
Endocrine Mucin-Producing Sweat Gland Carcinoma: Case Presentation with a Comprehensive Review of the Literature

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
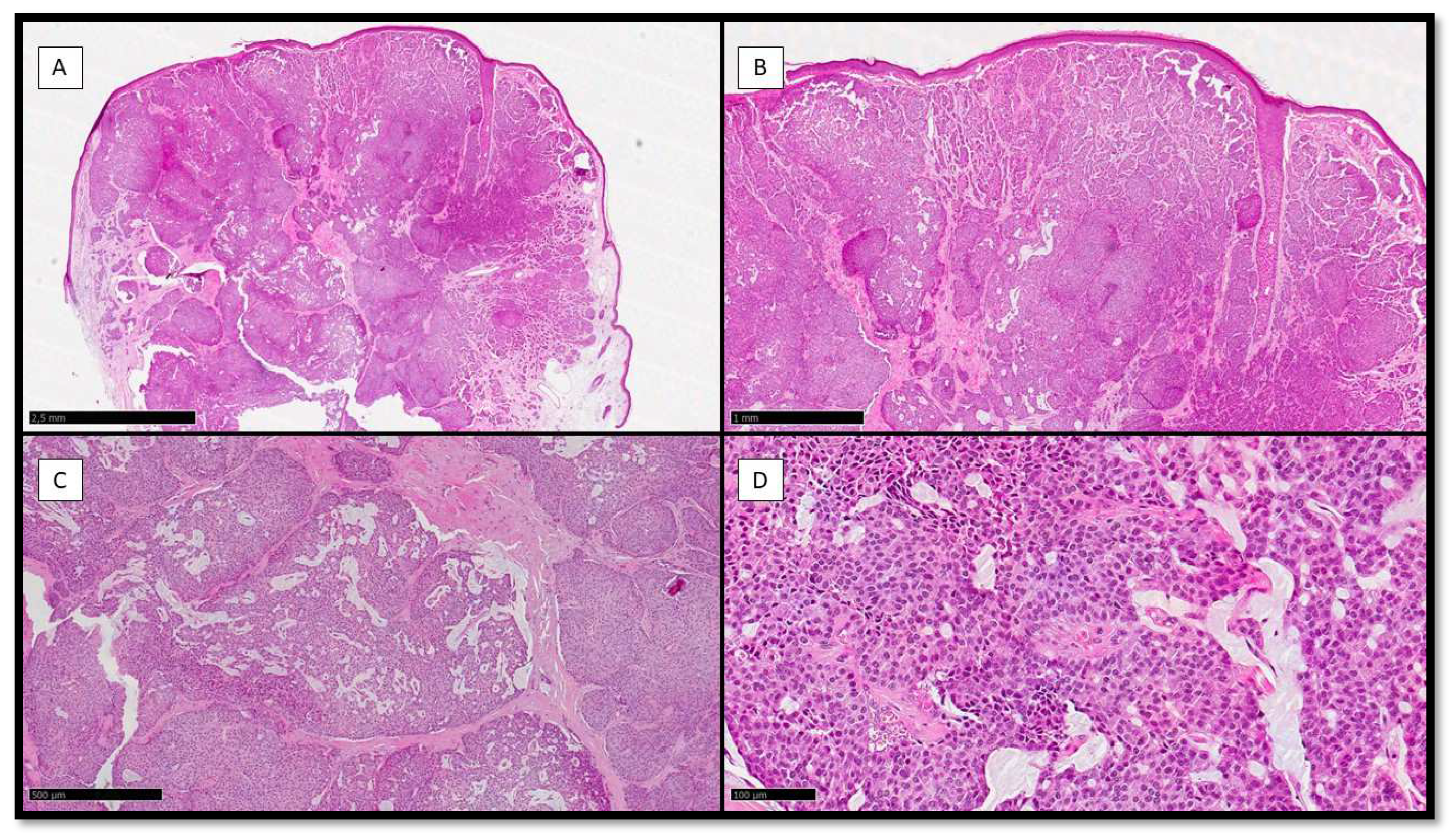
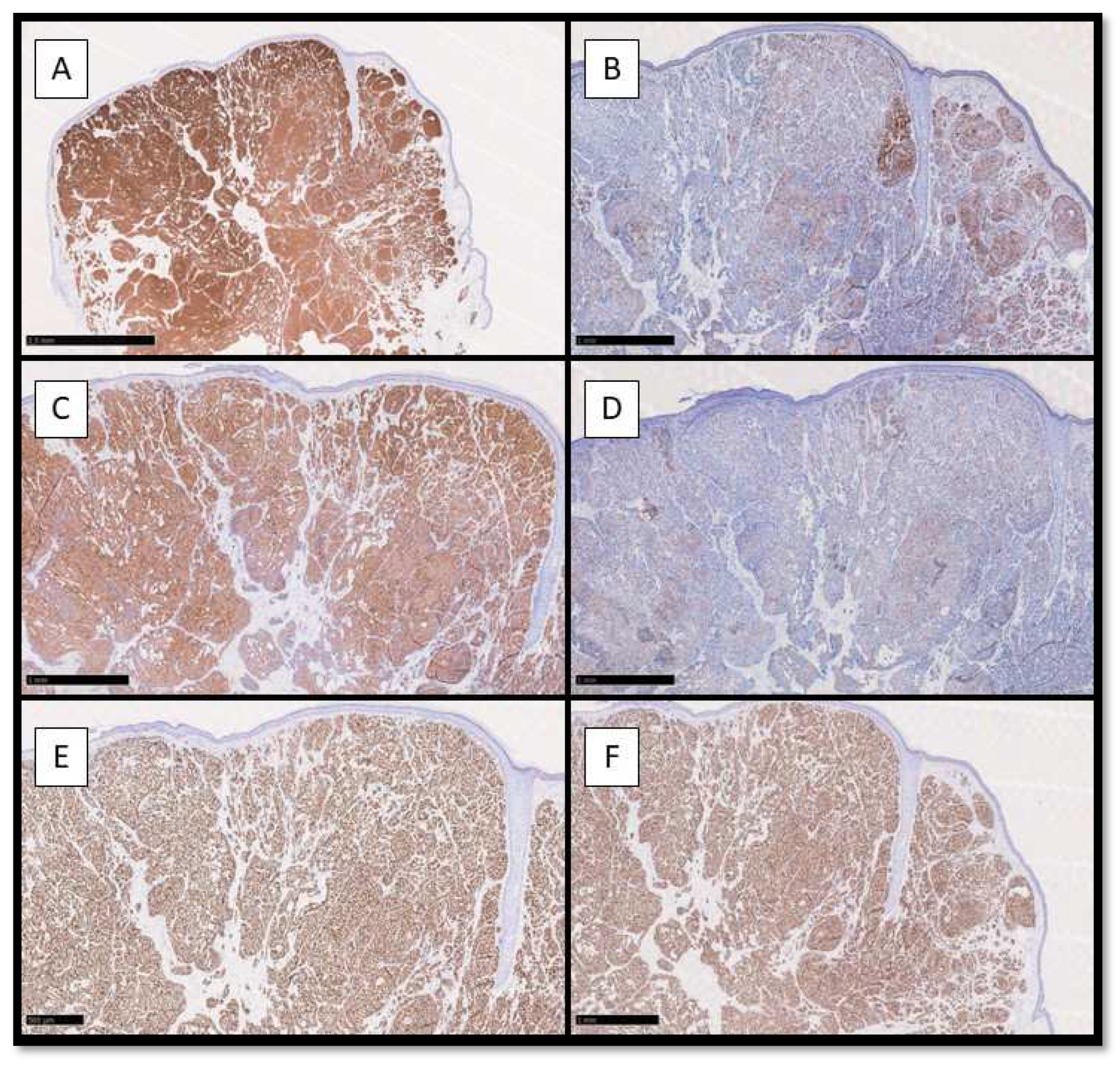
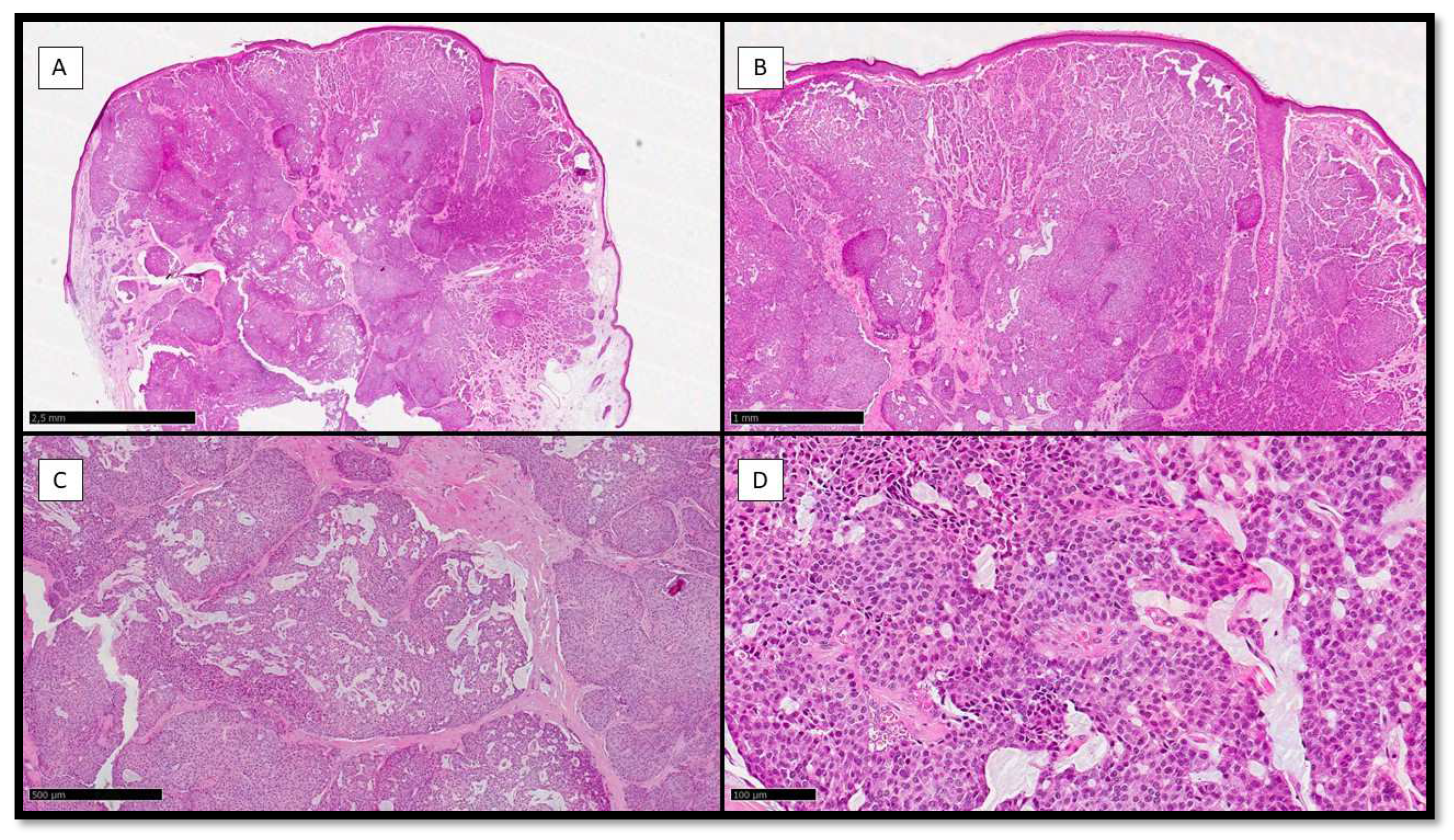
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flieder, A.; Koerner, F.C.; Pilch, B.Z.; Maluf, H.M. Endocrine mucin-producing sweat gland carcinoma: A cutaneous neoplasm analogous to solid papillary carcinoma of breast. Am. J. Surg. Pathol. 1997, 21, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Elder, D.; Massi, D.; Scolyer, A.; Willemze, R. WHO Classification of Skin Tumours; IARC: Lyon, France, 2018; pp. 168–169. [Google Scholar]
- Requena, L.; Sangueza, O. Cutaneous Adnexal Neoplasms; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Tsai, J.H.; Hsiao, T.L.; Chen, Y.Y.; Hsiao, C.H.; Liau, J.Y. Endocrine mucin-producing sweat gland carcinoma occurring on extra-facial site: A case report. J. Cutan. Pathol. 2014, 41, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Tannous, Z.S.; Avram, M.M.; Zembowicz, A.; Mihm, M.C.; Liteplo, M.; Kwan, T.; Olbricht, S.M. Treatment of synchronous mucinous carcinoma and endocrine mucin-producing sweat gland carcinoma with Mohs’ micrographic surgery. Dermatol. Surg. 2005, 31, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Zembowicz, A.; Garcia, C.F.; Tannous, Z.S.; Mihm, M.C.; Koerner, F.; Pilch, B.Z. Endocrine mucin-producing sweat gland carcinoma: Twelve new cases suggest that it is a precursor of some invasive mucinous carcinomas. Am. J. Surg. Pathol. 2005, 29, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Froehlich, M.H.; Conti, K.R.; Norris, I.I.; Allensworth, J.J.; Ufkes, N.A.; Nguyen, S.A.; Bruner, E.T.; Cook, J.; Day, T.A. Endocrine mucin-producing sweat gland carcinoma: A systematic review and meta-analysis. J. Dermatol. Treat. 2022, 33, 2182–2191. [Google Scholar] [CrossRef]
- Held, L.; Ruetten, A.; Kutzner, H.; Palmedo, G.; John, R.; Mentzel, T. Endocrine mucin-producing sweat gland carcinoma: Clinicopathologic, immunohistochemical, and molecular analysis of 11 cases with emphasis on MYB immunoexpression. J. Cutan. Pathol. 2018, 45, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Parra, O.; Linos, K.; Yan, S.; Lilo, M.; LeBlanc, R.E. Comparative performance of insulinoma-associated protein 1 (INSM1) and routine immunohistochemical markers of neuroendocrine differentiation in the diagnosis of endocrine mucin-producing sweat gland carcinoma. J. Cutan. Pathol. 2021, 48, 41–46. [Google Scholar] [CrossRef]
- Mathew, J.G.; Bowman, A.S.; Saab, J.; Busam, K.J.; Nehal, K.; Pulitzer, M. Next-generation sequencing analysis suggests varied multistep mutational pathogenesis for endocrine mucin-producing sweat gland carcinoma with comments on INSM1 and MUC2 suggesting a conjunctival origin. J. Am. Acad. Dermatol. 2022, 86, 1072–1079. [Google Scholar] [CrossRef]
- Bulliard, C.; Murali, R.; Maloof, A.; Adams, S. Endocrine mucin-producing sweat gland carcinoma: Report of a case and review of the literature. J. Cutan. Pathol. 2006, 33, 812–816. [Google Scholar] [CrossRef]
- Emanuel, P.O.; de Vinck, D.; Waldorf, H.A.; Phelps, R.G. Recurrent endocrine mucin-producing sweat gland carcinoma. Ann. Diagn. Pathol. 2007, 11, 448–452. [Google Scholar] [CrossRef]
- Mehta, S.; Thiagalinga, S.; Zembowicz, A.; Hatton, M.P. Endocrine mucin-producing sweat gland carcinoma of the eyelid. Ophthalmic. Plast. Reconstr. Surg. 2008, 24, 164–165. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.; Shim, S.H.; Joo, M.; Kim, H.; Kim, Y.K. A Case of Endocrine Mucin-Producing Sweat. Gland Carcinoma Co-existing with Mucinous Carcinoma: A Case Report. J. Pathol. Transl. Med. 2010, 44, 97–100. [Google Scholar] [CrossRef]
- Inozume, T.; Kawasaki, T.; Harada, K.; Tanaka, K.; Kawamura, T.; Shibagaki, N.; Katoh, R.; Shimada, S. A case of endocrine mucin-producing sweat gland carcinoma. Pathol. Int. 2012, 62, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Salim, A.A.; Karim, R.Z.; McCarthy, S.W.; Scolyer, R.A. Endocrine mucin producing sweat gland carcinoma: A clinicopathological analysis of three cases. Pathology 2012, 44, 568–571. [Google Scholar] [CrossRef]
- Koike, T.; Mikami, T.; Maegawa, J.; Iwai, T.; Wada, H.; Yamanaka, S. Recurrent endocrine mucin-producing sweat gland carcinoma in the eyelid. Australas. J. Dermatol. 2013, 54, e46–e49. [Google Scholar] [CrossRef]
- Dhaliwal, C.A.; Torgersen, A.; Ross, J.J.; Ironside, J.W.; Biswas, A. Endocrine mucin-producing sweat gland carcinoma: Report of two cases of an under-recognized malignant neoplasm and review of the literature. Am. J. Dermatopathol. 2013, 35, 117–124. [Google Scholar] [CrossRef]
- Hoguet, A.; Warrow, D.; Milite, J.; McCormick, S.A.; Maher, E.; Della Rocca, R.; Della Rocca, D.; Goldbaum, A.; Milman, T. Mucin-producing sweat gland carcinoma of the eyelid: Diagnostic and prognostic considerations. Am. J. Ophthalmol. 2013, 155, 585–592.e2. [Google Scholar] [CrossRef]
- Shimizu, I.; Dufresne, R.; Robinson-Bostom, L. Endocrine mucin-producing sweat gland carcinoma. Cutis 2014, 93, 47–49. [Google Scholar]
- Shon, W.; Salomão, D.R. WT1 expression in endocrine mucin-producing sweat gland carcinoma: A study of 13 cases. Int. J. Dermatol. 2014, 53, 1228–1234. [Google Scholar] [CrossRef]
- Collinson, A.C.; Sun, M.T.; James, C.; Huilgol, S.C.; Selva, D. Endocrine mucin-producing sweat gland carcinoma of the eyelid. Int. Ophthalmol. 2015, 35, 883–886. [Google Scholar] [CrossRef]
- Fernandez-Flores, A.; Cassarino, D.S. Endocrine mucin-producing sweat gland carcinoma: A study of three cases and CK8, CK18 and CD5/6 immunoexpression. J. Cutan. Pathol. 2015, 42, 578–586. [Google Scholar] [CrossRef]
- Jedrych, J.; Jones, M.; Seethala, R.; Ho, J. Primary cutaneous endocrine mucin-producing sweat gland carcinoma co-occurring simultaneously with low-grade ductal mucinous breast cancer: A clinicopathologic conundrum. Am. J. Dermatopathol. 2015, 37, 425–427. [Google Scholar] [CrossRef]
- Turnbull, L.I.; Puchalsky, D.R.; Xu, Y.G.; Bennett, D.D. A cystic growth on the lower eyelid: A presentation of two cases. Int. J. Dermatol. 2015, 54, 737–739. [Google Scholar] [CrossRef] [PubMed]
- Bamberger, M.; Medline, P.; Cullen, J.B.; Gill, H. Histopathology of endocrine mucin-producing sweat gland carcinoma of the eyelid. Can. J. Ophthalmol. 2016, 51, e72–e75. [Google Scholar] [CrossRef] [PubMed]
- Cornejo, K.M.; Hutchinson, L.; Meng, X.; O’Donnell, P.; Deng, A. Endocrine Mucin-Producing Sweat Gland Carcinoma of the Eyelid: A Report of a Case with Molecular Analysis. Am. J. Dermatopathol. 2016, 38, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Abdulkader, M.; Kuhar, M.; Hattab, E.; Linos, K. GATA3 Positivity in Endocrine Mucin-Producing Sweat Gland Carcinoma and Invasive Mucinous Carcinoma of the Eyelid: Report of 2 Cases. Am. J. Dermatopathol. 2016, 38, 789–791. [Google Scholar] [CrossRef]
- Ross, A.G.; Chan, A.A.; Mihm, M.C., Jr.; Yu, J.Y. Endocrine Mucin-Producing Sweat Gland Carcinoma: An Uncommon Presentation. Semin. Ophthalmol. 2017, 32, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Brett, M.A.; Salama, S.; Gohla, G.; Alowami, S. Endocrine Mucin-Producing Sweat Gland Carcinoma, a Histological Challenge. Case Rep. Pathol. 2017, 2017, 6343709. [Google Scholar] [CrossRef]
- Scott, B.L.; Anyanwu, C.O.; Vandergriff, T.; Nijhawan, R.I. Endocrine Mucin-Producing Sweat Gland Carcinoma Treated With Mohs Micrographic Surgery. Dermatol. Surg. 2017, 43, 1498–1500. [Google Scholar] [CrossRef]
- Chou, Y.H.; Chang, Y.C.; Huang, Y.L.; Wu, C.T. Endocrine mucin-producing sweat gland carcinoma with GATA3 expression: Report of two cases. Pathology 2017, 49, 805–808. [Google Scholar] [CrossRef]
- Charles, N.C.; Proia, A.D.; Lo, C. Endocrine Mucin-Producing Sweat Gland Carcinoma of the Eyelid Associated With Mucinous Adenocarcinoma. Ophthalmic Plast. Reconstr. Surg. 2018, 34, e37–e38. [Google Scholar] [CrossRef]
- Qin, H.; Moore, R.F.; Ho, C.Y.; Eshleman, J.; Eberhart, C.G.; Cuda, J. Endocrine mucin-producing sweat gland carcinoma: A study of 11 cases with molecular analysis. J. Cutan. Pathol. 2018, 45, 681–687. [Google Scholar] [CrossRef]
- Hasegawa-Murakami, Y.; Kono, M.; Yokota, K.; Inaba, H.; Fukumoto, T.; Akiyama, M. Dermoscopic features of endocrine mucin-producing sweat gland carcinoma. J. Dermatol. 2018, 45, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.G.; Bhargava, R.; Furniturewala, A.U. Endocrine mucin-producing sweat gland carcinoma of the eyelid: A clinical and histological conundrum. Indian J. Ophthalmol. 2018, 66, 1042–1044. [Google Scholar] [CrossRef] [PubMed]
- Navrazhina, K.; Petukhova, T.; Wildman, H.F.; Magro, C.M.; Minkis, K. Endocrine mucin-producing sweat gland carcinoma of the scalp treated with Mohs micrographic surgery. JAAD Case Rep. 2018, 4, 887–889. [Google Scholar] [CrossRef]
- Kawasaki, T.; Kubota, T.; Ichihara, S.; Horibe, K.; Hasebe, T. Neuroendocrine cells associated with endocrine mucin-producing sweat gland carcinoma: A potential precursor lesion? Pathology 2018, 50, 573–575. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Wang, S.-H.; Chang, Y.-J. Endocrine mucin-producing sweat gland carcinoma: Report of two cases. Dermatol. Sin. 2018, 36, 262–263. [Google Scholar] [CrossRef]
- Mulay, K.; Menon, V.; Lahane, S.; Sharma, M.; Honavar, S.G. Endocrine mucin-producing sweat gland carcinoma (EMPSGC) of the eyelid: Clinicopathologic features, immunohistochemical findings and review of literature. Indian J. Ophthalmol. 2019, 67, 1374–1377. [Google Scholar] [CrossRef]
- Meltzer, O.A.; Joseph, J.M. Delayed treatment of endocrine mucin-producing sweat gland carcinoma initially diagnosed as a chalazion. JAAD Case Rep. 2019, 5, 789–791. [Google Scholar] [CrossRef]
- Ansari, A.N.; Bobos, M.; Shih, S.; Chen, M.C.; Ardakani, N.M.; Rosales, C.M.; Chen, C.J.; Savage, C.; Bracey, T.; McKee, P.H.; et al. Renal Cell Carcinoma Antigen Expression in Primary Cutaneous Endocrine Mucinous Carcinomas: A Case Series of 14 Patients and Review of the Literature. Am. J. Dermatopathol. 2019, 41, 571–577. [Google Scholar] [CrossRef]
- Nathan, N.R.; Emerick, K.S.; Hoang, M.P.; Smith, G.P.; Yancovitz, M. Perineural and Vascular Invasion in an Endocrine Mucin-Producing Sweat Gland Carcinoma of the Ear with Associated Mucinous Carcinoma. Dermatopathology 2020, 6, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Nasser, H.; Siddiqui, S. Endocrine Mucin-Producing Sweat Gland Carcinoma: Two New Eyelid Cases and Review of the Literature. Int. J. Surg. Pathol. 2020, 28, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Murshed, K.A.; Ben-Gashir, M. A Case of Endocrine Mucin-Producing Sweat Gland Carcinoma: Is it Still an Under-Recognized Entity? Case Rep. Dermatol. 2020, 12, 255–261. [Google Scholar] [CrossRef]
- Bakrin, I.H.; Rajaintharan, P.S.; Tawil, Z.; Mahayidin, H. Endocrine mucin-producing sweat gland carcinoma—Newly described skin appendageal tumours. Malays. J. Pathol. 2020, 42, 111–114. [Google Scholar]
- Shah, S.; Parekh, P.; Rodriguez, M. Endocrine Mucin-Producing Sweat Gland Carcinoma in an Elderly Man. Am. J. Dermatopathol. 2020, 42, 153–155. [Google Scholar] [CrossRef]
- Agni, M.; Raven, M.L.D.; Bowen, R.C.; Laver, N.V.; Chevez-Barrios, P.; Milman, T.; Eberhart, C.G.; Couch, S.; Bennett, D.D.; Albert, D.M.; et al. An Update on Endocrine Mucin-producing Sweat Gland Carcinoma: Clinicopathologic Study of 63 Cases and Comparative Analysis. Am. J. Surg. Pathol. 2020, 44, 1005–1016. [Google Scholar] [CrossRef]
- Froehlich, M.; Cook, J.; Bruner, E.; Stalcup, S.; Patel, K.; Day, T. Endocrine Mucin-Producing Sweat Gland Carcinoma of the Eyelid with Locoregional Metastasis to the Parotid Gland. Dermatol. Surg. 2020, 46, 1116–1118. [Google Scholar] [CrossRef]
- Nakamura, M.; Sakurai, M.; Ozawa, H.; Morita, A. Four male cases of endocrine mucin-producing sweat gland carcinoma: Specific gender differences in East Asia. Kaohsiung J. Med. Sci. 2020, 36, 467–468. [Google Scholar] [CrossRef] [PubMed]
- Katsura, Y.; Sasaki, A.; Minagawa, D.; Kato, I.; Ueda, T. Endocrine mucin-producing sweat gland carcinoma of the cheek. Dermatol. Online J. 2021, 27. [Google Scholar] [CrossRef]
- Hadi, R.; Xu, H.; Barber, B.R.; Shinohara, M.M.; Moshiri, A.S. A case of endocrine mucin-producing sweat gland carcinoma with distant metastasis. J. Cutan. Pathol. 2021, 48, 937–942. [Google Scholar] [CrossRef]
- Nishimoto, A.; Kuwahara, H.; Ohashi, R.; Ansai, S.I. Multicentric endocrine mucin-producing sweat gland carcinoma and mucinous carcinoma of the skin: A case report. J. Cutan. Pathol. 2021, 48, 165–170. [Google Scholar] [CrossRef]
- Shah, M.; Aman, A.; Srinivaas, K.; Gudipati, A.; Chavali, P. Endocrine mucin-producing sweat gland carcinoma of the peno-scrotum with systemic metastases: A rare case report. Indian J. Pathol. Microbiol. 2021, 64, 180–182. [Google Scholar] [CrossRef] [PubMed]
- Homer, N.A.; Hoesly, P.M.; Durairaj, V.D. Atypical presentation of an endocrine mucin-producing sweat gland carcinoma of the eyelid. Orbit 2021, 40, 81–82. [Google Scholar] [CrossRef] [PubMed]
- Schafer, C.N.; Hurst, E.A.; Rosman, I.S.; Council, M.L. Endocrine Mucin-Producing Sweat Gland Carcinoma Treated with Mohs Micrographic Surgery. Dermatol. Surg. 2022, 48, 362–364. [Google Scholar] [CrossRef]
- Chuang, I.C.; Jang, C.S. Endocrine mucin-producing sweat gland carcinoma: Reappraisal of patient demographics and tumour immunophenotypes. Indian J. Dermatol. Venereol. Leprol. 2022, 88, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Ravi, P.Y.; Walsh, N.M.; Archibald, C.; Pasternak, S. Endocrine Mucin-Producing Sweat Gland Carcinoma: Emerging Evidence of Multicentric Cutaneous Origin and Occasional Concurrence with Analogous Breast Tumors. Am. J. Dermatopathol. 2022, 44, 321–326. [Google Scholar] [CrossRef]
- Sarangi, J.; Konkimalla, A.; Kaur, K.; Sikka, K.; Sen, S.; Kakkar, A. Endocrine Mucin Producing Sweat Gland Carcinoma with Metastasis to Parotid Gland: Not as Indolent as Perceived? Head Neck Pathol. 2022, 16, 331–337. [Google Scholar] [CrossRef]
- Shah, D.S.; Homer, N.A.; Epstein, A.; Durairaj, V.D. Simultaneous presentation of orbital mantle cell lymphoma and endocrine mucin-producing sweat gland carcinoma. Orbit 2022, 41, 509–513. [Google Scholar] [CrossRef]
- Wang, D.; Deng, W.; LoBue, S.; Giovinazzo, K.; Rosen, M.; Heilman, E.; Hodgson, N.M. Bilateral Concurrent Endocrine Mucin-Producing Sweat Gland Carcinoma and Mucinous Carcinoma of the Eyelids. Ophthalmic Plast. Reconstr. Surg. 2022, 38, e96–e99. [Google Scholar] [CrossRef]
- Au, R.T.M.; Bundele, M.M. Endocrine mucin-producing sweat gland carcinoma and associated primary cutaneous mucinous carcinoma: Review of the literature. J. Cutan. Pathol. 2021, 48, 1156–1165. [Google Scholar] [CrossRef]
- Quattrochi, B.; Russell-Goldman, E. Utility of Insulinoma-Associated Protein 1 (INSM1) and Mucin 2 (MUC2) Immunohistochemistry in the Distinction of Endocrine Mucin-Producing Sweat Gland Carcinoma from Morphologic Mimics. Am. J. Dermatopathol. 2022, 44, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Saggini, A.; Cota, C. Local invasion in endocrine mucin-producing sweat gland carcinoma: Still an open issue. J. Cutan. Pathol. 2020, 47, 192–194. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Author(s) | Year | Patient(s) Gender | Age | Localization | IHC Features (Only Positive) |
|---|---|---|---|---|---|
| Flieder et al. [1] | 1997 | 2 female | 60, 75 | 2 eyelids | Syn+ CgA+ ER, PgR+ |
| Tannous et al. [5] | 2005 | 1 female | 79 | lateral right canthus | Syn+ CgA+ ER, PgR+ |
| Zembowicz et al. [6] | 2005 | 12 cases (8 f, 4 m) | 70 (48–84) | 8 lower eyelids 2 upper eyelids 2 cheek | At least one of: Syn, CgA, EMA, CK7, CK8/18, ER, PgR |
| Bulliard et al. [11] | 2006 | 1 female | 72 | right lower eyelid | Syn+ CK+ |
| Emanuel et al. [12] | 2007 | 1 female | 61 | left lower eyelid | Syn+ CgA+ |
| Mehta et al. [13] | 2008 | 1 female | 70 | left upper eyelid | Syn+ |
| Chang et al. [14] | 2010 | 1 male | 51 | eyelid | CgA, Syn+ ER, PgR+ CK7, EMA+ |
| Inozume et al. [15] | 2012 | 1 male | 55 | upper cheek | Syn+ CgA+ CK8/18 and CK7+ |
| Salim et al. [16] | 2012 | 2 female 1 male | 69 and 53 36 | eyelids | Syn+ CgA+ CK7, CEA+ ER, PgR+ |
| Koike et al. [17] | 2013 | 1 male | 61 | left upper eyelid | focal Syn+ |
| Dhaliwal et al. [18] | 2013 | 2 female | 61 and 64 | eyelids | Syn+ CgA+ CKAE1/AE3, CAM5.2+ CK7+ |
| Hoguet et al. [19] | 2013 | 11 male 5 female | 70 (53–87) | 9 upper eyelids 6 lower eyelids 1 not available | All (15): LWCK+ CEA+ ER, PgR+ BRST-2+ At least one of: Syn, CgA, CD56, NSE |
| Tsai et al. [4] | 2014 | 1 male | 57 | left chest (areolar) | Syn+ CgA+ ER, PgR+ P63+ (myoepithelial cells) |
| Shimizu et al. [20] | 2014 | 1 female 1 male | 72 74 | eyelids | Syn+ CgA+ CKAE1/AE3, CAM5.2+ CK7+ |
| Shon et al. [21] | 2014 | 8 female 5 male | 61.2 (40–77 years) | eyelids | WT1, CK7, ER, P-CEA and EMA+ Syn, CgA+ |
| Collinson et al. [22] | 2015 | 1 female | 78 | left upper eyelid | Ber-EP4+ CK7+ EMA+ Syn, CgA focal+ ER, PgR+ |
| Fernandez-Flores et al. [23] | 2015 | 1 male 1 male 1 female | 88 76 69 | cheek right upper eyelid right upper eyelid | CK8/18+ CK7+ Syn, CgA+ ER, PgR+ |
| Jedrych et al. [24] | 2015 | 1 female | 75 | left lower eyelid | CK AE1/AE3+ ER, PgR+ GCDFP-15+ CK7+ Syn focal+ |
| Turnbull et al. [25] | 2015 | 1 male 1 male | 62 57 | left lower eyelid right lower eyelid | Syn, NSE focal+ CK7+ ER, PgR+ (case 1) |
| Bamberger et al. [26] | 2016 | 1 male | 74 | left eyelid | CK7+ NSE+ CD57+ Syn, CgA+ ER+ |
| Cornejo et al. [27] | 2016 | 1 female | 71 | left upper eyelid | CK CAM5.2+ Syn, CgA, NSE+ ER, PgR+ Ber-EP4+ EMA+ |
| Abdulkader et al. [28] | 2016 | 1 female 1 female | 83 51 | left lower eyelid right upper lid | CK7+ EMA+ GCDFP-15+ ER, PgR+ Syn, CgA+ GATA-3+ Syn+ CgA focal+ ER, PgR+ GATA-3+ |
| Ross et al. [29] | 2017 | 1 female | 29 | right lateral lid | NSE+ |
| Brett et al. [30] | 2017 | 1 female | 73 | upper right eyelid | Syn, CgA, NSE, CD57+ CK CAM 5.2, CK7, GCDFP-15+ ER, PgR+ EMA focal+ |
| Scott et al. [31] | 2017 | 1 female | 70 | eyelid | Syn, CD56+ CK7+ ER, PgR+ |
| Chou et al. [32] | 2017 | 1 male 1 female | 87 55 | cheek left upper eyelid | ER, PgR+ GATA-3+ WT1+ Syn+ ER, PgR+ GATA-3+ Syn+ |
| Held et al. [8] | 2018 | 7 male 4 female | 66 years (range, 61–84 years | 5 lower eyelid 1 upper eyelid 2 cheek 1 supra-auricular 1 retro-auricular 1 occipital | Ber-EP4+ At least one of: Syn, CgA+ CK7, CK CAM 5.2+ ER and/or PgR+ MYB+ |
| Charles et al. [33] | 2018 | 1 male | 59 | eyelid | Syn, CgA+ CK7, CK CAM 5.2+ ER, PgR+ |
| Qin et al. [34] | 2018 | 8 female 3 male | 66 years (56–83) | eyelids and cantus | Syn, CgA+ CK7, CK CAM 5.2+ ER, PgR+ |
| Hasegawa-Murakami et al. [35] | 2018 | 1 male | 78 | right temple | focal Syn, CgA+ CK7+, CK CAM5.2+ NSE+ ER, PgR+ |
| Nair et al. [36] | 2018 | 1 male | 60 | left upper lid | CK7, CK8+ ER, PgR+ Syn+ GCDFP-15+ NSE+ |
| Navrazhina et al. [37] | 2018 | 1 female | 81 | scalp | Syn+ focal CK7+ |
| Kawasaki et al. [38] | 2018 | 1 male | 51 | eyelid | Syn, CgA+ CK, ER, PgR+ |
| Chen et al. [39] | 2018 | 1 male 1 male | 55 87 | left cheek left cheek | CK7, GATA3+ Syn, p63, ER, PgR focal+ CK7, GATA3+ ER, PgR+ Syn, CgA focal+ |
| Mulay et al. [40] | 2019 | 7 female 3 male | 55–82 (average, 68.7) | eyelids | ER, PgR+ Pan-CK+ EMA, GCDFP-15+ NSE, CgA focal+ |
| Meltzer et al. [41] | 2019 | 1 female | 64 | left lower eyelid | Syn, CgA+ CK7+ |
| Ansari et al. [42] | 2019 | 7 female 2 male | 50–86 (limits) | 8 eyelids 1 scalp | At least of: Syn, CgA, NSE+ CK-7, EMA+ RCC+ |
| Nathan et al. [43] | 2020 | 1 female | 74 | right tragus | Syn, CgA+ CK7+ ER, AgR+ |
| Nasser et al. [44] | 2020 | 1 male 1 female | 72 77 | left lower eyelids | Ber-EP4+ ER+ CgA+ |
| Murshed et al. [45] | 2020 | 1 male | 78 | eyelid | CK7, CK8/18+ Syn+ ER, PgR+ GCFDP-15+ EMA+ |
| Bakrin et al. [46] | 2020 | 1 male | 59 | eyelid | CK7, EMA+ GCDFP-15, Mammoglobin+ ER, PgR+ Syn, CgA+ Syn, CgA+ |
| Shah et al. [47] | 2020 | 1 male | 70 | eyelid | CK7+ ER+ GATA-3+ Syn+ |
| Agni et al. [48] | 2020 | 42 female 21 male | 64 (47–87) | 62 eyelids 1 temple | ER, PgR+ Syn, CgA+ |
| Froehlich et al. [49] | 2020 | 1 female | 71 | right eyelid | Syn, CgA+ |
| Nakamura et al. [50] | 2020 | 4 male | 70 72 53 66 | cheek cheek lower jaw cheek | CK7+ ER, PgR+ Syn+ CK AE1/AE3+ |
| Katsura et al. [51] | 2021 | 1 male | 90 | cheek | CK7+ ER, AgR+ |
| Hadi et al. [52] | 2021 | 1 male | 66 | upper eyelid | GATA-3+ |
| Nishimoto et al. [53] | 2021 | 1 female | 71 | left cheek and upper eyelids right cheek (multiple lesions) | Mammoglobin+ Syn, CgA focal+ CK7+ ER, PgR+ |
| Shah et al. [54] | 2021 | 1 male | 60 | scrotum | CgA+ CK7+ ER, GATA-3+ CgA, Syn+ |
| Homer et al. [55] | 2021 | 1 male | 40 | eyelid | Syn, EMA, CK7+ Syn, CgA+ INSM1+ |
| Parra et al. [9] | 2021 | 5 female 3 male | 51–84 | 4 eyelids, 1 cheek 2 eyelids, 1 cheek | GATA-3, ER, PgR+ CK7, Syn, CgA+ ER, PgR, INSM1+ MYB+ |
| Schafer et al. [56] | 2022 | 6 female 2 male | 64 mean | 7 eyelids 1 cheek | at least one of NM+ |
| Chuang et al. [57] | 2022 | 3 male | 68, 52, 54 | infraocular | GCDFP-15+ CK7, ER, PgR+ GATA-3+ |
| Ravi et al. [58] | 2022 | 4 male 3 female | 76 (range, 59–98) | eyelids | CK7+ Syn, CgA+ |
| Sarangi et al. [59] | 2022 | 1 male | 78 | preauricular | ER, PgR, AgR+ GCDFP-15+ Mammoglobin+ Syn, CgA+ |
| Shah et al. [60] | 2022 | 1 male | 77 | upper lid | at least of NM |
| Wang et al. [61] | 2022 | 1 female | 55 | eyelid | CK7+ |
| Mathew et al. [10] | 2022 | 15 female 7 male | 71.8 (53–88) | eyelids/peri-orbital | INMS1+ Bcl2+ B-cat+ AgR+ RB1+ partial MUC2+ focal MUC4+ |
| Reference(s) | Sample(s) (n) | Recurrence Follow-Up (Months) | Clinical Outcomes (Recurrence/Metastasis) (n) |
|---|---|---|---|
| [1] | 2 | 72 | 1 |
| [5] | 1 | 24 | 0 |
| [6] | 12 | 228 | 0 |
| [11] | 1 | 7 | 0 |
| [12] | 1 | 36 | 1 |
| [13] | 1 | 6 | 0 |
| [14] | 1 | - | - |
| [15] | 1 | 2 | 0 |
| [16] | 3 | 88 | 0 |
| [17] | 1 | 6 | 0 |
| [18] | 2 | 31 | 0 |
| [19] | 16 | 242 | 2 |
| [4] | 1 | 30 | 0 |
| [20] | 2 | - | - |
| [21] | 13 | 144 | 0 |
| [22] | 1 | 8 | 0 |
| [23] | 3 | - | - |
| [24] | 1 | - | - |
| [25] | 2 | - | - |
| [26] | 1 | 12 | 0 |
| [27] | 1 | 1 | 0 |
| [28] | 2 | 13 | 0 |
| [29] | 1 | - | 0 |
| [30] | 1 | 6 | 0 |
| [31] | 1 | - | - |
| [32] | 2 | 14 | 0 |
| [8] | 11 | 0 | 0 |
| [33] | 1 | - | - |
| [34] | 11 | - | - |
| [35] | 1 | 36 | 0 |
| [36] | 1 | 6 | 0 |
| [37] | 1 | - | - |
| [38] | 1 | - | - |
| [39] | 2 | 16 | 0 |
| [40] | 10 | 6–36 | 1 |
| [41] | 1 | 6 | 0 |
| [42] | 9 | not retrieved | not retrieved |
| [43] | 1 | 18 | 0 |
| [44] | 2 | 17/38 | 0 |
| [45] | 1 | 24 | 0 |
| [46] | 1 | 3 | 0 |
| [47] | 1 | - | 0 |
| [48] | 63 | 1–67 | 9 |
| [49] | 1 | not retrieved | 1 |
| [50] | 4 | - | 0 |
| [51] | 1 | 42 | 0 |
| [52] | 1 | 11 months (after metastasis) | 1 |
| [53] | 1 | 12 | 0 |
| [54] | 1 | - | 1 |
| [55] | 1 | 8 | 0 |
| [9] | 8 | 84 (mean) | 0 |
| [56] | 8 | 24 (mean) | 0 |
| [57] | 3 | 9/21/7 | 0 |
| [58] | 7 | not retrieved | 0 |
| [59] | 1 | 108 | 1 |
| [60] | 1 | 11 | 0 |
| [61] | 1 | not retrieved | 0 |
| [10] | 22 | 43.25 (mean) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzato, G.; Bellitti, E.; Trilli, I.; Colagrande, A.; Sgarro, N.; Scarcella, V.S.; Lettini, T.; Ingravallo, G.; Piscitelli, D.; Resta, L.; et al. Endocrine Mucin-Producing Sweat Gland Carcinoma: Case Presentation with a Comprehensive Review of the Literature. Dermatopathology 2023, 10, 266-280. https://doi.org/10.3390/dermatopathology10030035
Cazzato G, Bellitti E, Trilli I, Colagrande A, Sgarro N, Scarcella VS, Lettini T, Ingravallo G, Piscitelli D, Resta L, et al. Endocrine Mucin-Producing Sweat Gland Carcinoma: Case Presentation with a Comprehensive Review of the Literature. Dermatopathology. 2023; 10(3):266-280. https://doi.org/10.3390/dermatopathology10030035
Chicago/Turabian StyleCazzato, Gerardo, Emilio Bellitti, Irma Trilli, Anna Colagrande, Nicoletta Sgarro, Vincenza Sara Scarcella, Teresa Lettini, Giuseppe Ingravallo, Domenico Piscitelli, Leonardo Resta, and et al. 2023. "Endocrine Mucin-Producing Sweat Gland Carcinoma: Case Presentation with a Comprehensive Review of the Literature" Dermatopathology 10, no. 3: 266-280. https://doi.org/10.3390/dermatopathology10030035
APA StyleCazzato, G., Bellitti, E., Trilli, I., Colagrande, A., Sgarro, N., Scarcella, V. S., Lettini, T., Ingravallo, G., Piscitelli, D., Resta, L., & Lospalluti, L. (2023). Endocrine Mucin-Producing Sweat Gland Carcinoma: Case Presentation with a Comprehensive Review of the Literature. Dermatopathology, 10(3), 266-280. https://doi.org/10.3390/dermatopathology10030035