
Evaluation of the Efficacy of Corticotomy and Piezocision on Canine Retraction: A Systematic Review

 , and
, and 
Abstract
1. Introduction
- (1)
- (2)
- (3)
- Surgical: corticotomy, corticision, and piezocision.
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Collection
- (a)
- Authors and year of publication;
- (b)
- Study type;
- (c)
- Sample size of study group and of control group;
- (d)
- Gender of participants;
- (e)
- Average age;
- (f)
- Characteristics of malocclusion;
- (g)
- Surgical intervention;
- (h)
- Type of orthodontic fixed appliances;
- (i)
- Force reactivation;
- (j)
- Results.
2.5. Quality Assessment
3. Results
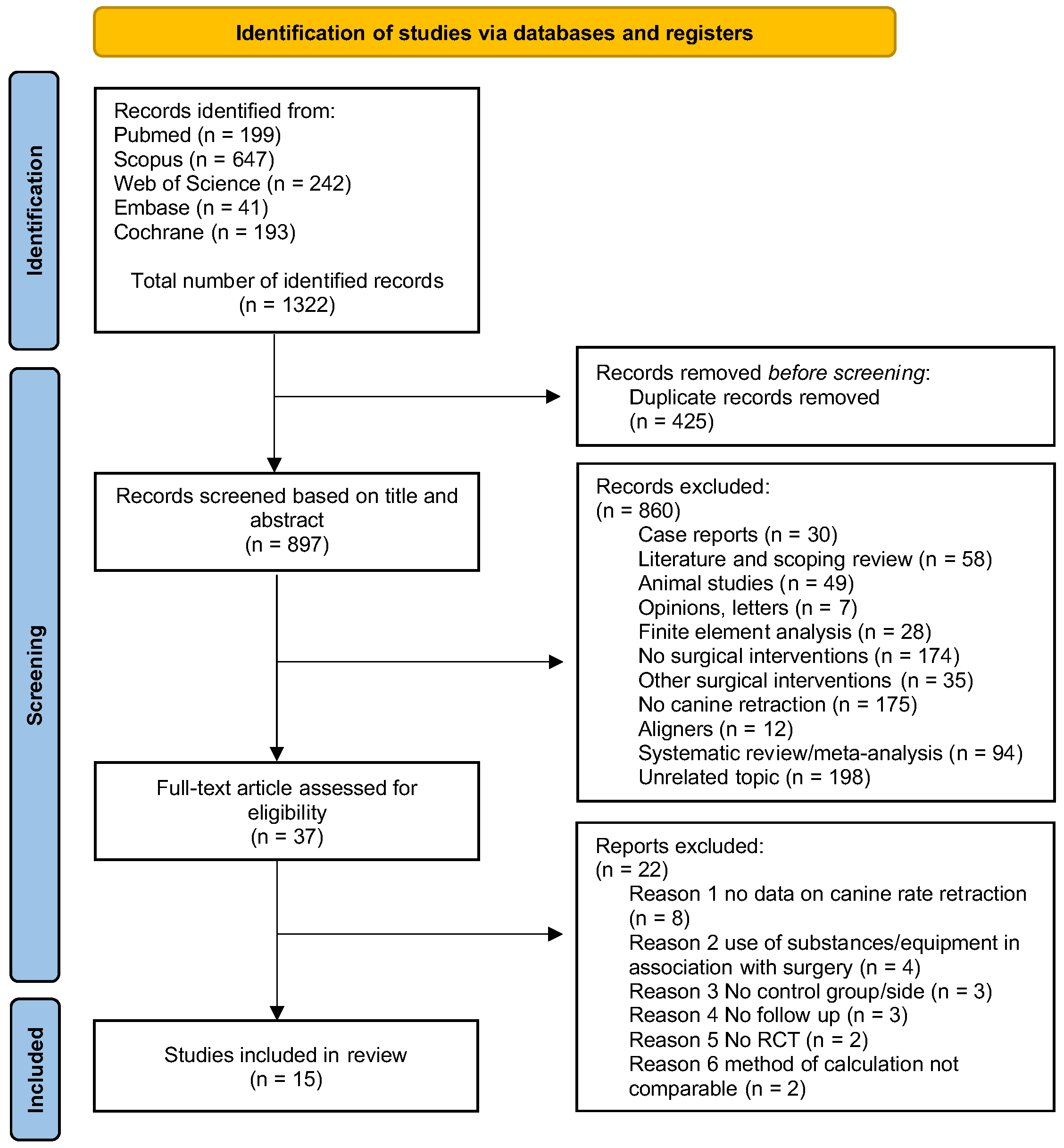
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Surgical Technique
3.2.2. Orthodontic Appliance
3.3. Canine Rate Retraction
3.4. Risk of Bias Assessment
4. Discussion
5. Conclusions
- -
- Corticotomy has been shown to be slightly more effective, with a rate of 1.5 to 4 times higher than conventional therapy.
- -
- Piezocision results in canine retraction that is 1.5 to 2 times faster than conventional treatment.
- -
- The two surgical techniques studied did not show statistically significant adverse effects on the periodontal ligament, molar anchorage loss, or root resorption.
- -
- Patients report experiencing mild to moderate pain, which is nonetheless regarded as tolerable.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giannopoulou, C.; Dudic, A.; Pandis, N.; Kiliaridis, S. Slow and fast orthodontic tooth movement: An experimental study on humans. Eur. J. Orthod. 2016, 38, 404–408. [Google Scholar] [CrossRef]
- Ireland, A.J.; Songra, G.; Clover, M.; Atack, N.E.; Sherriff, M.; Sandy, J.R. Effect of gender and Frankfort mandibular plane angle on orthodontic space closure: A randomized controlled trial. Orthod. Craniofac. Res. 2016, 19, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, F.; Tozlu, M.; Germec-Cakan, D. Cortical bone thickness of the alveolar process measured with cone-beam computed tomography in patients with different facial types. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Chugh, T.; Jain, A.K.; Jaiswal, R.K.; Mehrotra, P.; Mehrotra, R. Bone density and its importance in orthodontics. J. Oral Biol. Craniofac. Res. 2013, 3, 92–97. [Google Scholar] [CrossRef]
- Segal, G.R.; Schiffman, P.H.; Tuncay, O.C. Meta analysis of the treatment-related factors of external apical root resorption. Orthod. Craniofac. Res. 2004, 7, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Moradinejad, M.; Yazdi, M.; Mard, S.A.; Razavi, S.M.; Shamohammadi, M.; Shahsanaei, F.; Rakhshan, V. Efficacy of the systemic co-administration of vitamin D3 in reversing the inhibitory effects of sodium alendronate on orthodontic tooth movement: A preliminary experimental animal study. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e17–e27. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, M.; Shafaee, H.; Saghravania, N.; Peel, S.; Giddon, D.; Sohrabi, K. Effect of corticosteroids on orthodontic tooth movement in a rabbit model. J. Clin. Pediatr. Dent. 2014, 38, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Arias, O.R.; Marquez-Orozco, M.C. Aspirin, acetaminophen, and ibuprofen: Their effects on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Kharat, D.S.; Pulluri, S.K.; Parmar, R.; Choukhe, D.M.; Shaikh, S.; Jakkan, M. Accelerated Canine Retraction by Using Mini Implant With Low-Intensity Laser Therapy. Cureus 2023, 15, e33960. [Google Scholar] [CrossRef]
- Sambevski, J.; Papadopoulou, A.K.; Foley, M.; Dalci, K.; Petocz, P.; Darendeliler, M.A.; Dalci, O. Physical properties of root cementum: Part 29. The effects of LED-mediated photobiomodulation on orthodontically induced root resorption and pain: A pilot split-mouth randomized controlled trial. Eur. J. Orthod. 2022, 44, 650–658. [Google Scholar] [CrossRef]
- Siriphan, N.; Leethanakul, C.; Thongudomporn, U. Effects of two frequencies of vibration on the maxillary canine distalization rate and RANKL and OPG secretion: A randomized controlled trial. Orthod. Craniofac. Res. 2019, 22, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Frost, H.M. The regional acceleratory phenomenon: A review. Henry Ford Hosp. Med. J. 1983, 31, 3–9. [Google Scholar] [PubMed]
- Kole, H. Surgical operations on the alveolar ridge to correct occlusal abnormalities. Oral Surg. Oral Med. Oral Pathol. 1959, 12, 515–529. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.G. Corticision: A Flapless Procedure to Accelerate Tooth Movement. Front. Oral Biol. 2016, 18, 109–117. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, Y.G.; Kang, S.G. Effects of Corticision on paradental remodeling in orthodontic tooth movement. Angle Orthod. 2009, 79, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.A.; Chandhoke, T.; Kalajzic, Z.; Flynn, R.; Utreja, A.; Wadhwa, S.; Nanda, R.; Uribe, F. Effect of corticision and different force magnitudes on orthodontic tooth movement in a rat model. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Dibart, S.; Sebaoun, J.D.; Surmenian, J. Piezocision: A minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend. Contin. Educ. Dent. 2009, 30, 342–350. [Google Scholar]
- Dibart, S. Piezocision™: Accelerating Orthodontic Tooth Movement While Correcting Hard and Soft Tissue Deficiencies. Front. Oral Biol. 2016, 18, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Wazwaz, F.; Seehra, J.; Carpenter, G.H.; Papageorgiou, S.N.; Cobourne, M.T. Duration of canine retraction with fixed appliances: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2023, 163, 154–172. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Abbas, N.H.; Sabet, N.E.; Hassan, I.T. Evaluation of corticotomy-facilitated orthodontics and piezocision in rapid canine retraction. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Ela, S.M.; El-Beialy, A.R.; El-Sayed, K.M.; Selim, E.M.; El-Mangoury, N.H.; Mostafa, Y.A. Miniscrew implant-supported maxillary canine retraction with and without corticotomy-facilitated orthodontics. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 252–259. [Google Scholar] [CrossRef]
- Aksakalli, S.; Calik, B.; Kara, B.; Ezirganli, S. Accelerated tooth movement with piezocision and its periodontal-transversal effects in patients with Class II malocclusion. Angle Orthod. 2016, 86, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Alfawal, A.M.H.; Hajeer, M.Y.; Ajaj, M.A.; Hamadah, O.; Brad, B. Evaluation of piezocision and laser-assisted flapless corticotomy in the acceleration of canine retraction: A randomized controlled trial. Head Face Med. 2018, 14, 4. [Google Scholar] [CrossRef]
- Al-Naoum, F.; Hajeer, M.Y.; Al-Jundi, A. Does alveolar corticotomy accelerate orthodontic tooth movement when retracting upper canines? A split-mouth design randomized controlled trial. J. Oral Maxillofac. Surg. 2014, 72, 1880–1889. [Google Scholar] [CrossRef] [PubMed]
- Alqadasi, B.; Xia, H.Y.; Alhammadi, M.S.; Hasan, H.; Aldhorae, K.; Halboub, E. Three-dimensional assessment of accelerating orthodontic tooth movement-micro-osteoperforations vs. piezocision: A randomized, parallel-group and split-mouth controlled clinical trial. Orthod. Craniofac. Res. 2021, 24, 335–343. [Google Scholar] [CrossRef]
- Bakr, A.R.; Nadim, M.A.; Sedky, Y.W.; El Kady, A.A. Effects of Flapless Laser Corticotomy in Upper and Lower Canine Retraction: A Split-mouth, Randomized Controlled Trial. Cureus 2023, 15, e37191. [Google Scholar] [CrossRef] [PubMed]
- Eid, F.Y.; El-Kalza, A.R. The effect of single versus multiple piezocisions on the rate of canine retraction: A randomized controlled trial. BMC Oral Health 2024, 24, 1024. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, V.M.; Papadopoulou, A.K.; Wong, M.; Pandis, N.; Dalci, O.; Darendeliler, M.A. The effect of piezocision vs. no piezocision on maxillary extraction space closure: A split-mouth, randomized controlled clinical trial. Am. J. Orthod. Dentofac. Orthop. 2022, 16, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Jahanbakhshi, M.R.; Motamedi, A.M.; Feizbakhsh, M.; Mogharehabed, A. The effect of buccal corticotomy on accelerating orthodontic tooth movement of maxillary canine. Dent. Res. J. 2016, 13, 303–308. [Google Scholar] [CrossRef]
- Raj, S.C.; Praharaj, K.; Barik, A.K.; Patnaik, K.; Mahapatra, A.; Mohanty, D.; Katti, N.; Mishra, D.; Panda, S.M. Retraction With and Without Piezocision-Facilitated Orthodontics: A Randomized Controlled Trial. Int. J. Periodontics Restor. Dent. 2020, 40, e19–e26. [Google Scholar] [CrossRef] [PubMed]
- Raza, M.; Sharma, P.; Kumar, P.; Vaish, S.; Pathak, B. Comparison of canine retraction by conventional and corticotomy-facilitated methods: A split mouth clinical study. J. Orthod. Sci. 2021, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Gupta, S.; Ahuja, S.; Bhambri, E.; Sharma, R. Does corticotomy accelerate canine retraction with adequate anchorage control? A split mouth randomized controlled trial. Orthod. Waves 2020, 79, 11–21. [Google Scholar] [CrossRef]
- Toodehzaeim, M.H.; Maybodi, F.R.; Rafiei, E.; Toodehzaeim, P.; Karimi, N. Effect of laser corticotomy on canine retraction rate: A split-mouth randomized clinical trial. BMC Oral Health 2024, 24, 448. [Google Scholar] [CrossRef]
- Alfailany, D.T.; Hajeer, M.Y.; Al-Bitar, M.I.; Alsino, H.I.; Jaber, S.T.; Brad, B.; Darwich, K. Effectiveness of Flapless Cortico-Alveolar Perforations Using Mechanical Drills Versus Traditional Corticotomy on the Retraction of Maxillary Canines in Class II Division 1 Malocclusion: A Three-Arm Randomized Controlled Clinical Trial. Cureus 2023, 15, e44190. [Google Scholar] [CrossRef]
- Ziegler, P.; Ingervall, B. A clinical study of maxillary canine retraction with a retraction spring and with sliding mechanics. Am. J. Orthod. Dentofac. Orthop. 1989, 2, 99–106. [Google Scholar] [CrossRef]
- Benetti, M.; Montresor, L.; Cantarella, D.; Zerman, N.; Spinas, E. Does Miniscrew-Assisted Rapid Palatal Expansion Influence Upper Airway in Adult Patients? A Scoping Review. Dent. J. 2024, 12, 60. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, A.; Suárez-Fernández, C.; Miquel, A.; Bardini, G.; Spinas, E. Biological Effects of Orthodontic Tooth Movement on the Periodontium in Regenerated Bone Defects: A Scoping Review. Dent. J. 2024, 12, 50. [Google Scholar] [CrossRef]
- Lo Russo, L.; Zhurakivska, K.; Montaruli, G.; Salamini, A.; Gallo, C.; Troiano, G.; Ciavarella, D. Effects of crown movement on periodontal biotype: A digital analysis. Odontology 2018, 106, 414–421. [Google Scholar] [CrossRef]
- Tepedino, M.; Esposito, R.; Potrubacz, M.I.; Xhanari, D.; Ciavarella, D. Evaluation of the relationship between incisor torque and profile aesthetics in patients having orthodontic extractions compared to non-extractions. Clin. Oral Investig. 2023, 27, 5233–5248. [Google Scholar] [CrossRef] [PubMed]
- Hatrom, A.A.; Zawawi, K.H.; Al-Ali, R.M.; Sabban, H.M.; Zahid, T.M.; Al-Turki, G.A.; Hassan, A.H. Effect of piezocision corticotomy on en-masse retraction. Angle Orthod. 2020, 90, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Kumar, S.; Hassan, N.; Mazhar, S.; Anjan, R.; Anand, B. Comparison of the Efficiency and Treatment Outcome of Patients Treated with Corticotomy-Assisted En masse Orthodontic Retraction with the En masse Retraction without Corticotomy. J. Pharm. Bioallied Sci. 2021, 13, S1320–S1323. [Google Scholar] [CrossRef]
- Mousa, M.R.; Hajeer, M.Y.; Burhan, A.S.; Heshmeh, O.; Alam, M.K. The effectiveness of minimally-invasive corticotomy-assisted orthodontic treatment of palatally impacted canines compared to the traditional traction method in terms of treatment duration, velocity of traction movement and the associated dentoalveolar changes: A randomized controlled trial. F1000Research 2023, 12, 699. [Google Scholar] [CrossRef]
- Ma, Z.; Xu, G.; Yang, C.; Xie, Q.; Shen, Y.; Zhang, S. Efficacy of the technique of piezoelectric corticotomy for orthodontic traction of impacted mandibular third molars. Br. J. Oral Maxillofac. Surg. 2015, 53, 326–331. [Google Scholar] [CrossRef]
- Al-Areqi, M.M.; Abu Alhaija, E.S.; Al-Maaitah, E.F. Effect of piezocision on mandibular second molar protraction. Angle Orthod. 2020, 3, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Alhaija, E.S.A.; Al-Areqi, M.M.; Maaitah, E.F.A. Comparison of second molar protraction using different timing for piezocision application: A randomized clinical trial. Dent. Press J. Orthod. 2022, 4, e2220503. [Google Scholar] [CrossRef]
- Patterson, B.M.; Dalci, O.; Darendeliler, M.A.; Papadopoulou, A.K. Corticotomies and Orthodontic Tooth Movement: A Systematic Review. J. Oral. Maxillofac. Surg. 2016, 3, 453–473. [Google Scholar] [CrossRef]
- Han, S.H.; Park, W.J.; Park, J.B. Comparative Efficacy of Traditional Corticotomy and Flapless Piezotomy in Facilitating Orthodontic Tooth Movement: A Systematic Review and Meta-Analysis. Medicina 2023, 10, 1804. [Google Scholar] [CrossRef]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Participant | Orthodontic permanent dentition patients requiring first premolar extraction and consequent maxillary canine retraction | Patients with periodontal disease or any disorders/therapies that might have affected bone turnover or density, systematic diseases, previous orthodontic treatment, no first premolar extraction |
| Intervention | Fixed orthodontic appliance with corticotomy and/or piezocision procedures | Orthognathic surgery, osteogenic distraction, no surgical procedures |
| Comparison | Fixed orthodontics appliance only | Aligners or any removable appliances |
| Outcome | Duration of treatment, speed, and/or rate of tooth movement | / |
| Study design | RCTs 1 | Case-control, cohort, cross-sectional, Nr-RCTs 2; reviews; case reports; case series; in vitro; and animal studies |
| Database | Search Strategy |
|---|---|
| PubMed | (((((((((((((corticotomy) OR (piezocision)) OR (piezosurg*)) OR (corticotomy facilitated orthod*)) OR (regional acceleratory phenomenon)) OR (periodontally accelerated osteogenic orthod*)) OR (piezotomy)) OR (piezopuncture)) OR (corticision)) OR (Wilckodontics)) AND (tooth movement)) OR (rate tooth movement)) AND (canine retraction)) AND (orthodontic*) |
| Scopus | (ALL (corticotomy) OR ALL (piezocision) OR ALL (piezosurgery) OR ALL (corticotomy AND facilitated AND orthod*) OR ALL (regional AND acceleratory AND phenomenon) OR ALL (periodontally AND accelerated AND osteogenic AND orthod*) OR ALL (piezotomy) OR ALL (piezopuncture) OR ALL (corticision) OR ALL (wilckodontics) AND ALL (tooth AND movement) OR ALL (rate AND tooth AND movement) AND ALL (canine AND retraction) AND ALL (orthodontics)) |
| Web of Science | (((((((((((((ALL = (corticotomy)) OR ALL = (piezocision)) OR ALL = (piezosurg*)) OR ALL = (corticotomy facilitated orthod*)) OR ALL = (regional acceleratory phenomenon)) OR ALL = (periodontally accelerated osteogenic orthod*)) OR ALL = (piezotomy)) OR ALL = (piezopuncture)) OR ALL = (corticision)) OR ALL = (Wilckodontics)) AND ALL = (tooth movement)) OR ALL = (rate tooth movement)) AND ALL = (canine retraction)) AND ALL = (orthodontic*) |
| Embase | ((‘corticotomy’/exp OR ‘corticotomy’ OR ‘piezocision’/exp OR ‘piezocision’ OR ‘piezosurgery’/exp OR ‘piezosurgery’ OR ‘corticotomy facilitated orthod* ’ OR ‘regional acceleratory phenomenon’ OR ‘periodontally accelerated osteogenic orthodontics’/exp OR ‘periodontally accelerated osteogenic orthodontics’ OR ‘piezotome’/exp OR ‘piezotome’ OR ‘piezopuncture’ OR ‘corticision’ OR ‘wilckodontics’) AND (‘tooth movement’/exp OR ‘tooth movement’) OR ‘ate tooth movement’) AND (‘canine retraction’/exp OR ‘canine retraction’) AND (‘orthodontics’/exp OR ‘orthodontics’)\ |
| Cochrane Central Register of Controlled Trials | corticotomy in All Text OR piezocision in All Text AND rate tooth movement in All Text AND canine retraction in All Text AND orthodontic in All Text |
| Authors and Year | Type of Article | Intervention | Participants | Mean Age (Year) | Initial Malocclusion | Orthodontic Fixed Appliance | Force Reactivation | Primary Outcome | Secondary Outcome | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|
| Abbas et al. (2016) [23] | RCT, split-mouth design | C, P | 20 patients (gender N/A) 10 C 10 P | 15 to 25 | Class II\1 | 0.016 × 0.022 SSW (SW Roth) NiTi CLS (150 gr) | Every 2 weeks | CR is 1.5 to 2 times faster on C-side than CG-side. CR is 1.5 times faster on P-side than CG-side. | - MAL: no differences (p > 0.05) - PD: N/A - PH: no differences (p > 0.05) - RS: CG- side exhibit a greater canine root resorption than C- and P-side | 3 months |
| Aboul-Ela et al. (2011) [24] | RCT, split-mouth design | C | 13 patients (5 M, 8 F) | 19 | Class II\1 | 0.016 × 0.022 SSW NiTi CLS (150 gr) from miniscrew (U6–U7) | Every 4 weeks | CR is 2 times faster on C-side than CG-side in the first 2 months, declining to 1.6 the 3rd month, and 1.06 by the end of the 4th month. | - MAL: no differences (p > 0.05) - PD: N/A - PH: no differences (p > 0.05), except for the gingival index higher (p < 0.05) CG-side - RS: N/A | 4 months |
| Aksakalli et al. (2016) [25] | RCT, split-mouth design | P | 10 patients (4 M, 6 F) | 16.3 ± 2.4 | Class II | 0.016 × 0.022 SSW (SW Roth) Elastomeric chains (150 gr) | Every 2 weeks | CR is 2 times faster on P-side than CG-side. | - MAL: lesser in P-side. - PD: N/A - PH: no differences (p > 0.05) - RS: N/A | 3.5 months |
| Alfailany et al. (2023) [37] | RCT, single-blinded, single-center | C | 34 patients (13M, 21 F) CTG: 17 (6M,11F) CG: 17(7M, 10 F) | 20.98 ± 1.95 CTG: 21.23 ± 2.33 CG: 20.62 ± 1.48 | Class II\1 | 0.019 × 0.025 SSW (SW MBT) NiTi CLS (150 gr) Transpalatal arch | Every 2 weeks | CR is significantly faster in CTG than CG until the end of the 2nd month. | - MAL: CTG showed less MAL than CG - PD: N/A - PH: N/A - RS: N/A | 4 months |
| Alfawal et al. (2018) [26] | RCT, split-mouth design | C, P | 36 patients (24M, 12 F) 18 C 18 P | 18.08 ± 3.5C | Class II\1 | 0.019 × 0.025 SSW (SW MBT) NiTi CLS (150 gr) Transpalatal arch | Every 2 weeks | CR was significantly higher on the C- and P-side than CG-side during the first 2 months. | - MAL: no differences (p > 0.05) - PD: N/A - PH: N/A - RS: N/A | 4 months |
| Al-Naoum et al. (2014) [27] | RCT, split-mouth design | C | 30 patients (15 M, 15 F) | 20.04 ± 3.63 | Class II\1 and 2 | 0.019 × 0.025 SSW (SW MBT) NiTi CLS (120 gr) Transpalatal arch | Every 2 weeks | CR is 4 times faster on C-side than CG-side at 0–2 wks, is 3 times faster at 4 and 12 wks. | - MAL: N/A - PD: >50% of the sample had moderate to severe discomfort on the surgical side - PH: N/A - RS: N/A | 3 months |
| Alqadasi et al. (2021) [28] | RCT, split-mouth design | P | 11 patients (5 M, 6 F) | 20.89 ± 4.46 | Class II\1 | 0.018 × 0.025 SSW (SW MBT) NiTi CLS (150 gr) from miniscrew (U5-U6) | Every 28 days | CR on P-side was significantly faster than CG-side until the end of the 2nd month. | - MAL: N/A - PD: N/A - PH: N/A - RS: no differences (p > 0.05) | 3 months |
| Bakr et al. (2023) [29] | RCT, split-mouth design | C | 14 patients (2 M, 12 F) | 20.4 ± 2.5 | Class I biprotrusion | 0.017 × 0.025 SSW (SW MBT) NiTi CLS (150 gr) from miniscrew (U5-U6) | Every 2 weeks | No significant difference in the CR between the C-side and CG-side. | - MAL: no differences (p > 0.05) - PD: N/A - PH: no differences (p > 0.05) - RS: no differences (p > 0.05) | 3 months |
| Eid et al. (2024) [30] | RCT, split-mouth design | P | 30 patients (16 M, 14 F) SP 15 (9 M, 6 F) MP 15(7 M, 8 F) | 15 to 25 SP 17.33 ± 1.88 MP 17.40 ± 1.92 | Class I biprotrusion, Class II\1 | 0.016 × 0.022 SSW (SW Roth) Nitin CLS (150 gr) from miniscrew (U5-U6) | Every 4 weeks | CR registered a significant increase in SG- and MGP-side than CG-side. Non-significant differences have been observed between SP and MP (p > 0.05). | - MAL: N/A - PD: N/A - PH: N/A - RS: higher root resorption risk accompanies both SP- and MP-side than CG-side. | 3 months |
| Hawkins et al. (2022) [31] | RCT, split-mouth design | P | 20 patients (8 M, 12 F) | 18.7 ± 1.12 | N/A | 0.020 SSW (selfligating), NiTi CLS (250 gr) Nance Transpalatal arch | Every 6 weeks | No statistically significant differences in CR between P-side and CG-side. | - MAL: no differences (p > 0.05) - PD: all patients except for one, had minimal pain - PH: N/A - RS: N/A | 4,5 months |
| Jahanbakhshi et al. (2016) [32] | RCT, split-mouth design | C | 15 patients (15 F) | 25 | N/A | 0.016 × 0.016 SSW Open loop (200 gr) Miniscrew (U6-U7) | Every 2 weeks | CR is faster on C-side than CG-side (Averages of 1.8 mm/month vs. 1.1 mm/month) | - MAL: N/A - PD: N/A - PH: N/A - RS: N/A | 4 months |
| Raj et al. (2020) [33] | RCT, split-mouth design | P | 20 patients (6 M, 14 F) | 23.18 ± 1.41 | Class II\1 | 0.016 × 0.022 SSW, NiTi CLS (150 gr) Transpalatal arch | Every 2 weeks | The rate of CR is higher on P-side at all time intervals (p < 0.001). | - MAL: N/A - PD: N/A - PH: no differences (p > 0.05) - RS: no differences (p > 0.05) | 7 months |
| Raza et al. (2021) [34] | RCT, split-mouth design | C | 10 patients (N/A) | 18 to 25 | N/A | 0.018 SSW SSW (SW MBT) NiTi CLS (150 gr) Nance Transpalatal arch | Every 4 weeks | There was an overall reduction in the time taken for canine retraction on C-side (5.7 mo) than CG-side (7.1 mo). | - MAL: N/A - PD: was more in C-side than CG- side at 24 h, but similar after one week. - PH: N/A - RS: CG-side exhibit a greater canine root resorption than C-side | 8 months |
| Sharma et al. (2020) [35] | RCT, split-mouth design | C | 16 patients (4 M, 12 F) | 14 to 25 | Class I biprotrusion, Class II\1 | 0.016 × 0.022 SSW (SW MBT) NiTi CLS (150 gr) From miniscrew (U5-U6) | Every 3 weeks | CR on C-side is significantly greater than CG-side for the initial 2 months. | - MAL: no differences (p > 0.05) - PD: mild to moderate pain, discomfort—PH: no differences (p > 0.05) and swelling in C-side. - RS: N/A | 6 months |
| Toodehzaeim et al. (2024) [36] | RCT, split-mouth design | C | 12 patients (5M, 7F) | 15 to 30 | Class I biprotrusion Class II\1 | 0.019 × 0.025 SSW (SW MBT) NiTi CLS (150 gr) Transpalatal arch | Every 2 weeks | CR was significantly greater on the C-side than CG-side (p < 0.05). | - MAL: no differences (p > 0.05) - PD: no differences (p > 0.05) - PH: no differences (p > 0.05) - RS: N/A | 4 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipani, E.; Pisani, E.; Verrone, M.; Bitonto, F.; Verdecchia, A.; Spinas, E. Evaluation of the Efficacy of Corticotomy and Piezocision on Canine Retraction: A Systematic Review. Dent. J. 2025, 13, 57. https://doi.org/10.3390/dj13020057
Lipani E, Pisani E, Verrone M, Bitonto F, Verdecchia A, Spinas E. Evaluation of the Efficacy of Corticotomy and Piezocision on Canine Retraction: A Systematic Review. Dentistry Journal. 2025; 13(2):57. https://doi.org/10.3390/dj13020057
Chicago/Turabian StyleLipani, Erica, Elisa Pisani, Mariagrazia Verrone, Federica Bitonto, Alessio Verdecchia, and Enrico Spinas. 2025. "Evaluation of the Efficacy of Corticotomy and Piezocision on Canine Retraction: A Systematic Review" Dentistry Journal 13, no. 2: 57. https://doi.org/10.3390/dj13020057
APA StyleLipani, E., Pisani, E., Verrone, M., Bitonto, F., Verdecchia, A., & Spinas, E. (2025). Evaluation of the Efficacy of Corticotomy and Piezocision on Canine Retraction: A Systematic Review. Dentistry Journal, 13(2), 57. https://doi.org/10.3390/dj13020057