

Computer System for the Capture and Preparation of Cytopathological Reports for Cervical Cancer Detection and His Utility in Training for Health Personnel

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
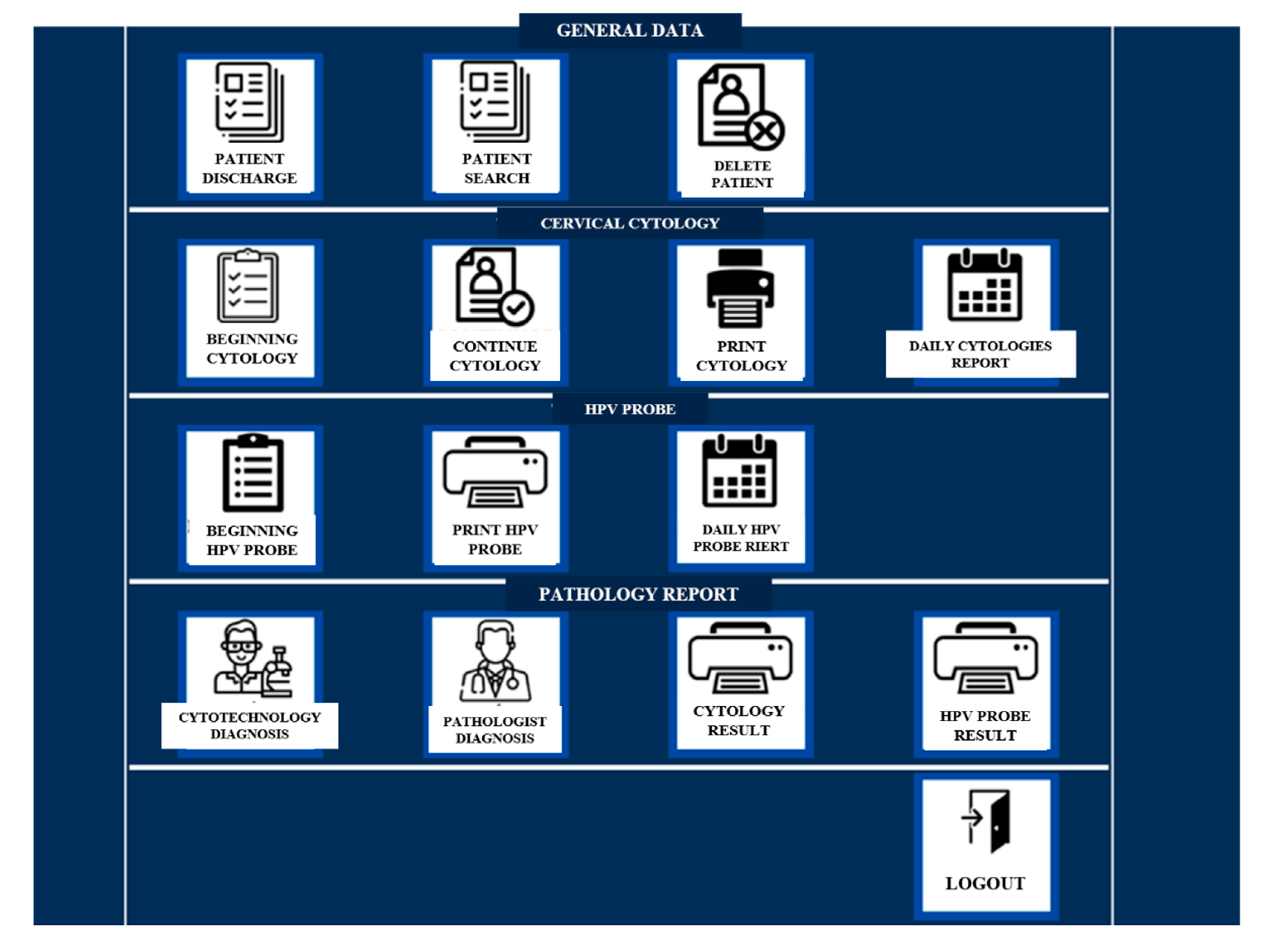
2.1. System Design and Operation
2.2. Participants
2.3. Training for System Execution
2.4. Instruments for System Testing
2.5. System Implementation
2.6. Data Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Globocan 2020: New Global Cancer Data. Available online: https://www.uicc.org/news/globocan-2020-new-global-cancer-data (accessed on 12 March 2020).
- Centro Nacional de Equidad de Género y Salud Reproductiva, Secretaría de Salud-México. Hoja de Datos Sobre Cáncer de Cuello Uterino. Semana de Sensibilización en Cáncer de Cuello Uterino. 2019. Available online: https://www.gob.mx/cms/uploads/attachment/file/487307/Hoja_de_Datos_2019_CACU.pdf (accessed on 14 December 2021).
- Cancer Today, IARC 2020. Available online: https://gco.iarc.fr/today/home (accessed on 18 December 2021).
- Global Initiative or Cancer Registry Development. Available online: https://gicr.iarc.fr/about-the-gicr/the-value-of-cancer-data/ (accessed on 14 December 2021).
- Cervical Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 1 March 2022).
- Strengthening Health Information Systems. Available online: https://www3.paho.org/hq/index.php?option=com_content&view=article&id=5548:2011-strengthening-health-information-systems-pevs&Itemid=3976&lang=en (accessed on 1 March 2022).
- Programa de Acción Específico Información en Salud. Available online: http://www.dgis.salud.gob.mx/descargas/pdf/PAE_2013-2018_DGIS_18DIC2014.pdf. (accessed on 27 February 2021).
- Pirovano, A.; Almeida, L.G.; Ladjal, S.; Bloch, I.; Berlemont, S. Computer-aided diagnosis tool for cervical cancer screening with weakly supervised localization and detection of abnormalities using adaptable and explainable classifier. Med. Image. Anal. 2021, 73, 102167. [Google Scholar] [CrossRef] [PubMed]
- Alholm, Z.; Ding, H.; Ting, J.; Zhang, Y.J.; Sudharshan, L.; Leong, T.; Coleman, R.L.; Monk, B.J. Real-world treatment drop-off among recurrent or metastatic cervical cancer patients: A US community oncology-based analysis. Gynecol. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- México: Centro Nacional de Equidad de Género y Salud Reproductiva. Programa de Acción Específico Prevención y Control del Cáncer de la Mujer 2013-2018. 2013. Available online: http://cnegsr.salud.gob.mx/contenidos/descargas/cama/PrevencionyControldelCancerdelaMujer_2013_2018.pdf. (accessed on 12 April 2022).
- Norma Oficial Mexicana NOM-014-SSA2-1994 Para la Prevención, Detección, Diagnóstico, Tratamiento, Control y Vigilancia Epidemiológica del Cáncer Cervicouterino. Available online: http://www.salud.gob.mx/unidades/cdi/nom/m014ssa294.pdf (accessed on 2 April 2022).
- Vidales Cerda, M.T.J. Caracterización De Los Sistemas de Información Que Se Utilizan En El Programa De Cáncer Cervicouterino De Los Servicios De Salud De San LUIS POTOSÍ, S.L.P. Master’s Thesis, Universidad Autónoma de San Luis Potosí, San Luis Potosí, México, 2017. Available online: https://repositorioinstitucional.uaslp.mx/xmlui/handle/i/4490. (accessed on 2 April 2022).
- Norma Oficial Mexicana NOM-004-SSA3-2012. Del expediente clínico. Available online: http://dof.gob.mx/nota_detalle_popup.php?codigo=5272787 (accessed on 12 April 2022).
- Vargas Herrera, J.; Manrique, J.; Nuñez, M.C.; Sánchez, P.; Miraval, M.; Merejildo, M.; Puntas, V. Aplicación de un sistema de información electrónico al programa de tamizaje de cáncer de cuello uterino. Rev Perú Med Exp Salud Publica 2013, 30, 521–530. Available online: http://www.scielo.org.pe/pdf/rins/v30n3/a26v30n3.pdf (accessed on 12 December 2021). [CrossRef]
- Rygaard, C. The Danish Quality Database for Cervical Cancer Screening. Clin. Epidemiol. 2016, 25, 655–660. [Google Scholar] [CrossRef]
- Freyermuth Enciso, G.; Meneses Navarro, S.; Romero Martínez, M. Evaluación de los programas de atención a la salud de las mujeres en las principales instituciones del sistema de salud de México. Cad. Saúde. Pública 2015, 31, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Enríquez, S.O.; Gaytán-Hernández, D.; Zamarripa-Leyva, J.M.; Terán- Figueroa, Y. Desempeño del personal de salud en la toma de las citologías cervicales: Conocimientos teóricos y ejecución práctica. Ginecol Obstet Mex 2014, 82, 296–306. Available online: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=49549 (accessed on 25 July 2020).
- Gutiérrez-Enríquez, S.O.; Terán-Figueroa, Y.; Monreal-Delgado, L.; Nieva de Jesús, R.; Gaytán-Hernández, D. Calidad de los registros en programa de detección oportuna de cáncer cervicouterino. Medicas UIS 2017, 30, 59–65. Available online: https://biblat.unam.mx/hevila/MedicasUIS/2017/vol30/no3/7.pdf. (accessed on 25 July 2020). [CrossRef]
- Terán-Figueroa, Y.; Muñiz-Carreón, P.; Fernández Moya, M.; Galán-Cuevas, S.; Noyola-Rangel, N.; Gutiérrez-Enríquez, S.O.; Ortiz-Valdez, J.A.; Cruz-Valdez, A. Repercusiones del cáncer cervicouterino en pacientes con limitaciones de acceso a los servicios de salud. Ginecol. Obstet. Mex. 2015, 83, 162–172. Available online: https://www.medigraphic.com/pdfs/ginobsmex/gom-2015/gom153e.pdf (accessed on 25 July 2020).
- Gutiérrez-Enríquez, S.O.; Chávez-Hernández, L.; Terán-Figueroa, Y.; Gaytán- Hernández, D.; Oros-Ovalle, C.; Gallegos-García, V.; Díaz-Oviedo, A.; González- Acevedo, C. Concordance in the Interpretation of Cervical Cytology for the Early Diagnosis of Cervical Cancer. Open J. Obstet. Ginecol. 2016, 6, 714–724. [Google Scholar] [CrossRef]
- Guerrero-Zacarías, M.C.; Gutiérrez-Enríquez, S.O.; Terán-Figueroa, Y. Factibilidad para implementar un sistema electrónico de registros de citología cervical. Rev. Enferm. Inst. Mex. Seguro. Soc. 2020, 28, 92–101. Available online: http://www.revistaenfermeria.imss.gob.mx/editorial/index.php/revista_enfermeria/article/view/991/1060 (accessed on 25 July 2020).
- Dunbar, B. Technology Readiness Level. October. Available online: https://www.nasa.gov/directorates/heo/scan/engineering/technology/txt_accordion1.html (accessed on 2 April 2022).
- Norma Oficial Mexicana NOM-024-SSA3-2010. Que Establece los Objetivos Funcionales y Funcionalidades Que Deberán Observar los Productos de Sistemas de Expediente Clínico Electrónico Para Garantizar la Interoperabilidad, Procesamiento, Interpretación, Confidencialidad, Seguridad y Uso de Estándares y Catálogos de la Información de los Registros Electrónicos en Salud. Diario Oficial de la Federación, 2010. Available online: http://www.dgis.salud.gob.mx/descargas/pdf/NOM-024-SSA3-2010_SistemasECE.pdf (accessed on 22 August 2022).
- Norma Oficial Mexicana NOM-024-SSA3-2012 Sistemas de Información de Registro Electrónico para la Salud. Intercambio de Información en Salud. Available online: https://dof.gob.mx/nota_detalle.php?codigo=5280847&fecha=30/11/2012 (accessed on 2 April 2022).
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The use of Electronic Health Records to Support Population Health: A Systematic Review of the Literature. J. Med. Syst. 2018, 42, 214. [Google Scholar] [CrossRef] [PubMed]
- Cifuentes, M.; Davis, M.; Fernald, D.; Gunn, R.; Dickinson, P.; Cohen, D.J. Electronic Health Record Challenges, Workarounds, and Solutions Observed in Practices Integrating Behavioral Health and Primary Care. J. Am. Board Fam. Med. 2015, 28 (Suppl. 1), S63–S72. [Google Scholar] [CrossRef] [PubMed]
- Akhu Zaheya, L.; Al Maaitah, R.; Bany Hani, S. Quality of nursing documentation: Paper-based health records versus electronic-based health records. J. Clin. Nurs. 2018, 27, e578–e589. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Yu, P.; Hailey, D. Description and comparison of documentation of nursing assessment between paper-based and electronic systems in Australian aged care homes. Int. J. Med. Inform. 2013, 82, 789–797. [Google Scholar] [CrossRef]
- Kuziemsky, C.E.; Andreev, P.; Benyoucef, M.; O’Sullivan, T.; Jamaly, S.A. Connectivity Framework for Social Information Systems Design in Healthcare. AMIA Annu. Symp. Proc. 2017, 10, 734–742. [Google Scholar] [PubMed]
- Palma Pinedo, H.; Reyes Vega, M. Barreras para la calidad de información en establecimientos de salud de la Amazonía: El caso de tres sistemas de información de VIH/Sida, hepatitis B y sífilis congénita. Perú. Rev. Peru. Med. Exp. Salud Publica 2018, 35, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Aalsma, M.C.; Schwartz, K.; Haight, K.A.; Jarjoura, G.R.; Dir, A.L. Applying an Electronic Health Records Data Quality Framework Across Service Sectors: A Case Study of Juvenile Justice System Data. eGEMs 2019, 11, 26. [Google Scholar] [CrossRef]
- Tomines, A.; Readhead, H.; Readhead, A.; Teutsch, S. Applications of electronic health information in public health: Uses, opportunities & barriers. eGEMs 2013, 1, 1019. [Google Scholar] [CrossRef]
- Harron, K.; Wade, A.; Gilbert, R.; Muller-Pebody, B.; Goldstein, H. Evaluating bias due to data linkage error in electronic healthcare records. BMC Med. Res. Methodol. 2014, 14, 36. [Google Scholar] [CrossRef]
- Ovies Bernal, D.P.; Agudelo Londoño, S.M. Lecciones aprendidas en la implementación de sistemas nacionales de información de salud interoperables: Una revisión sistemática. Rev. Panam. Salud Publica 2014, 35, 415–423. Available online: https://www.scielosp.org/pdf/rpsp/v35n5-6/17.pdf (accessed on 22 August 2022). [PubMed]
- Jamieson, T.; Ailon, J.; Chien, V.; Mourad, O. An electronic documentation system improves the quality of admission notes: A randomized trial. J. Am. Med. Inform. Assoc. 2017, 24, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Wagner de Almeida, S.R.; Marcon Dal Sasso, G.T.; Carvalho Barra, D.C. Computerized nursing process in the Intensive Care Unit: Ergonomics and usability. Rev. Esc. Enferm. USP 2016, 50, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Montgomery, D.C.; Philpot, L.M.; Barnes, S.A.; Compton, J.; Kennerly, D. Development of a Tool to Measure User Experience Following Electronic Health Record Implementation. J. Nurs. Adm. 2014, 44, 423–428. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Functionality Criteria | Compliance Description |
|---|---|
| Authentication. | The system requests a username and password. |
| Application for diagnostic assistants. | Allows the request for analysis by the pathologist. |
| Clinical communication support. | Maintains communication flows between personnel involved in the cervical screening process. |
| Capture, administer, and review clinical information. | Create a unique record for each patient with the option to update the information. |
| Patient demographic data management. | It stores the identification and demographic data of each patient, with the possibility of identifying it during any interaction in the care process. |
| Problem list management. | Displays diagnostic reports to follow up on patients. |
| Registration, update, and administration of the patient’s medical history. | Validates the filling of mandatory minimum information, and provides updated information. |
| Patient Directory. | It has a database of identification and location of patients. |
| Measurements, monitoring, and analysis. | Complies with the Official Mexican Standards regarding health information and CC. |
| Reports generation. | It allows for the creation of electronic reports for the clinical and administrative decision-making process. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Enríquez, S.O.; Guerrero-Zacarías, M.C.; Oros-Ovalle, C.; Terán-Figueroa, Y.; Acuña-Aradillas, J.M. Computer System for the Capture and Preparation of Cytopathological Reports for Cervical Cancer Detection and His Utility in Training for Health Personnel. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1323-1333. https://doi.org/10.3390/ejihpe12090092
Gutiérrez-Enríquez SO, Guerrero-Zacarías MC, Oros-Ovalle C, Terán-Figueroa Y, Acuña-Aradillas JM. Computer System for the Capture and Preparation of Cytopathological Reports for Cervical Cancer Detection and His Utility in Training for Health Personnel. European Journal of Investigation in Health, Psychology and Education. 2022; 12(9):1323-1333. https://doi.org/10.3390/ejihpe12090092
Chicago/Turabian StyleGutiérrez-Enríquez, Sandra Olimpia, Miriam Celeste Guerrero-Zacarías, Cuauhtémoc Oros-Ovalle, Yolanda Terán-Figueroa, and Jorge Martín Acuña-Aradillas. 2022. "Computer System for the Capture and Preparation of Cytopathological Reports for Cervical Cancer Detection and His Utility in Training for Health Personnel" European Journal of Investigation in Health, Psychology and Education 12, no. 9: 1323-1333. https://doi.org/10.3390/ejihpe12090092
APA StyleGutiérrez-Enríquez, S. O., Guerrero-Zacarías, M. C., Oros-Ovalle, C., Terán-Figueroa, Y., & Acuña-Aradillas, J. M. (2022). Computer System for the Capture and Preparation of Cytopathological Reports for Cervical Cancer Detection and His Utility in Training for Health Personnel. European Journal of Investigation in Health, Psychology and Education, 12(9), 1323-1333. https://doi.org/10.3390/ejihpe12090092