
Designing a Patient Outcome Clinical Assessment Tool for Modified Rankin Scale: “You Feel the Same Way Too”


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Modified Rankin Scale Overview and Related Works
2.1. Current Modified Rankin Scale Collection Process
2.2. Reliability of the Modified Rankin Scale
3. Methods: Online Survey
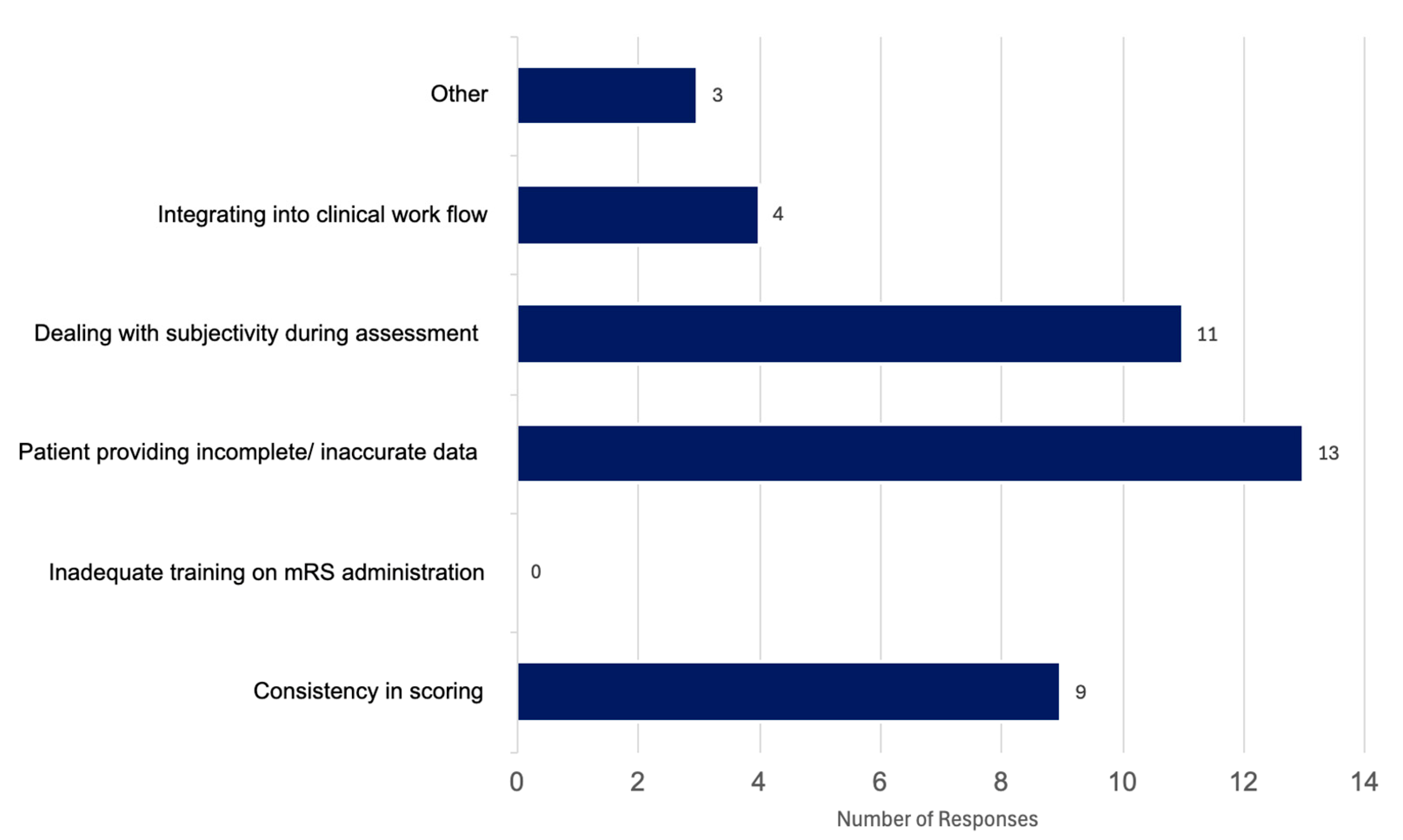
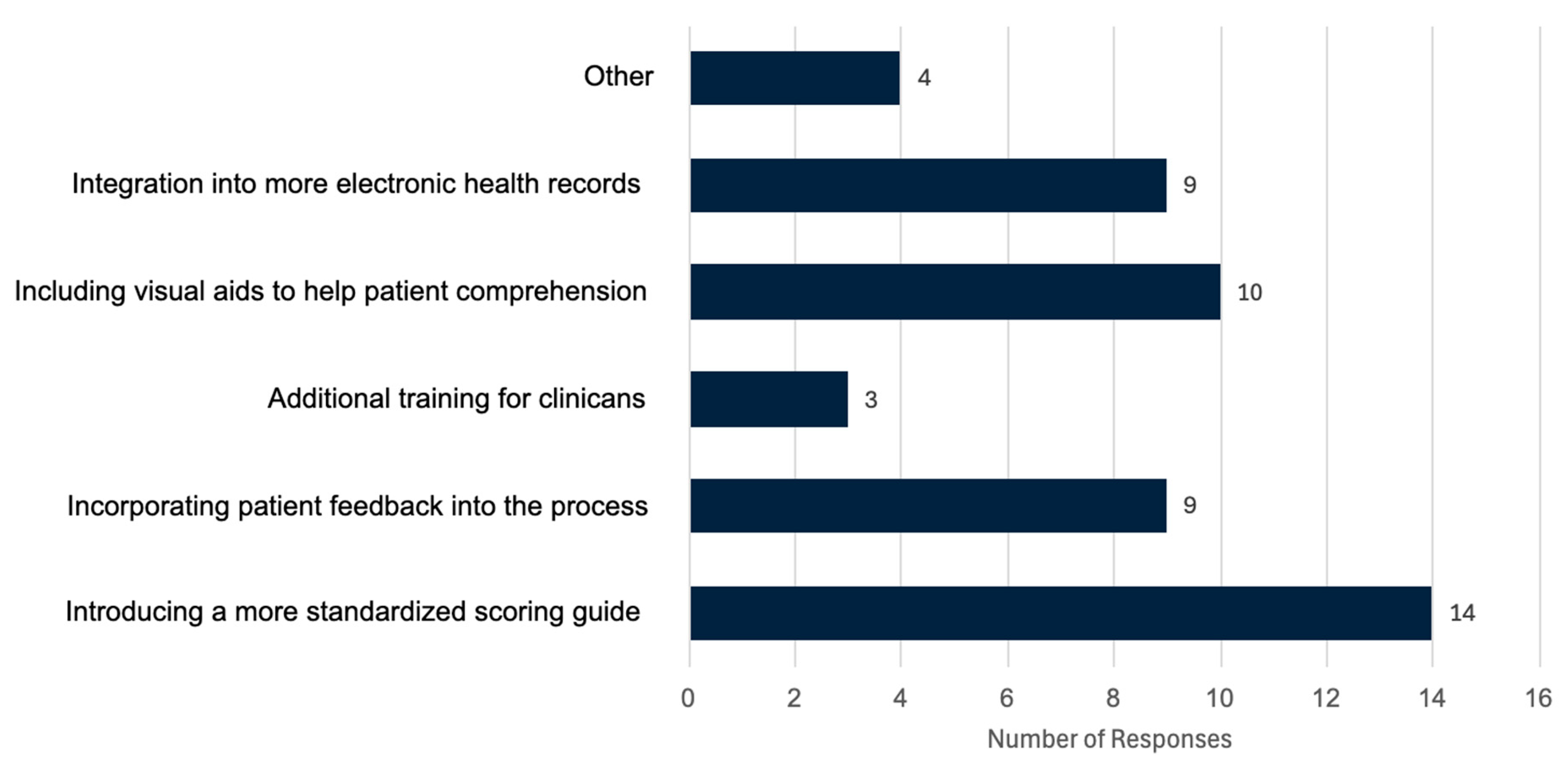
4. Results: Online Survey
“Patient function can vary due to stroke symptoms and comorbidities; factors such as fatigue or depression may lead to lower scores”;
“The tool is considered helpful, but is a crude measure that doesn’t adequately account for cognitive status”;
“The tool is easy to administer, but provides only a broad measure of recovery”;
“The tool is generally effective until patients reach a level of independent functioning, at which point important nuances in recovery and disability can be lost”;
“The tool sometimes reflects patient needs, but many important aspects are not captured by the mRS, limiting its ability to fully represent patient outcomes”.
“Changing to another similar scoring system that reflects more of the issues faced”;
“Frequently, patients’ caregiver, or family members need to administer it [the mRS] for objectivity, and the current mRS is very limited in capturing all needs, AI may be helpful”;
“Redevelopment to capture more nuance or maybe collaborations with other existing tests”.
5. Designing an mRS Collection Tool: Principles for a Clinical Assessment Tool
6. Design Principles for a Clinical Assessment Tool for the Modified Rankin Scale
6.1. Domains
6.2. Images
6.3. Phrasing
6.4. Providing Examples
6.5. Number of Options
6.6. Visual Esthetics
6.7. User Satisfaction Engagement
7. Impact
8. Discussion
8.1. Future Direction
8.2. Limitations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Pożarowszczyk, N.; Kurkowska-Jastrzębska, I.; Sarzyńska-Długosz, I.; Nowak, M.; Karliński, M. Reliability of the modified Rankin Scale in clinical practice of stroke units and rehabilitation wards. Front. Neurol. 2023, 14, 1064642. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Collier, J.M.; Quah, D.M.; Purvis, T.; Bernhardt, J. The Modified Rankin Scale in Acute Stroke Has Good Inter-Rater-Reliability but Questionable Validity. Cerebrovasc. Dis. 2010, 29, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Zeltzer, L. Modified Rankin Scale (MRS). Stroke Engine. Available online: https://strokengine.ca/en/assessments/modified-rankin-scale-mrs/#Purpose (accessed on 19 April 2008).
- Quinn, T.; Dawson, J.; Walters, M. Dr John Rankin; His Life, Legacy and the 50th Anniversary of the Rankin Stroke Scale. Scott. Med. J. 2008, 53, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Rethnam, V.; Bernhardt, J.; Johns, H.; Hayward, K.S.; Collier, J.M.; Ellery, F.; Gao, L.; Moodie, M.; Dewey, H.; Donnan, G.A.; et al. Look closer: The multidimensional patterns of post-stroke burden behind the modified Rankin Scale. Int. J. Stroke Off. J. Int. Stroke Soc. 2021, 16, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cumming School of Medicine. ESCAPE Stroke. University of Calgary. Available online: https://cumming.ucalgary.ca/escape-stroke (accessed on 9 April 2025).
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized Assessment of Rapid Endovascular Treatment of Ischemic Stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.D.; Goyal, M.; Menon, B.K.; Nogueira, R.G.; McTaggart, R.A.; Demchuk, A.M.; Graziewicz, M. Efficacy and safety of nerinetide for the treatment of acute ischaemic stroke (ESCAPE-NA1): A multicentre, double-blind, randomised controlled trial. Lancet 2020, 395, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.L.; Kaufman, D.R.; Kannampallil, T.G. Diagnostic Reasoning and Decision Making in the Context of Health Information Technology. Rev. Hum. Factors Ergon. 2013, 8, 149–190. [Google Scholar] [CrossRef]
- Sharma, S.K.; Mudgal, S.K.; Gaur, R.; Chaturvedi, J.; Rulaniya, S.; Sharma, P. Navigating Sample Size Estimation for Qualitative Research. J. Med. Evid. 2024, 5, 133–139. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.E.; Langton, K.B.; Haynes, R.B.; Mathieu, A. Effects of computer-based clinical decision support systems on clinician performance and patient outcome: A critical appraisal of research. Ann. Intern. Med. 1994, 120, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.L.; Kaufman, D.R.; Kannampallil, T. Human-Computer Interaction, Usability, and Workflow. In Biomedical Informatics; Shortliffe, E.H., Cimino, J.J., Eds.; Springer: Cham, Switzerland, 2021. [Google Scholar] [CrossRef]
- Lidwell, W.; Holden, K.; Butler, J. Universal Principles of Design: 125 Ways to Enhance Usability, Influence Perception, Increase Appeal, Make Better Design Decisions, and Teach Through Design (Revised and Updated); Rockport Publishers: Beverly, MA, USA, 2010. [Google Scholar]
- Johnson, J. Designing with the Mind in Mind: Simple Guide to Understanding User Interface Design Guidelines; Morgan Kaufmann: Cambridge, MA, USA, 2014. [Google Scholar]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
London, L.; Kamal, N. Designing a Patient Outcome Clinical Assessment Tool for Modified Rankin Scale: “You Feel the Same Way Too”. Informatics 2025, 12, 78. https://doi.org/10.3390/informatics12030078
London L, Kamal N. Designing a Patient Outcome Clinical Assessment Tool for Modified Rankin Scale: “You Feel the Same Way Too”. Informatics. 2025; 12(3):78. https://doi.org/10.3390/informatics12030078
Chicago/Turabian StyleLondon, Laura, and Noreen Kamal. 2025. "Designing a Patient Outcome Clinical Assessment Tool for Modified Rankin Scale: “You Feel the Same Way Too”" Informatics 12, no. 3: 78. https://doi.org/10.3390/informatics12030078
APA StyleLondon, L., & Kamal, N. (2025). Designing a Patient Outcome Clinical Assessment Tool for Modified Rankin Scale: “You Feel the Same Way Too”. Informatics, 12(3), 78. https://doi.org/10.3390/informatics12030078