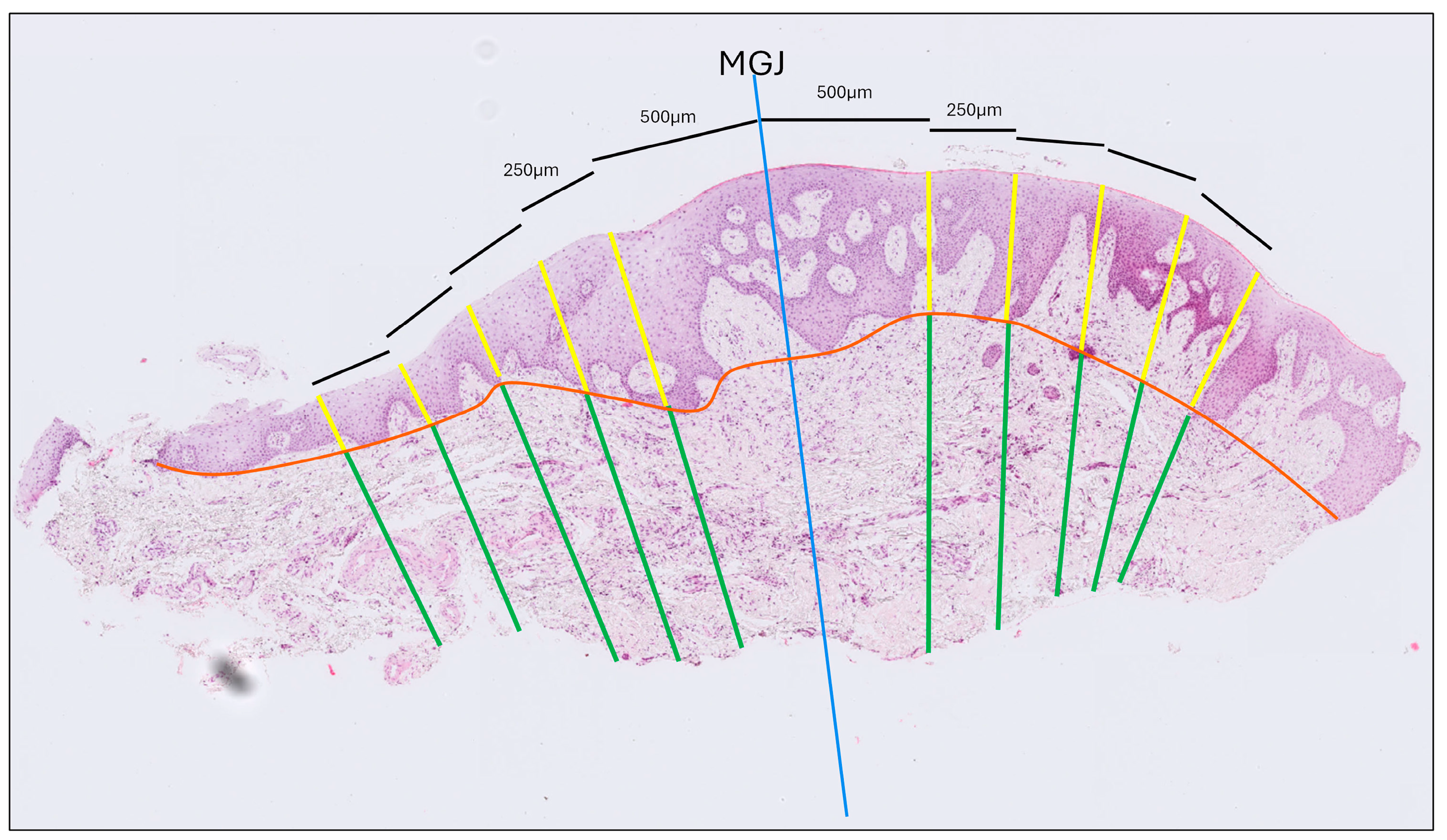
- Gingival Thickness (GT): Defined as the length of a line drawn perpendicular to the epithelial surface, extending from the epithelial surface to the excised surface of the connective tissue and calculated as the mean of five measurements taken at 500, 750, 1000, 1250 and 1500 μm coronally to the MGJ (Figure 2).
- (b)
- Gingival Epithelium Thickness (G-Ep): Calculated by averaging the lengths of the epithelial portions of the previously drawn lines. For this measurement, a line connecting the deepest points of the epithelial projections was drawn to delineate the boundary between the epithelium and connective tissue (Figure 2).
- (c)
- Gingival Connective Tissue Thickness (G-CT): Measured using the same set of lines as the average length of the portions extending from the excised surface of the connective tissue to the epithelial boundary line (Figure 2).
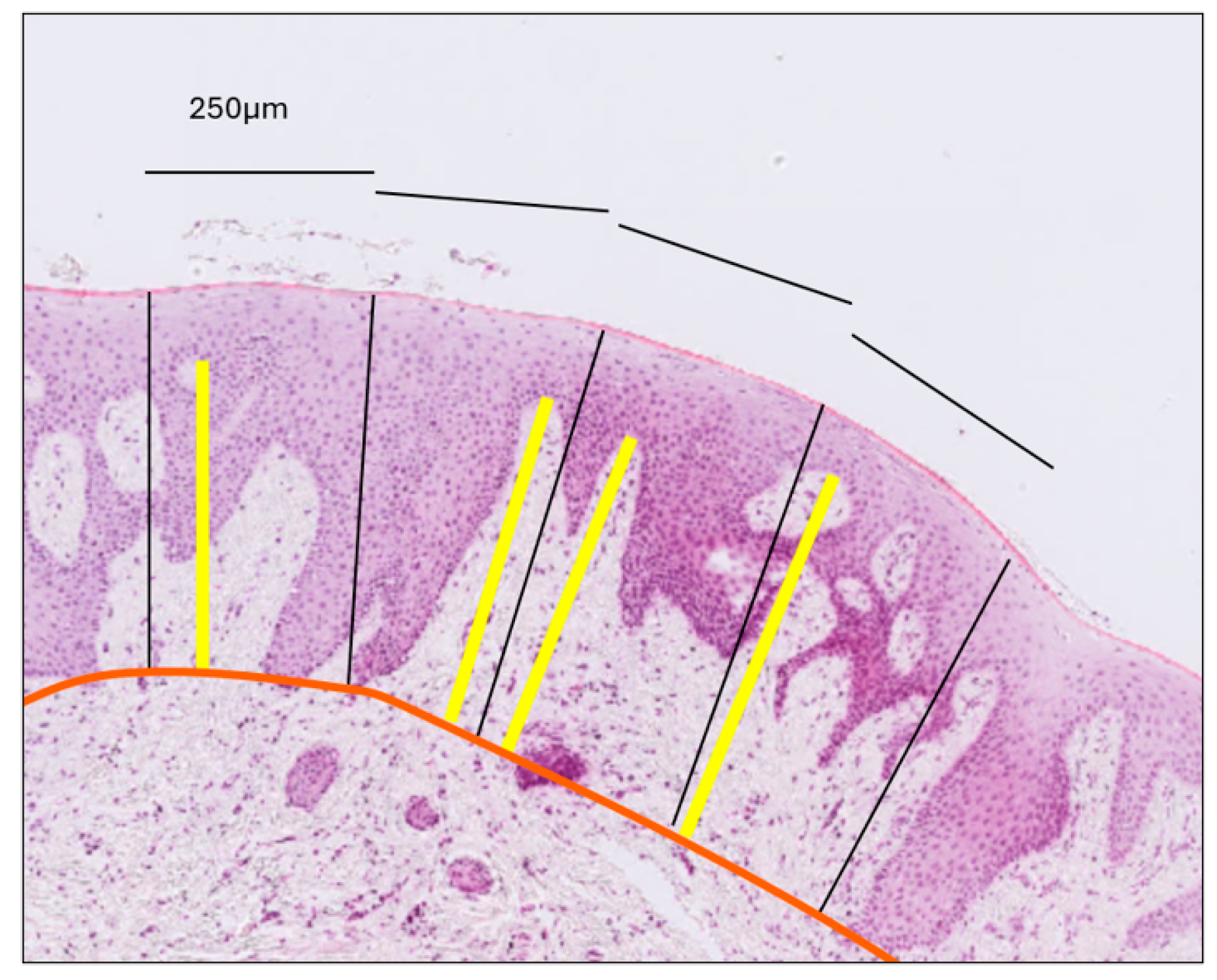
- (d)
- Gingival Papilla Length (G-P): Assessed as the average length of the longest papillae observed within each epithelial compartment, as defined by the previously established perpendicular lines (Figure 3).
- (e)
- Gingival Papilla Density (G-Pd) (number/mm): Assessed as the number of clearly identifiable epithelial papillae divided by the total length of the epithelial surface.
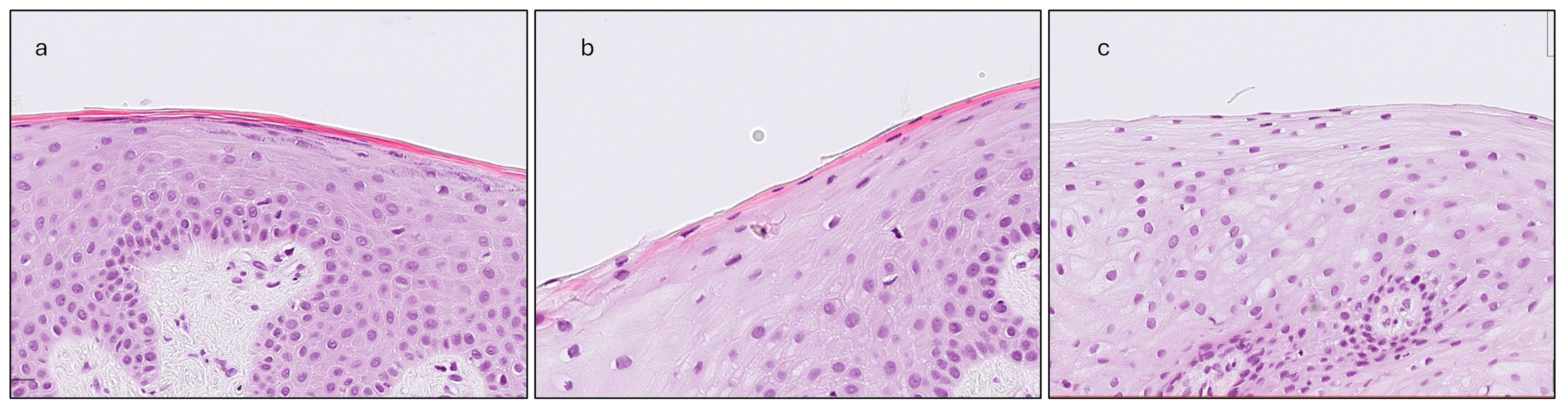
- (f)
- Gingival Keratinization (G-Ker): Assessed as the highest level of keratinization observed across the superficial layer of the gingiva epithelium. The levels recorded were defined as follows: ortho-keratinization, when a well-defined keratin layer with anucleate cells was observed; para-keratinization, when a keratin layer with flattened cells that retained their nuclei were observed; and non-keratinization, when a keratin layer was not observed, and superficial cells retained their shape and nuclei (Figure 4).
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malpartida-Carrillo, V.; Tinedo-Lopez, P.L.; Guerrero, M.E.; Amaya-Pajares, S.P.; Özcan, M.; Rösing, C.K. Periodontal phenotype: A review of historical and current classifications evaluating different methods and characteristics. J. Esthet. Restor. Dent. 2021, 33, 432–445. [Google Scholar] [CrossRef]
- Zweers, J.; Thomas, R.Z.; Slot, D.E.; Weisgold, A.S.; Van Der Weijden, F.G.A. Characteristics of periodontal biotype, its dimensions, associations and prevalence: A systematic review. J. Clin. Periodontol. 2014, 41, 958–971. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.M.; Bassir, S.H.; Nguyen, T.T. Effect of gingival phenotype on the maintenance of periodontal health: An American Academy of Periodontology best evidence review. J. Periodontol. 2020, 91, 311–338. [Google Scholar] [CrossRef]
- Pontoriero, R.; Carnevale, G. Surgical crown lengthening: A 12-month clinical wound healing study. J. Periodontol. 2001, 72, 841–848. [Google Scholar] [CrossRef]
- Tao, J.; Wu, Y.; Chen, J.; Su, J. A follow-up study of up to 5 years of metal-ceramic crowns in maxillary central incisors for different gingival biotypes. Int. J. Periodontics Restor. Dent. 2014, 34, 85–92. [Google Scholar] [CrossRef]
- De Rouck, T.; Eghbali, R.; Collys, K.; De Bruyn, H.; Cosyn, J. The gingival biotype revisited: Transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J. Clin. Periodontol. 2009, 36, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Rungcharassaeng, K.; Umezu, K.; Kois, J.C. Dimensions of peri-implant mucosa: An evaluation of maxillary anterior single implants in humans. J. Periodontol. 2003, 74, 557–562. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.K.; Morimoto, T.; Rungcharassaeng, K.; Roe, P.; Smith, D.H. Gingival biotype assessment in the esthetic zone: Visual versus direct measurement. Int. J. Periodontics Restor. Dent. 2010, 30, 237–243. [Google Scholar]
- Müller, H.-P.; Heinecke, A.; Schaller, N.; Eger, T. Masticatory mucosa in subjects with different periodontal phenotypes. J. Clin. Periodontol. 2000, 27, 621–626. [Google Scholar] [CrossRef]
- Nikiforidou, M.; Tsalikis, L.; Angelopoulos, C.; Menexes, G.; Vouros, I.; Konstantinides, A. Classification of periodontal biotypes with the use of CBCT. A cross-sectional study. Clin. Oral Investig. 2016, 20, 2061–2071. [Google Scholar] [CrossRef]
- Abdelhafez, R.S.; Mustafa, N.M. Determining the periodontal phenotype—Probe transparency versus actual: A diagnostic study. J. Esthet. Restor. Dent. 2023, 35, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Couso-Queiruga, E.; Barboza, E.P.; Avila-Ortiz, G.; Gonzalez-Martin, O.; Chambrone, L.; Rodrigues, D.M. Relationship between supracrestal soft tissue dimensions and other periodontal phenotypic features: A cross-sectional study. J. Periodontol. 2023, 94, 944–955. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.M.; Petersen, R.L.; De Moraes, J.R.; Barboza, E.P. Gingival landmarks and cutting points for gingival phenotype determination: A clinical and tomographic cross-sectional study. J. Periodontol. 2022, 93, 1916–1928. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S237–S248. [Google Scholar] [CrossRef]
- Chavrier, C.; Couble, M.L.; Magloire, H.; Grimaud, J.A. Connective tissue organization of healthy human gingiva: Ultrastructural localization of collagen types I–III–IV. J. Periodontal Res. 1984, 19, 221–229. [Google Scholar] [CrossRef]
- Motta, S.H.G.; Camacho, M.P.F.; Quintela, D.C.; Santana, R.B. Relationship Between Clinical and Histologic Periodontal Biotypes in Humans. Int. J. Periodontics Restor. Dent. 2017, 37, 737–741. [Google Scholar] [CrossRef]
- Hwang, D.; Wang, H.-L. Flap Thickness as a Predictor of Root Coverage: A Systematic Review. J. Periodontol. 2006, 77, 1625–1634. [Google Scholar] [CrossRef]
- Stein, J.M.; Lintel-Höping, N.; Hammächer, C.; Kasaj, A.; Tamm, M.; Hanisch, O. The gingival biotype: Measurement of soft and hard tissue dimensions—A radiographic morphometric study. J. Clin. Periodontol. 2013, 40, 1132–1139. [Google Scholar] [CrossRef]
- Chen, H.; Luo, T.; He, S.; Sa, G. Regulatory mechanism of oral mucosal rete peg formation. J. Mol. Histol. 2021, 52, 859–868. [Google Scholar] [CrossRef]
- Da Costa, F.A.; Perussolo, J.; Dias, D.R.; Araújo, M.G. Identification of thin and thick gingival phenotypes by two transparency methods: A diagnostic accuracy study. J. Periodontol. 2023, 94, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.R.; Richter, T.; Kebschull, M.; Petersen, N.; Fickl, S. On the relationship between gingival biotypes and gingival thickness in young Caucasians. Clin. Oral Implant. Res. 2015, 26, 865–869. [Google Scholar] [CrossRef]
- Shah, R.; Sowmya, N.; Mehta, D. Prevalence of gingival biotype and its relationship to clinical parameters. Contemp. Clin. Dent. 2015, 6, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Amid, R.; Mirakhori, M.; Safi, Y.; Kadkhodazadeh, M.; Namdari, M. Assessment of gingival biotype and facial hard/soft tissue dimensions in the maxillary anterior teeth region using cone beam computed tomography. Arch. Oral Biol. 2017, 79, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ruan, Y.; Chen, J.; Luo, Y.; Yang, F. Assessment of the relationship between labial gingival thickness and the underlying bone thickness in maxillary anterior teeth by two digital techniques. Sci. Rep. 2022, 12, 709. [Google Scholar] [CrossRef] [PubMed]
- Goktas, S.; Dmytryk, J.J.; McFetridge, P. Biomechanical Behavior of Oral Soft Tissues. J. Periodontol. 2011, 82, 1178–1186. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Thin | Thick | |
|---|---|---|---|
| Subjects | 45 | 21 | 24 |
| Age (mean, SD) | 36.11 ± 10.9 | 37.33 ± 12.16 | 35.04 ± 9.81 |
| Female/male | 26/19 | 15/6 | 11/13 |
| Smokers/non-smokers | 13/32 | 4/17 | 9/15 |
| Histological samples | 36 | 17 | 19 |
| Total | Thin | Thick | Δ Thin–Thick | |
|---|---|---|---|---|
| GT | 1.05 ± 0.25 | 1.00 ± 0.22 | 1.09 ± 0.26 | 0.298 |
| G-CT | 0.68 ± 0.20 | 0.64 ± 0.15 | 0.72 ± 0.23 | 0.212 |
| G-Ep | 0.36 ± 0.09 | 0.35 ± 0.09 | 0.37 ± 0.10 | 0.626 |
| G-P | 0.26 ± 0.09 | 0.23 ± 0.08 | 0.27 ± 0.08 | 0.142 |
| G-Pd | 7.12 ± 1.59 | 7.38 ± 1.89 | 6.89 ± 1.28 | 0.368 |
| MT | 1.00 ± 0.23 | 0.94 ± 0.20 | 1.07 ± 0.25 | 0.128 |
| M-CT | 0.75 ± 0.23 | 0.69 ± 0.29 | 0.82 ± 0.27 | 0.121 |
| M-Ep | 0.25 ± 0.08 | 0.25 ± 0.08 | 0.25 ± 0.07 | 0.930 |
| M-P | 0.14 ± 0.07 | 0.14 ± 0.07 | 0.24 ± 0.07 | 0.635 |
| M-Pd | 5.70 ± 1.75 | 5.61 ± 1.66 | 5.79 ± 1.88 | 0.788 |
| KTW | 4.21 ± 1.00 | 3.90 ± 0.86 | 4.48 ± 1.06 | 0.023 * |
| Δ | Mean (mm) | p |
|---|---|---|
| GT–MT | 0.09 ± 0.15 | 0.003 * |
| G-CT–M-CT | −0.03 ± 0.35 | 0.301 |
| G-Ep–M-Ep | 0.11 ± 0.08 | <0.001 * |
| G-P–M-P | 0.12 ± 0.08 | <0.001 * |
| G-Pd–M-Pd (mm−1) | 1.24 ± 1.76 | <0.001 * |
| PV | GT | MT | KTW | |||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| GT | 0.178 | 0.298 | - | - | 0.602 | <0.001 * | 0.276 | 0.187 |
| G-CT | 0.213 | 0.212 | 0.917 | <0.001 * | 0.716 | <0.001 * | 0.067 | 0.699 |
| G-Ep | 0.084 | 0.626 | 0.630 | <0.001 * | 0.350 | 0.067 | 0.386 | 0.020 * |
| G-P | 0.249 | 0.142 | 0.737 | <0.001 * | 0.410 | 0.030 * | 0.351 | 0.036 * |
| G-Pd | −0.154 | 0.368 | −0.348 | 0.036 * | −0.029 | 0.996 | −0.233 | 0.171 |
| MT | 0.295 | 0.128 | 0.602 | <0.001 * | - | - | 0.131 | 0.508 |
| M-CT | 0.300 | 0.121 | 0.725 | <0.001 * | 0.944 | <0.001 * | 0.149 | 0.450 |
| M-Ep | 0.001 | 0.997 | 0.234 | 0.222 | 0.109 | 0.581 | 0.066 | 0.733 |
| M-P | −0.035 | 0.851 | 0.202 | 0.284 | 0.057 | 0.771 | 0.167 | 0.369 |
| M-Pd | 0.050 | 0.788 | 0.005 | 0.980 | 0.058 | 0.769 | 0.242 | 0.190 |
| G-Ker | 0.003 | 0.955 | 0.323 | 0.062 | 0.240 | 0.219 | 0.036 | 0.836 |
| M-Ker | 0.253 | 0.232 | 0.367 | 0.046 * | 0.532 | 0.004 * | 0.096 | 0.607 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papapetros, D.; Nylander, K.; Kalfas, S. Histomorphometric Evaluation of Gingival Phenotypic Characteristics: A Cross-Sectional Study. Dent. J. 2025, 13, 350. https://doi.org/10.3390/dj13080350
Papapetros D, Nylander K, Kalfas S. Histomorphometric Evaluation of Gingival Phenotypic Characteristics: A Cross-Sectional Study. Dentistry Journal. 2025; 13(8):350. https://doi.org/10.3390/dj13080350
Chicago/Turabian StylePapapetros, Dimitrios, Karin Nylander, and Sotirios Kalfas. 2025. "Histomorphometric Evaluation of Gingival Phenotypic Characteristics: A Cross-Sectional Study" Dentistry Journal 13, no. 8: 350. https://doi.org/10.3390/dj13080350
APA StylePapapetros, D., Nylander, K., & Kalfas, S. (2025). Histomorphometric Evaluation of Gingival Phenotypic Characteristics: A Cross-Sectional Study. Dentistry Journal, 13(8), 350. https://doi.org/10.3390/dj13080350