
AGREEing on Clinical Practice Guidelines for Autism Spectrum Disorders in Children: A Systematic Review and Quality Assessment

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. The Capacity Building for Using the AGREE II Instrument
2.4. Quality Assessment of ASD CPGs Using AGREE II
2.5. Analysis Plan
Inter-Rater Analysis
3. Results
3.1. Characteristics of Included ASD CPGs
3.2. Quality Assessment of the ASD CPGs
3.2.1. Domain 1: Scope and Purpose
3.2.2. Domain 2: Stakeholder Involvement
3.2.3. Domain 3: Rigor of Development
3.2.4. Domain 4: Clarity of Presentation
3.2.5. Domain 5: Applicability
3.2.6. Domain 6: Editorial Independence
3.2.7. Overall Assessment
3.2.8. Recommending the ASD CPGs for Use in Practice
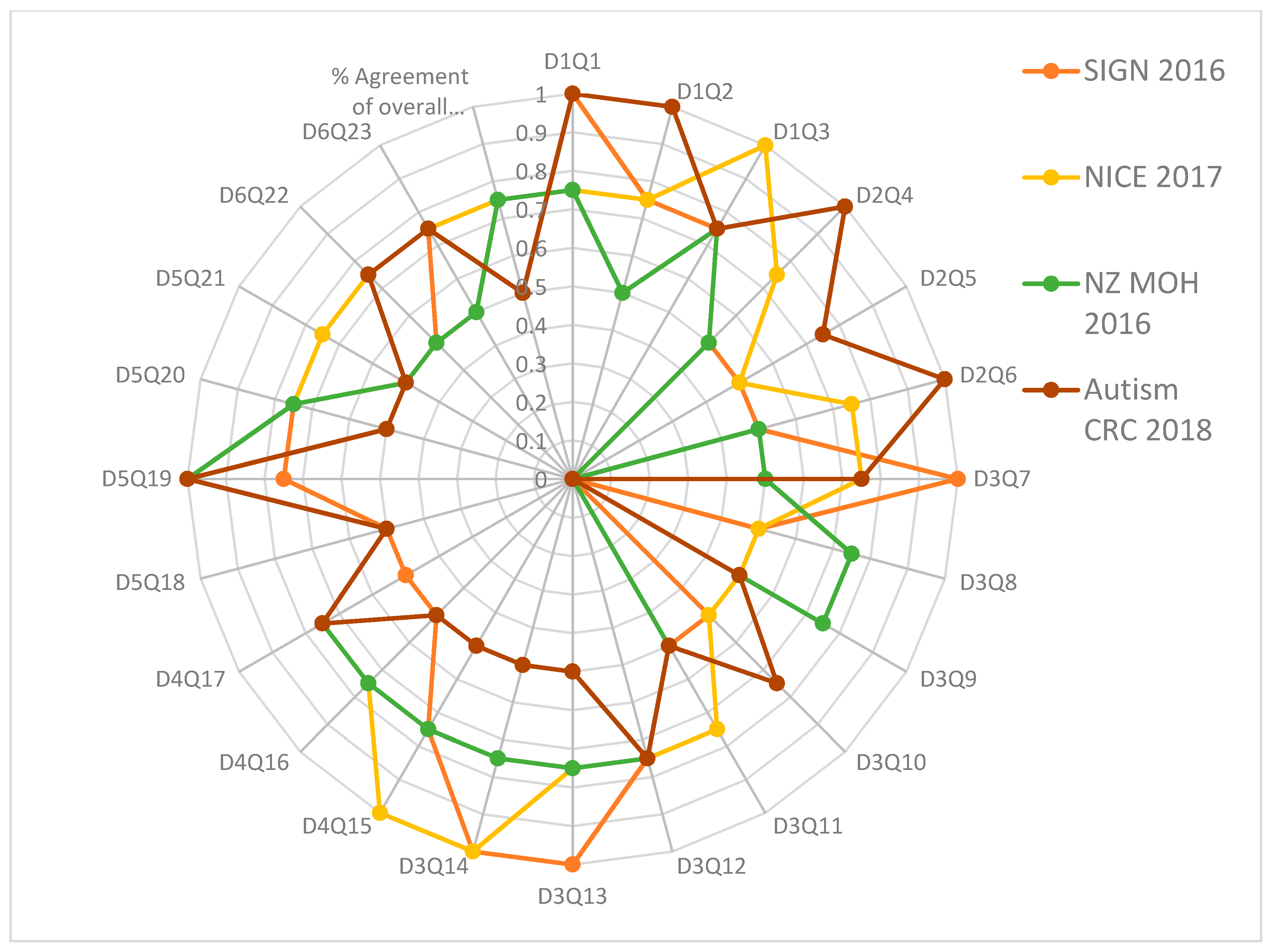
3.3. Inter-Rater Analysis
4. Discussion
4.1. Early Identification and Diagnosis
4.2. Interventions and Management of ASD
4.3. The transition of Care and Community Support
4.4. Challenging Behaviors
4.5. At Local and International Levels
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- APA—American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Lord, C.; Elsabbagh, M.; Baird, G.; Veenstra-Vanderweele, J. Autism spectrum disorder. Lancet 2018, 392, 508–520. [Google Scholar] [CrossRef]
- Gillberg, C.; Wing, L. Autism: Not an extremely rare disorder. Acta Psychiatr. Scand. 1999, 99, 399–406. [Google Scholar] [CrossRef] [PubMed]
- APA—American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- APA—American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- World Health Organization. Autism Spectrum Disorders 2019 [Cited 2020. July 19. Cited 2019 November]. Available online: https://www.who.int/news-room/fact-sheets/detail/autism-spectrum-disorders (accessed on 1 July 2022).
- Maenner, M.J.; Shaw, K.A.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Esler, A.; Furnier, S.M.; Hallas, L.; Hall-Lande, J.; Hudson, A.; et al. Prevalence and Characteristics of Autism Spectrum Disorder among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2018. MMWR Surveill. Summ. 2021, 70, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Mandy, W.; Lai, M.C. Towards sex- and gender-informed autism research. Autism 2017, 21, 643–645. [Google Scholar] [CrossRef] [Green Version]
- Rivet, T.T.; Matson, J.L. Review of gender differences in core symptomatology in autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 957–976. [Google Scholar] [CrossRef]
- Luo, Y.; Eran, A.; Palmer, N.; Avillach, P.; Levy-Moonshine, A.; Szolovits, P.; Kohane, I.S. A multidimensional precision medicine approach identifies an autism subtype characterized by dyslipidemia. Nat. Med. 2020, 26, 1375–1379. [Google Scholar] [CrossRef]
- Ferri, S.L.; Abel, T.; Brodkin, E.S. Sex Differences in Autism Spectrum Disorder: A Review. Curr. Psychiatry Rep. 2018, 20, 9. [Google Scholar] [CrossRef]
- Idring, S.; Lundberg, M.; Sturm, H.; Dalman, C.; Gumpert, C.; Rai, D.; Lee, B.K.; Magnusson, C. Changes in the prevalence of autism spectrum disorders in 2001–2011: Findings from the Stockholm youth cohort. J. Autism. Dev. Disord. 2015, 45, 1766–1773. [Google Scholar] [CrossRef]
- Lai, M.C.; Baron-Cohen, S.; Buxbaum, J.D. Understanding autism in the light of sex/gender. Mol. Autism 2015, 6, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Daniels, A.M.; Halladay, A.K.; Shih, A.; Elder, L.M.; Dawson, G. Approaches to enhancing the early detection of autism spectrum disorders: A systematic review of the literature. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 141–152. [Google Scholar] [CrossRef]
- Hill, T.L.; White, T.C.; Anthony, B.J.; Reaven, J.; Harris, B.; Reyes, N.; Anthony, L.G. Disparities in autism spectrum disorder diagnoses among 8-year-old children in Colorado: Who are we missing? Autism 2021, 25, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.; Mancher, M.; Miller Wolman, D.; Greenfield, S.; Steinberg, E. Clinical Practice Guidelines We Can Trust; National Academies Press (US): Washington, DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK209539/ (accessed on 3 July 2022).
- Hayes, J.; Ford, T.; Rafeeque, H.; Russell, G. Clinical practice guidelines for diagnosis of autism spectrum disorder in adults and children in the UK: A narrative review. BMC Psychiatry 2018, 18, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwers, M.C.; Kho, M.E.; Browman, G.P.; Burgers, J.S.; Cluzeau, F.; Feder, G.; Fervers, B.; Graham, I.D.; Grimshaw, J.; Hanna, S.E.; et al. AGREE II: Advancing guideline development, reporting and evaluation in health care. Cmaj Can. Med. Assoc. J. 2010, 182, E839–E842. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, M.C.; Spithoff, K.; Lavis, J.; Kho, M.E.; Makarski, J.; Florez, I.D. What to do with all the AGREEs? The AGREE portfolio of tools to support the guideline enterprise [published online ahead of print, May 29 2020]. J. Clin. Epidemiol. 2020, 125, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Siering, U.; Eikermann, M.; Hausner, E.; Hoffmann-Eßer, W.; Neugebauer, E.A. Appraisal Tools for Clinical Practice Guidelines: A systematic review. PLoS ONE 2013, 8, e82915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amer, Y.S.; Wahabi, H.A.; Abou Elkheir, M.M.; Bawazeer, G.A.; Iqbal, S.M.; Titi, M.A.; Ekhzaimy, A.; Alswat, K.A.; Alzeidan, R.A.; Al-Ansary, L.A. Adapting evidence-based clinical practice guidelines at university teaching hospitals: A model for the eastern Mediterranean Region. J. Eval. Clin. Pract. 2019, 25, 550–560. [Google Scholar] [CrossRef]
- Amer, Y.S.; Elzalabany, M.M.; Omar, T.I.; Ibrahim, A.G.; Dowidar, N.L. The ‘Adapted ADAPTE’: An approach to improve utilization of the ADAPTE guideline adaptation resource toolkit in the Alexandria Center for Evidence-Based Clinical Practice Guidelines. J. Eval. Clin. Pract. 2015, 21, 1095–1106. [Google Scholar] [CrossRef]
- Johnston, A.; Kelly, S.; Hsieh, S.C.; Skidmore, B.; Wells, G.A. Systematic reviews of clinical practice guidelines: A methodological guide. J. Clin. Epidemiol. 2019, 108, 64–76. [Google Scholar] [CrossRef]
- Alenezi, S.; Bashiri, F.A.; Alawami, A.H.; Alhazmi, A.S.; Aladamawai, S.A.; Alnemary, F.; Alqahtani, Y.; Buraik, M.W.; AlSuwailem, S.S.; Akhalifah, S.M.; et al. Quality Assessment of Clinical Practice Guidelines for the Management of Autism Spectrum Disorders (ASD) in Children: A Protocol for a Systematic Review and Assessment Using the AGREE II Instrument [Internet]. OSF. 2021. Available online: https://osf.io/n39xz/ (accessed on 10 May 2022).
- Penner, M.; Anagnostou, E.; Andoni, L.Y.; Ungar, W.J. Systematic review of clinical guidance documents for autism spectrum disorder diagnostic assessment in select regions. Autism 2018, 22, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Norris, S.; Bero, L. The advantages and limitations of guideline adaptation frameworks. Implement Sci. 2018, 13, 72. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Hasim, N.; Bakar, M.A.; Islam, M.A. Efficacy and Safety of Isotonic and Hypotonic Intravenous Maintenance Fluids in Hospitalised Children: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Children 2021, 8, 785. [Google Scholar] [CrossRef]
- Login—AGREE Enterprise Website. Agreetrust.org. Available online: https://www.agreetrust.org/my-agree/ (accessed on 27 December 2021).
- Altokhais, T.I.; Al-Obaid, O.A.; Kattan, A.E.; Amer, Y.S. CPG Collaborative Groups. Assessment of implementability of an adapted clinical practice guideline for surgical antimicrobial prophylaxis at a tertiary care university hospital. J. Eval. Clin. Pract. 2017, 23, 156–164. [Google Scholar] [CrossRef]
- Alhasan, K.A.; Al Khalifah, R.; Aloufi, M.; Almaiman, W.; Hamad, M.; Abdulmajeed, N.; Al Salloum, A.; Kari, J.A.; AlJelaify, M.; Bassrawi, R.K.; et al. AGREEing on clinical practice guidelines for idiopathic steroid-sensitive nephrotic syndrome in children. Syst. Rev. 2021, 10, 144. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Measur. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Fleiss, J.L.; Shrout, P.E. Approximate interval estimation for a certain intraclass correlation coefficient. Psychometrika 1978, 43, 259–262. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistics Notes: Measurement error and correlation coefficients. BMJ 1996, 313, 41–42. [Google Scholar] [CrossRef]
- Autism CRC The University of Queensland. Australian National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders|Autism CRC. 2018. Available online: https://www.autismcrc.com.au/access/national-guideline (accessed on 27 January 2021).
- Ministry of Health New Zealand (NZ). New Zealand Autism Spectrum Disorder Guideline. 2016. Available online: https://www.health.govt.nz/publication/new-zealand-autism-spectrum-disorder-guideline (accessed on 27 January 2021).
- National Institute for Health and Care Excellence (NICE). Autism Spectrum Disorder in under 19s: Recognition, Referral and Diagnosis | Guidance | NICE. 2017. Available online: https://www.nice.org.uk/guidance/cg128 (accessed on 27 January 2021).
- Scottish Intercollegiate Guidelines Network (SIGN) Healthcare Improvement Scotland (HIS). Assessment, Diagnosis and Interventions for Autism Spectrum Disorders. 2016. Available online: https://www.sign.ac.uk/our-guidelines/assessment-diagnosis-and-interventions-for-autism-spectrum-disorders/ (accessed on 27 January 2021).
- Wickstrom, J.; Dell’Armo, K.; Salzman, E.; Hooker, J.L.; Delehanty, A.; Bishop, S.; Tassé, M.J.; Wetherby, A.M.; Piergies, A.M.; Damiano, D.; et al. Systematic Review: Recommendations for Rehabilitation in ASD and ID from Clinical Practice Guidelines. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100140. [Google Scholar] [CrossRef]
- Pattison, E.; Ure, A.; Mittiga, S.R.; Williams, K.; Freeman, N.C. The Feedback Session of an Autism Assessment: A Scoping Review of Clinical Practice Guideline Recommendations. J. Autism. Dev. Disord. 2021, 52, 1–20. [Google Scholar] [CrossRef]
- Brouwers, M.C.; Spithoff, K.; Kerkvliet, K.; Alonso-Coello, P.; Burgers, J.; Cluzeau, F.; Férvers, B.; Graham, I.; Grimshaw, J.; Hanna, S.; et al. Development and validation of a tool to assess the quality of clinical practice guideline recommendations. JAMA Netw. Open 2020, 3, e205535. [Google Scholar] [CrossRef]
- Hoffmann-Eßer, W.; Siering, U.; Neugebauer, E.A.; Lampert, U.; Eikermann, M. Systematic review of current guideline appraisals performed with the Appraisal of Guidelines for Research & Evaluation II instrument—A third of AGREE II users apply a cut-off for guideline quality. J. Clin. Epidemiol. 2018, 95, 120–127. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Organization, Country (Abbreviation) | Health System, Economic Classification | CPG Title | Year of Publication |
|---|---|---|---|
| Australian Autism CRC, Australia (ACRC) | National Health Insurance, High-income country | Australian National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders | 2018 |
| Ministry of Health New Zealand, New Zealand (NZ) | National Health Insurance, High-income country | New Zealand Autism Spectrum Disorder Guideline | 2016 |
| National Institute for Health and Care Excellence, United Kingdom (NICE) | National Health Service, High-income country | Autism spectrum disorder in under 19s: recognition, referral and diagnosis | 2017 |
| Scottish Intercollegiate Guidelines Network (SIGN), Healthcare Improvement Scotland, Scotland (HIS) | National Health Service, High-income country | Assessment, diagnosis and interventions for autism spectrum disorders | 2019 |
| Source CPGs/AGREE II Domains Scores (%) | ACRC 2018 [35] | NZ 2016 [36] | NICE 2017 [37] | SIGN 2019 [38] |
|---|---|---|---|---|
| Domain 1. Scope and Purpose Items 1–3: Objectives; health question(s); population (patients, public, etc.) | 99% | 93% | 96% | 97% |
| Domain 2. Stakeholder Involvement Items 4–6: Group membership; target population preferences and views; target users | 99% | 71% | 72% | 79% |
| Domain 3. Rigor of development Items 7–14: Search methods; evidence selection criteria; strengths and limitations of the evidence; formulation of recommendations; consideration of benefits and harms; link between recommendations and evidence; external review; updating procedure. | 84% | 86% | 93% | 85% |
| Domain 4. Clarity and presentation Items 15–17: Specific and unambiguous recommendations; management options; identifiable key recommendations | 93% | 94% | 97% | 93% |
| Domain 5. Applicability Items 18–21: Facilitators and barriers to application; implementation advice/tools; resource implications; monitoring/auditing criteria | 92% | 54% | 89% | 85% |
| Domain 6. Editorial independence Items 22, 23: Funding body; competing interests | 92% | 69% | 92% | 92% |
| Overall Assessment 1 (Overall quality) | 92% | 88% | 96% | 92% |
| Overall Assessment 2 (Recommend the CPG for use by four appraisers) | Yes—3, Yes with modifications—1, No—0 | Yes—4, Yes with modifications—0, No—0 | Yes—2, Yes with modifications—2, No—0 | Yes—2, Yes with modifications—2, No—0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amer, Y.S.; Alenezi, S.; Bashiri, F.A.; Alawami, A.H.; Alhazmi, A.S.; Aladamawi, S.A.; Alnemary, F.; Alqahtani, Y.; Buraik, M.W.; AlSuwailem, S.S.; et al. AGREEing on Clinical Practice Guidelines for Autism Spectrum Disorders in Children: A Systematic Review and Quality Assessment. Children 2022, 9, 1050. https://doi.org/10.3390/children9071050
Amer YS, Alenezi S, Bashiri FA, Alawami AH, Alhazmi AS, Aladamawi SA, Alnemary F, Alqahtani Y, Buraik MW, AlSuwailem SS, et al. AGREEing on Clinical Practice Guidelines for Autism Spectrum Disorders in Children: A Systematic Review and Quality Assessment. Children. 2022; 9(7):1050. https://doi.org/10.3390/children9071050
Chicago/Turabian StyleAmer, Yasser S., Shuliweeh Alenezi, Fahad A. Bashiri, Amel Hussain Alawami, Ayman Shawqi Alhazmi, Somayyah A. Aladamawi, Faisal Alnemary, Yasser Alqahtani, Maysaa W. Buraik, Saleh S. AlSuwailem, and et al. 2022. "AGREEing on Clinical Practice Guidelines for Autism Spectrum Disorders in Children: A Systematic Review and Quality Assessment" Children 9, no. 7: 1050. https://doi.org/10.3390/children9071050
APA StyleAmer, Y. S., Alenezi, S., Bashiri, F. A., Alawami, A. H., Alhazmi, A. S., Aladamawi, S. A., Alnemary, F., Alqahtani, Y., Buraik, M. W., AlSuwailem, S. S., Akhalifah, S. M., Augusta de Souza Pinhel, M., Penner, M., & Elmalky, A. M. (2022). AGREEing on Clinical Practice Guidelines for Autism Spectrum Disorders in Children: A Systematic Review and Quality Assessment. Children, 9(7), 1050. https://doi.org/10.3390/children9071050