Abstract
This study aims to investigate the potential scope of rural bioenergy production from the valorisation of non-hazardous waste, particularly from institutional health and family planning facilities. A crude bioenergy production potential will be determined, as well as relevant interrelationships with food security, equality and inclusivity, poverty reduction, and their contribution to achieving sustainable development goals (SDGs). Solid waste generation at LAMB Hospital in Bangladesh was assessed. Its energy yield capacity and replacement of conventional, inefficient fuel sources were estimated, analysed, and specified. Results showed that the biogas yield capacity of non-hazardous solid waste from the LAMB hospital is 62 m3, which is equivalent to the gas required to cook 31 family meals. From small-to-medium institutes, such as the LAMB hospital, derived waste has the capacity to meet the cooking energy demand of rural villages. The electrical yield capacity of this amount of gas is 124 kWh, and this amount of energy can replace the use of 41 tonnes of firewood that cause emissions, deforestation, and increases the propensity for flooding. The adoption of Anaerobic Digestion (AD) for biogas production also has an impact on waste management, stimulating improved governance and infrastructure and supporting agriculture through the production of nutrient-dense biofertiliser. Further analysis showed that biogas not only provides a clean and affordable fuel but, in turn, has benefits with regard to health issues. Emissions from traditional cooking fuels have deleterious impacts on health due to Indoor Air Pollution (IAP), which generally affects women to a greater extent. All of these factors contribute to achieving sustainable development goals. This study could help to reduce environmental pollution from the health sector and mitigate climate change impacts, and there is a potential for scaling up this study nationwide.
1. Introduction
An estimated 1.1 billion people (14% of the global population) do not have access to electricity, according to Energy Access Outlook [1] Additionally, significant numbers of people suffer limited energy access. Around 84% of those without electricity are based in rural areas, and more than 95% of those living without electricity are in countries in sub-Saharan Africa (SSA) and South Asia. According to research from World Bank [2], thirteen countries in Sub-Sahara Africa have less than 25% access to electricity, compared to only one in developing Asia [2]. Economic growth in Sub-Saharan Africa was estimated to be approximately 2.8% in 2018, which is relatively low compared to South Asia at 7.1% [3]. Limited access to energy also has a significant impact on wider sustainable development as well as economic growth [4]. More than 2.8 billion people, mainly in South Asia and Sub-Saharan Africa (38% of the world’s population), lack access to clean cooking systems, and commonly use inefficient stoves or open fires in poorly ventilated spaces [1]. Bangladesh is a country in South Asia that has a deficiency of clean and affordable cooking fuel. Bioenergy generation from waste biomass could provide some of the energy needs of rural people in this country. Bangladesh is still a Lower Medium Income Country (LMIC) with substantial poverty, inequality, and deprivation. The efficacy of rural bioenergy projects and their impacts on poverty alleviation can be measured using socioeconomic indicators. Different types of waste could be potential raw material sources for energy generation, including in the health sector. Worldwide, there is a huge deficiency of basic medical waste management services, and a WHO report [5] shows that 9 out of 10 hospitals in Bangladesh and 1 out of 3 hospitals globally have a lack in waste management. This paper describes a socioeconomic impact assessment of the adoption of a small-scale bioenergy project in Bangladesh from health-related sources, using LAMB hospital as an example. The analysed results provide indicators that relate to sustainable development goals and indices. The indicators and sources of the health and family planning sector in Bangladesh are shown in Table 1.

Table 1.
Indicators and sources of the Health and Family Planning Sector in Bangladesh.
Management of health-related hospital waste remains problematic in developing countries such as Bangladesh. The main reason for this is the lack of relevant legislation/regulation as well as limited waste management facilities. There is also a lack of awareness, and at the same time, the density of the population is very high. Data pertaining to the scale and nature of this problem in a specific region of Bangladesh (Jessore District) is illustrated in Table 2.
Table 2.
Difficulties of health-related waste management in Jessore City, Bangladesh [7].
1.1. The Key Feature of the Health Sector in Bangladesh
Worldwide 5.2 million people, including 4 million children, die due to medical waste-related diseases [8]. Medical waste can be surgical, toxic chemicals, old medicines, needles/sharps, etc. For this study, the focus is on non-hazardous, organic waste materials such as outdoor dressing, protective clothing like masks, plaster, and similar waste. For developing countries like Bangladesh, the rapid growth of urban populations has resulted in multiple challenges: lower educational status, widespread health problems, and higher levels of environmental pollution [9]. HCWM (Health Car Waste Management). These all present key challenges for health facilities in developing countries, with surrounding populations and staff directly related to health care are frequently exposed to risk due to the poor management of waste [10]. The improper management of medical waste can also cause severe pollution and contamination of air, soil, and both ground and surface water. Globally, hospital waste is considered a hazardous material, and, therefore, it must be treated accordingly [11]. Furthermore, hospital waste management remains a concern due to the lack of knowledge and awareness of appropriate treatment options for those wastes. It is, therefore, important to manage and process healthcare waste in an efficient way. One option is to valorise organic waste to produce energy and biofertiliser via a sustainable energy conversion process called Anaerobic Digestion (AD). The Infrastructural Company Limited (IDCOL) in Bangladesh are facilitating a national biogas program under their renewable energy (RE) program and has the opportunity to better understand and support the health sector (Figure 1).
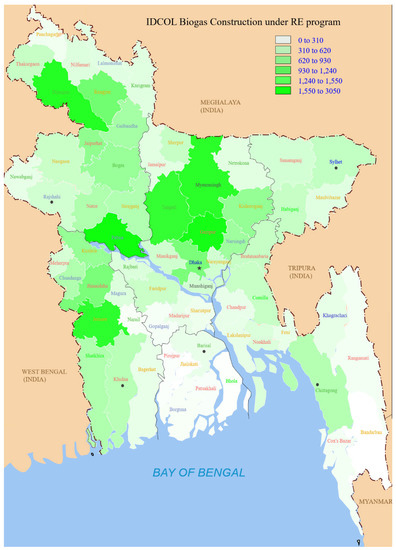
Figure 1.
IDCOL Biogas Construction under the Renewable Energy program.
The FAO [12] has estimated the annual per capita food waste (FW) production in developing countries at the consumer level to be 6–11 kg, as compared with 95–115 kg in developed countries [13]. The per capita total annual FW in South and South-East Asia was estimated to be about 125 kg, of which 110 kg was found as losses during production to retailing, with the remaining 15 kg of loss occurring during consumption [13].
In this study, waste management practices and the current scenario of LAMB hospital will be highlighted to understand the potential bioenergy yield capacity of a hospital in Bangladesh.
1.2. Hospital Waste Management
According to the Bureau of Statistics Bangladesh [6], there are 460 upazila (sub-district) level Hospitals, 9722 community-level clinics, and about 1449 outdoor health facilities at the Union level that falls under the Directorate General of Health Service (DGHS) Bangladesh. The increased number of clinics and hospitals in Bangladesh means an increased amount of waste generation. The findings from a survey from an upazila in the Jessore District in Bangladesh have calculated the amount of medical waste produced from medical services. The average waste generation rate was 37.11 kg per hospital, 1.56 kg/bed/day, and 1.90 kg/patient/day. Hazardous waste was recorded at 9.71%, and non-hazardous waste at 90.29%. Medical waste consists of eight categories of waste materials, with vegetables and food being the largest component (74%) [10,14]. However, proper quantification and management are always a big challenge in most developing countries such as Bangladesh.
Hospital waste contains toxic chemicals and hazardous materials from several diagnostic and treatment processes. The present waste disposal system of Bangladesh is unhygienic and unsafe, and it is important to identify and develop improved processes for waste management. The knowledge level of hospital staff on the harmful impacts of improper waste disposal was also very low based on a preliminary assessment of their waste management practice. Implementation of rules, regulations, and laws regarding hospital waste management is recommended, with an emphasis on raising awareness, improving waste handling practices, and improving disposal technologies and systems (Figure 2).

Figure 2.
A dumping ground in Parairchawk of Sylhet, where medical waste is mixed with other wastes Untreated medical waste: A serious threat to public health [15].
This study aimed to investigate the potential scope of rural bioenergy and considers aspects of public health, waste, and energy management from the health sector (which is an untouched sector in the aspect of energy generation) and sustainable development goals.
1.3. LAMB Hospital
The hospital run by Lutheran Aid to Medicine Bangladesh (LAMB) community hospital is situated in Diajpur, in rural Northwest Bangladesh (Figure 3). Providing healthcare and other services to 700,000 impoverished people in the surrounding community [16]. The hospital occupies about 5 hectares, including 150 beds, a school and training centre, other departments, and staff residences. The various buildings generate waste which is presently either dumped, burned, or incinerated.

Figure 3.
LAMB Hospital Dinajpur, Northern part of Bangladesh.
It is a general hospital offering both in-patient and out-patient care with diagnostic services (shown in Figure 4). It also runs 16 healthcare centres in the area around the hospital. LAMB also provides technical support to 126 family welfare centres and 231 community clinics run by the Government of Bangladesh. It has a large health-focused training centre with nine classrooms and residential accommodation for trainees. The hospital caters to a population of around 1.5 million, with the wider community health and development programs helping a population of around 5.7 million.
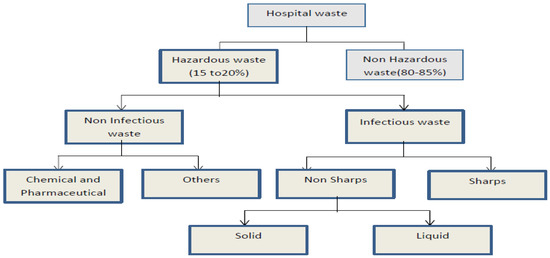
Figure 4.
Categories of hospital waste [17].
The World Health Organization (WHO) divides hospital waste into hazardous and non-hazardous categories (Figure 4). Recycling hazardous waste, such as medical waste, is not viable due to the potential health risks. The non-hazardous part of the waste is suitable for recycling as well as for recovering energy (AD) from the waste. Capacity building and waste management education programs need to be implemented before medical waste can be managed in an environmentally sound manner.
2. Background Research
2.1. Waste and Sustainable Energy Sources
The demand for energy is growing rapidly in Bangladesh, with a 3.3% urban growth rate and a 1.4% national population growth rate. Urban expansion has led to a rising demand for wood fuel, which results in deforestation and a steady loss of arable lands. These, in turn, may result in future food shortages [18]. Conditions that exist when people have physical and economic access to sufficient safe and nutritious food can mean they have an active and healthy life [19]. Many factors that affect access to food resources include availability, stability, accessibility, and use of food. These also include distributional and contextual issues that also affect people’s vulnerability and hunger [20]. As the world challenges climate change, demand will increase for both bioenergy and sustainable food sources. The potential for producing bioenergy from institutional sources, for example, school and hospital, is an old practice in many South Asian countries, for example, India [21], and have similar scope to Bangladesh having many similarities in practice, culture, need, and demand.
Bioenergy and Sustainable Development Goals (SDGs)
Five basic ethical issues related to biofuel production include Human Rights, Environmental Sustainability, Climate Change, Just Rewards and Rights for People, and Equitable costs and benefits [22]. Sustainability standards for biofuels will include guidelines for environmentally and socially acceptable production and distribution. To exploit the full potential of biofuels, policies need to be justified [23]. Ethics and Environmental/Engineering Environmental ethics would be an important subject to consider while working with biogas production from an anaerobic digestion system of hospital waste. The main reason is the raw materials involved with this system have some management and technological issues and could thread to the plant and animals. To consider a better waste management practice in a hospital, it is very important to emphasise sustainability-related challenges, for example, health and safety, supply chain management, and policy. Biogas generation from waste biomass through anaerobic digestion (AD) could be a sustainable solution as it produces a clean cooking fuel as well as mitigates environmental pollution from smoke. An installation of a bioenergy plant from waste could be a potential indication of achieving sustainable development goals, for example, SDG 6, 7, 9, 12, and 15 [24]. Sustainable waste management should be dealt with through a complete approach to draw the consideration of legislators and facilitate the deployment of resources. An upgrading in waste management, generating biogas from waste can foster, for example, the attainment of SDG 11 (Sustainable Cities and Communities) and help achieve other goals such as SDG 7 (Affordable and Clean Energy) [25].
As a developing country, Bangladesh is committed to achieving the UN’s Sustainable Development Goals. Improved management and valorisation of hospital waste via an energy recovery process such as AD would go some way towards achieving sustainability and meeting the country’s SDG targets.
2.2. Biomass Cooking and Biogas Cooking
Around 80% of Bangladesh’s population relies on solid fuel for their household cooking and heating needs. Products from the incomplete combustion of firewood cause indoor air pollution and increase the propensity to diseases, such as pneumonia and other acute lower respiratory infections and chronic obstructive pulmonary diseases [26]. Coal and kerosene are two commercial fossil fuels that are the most common fuels used for cooking, contributing to climate change, and are expensive to use [27,28]. If biogas is generated and produced from biomass resources, such as dung, then the heating efficiency is about 60% [29,30]. In comparison, burning a ton of straw in traditional burners will reportedly produce 3 kg of particulate matter, 60 kg of carbon monoxide, 1460 kg of carbon dioxide, 199 kg of dust, and 2 kg of sulfur dioxide [31,32]. These gases play an important role in affecting the atmosphere and environment, which leads to global climate change [32]. In particular, the elements can also easily invade the lungs causing respiratory disease, especially for children and patients with asthma. Additionally, incomplete combustion produces carbon monoxide and carcinogenic hydrocarbons, which could cause cancer [33].
A comparison of current and future cooking fuel use has been compared and is shown in Figure 5 the comparison of their impact in terms of global warming potential (GWP) and health impact.
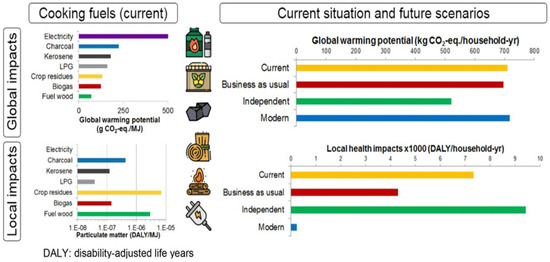
Figure 5.
Environmental sustainability of cooking fuels in remote communities [34].
In rural areas, biogas is used most commonly for cooking and lighting purposes and replaces the use of wood biomass. The low efficiency of combustion in open fires (approximately 14%); [35] suggests that much of the energy in the wood is wasted. Biogas is an environmentally friendly cooking gas produced by anaerobic digestion and is a better solution for household cooking that reduces pollution and reduces the impact associated with the inefficient burning of biomass. In Bangladesh, waste from institutions such as hospitals is a possible source of biomass and bioenergy recovery from this sector. Other institutions that could generate their own energy from biomass wastes include schools, colleges, and universities. To use the hospital waste as biogas feedstock, it is very important to have segregation of waste in practice.
3. Methodology
The study includes a literature review of current waste management practices surrounding hospital wastes (both in Bangladesh and globally). A review of waste management practices has been conducted at a particular hospital, including an analysis of the waste composition, collection method, and sustainability analysis of potential options. An assessment was also made of traditional biomass-based cooking and biogas cooking. A preliminary review was carried out to determine the data/information gap. This was followed by the main studies to obtain key information. Each of the methods used to obtain the secondary data are described below, as is the normalization of the data.
3.1. Literature Review
The literature on biomass, bioenergy, waste management, Institutional waste, and Sustainable Development Goals (SDGs) were reviewed. Different waste management and waste collection processes and scenarios were viewed and analysed. Informal waste collection approaches were observed in Dhaka City. Moreover, the waste management used by different institutes, their waste management activities, and practices were recorded. Waste pickers in many developing countries such as Bangladesh (locally called “Tokai”) are mainly women and children (10–15 years old) who are at high risk of health hazards, for example, due to contamination, infectious diseases, and disease vectors (Figure 6).

Figure 6.
Waste pickers in Asian countries are at a high risk of health hazards.
3.2. Development Studies on Anaerobic Digestion and Biogas
Visits were made to biogas and anaerobic digestion expert organizations, including Grameen Shakti (GS), Advance Engineering, Practical Action, German Development Organization (GIZ/KfW), Netherland Development Organization (SNV), Bangladesh Council of Scientific and Industrial Research (BCSIR) and Department of Livestock Services (DLS). Contact has been made some key people/organisations in case any information and data gaps.
Activity in Different Supply Chain Steps
There are several aspects that are related to using biomass waste materials to generate energy for institutions, such as hospitals, and these are listed below:
- Sustainable waste management solutions for community hospitals in Bangladesh
- Waste collection and segregation at the source
- Manual segregation
- Chopping/grinding/maceration
- Inlet of anaerobic digester
- Anaerobic digester
- Biogas production
- Gas use/distribution
3.3. Evolution of Biogas Bangladesh—The Key Stakeholders Studies
Biogas technology has been used in Bangladesh since 1972. To date, about 100,000 biogas plants have been built in the country by different organizations. According to experts, the country has the potential to construct 4 million biogas plants. Infrastructure Development Company Ltd. (IDCOL) launched its biogas program in 2006 with financial support from SNV in the Netherlands and KfW (Figure 7). Subsequently, other donors have become involved, such as GIZ, ADB, World Bank, JICA, etc. IDCOL is implementing the project through 48 partner organizations (POs) that build the digesters. To raise awareness among the common people, the POs organise orientation meetings. To attract farmers, a subsidy is provided. To reduce the initial investment, IDCOL also provides soft loans of up to 85% of the cost. However, in many cases, the loan recovery rate is highly discouraging. To accelerate the pace of progress, ensure a 100% success rate and 100% loan recovery rate, and ensure sustainability, an approach called the ‘Village Approach’ has been adopted as an appropriate solution. The model may be widely replicated, not only in Bangladesh but also in other developing countries of the world. The village approach focuses on the concentration of activities in a limited area. This helps economic and efficient monitoring and supervision of work. In this system, all supervisors and technicians are recruited locally and trained properly. This ensures after-sale services, even after the project period, and, thus, ensures sustainability.

Figure 7.
Sand Cement Brick—Fixed dome anaerobic digester Bangladesh.
3.4. Waste and Energy (Energy Estimation)
A survey of the waste streams from the LAMB hospital of solid non-hazardous biomass waste per day has been investigated. If waste from a few tea stalls and small food processing businesses in a 1-mile radius of LAMB hospital, another 200 kg of solid waste were estimated to be available. Solid waste includes kitchen waste, food waste, fruit and vegetable residue, and packaging waste. This means the LAMB site, as a community hospital including its closest sources, has the potential to generate 500 kg of solid waste a day (of which 95% of them is biomass). This waste has the potential to generate energy and organic fertiliser [36]. Only the waste data were collected from the LAMB authority as primary resources, but the calculation of waste to biogas yield and its energy yield has been calculated/and collected from secondary resources [9].
4. Results and Discussions
The analysis of an energy-from-waste project must first include an estimate of the energy that could be made available. It also needs to consider the sustainability of such as project and its impact on issues such as gender equality and social inclusion.
A survey of the waste streams from LAMB hospital suggests a total of 300 kg of solid non-hazardous biomass waste is available per day. Tests have shown that biogas production from municipal solid waste is 0.125 m3/kg [37]. Standard figures for Bangladesh show that the household cooking energy requirement by a family of five people is 2 m3 of biogas. The electrical energy that can be generated from 1 m3 of biogas is estimated at 2 kWh. It is suggested that the generation of a minimum of 75 kWh of electrical power is considered cost-effective for an institution such as a hospital. This suggests a biogas plant needs to yield 37 m3 of biogas a day to be economically viable. A domestic-sized biogas plant can be estimated to produce 3.2 m3 of biogas per day, which corresponds to approximately 80 MJ of energy per day. Assuming that the calorific value is 15.5 MJ/kg for wood and 43 MJ/kg for kerosene [38], this digester would replace 1.9 tonnes of fuel wood or 632 kg of kerosene per year [9].
The biomass waste from LAMB hospital could generate 62 m3 of biogas, equivalent to the gas required to cook meals for 31 families of 5 people. This suggests that biomass waste from an institution of the size of LAMB has the capacity to meet the cooking requirement of 155 people (Table 3). This would replace the use of 41 tonnes of firewood, reducing not only polluting emissions but also deforestation, thus, increasing the potential for food generation.
Table 3.
Biogas yield potential of waste and its energy estimation.
There are 460 upazila (sub-district) level Hospitals, 9722 community-level clinics, and about 1449 outdoor health facilities in Bangladesh. A scale-up of this could ensure a significant increase of energy as well as improve pollution and waste management.
4.1. Bioenergy and Sustainability
Aspects that need to be considered when assessing the sustainability of a bioenergy project are land use, land use change, greenhouse gases, biodiversity, air quality, productivity, social well-being, energy security, trade, profitability, resource conservation, and social acceptability [39,40]. Resource management practices are more important than crop type in determining environmental impacts [41]. Wise management of available resources supports both bioenergy sustainability and food security [42]. An analysis of interactions among resource management, bioenergy sustainability, and food security is discussed first in terms of paired interactions, followed by a consideration of a three-way nexus. A sustainability impact assessment suggests that there is a viable impact on waste management, food security (from the generation of compost), and bioenergy sustainability. This nexus requires good governance, effective infrastructure, reliable technology, integrated crop management, effective ecosystem services, and social services (Figure 8).
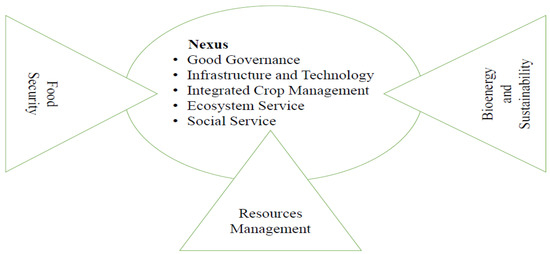
Figure 8.
The nexus of resource management, bioenergy sustainability, and food security.
4.2. Sustainable Development Goals (SDGs)
After the completion of the Millennium Development Goals (MDGs), the ‘Sustainable Development Goals’ (SDGs) were defined by the United Nations Conference on Sustainable Development in 2015 and included the planet, the people, sustainable energy, economy, justice, equity, and partnership. Leaders from 193 countries solidly adopted the post-2015 agenda for international development for the period of 2015–2030. There are 17 goals (shown in Figure 8) that have 169 targets. These SDGs are characterised by an agenda including ending poverty and eliminating its root causes, tackling the adverse effects of climate change, fighting disparity, and ensuring a sustainable future for all [43]. The ultimate goals of SDGs help achieve environmental sustainability, which helps to improve the future lives of citizens. It helps to deal with the impacts of climate change, eliminate poverty through attaining gender equality and improved health and construct an inclusive society, which will help to reduce disparities and help economic progress [43].
Goal 5 states: achieve gender fairness and empower all women and girls. The reduction in gender inequality increases the empowerment of women and children. Women’s and children’s access to basic needs such as energy, land, water, and food form the basis of sustainable production and consumption. The Bangladesh government has defined a vision to provide affordable and reliable electricity for all by 2021 [44]. This is inspired by SDG 7: ensure access to affordable, reliable, sustainable, and modern energy for all. This includes a target that by 2030, the share of renewable energy in the global energy mix should be substantially increased. Sustainable modern energy fuels development, such as providing light to allow human beings to conduct their work. Universal access requires energy to be affordable and reliable. Generating energy must not irreversibly harm the environment.
Sustainable Development Goal 7: Affordable and Clean Energy
Sustainable Development Goal 7 is one of the 17 goals which has been established by the United Nations in 2015. The aim of this goal is to ensure clean, affordable, and sustainable modern energy for all (Figure 9).
Figure 9.
United Nations Sustainable Development Goals (SDGs).
4.3. Sustainable Development Goals (SDGs) and Human Development Index
UN member states are finalizing the sustainable development goals that will replace millennium development goals (MDGs). The idea of the SDGs has quickly gained ground because of the growing urgency of sustainable development for the entire world. Sustainable engineering should try to balance technical excellence, economic feasibility, ethical maturity, and cultural sensitivity. The implementation of a community-based rural AD or bioenergy project could be regarded as a way to use engineering to help people who are in poverty (Figure 10). This research shows that AD can help rural people in their daily lives. The SDGs provide a better tool to test the effectiveness of such a project than the old MDGs. Using SDGs also provide data that allow the project to be assessed in terms of measures such as the Human Development Index (HDI) and Multidimensional Poverty Index (MPI).
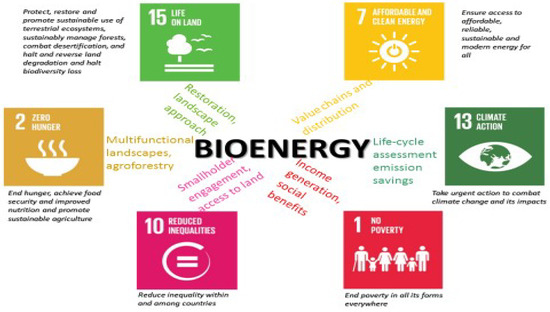
Figure 10.
Bioenergy and its influence on different goals.
4.4. Waste to Biogas and Sustainable Development Goals (SDGs)
The Sustainable Development Goals for 2030 proposed by the Open Working Group includes Goal 5, which states, “Achieve gender equality and empower all women and girls”. Goal 5 includes measures relevant to the energy sector, including ending all discrimination against women and girls, recognise and valuing unpaid care and domestic work through the provision of infrastructure, ensuring women’s effective participation and equal opportunities, and enhancing the use of enabling technologies. The use of a waste-to-energy biogas system reduces the workload of women and children by providing a more effective way to cook food (Table 4).
Table 4.
A summarization of integrated goals and index and the stands of bioenergy.
Goal 7 states: “Ensure access to affordable, reliable, sustainable, and modern energy for all”. By 2030, the targets are to ensure universal access to affordable, reliable, and modern energy services. By 2030, increase substantially the share of renewable energy in the global energy mix.
4.5. Bioenergy and Biofertiliser—Gender and Social Inclusion
Anaerobic Digester technology is generally classified as (a) Floating Dome Model, (b) Fixed Dome Model, and (c) Bag type.
In Bangladesh, the sizes of biogas plants are generally expressed in terms of the volume of gas produced per day.
- Small-size biogas plants are 1.2, 1.6, 2.0, 2.4, 3.2, and 4.8 m3 gas production per day.
- Medium-size biogas plant varies from 6 to 25 m3 of gas production per day.
- The large-size biogas plant is 26 m3 gas production per day to 200 m3 gas production per day and above (SNV, IDCOL).
In an on-site biogas plant on hospital premises, an engagement of rural women in biogas is not that much of a common scenario; however, an expansion of this program to the village could increase the scope of women’s engagement in the biogas program. Considering the potential role of women in the biogas program, it should be well understood that:
- Adoption of technology will be most effective if local village women are involved in motivating others; and
- The involvement of women would be greater if mobilised through village-level institutions; however, instead of creating new institutions, the focus should be on using institutions like Mother’s groups.
4.6. Challenges for Environmental Sustainability
It is always a challenge to ensure environmental sustainability in Bangladesh due to having both internal and external factors related to this issue. For example, agricultural practice/framing is an important sector causing greenhouse gas emissions. Land use, land use change, and forest, as well as sustainable waste management, can help to reduce GHG emissions from sustainable farming [45]. Another SDG 11 is for building sustainable cities and communities [46], and a number of sustainable issues are related to this goal. The most vital concern related to environmental sustainability is anthropogenic climate change [47,48]. It is now internationally recognised that Bangladesh is an innocent victim of climate change, and they are affected from beyond their boundaries.
4.7. Wider Impacts of Bioenergy
4.7.1. Economic Benefit
Sustainable hospital waste management reduces environmental pollution and waste transportation cost. Biogas is a clean and affordable fuel that can replace biomass firewood use and kerosene used for lighting. Community biogas facilities can save money on fuel costs.
4.7.2. Social Impact
By tradition, women in rural developing countries are mainly responsible for cooking for all members of a family as well as childcare. Inefficient biomass-based cooking systems cause adverse impacts on rural women and children. Biogas cooking save time, and this could, directly and indirectly, help to improve rural lifestyle and well-being. These also help to enhance child and women’s education, employability, and women’s empowerment. Illnesses from cooking and lighting fuel are estimated to cause the deaths of more women in many rural developing countries (such as Kenya, Bangladesh, and Nepal) than both malaria and tuberculosis [49]. The use of kerosene lanterns frequently leads to accidents where houses burn down after a lamp falls.
4.7.3. Environmental Impact
The energy crisis, the depletion of fossil fuels, global warming, and climate change are growing concerns worldwide and especially South Asia and sub-Sahara Africa. To cope with this situation the role of bioenergy could play a vital role in meeting energy demands. Clean energy sources, such as biogas, can solve the energy crisis problem to a great extent. Used 4 h per day, a kerosene lamp emits 100 kg of CO2 annually and 100 kg of CO2 is produced from burning 28.9 kg of kerosene [50]. Comparing these research results can prove that the GWP of kerosene and biogas are similar per unit of energy.
4.7.4. Regional Impact
Biogas and biogas-based electricity can save time as well as reduce energy costs for the LAMB hospital, as well as providing clean and affordable fuel (SDG7). Women will be benefitted in the region (SDG5) and enhance their lifestyle and well-being. It might help in industry, innovation, and infrastructure (SDG 9) through the expansion of the biogas sector in Bangladesh.
4.7.5. Energy, Gender, Health, and Climate
The program directly addresses several SDGs; contribution towards SDG 7 (Affordable and Clean Energy) is being made through the installation of biogas plants, which replaces the usage of firewood. Reduction of environmental pollution is directly contributing towards SDG 3 (Good Health and Well Being) and SDG 13 (Climate Action). The women who use biogas plants need less time for collecting fuel and cooking, which enables them to look after the education of the children and engage in economic activities, which contributes to achieving SDG 4 (Quality Education) and SDG 5 (Gender Equality).
5. Conclusions
Small-scale bioenergy projects are affordable, freeing time, empowering rural people, and accessible to the poor. Bioenergy replaced incompetent traditional fuel use and provided an improvement in efficiency, which saved time. This allows an increase in earned income or other quality-of-life benefits. This has economic, social, and environmental benefits and also maximises the benefits in terms of education and health. To make biogas technology more affordable, one of the major efforts would be to provide credit to spread loan periods over a longer period, thereby reducing the size of each payment. Microfinance is a tool widely applied in the bioenergy program in rural Bangladesh and has an impact on society. The installation of a small-unit rural bioenergy project could be an important tool for poverty alleviation in developing countries. The use of bioenergy enhances the Human Development Index (HDI) through its potential use. The interaction of bioenergy showed that it has a good nexus with clean fuel, health, emission, climate change, women’s equality, and social inclusion, which means these all help towards achieving a few sustainable development goals. For planning and policy-making, various impact assessments, such as EIA, SEA, or in general sustainability assessment, need to be conducted to inform where and how much the potential impacts are to achieve this goal. Scale up of this research would help to archive the UN’s Sustainable development goals and, at the same time, will help to reduce environmental pollution and contamination.
Limitations and Recommendations for Future Work
This study investigated the bioenergy capacity of a hospital, and it is possible to scale this study up to determine the energy capacity of thousands of hospitals in Bangladesh. As the literature and information from primary sources were collected during the pandemic, it was very difficult to collect data in person. There is scope to scale up this research countrywide in the health sector.
Author Contributions
Conceptualization, K.M.R. and L.M.; methodology, K.M.R.; investigation, K.M.R.; resources, K.M.R.; data curation, K.M.R. and L.M.; writing original draft preparation, K.M.R. and L.M.; writing—review and editing, K.M.R. and L.M.; supervision, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
A list of reference has been included and for any further data gap LAMB Hospital Bangladesh and some key organisation for example IDCOL, BCSIR, BBDF and BGEF.
Conflicts of Interest
The authors declare no conflict of interest.
References
- EAO. WEO-2017 Special Report: Energy Access Outlook—From Poverty to Prosperity; International Energy Agency: Paris, France, 2017. [Google Scholar]
- World Bank. Open Access Datasets. 2018. Available online: https://data.worldbank.org/indicator/eg.elc.accs.zs (accessed on 5 January 2023).
- IMF. Data Mapper, World Economic Outlook, October 2018. Available online: https://www.imf.org/external/datamapper/NGDP_RPCH@WEO/OEMDC/ADVEC/WEOWORLD/EAQ/APQ/SAQ (accessed on 7 January 2022).
- World Bank. Program-for-Results Information Document (PID); World Bank: Addis Ababa, Ethiopia, 2017. [Google Scholar]
- World Health Organization; United Nations Children’s Fund. Wash in Health Care Facilities: Global Baseline Report 2019; WHO: Geneva, Switzerland; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Bangladesh Bureau of Statistics; Bangladesh Borough of Statistics; Statistics and Informatics Division (SID); Ministry of Planning; Government of the People’s Republic of Bangladesh. 2018. Available online: www.bbs.gov.bd (accessed on 4 January 2022).
- Rahman, M.S.; Moumita, C.; Rikta, K. Medical Waste Management System: An Alarming Threat (A Case Study on Jessore Municipality, Bangladesh). J. Environ. Sci. Nat. Resour. 2013, 6, 181–189. [Google Scholar] [CrossRef]
- WHO. The World Health Organization Information on Biohazardous Waste: Safest Methods for Management; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Rahman, K.M.; Melville, L.; Fulford, D.; Huq, S.M.I. Green-house Gas Mitigation Capacity of a Small Scale Rural Biogas Plant Calculations for Bangladesh through a General Life Cycle Assessment. Waste Manag. Res. 2017, 35, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.L.; Uddin, M.J. Medical Waste Management at Upazila Level in Bangladesh. J. Environ. Treat. Tech. 2014, 2, 85–94. [Google Scholar]
- Ross, D.A.C.; Taylor, C.L.; Yaktine, A.L.; Del Valle, H.B.; Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium (Eds.) Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- FAO. An Introduction to the Basic Concepts of Food Security; FAO: Rome, Italy, 2018; Available online: http://www.fao.org/docrep/013/al936e/al936e00.pdf (accessed on 30 March 2022).
- Gustavsson, J.; Cederberg, C.; Sonesson, U.; van Otterdijk, R.; Meybeck, A. Global Food Losses and Food Waste; Food and Agriculture Organization of the United Nations: Rome, Italy, 2011; Available online: http://www.fao.org/docrep/014/mb060e/mb060e.pdf (accessed on 12 July 2015).
- Biswas, A.; Amanullah, A.S.M.; Santra, S.C. Medical Waste Management in the Tertiary Hospitals of Bangladesh: An Empirical Enquiry. Asa Univ. Rev. 2011, 5, 149–158. [Google Scholar]
- The Daily Star. Untreated Medical Waste: A Serious Threat to Public Health. 2020. Available online: https://www.nationthailand.com/news/30377805 (accessed on 5 January 2023).
- Edwards, C.; Saha, S. From home to hospital, a continuum of care: Making progress towards Millennium Development Goals 4 and 5 in rural Bangladesh. BJOG Int. J. Obstet. Gynaecol. 2011, 118 (Suppl. S2), 88–92. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health-Care Waste. 8 February 2018. Available online: http://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 2 February 2022).
- Nahar, K.; Sunny, S.A.; Shazi, S.S. Land Use Requirement and Urban Growth Implications for the Production of Biofuel in Bangladesh. Can. J. Sci. Ind. Res. 2015, 2, 195–208. [Google Scholar]
- FAO. Rome Declaration on World Food Security and World Food Summit Plan of Action. In Proceedings of the World Food Summit, Rome, Italy, 13–17 November 1996. [Google Scholar]
- Von Grebmer, K.; Saltzman, A.; Birol, E.; Wiesmann, D.; Prasai, N.; Yin, S.; Yohannes, Y.; Menon, P.; Thompson, J.; Sonntag, A. 2014 Global Hunger Index: The Challenge of Hidden Hunger; Welthungerhilfe, International Food Policy Research Institute, and Concern Worldwide: Bonn, Germany; Washington, DC, USA; Dublin, Ireland, 2014. [Google Scholar]
- Ashden Award. Biotech—Turning Food Waste into Cooking Gas. 2007. Available online: https://ashden.org/awards/winners/biotech/ (accessed on 10 March 2022).
- Paarlberg, R. Food Politics: What Everyone Needs to Know; Oxford University Press: Oxford, UK, 2010; Chapter 3. [Google Scholar]
- Global Bioenergy Partnership. About GBEP. 2011. Available online: http://www.globalbioenergy.org/ (accessed on 5 January 2023).
- Neto, G.C.d.O.; Leite, R.R.; Lucato, W.C.; Vanalle, R.M.; Amorim, M.; Matias, J.C.O.; Kumar, V. Overcoming Barriers to the Implementation of Cleaner Production in Small Enterprises in the Mechanics Industry: Exploring Economic Gains and Contributions for Sustainable Development Goals. Sustainability 2022, 14, 2944. [Google Scholar] [CrossRef]
- Islam, S. Urban Waste Management in Bangladesh: An Overview with a Focus on Dhaka. In Proceedings of the 23rd ASEF Summer University ASEF Education Department, Virtual, 20 September–15 November 2021; Available online: https://asef.org/projects/23rd-asef-summer-university-asefsu23/ (accessed on 5 March 2022).
- World Health Organization. Report: Indoor Air Pollution, Health and the Burden of Disease; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Gautam, R.; Baral, S.; Herat, S. Biogas as a sustainable energy source in Nepal: Present status and future challenges. Renew. Sustain. Energy Rev. 2009, 13, 248–252. [Google Scholar] [CrossRef]
- Li, H.; Berrens, R.P.; Bohara, A.K.; Jenkins-Smith, H.C.; Silva, C.L.; Weimer, D.L. Testing for budget constraint effects in a National Advisory referendum survey on the Kyoto Protocol. J. Agric. Resour. Econ. 2005, 30, 350–366. [Google Scholar]
- Khandelwal, K.C.; Gupta, V.K. Popular Summary of the Test Reports on Biogas Stoves and Lamps Prepared by Testing Institutes in China, India and the Netherlands; Report; SNV (Netherlands Development Organisation): The Hague, The Netherlands, 2009. [Google Scholar]
- Mirza, U.K.; Ahmad, N.; Majeed, T. An overview of biomass energy utilization in Pakistan. Renew. Sustain. Energy Rev. 2008, 12, 1988–1996. [Google Scholar] [CrossRef]
- Indian Agricultural Research Institute. Crop Residues Management with Conservation Agriculture: Potential, Constraints and Policy Needs; Indian Agricultural Research Institute: New Delhi, India, 2012. [Google Scholar]
- Gupta, R.K.; Garg, S.C. Residue burning in rice-wheat cropping system: Causes and implications. Curr. Sci. 2004, 87, 1713–1717. [Google Scholar]
- Henderick, P.; Williams, R.H. Trigeneration in a Northern Chinese village using crop residues. Energy Sustain. Dev. 2000, 4, 26–42. [Google Scholar] [CrossRef]
- Aberilla, J.M.; Gallego-Schmid, A.; Stamford, L.; Azapagic, A. Environmental sustainability of cooking fuels in remote communities: Life cycle and local impacts. Sci. Total Environ. 2020, 713, 136445. [Google Scholar] [CrossRef] [PubMed]
- Ballard-Tremeer, G.; Jawurek, H.H. Comparison of five rural, wood burning cooking devices: Efficiencies and emissions. Biomass Bioenergy 1996, 11, 419–430. [Google Scholar] [CrossRef]
- Beswetherick, S. Sustainable Solid Waste Management in Bangladesh: A Case Study of a Community Hospital Using Mixed Methods. Master’s Thesis, Cranfield University, Cranfield, UK, 2018. [Google Scholar]
- Vijay, V.K. Biogas Enrichment and Bottling Technology for Automobile Fuel-IIT Delhi Technology—Case Study of Goshalain Rajasthan; Centre for Rural Development & Technology, Indian Institute of Technology Delhi: New Delhi, India, 2012. [Google Scholar]
- Azad, A.K.; Ameer Uddin, S.M.; Alam, M.M. Experimental study of DI diesel engine performance using biodiesel blends with kerosene. Int. J. Energy Environ. 2013, 4, 265–278. [Google Scholar]
- McBride, A.C.; Dale, V.H.; Baskaran, L.M.; Downing, M.E.; Eaton, L.M.; Efroymson, R.A.; Garten, C.T., Jr.; Kline, K.L.; Jager, H.I.; Mulholland, P.J.; et al. Indicators to support environmental sustainability of bioenergy systems. Ecol. Indic. 2011, 11, 1277–1289. [Google Scholar] [CrossRef]
- Dale, V.H.; Efroymson, R.A.; Kline, K.L.; Langholtz, M.H.; Leiby, P.N.; Oladosu, G.A.; Davis, M.R.; Downing, M.E.; Hilliard, M.R. Indicators for assessing socioeconomic sustainability of bioenergy systems: A short list of practical measures. Ecol. Indic. 2013, 26, 87–102. [Google Scholar] [CrossRef]
- Davis, S.C.; Boddey, R.M.; Alves, B.J.; Cowie, A.L.; George, B.H.; Ogle, S.M.; Smith, P.; van Noordwijk, M.; van Wijk, M.T. Management swing potential for bioenergy crops. GCB-Bioenergy 2013, 5, 623–638. [Google Scholar] [CrossRef]
- Manning, P.; Taylor, G.; Hanley, M.E. Bioenergy, food production and biodiversity—An unlikely alliance? GCB-Bioenergy 2018, 7, 570–576. [Google Scholar] [CrossRef]
- Andria, V.H.; Le, J.; Gilman, J.; Manda, P. Steele and Syaifullah. In Towards Sustainable Development Financing in Indonesia: Country Brief; UNDP and the Government of Indonesia: Jakarta, Indonesia, 2014. [Google Scholar]
- Alam, T. A Paradigm Shift in Bangladesh Energy Sector towards SDG-7: A Few Insights of Energy Statistics in Bangladesh; Ministry of Planning, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2016. [Google Scholar]
- Wolf, E.C. Avoiding a mass extinction of species. In State of the World; World Watch Institute, Ed.; W. W. Norton & Company: New York, NY, USA, 1988. [Google Scholar]
- Sachs, J.; Schmidt-Traub, G.; Kroll, C.; Durand-Delacre, D.; Teksoz, K. SDG Index and Dashboards Report 2017; Bertelsmann Stiftung: New York, NY, USA; Sustainable Development Solutions Network (SDSN): New York, NY, USA, 2017. [Google Scholar]
- Intergovernmental Panel on Climate Change. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the IPCC. In Synthesis Report; Core Writing Team, Pachauri, R.K., Meyer, L.A., Eds.; IPCC: Geneva, Switzerland, 2014; 151p. [Google Scholar]
- Brown, L.R.; Young, J.E. (Eds.) Feeding the world in the nineties. In State of the World, 1990; W. W. Norton & Company: New York, NY, USA, 1990. [Google Scholar]
- Bruce, M.C.; Donnelly, C.A.; Alpers, M.P.; Galinski, M.R.; Barnwell, J.W.; Walliker, D.; Day, K.P. Cross-species interactions between malaria parasites in humans. Science 2000, 287, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Raturi, A. CDM and the Pacific Island Countries Opportunities and Challenges USP, Presented at JICA-CDM TV Seminar, Suva. 2008. Available online: http://lrd.spc.int/publications/doc_download/743-fat-raturi-cdm-and-the-pacific-island-countries-compatibility-mode (accessed on 10 October 2022).










Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).