
Lichen Planus Pigmentosus with True Melanocytic Nests: A Case Report with a Comprehensive Literature Review

 , , ,
, , , 
Abstract
:1. Introduction
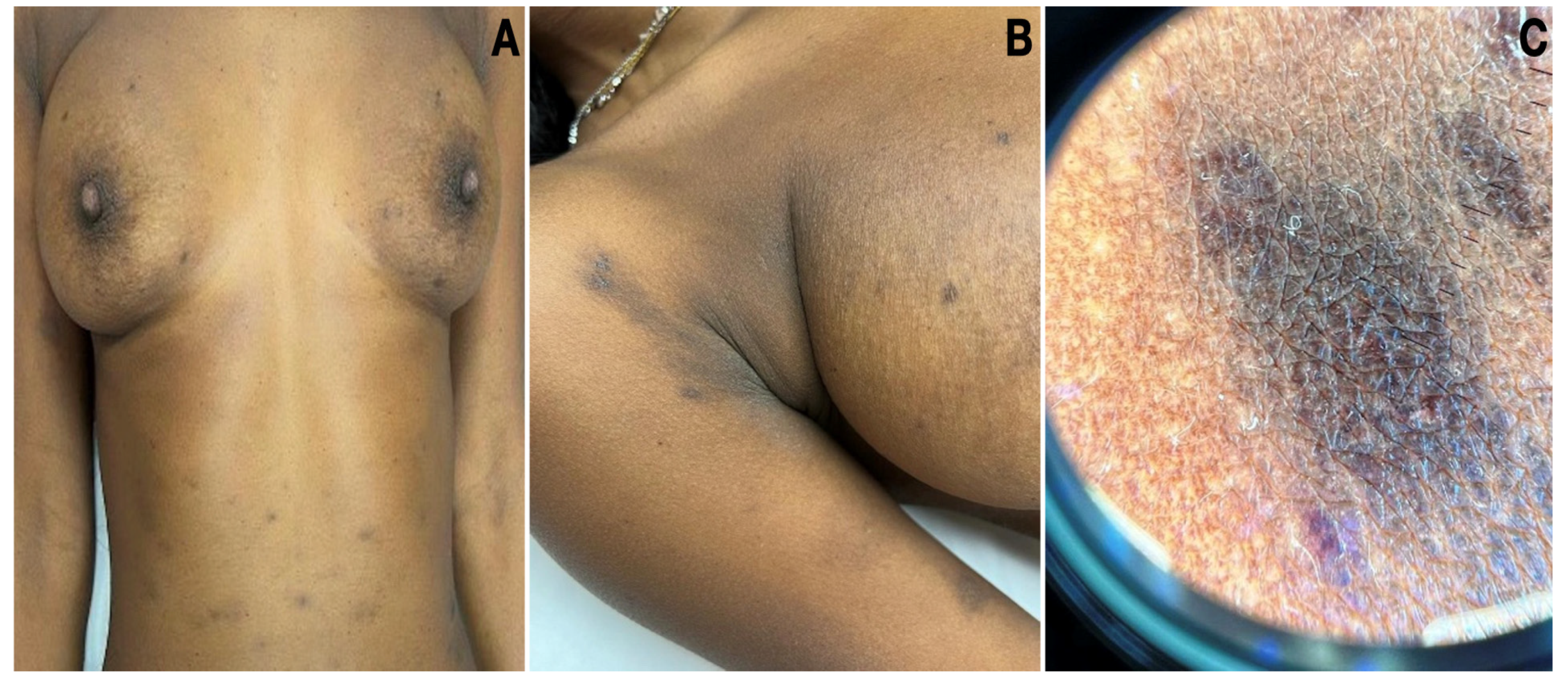
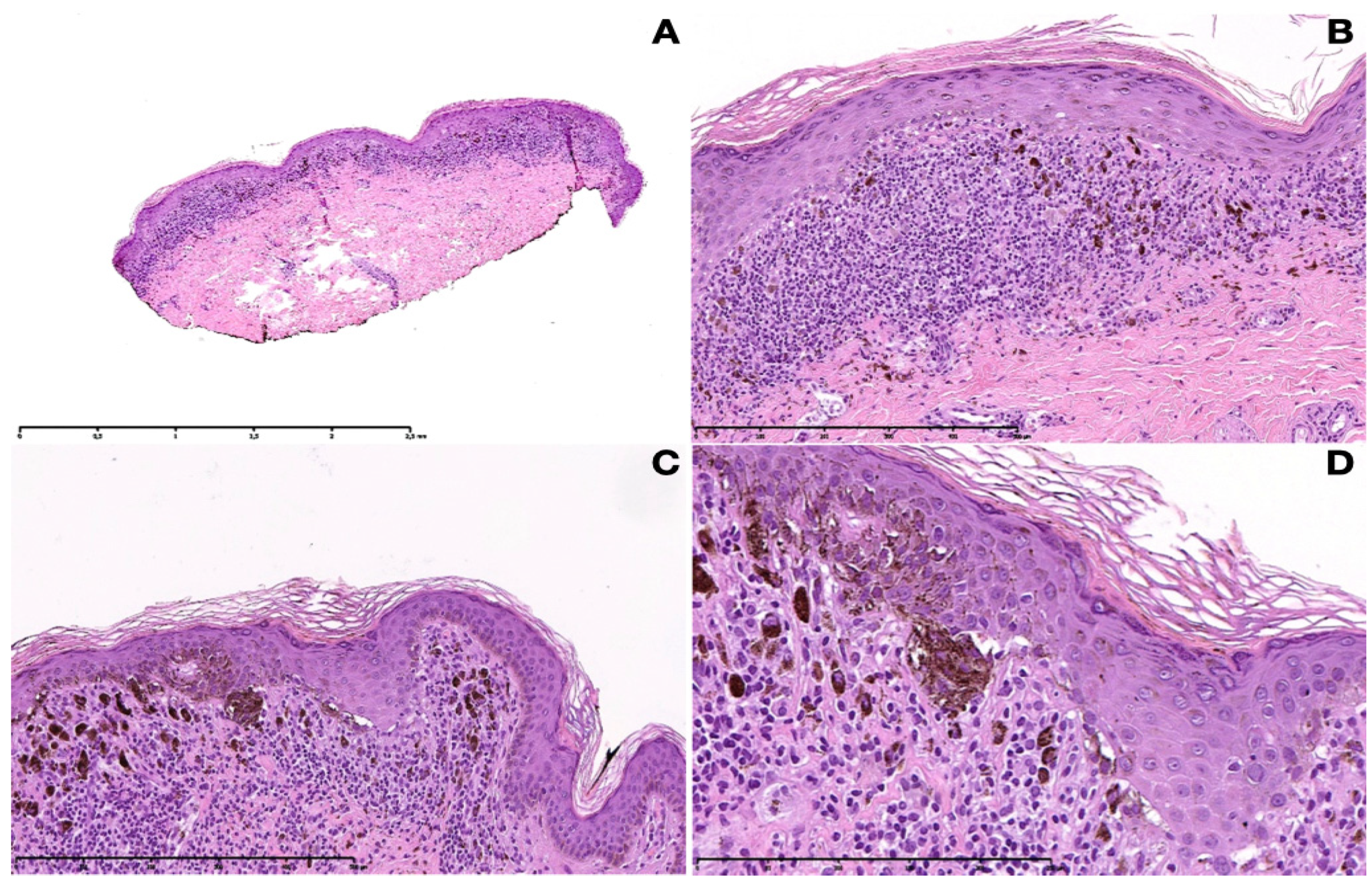
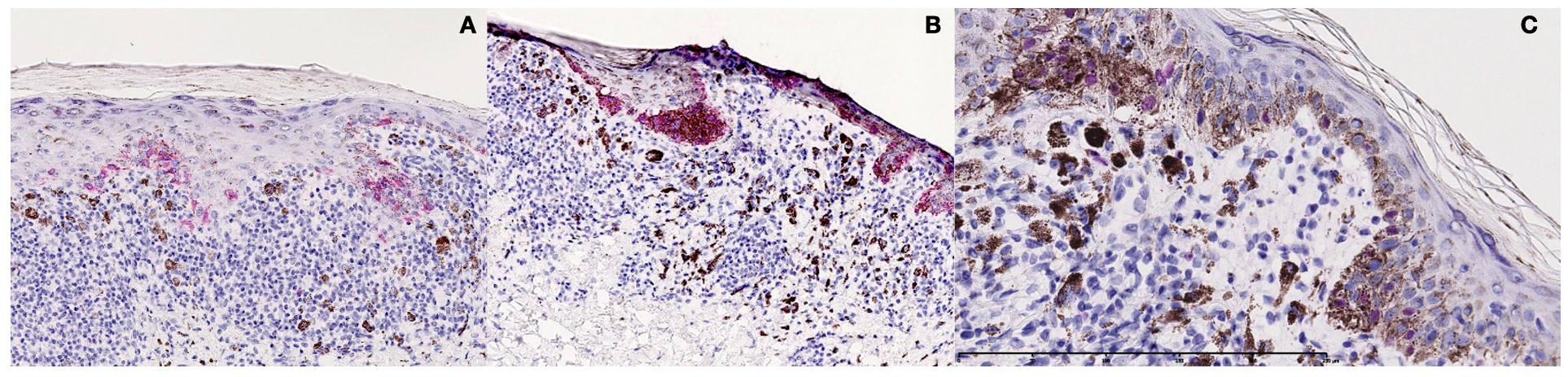
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rieder, E.; Kaplan, J.; Kamino, H.; Sanchez, M.; Pomeranz, M.K. Lichen planus pigmentosus. Dermatol. Online J. 2013, 19, 20713. [Google Scholar] [CrossRef]
- Ghosh, A.; Coondoo, A. Lichen Planus Pigmentosus: The Controversial Consensus. Indian J. Dermatol. 2016, 61, 482–486. [Google Scholar] [CrossRef]
- Maize, J.C., Jr.; Resneck JSJr Shapiro, P.E.; McCalmont, T.H.; LeBoit, P.E. Ducking stray “magic bullets”: A Melan-A alert. Am. J. Dermatopathol. 2003, 25, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Venturini, M.; Manganoni, A.M.; Zanca, A.; Bassissi, S.; Pavoni, L.; Gonzales, S.; Cesinaro, A.; Calzavara-Pinton, P. Pigmented actinic lichen planus (PALP) mimicking lentigo maligna melanoma: Usefulness of in vivo reflectance confocal microscopy in diagnosis and follow-up. JAAD Case Rep. 2018, 4, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, J.L.; Macedo, R.M.; Almeida, L.Y.; Silva, R.N.; Ribeiro-Silva, A.; León, J.E. Gingival melanoacanthoma associated with pseudomelanocytic nests: Expanding the clinicopathological spectrum of a recently described oral lesion. J. Cutan. Pathol. 2012, 45, 725–727. [Google Scholar] [CrossRef]
- McClanahan, D.; Choudhary, S.; Zahniser, J.; Ho, J. Diagnostic Pitfalls: Pseudomelanocytic Nests in the Setting of Lichenoid Inflammation. Actas Dermosifiliogr. 2019, 110, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, G.; Bradamante, M.; Broglia, I.; Petrillo, G.; Stefanato, C.M. Melanocytic and pseudomelanocytic nests coexist in interface dermatitis from head-neck sun-exposed skin: A report of three cases. J. Cutan. Pathol. 2020, 47, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Panse, G.; McNiff, J.M. Lichenoid dermatoses with pseudomelanocytic nests vs inflamed melanoma in situ: A comparative study. J. Cutan. Pathol. 2021, 48, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Bertlich, I.; Hartschuh, W.; Fink, C.; Haenssle, H.; Enk, A.; Toberer, F. Sudden reticular pigmentation of the face. J. Cutan. Pathol. 2022, 49, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Beltraminelli, H.; Shabrawi-Caelen, L.E.; Kerl, H.; Cerroni, L. Melan-a-positive “pseudomelanocytic nests”: A pitfall in the histopathologic and immunohistochemical diagnosis of pigmented lesions on sun-damaged skin. Am. J. Dermatopathol. 2009, 31, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, K.M.; Gerami, P. An immunohistochemical analysis of pseudomelanocytic nests mimicking melanoma in situ: Report of 2 cases. Am. J. Dermatopathol. 2010, 32, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.Y.; Goldberg, L.J.; Mahalingam, M.; Bhawan, J.; Wolpowitz, D. Nests with numerous SOX10 and MiTF-positive cells in lichenoid inflammation: Pseudomelanocytic nests or authentic melanocytic proliferation? J. Cutan. Pathol. 2011, 38, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Boros, A.L.; Handlers, J.P.; Melrose, R.J. Pseudomelanocytic nests mimicking atypical melanocytic proliferations: First reported cases in the oral cavity. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 118, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.J.; Simkin, A.D.; Bhawan, J.; Wolpowitz, D. “Melanocytic Nests Arising in Lichenoid Inflammation”: Reappraisal of the Terminology “Melanocytic Pseudonests”. Am. J. Dermatopathol. 2015, 37, 940–943. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.D.; Bodendorf, M.O.; Najarian, D.J.; Ferringer, T.; Elston, D. Soluble adenylyl cyclase (sAC) immunostaining distinguishes pseudomelanocytic nests in lichenoid tissue reaction. J. Cutan. Pathol. 2015, 42, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Pantaleão, L.; Orofino-Costa, R.; Torres, M.C.; Lazova, R.; Rochael, M.C. Report of two cases of vacuolar interface dermatitis initially suspected as melanomain situand review of the literature. J. Bras. Patol. Med. Lab. 2016, 52, 116–119. [Google Scholar] [CrossRef]
- Marques, L.C.; Santos, L.R.; da Silva, N.C.; Cunha, K.S.; Junior, A.S.; Conde, D.C. Oral Lichen Planus Associated with Lichen Planus Pigmentosus and Lichen Sclerosus in Monozygotic Twins. Am. J. Dermatopathol. 2021, 43, 368–372. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Reference | Age/Sex | Clinical Presentation and Location | Positive/Negative Nests Stains | Final Diagnosis | Interpretation of Nests |
|---|---|---|---|---|---|
| Maize et al., 2003 [3] | 35/M | Blue-gray macules on the left temple | Melan-A + HMB45, S100, Tyr, BCL2− | Discoid and melanotic LE | Pseudomelanocytic nests |
| Beltraminelli et al., 2009 [10] | 60/M | Ill-defined brown grayish pigmentation on the checks | Melan-A, CK + HMB45, S100− | Lichenoid phototoxic reaction | Pseudomelanocytic nests |
| Beltraminelli et al., 2009 [10] | 59/M | Irregular, partly confluent, reticulated pigmentation on the forehead | Melan-A, CK + HMB45, S100− | LPP | Pseudomelanocytic nests |
| Beltraminelli et al., 2009 [10] | 52/F | Small scaly plaque of the infraorbital region | Melan-A, CK + HMB45, S100− | Pigmented lichenoid keratosis | Pseudomelanocytic nests |
| Nicholson and Gerami 2010 [11] | 39/F | New asymptomatic brown macules along the hair line | Melan-A, CK, CD68, CD3 + HMB45, S100, MITF− | FDE | Pseudomelanocytic nests |
| Nicholson and Gerami 2010 [11] | 76/F | Well-demarcated hyperpigmented patch on the periocular arca | Melan-A, CK, CD3 + HMB45, S100, MITF, CD68 − | FDE | Pseudomelanocytic nests |
| Silva et al., 2011 [12] | 48/M | Discrete, reticulate, hyperpigmented patch of the neck | Melan-A, S100, SOX10, MITF, CK + − | LPP/Erythema dyschromicum perstans | Melanocytic pseudonests |
| Boros et al., 2014 [13] | 66/M | Solitary slightly elevated pigmented lesion on the interdental papilla | CD68 + Melan-A, SOX10, MITF− | Chronic mucositis | Pseudomelanocytic nests |
| Boros et al., 2014 [13] | 61/F | Solitary pigmented lesion on the hard plate | CD68 + Melan-A− | Melanophages | Pseudomelanocytic nests |
| Chung et al., 2015 [14] | 40/M | Violaceous, polygonal, flat-topped, mildly pruritic papules sited on the back, the ankles, and feet | Melan-A, SOX10+ − | LP | Melanocytic nests |
| Hall et al., 2015 [15] | 48/M | Irregular brown and violaceous patch on the chest | Melan-A, SOX10, MITF, S100 + − | LP actinicus | Melanocytic pseudonests |
| Pantaleão et al., 2016 [16] | 47/F | Pigmented lesion of the left upper arm | Melan-A, HMB45, S100, TYR + − | FDE | Pseudomelanocytic nest |
| Pantaleão et al., 2016 [16] | 34/M | Greyish brown plaque, scattered black papules, and greyish macules on the left forehead and right side of the face. | Melan-A + − | Vacuolar interface dermatitis | Pseudomelanocytic nests |
| Venturini et al., 2018 [4] | 40/M | Asymptomatic pigmented patch on the right cheek | Melan-A + − | Pigmented actinic LP | Melanocytic pseudonests |
| Dos Santos et al., 2018 [5] | 41/F | Irregularly pigmented lesion between the left maxillary central and lateral incisors | Melan-A, CK, CD68 + SOX10, S100− | Oral melanocanthoma | Pseudomelanocytic nests |
| McClanahan D et al., 2018 [6] | 32/M | Speckled brown appearance and areas of erythema on the anterior shoulder | Melan-A, S100, CK + SOX10− | Lichen striatus | Melanocytic pseudonests |
| Ferrara et al., 2020 [7] | 36/M | Brownish macule on the left temple | Melan-A, SOX10, MITF + S100, CK, PRAME− | Melanotic cutaneous LE | Melanocytic nests |
| Ferrara et al., 2020 [7] | 31/M | Linear atrophic hyperpigmented patch on the neck and the chin | Melan-A, SOX10, MITF, CK + S100, PRAME− | Discoid LE | Melanocytic pseudonests |
| Ferrara et al., 2020 [7] | 66/F | Bilateral symmetric grayish, slightly atrophic macules of the orolabial folds | Melan-A, SOX10, MITF + S100, PRAME− | Discoid LE | Melanocytic pseudonests |
| Panse et al., 2021 [8] | 48/F | Melasma, post-inflammatory hyperpigmentation of the cheek | SOX10, MITF + − | Lichenoid dermatitis | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 49/M | Erythema multiforme on the cheek | MITF + − | FDE | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 76/F | Changing lesion on the arm | MITF + − | LP like keratosis | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 42/M | Rash on the temple | MITF + − | LPP | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 49/M | Lichen Planus Pigmentosus on the preauricular region | MITF + S100− | LPP | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 48/M | Irritated SK on the neck | MITF + − | LP like keratosis | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 56/M | Sarcoidosis of the eyelid | MITF, SOX10 + − | LE | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 69/F | Lichen planus-like keratosis on the chest | MITF + − | LP like keratosis | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 69/M | Eczema on the back | MITF, SOX10 + S100− | Graft versus host disease | Pseudomelanocytic nests |
| Panse et al., 2021 [8] | 71/M | Recurrent BCC on the chest | MITF + − | Benign keratosis with reactive changes | Pseudomelanocytic nests |
| Bertlich et al., 2022 [9] | 39/M | Multiple brown macules in a retiform distribution on the left forehead and the left side of the nose and chin | Melan-A, SOX10, MITF, S100, CD68 + TYR, PRAME− | Cutaneus LE | Melanocytic pseudonests |
| Our case | 32/F | Grey-brown patches and macules located on the trunk, axillary flexures, and upper and lower extremities | Melan-A, HMB45, S100, SOX10 + CD68, CD3− | LPP | Melanocytic nests |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Podo Brunetti, A.; Bigotto, G.D.; Stabile, G.; Caputo, V.; Brambilla, L.; Guida, S.; Rongioletti, F. Lichen Planus Pigmentosus with True Melanocytic Nests: A Case Report with a Comprehensive Literature Review. Dermatopathology 2023, 10, 281-286. https://doi.org/10.3390/dermatopathology10030036
Podo Brunetti A, Bigotto GD, Stabile G, Caputo V, Brambilla L, Guida S, Rongioletti F. Lichen Planus Pigmentosus with True Melanocytic Nests: A Case Report with a Comprehensive Literature Review. Dermatopathology. 2023; 10(3):281-286. https://doi.org/10.3390/dermatopathology10030036
Chicago/Turabian StylePodo Brunetti, Antonio, Gianmarco Diego Bigotto, Giorgio Stabile, Valentina Caputo, Lucia Brambilla, Stefania Guida, and Franco Rongioletti. 2023. "Lichen Planus Pigmentosus with True Melanocytic Nests: A Case Report with a Comprehensive Literature Review" Dermatopathology 10, no. 3: 281-286. https://doi.org/10.3390/dermatopathology10030036
APA StylePodo Brunetti, A., Bigotto, G. D., Stabile, G., Caputo, V., Brambilla, L., Guida, S., & Rongioletti, F. (2023). Lichen Planus Pigmentosus with True Melanocytic Nests: A Case Report with a Comprehensive Literature Review. Dermatopathology, 10(3), 281-286. https://doi.org/10.3390/dermatopathology10030036