
Transcatheter Device Therapy and the Integration of Advanced Imaging in Congenital Heart Disease

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- A.
- Provide an overview of current transcatheter implantable devices and briefly discuss newer devices being developed.
- B.
- Discuss the role and integration of advanced imaging in transcatheter interventions.
- C.
- Explore the current patient friendly regulatory framework encouraging innovative device development.
2. Overview of Current Transcatheter Therapies for CHD
- Device closure of cardiac shunts
- Endovascular stenting for obstructed blood vessels
- Transcatheter valve therapies
- Vascular occlusion devices
2.1. Device Closure of Cardiac Shunts
2.1.1. Atrial Septal Defect Closure
- i.
- Erosion: The Amplatzer Septal Occluder has been associated with cardiac erosion causing pericardial effusion with or without cardiac tamponade, and rarely death [24,25]. While most cases of cardiac erosion occur early, erosions occurring several years after device closure have been reported [26]. Until 2020, the Gore family of ASD devices were not associated cardiac erosion; now two cases have been reported [27]. While a number of risk factors for cardiac erosion have been proposed, none are predictive of erosion [25,28,29]. ASD closure devices used outside the United States have also been associated with cardiac erosion [30,31].
- ii.
- Atrioventricular (AV) block: ASD Occluders have been associated with AV block [32]. Bink et al. have reported 15% incidence of preoperative first degree AV block; therefore careful preoperative evaluation with an electrocardiogram is important [33]. ASDs are also associated with risk of progressive AV block if genetically predisposed [34]. From an interventional standpoint, interaction between the device and the AV node in the triangle of Koch either from direct trauma or in response to inflammatory reaction have been postulated as possible mechanisms [32,35,36]. Proposed risk factors include large device (based on patient age, absolute device size, device to septal length ratio, device to height ratio), deficient postero-inferior rim, and direct contact of the device with the triangle of Koch following deployment [35]. Optimal approach for treatment of post-device closure AV block is controversial. Options include device retrieval and placement of a smaller device, medical therapy with high dose aspirin and steroids, and immediate device removal with surgical closure [32,35,36]. Treatment is likely best individualized, with medical therapy reserved for lower grades of AV block, and removal indicated for progressive AV block, failed medical therapy, or complete heart block.
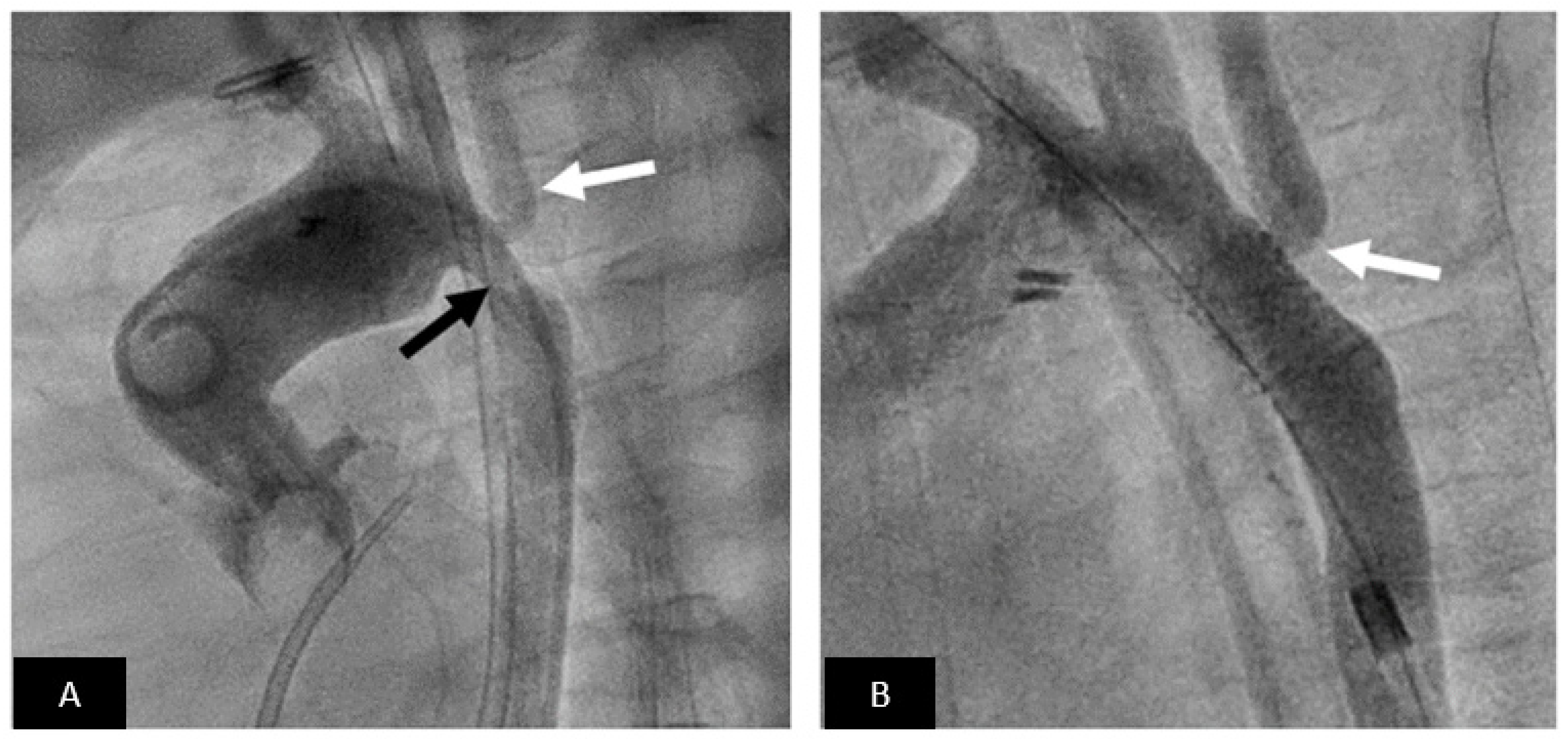
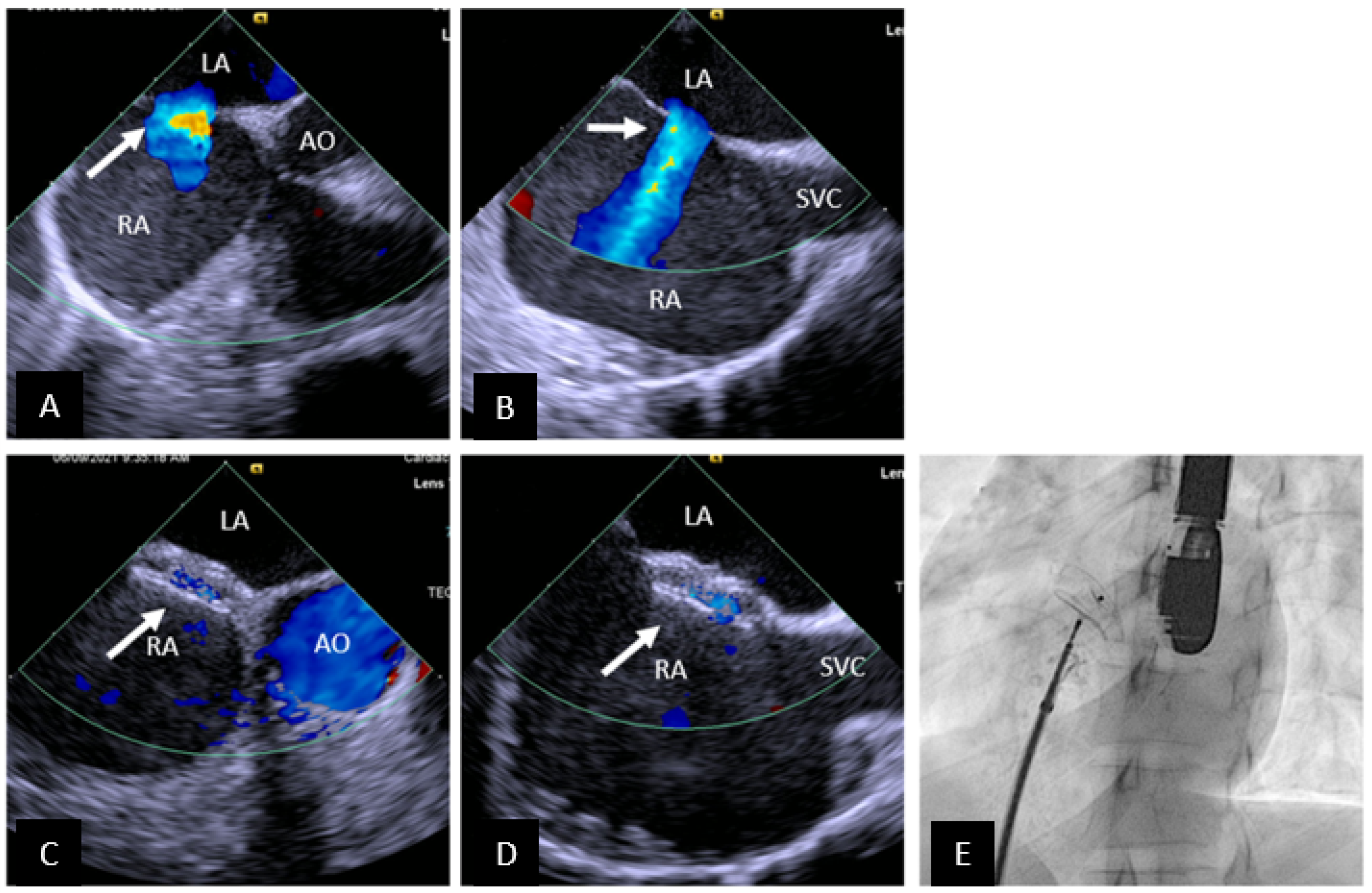
- iii.
- For transcatheter SVASD closure longer-term data will be necessary to determine optimal stent design, how to avoid residual shunting, optimal closure strategy for residual defects, and monitoring for development of late pulmonary vein obstruction or sinus node dysfunction.
2.1.2. Ventricular Septal Defect Closure
- i.
- The reported incidence of complete heart block after pmVSD closure varies from 0.1–22% [46,47]. The devices associated with the highest risk are no longer used. For reference, the risk of complete heart block after surgical repair is less than 2% [47]. Therefore longer-term data is necessary before pmVSD closure becomes standard of care.
- ii.
- Injury to the aortic valve and both AV valves (especially tricuspid) can be seen especially after transcatheter pmVSD closure. Again, longer-term data is lacking, and this information is necessary for acceptance of routine pmVSD closure.
- iii.
- Residual shunting is reported in 3–29% of cases; for certain devices such as the Nit-Occlud Lê VSD-Coil (PFM Medical AG, Cologne, Germany) the incidence is even higher [47]. Longer-term follow-up will be necessary to determine if these residual shunts are hemodynamically significant and if intravascular hemolysis is a clinical problem.
- iv.
2.1.3. Patent Ductus Arteriosus Closure
- i.
- Device embolization: The risk of device embolization was higher when coils were the only option; now with current technology the risk is lower. The ADO-I can be challenging to retrieve since the micro-screw is recessed. This is less problematic for the other Amplatzer devices.
- ii.
- Residual shunt with or without hemolysis is another complication that was more common when coils were routinely used. Fortunately, this risk is now very small.
- iii.
- Device related left pulmonary artery stenosis is an important consideration especially in small infants. Intraductal placement of the device and using a device without a disc on the pulmonary artery side are useful strategies.
- iv.
- Device-related aortic coarctation can occur. The risk is highest in small infants and neonates. Mild isthmic hypoplasia, protrusion of the device into the aorta, and short length of the PDA are some of the risk factors.
- v.
- Arterial injury: Until recently, arterial access was needed to perform assessment for residual shunting and arch obstruction prior to device release. The risk of arterial injury is highest in small infants. In premature infants, arterial access is not obtained; assessment for left pulmonary artery stenosis, aortic obstruction, and residual shunting is performed using transthoracic echocardiography. Many operators are now extending this experience to larger infants, further increasing the safety of the procedure.
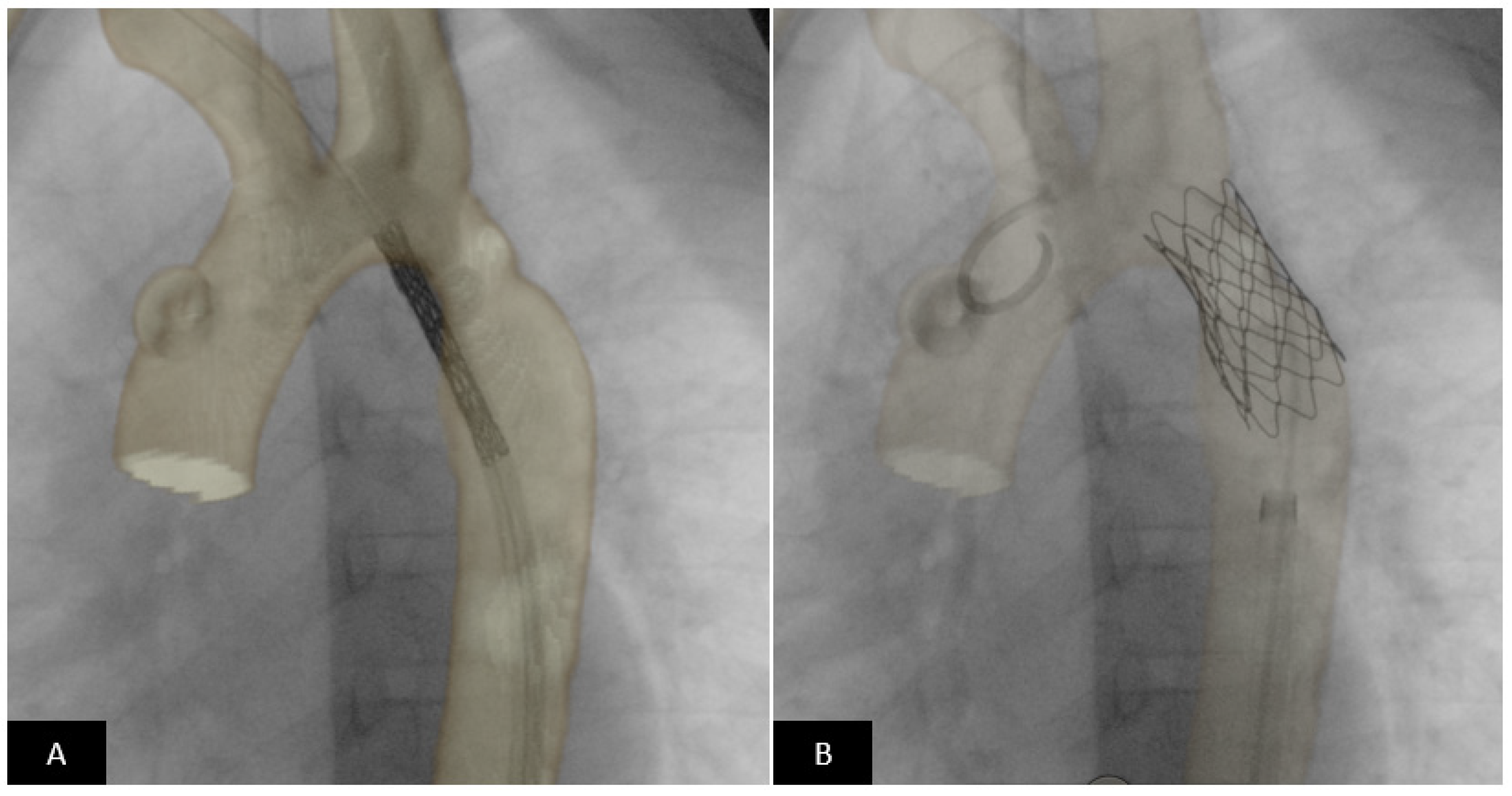
2.2. Endovascular Stenting of Obstructed Blood Vessels
- i.
- Acute risks include access site vascular injury, stent migration, implantation site vascular injury, need for emergency surgery, compression of adjacent vascular structures (coronary artery compression during right ventricular outflow stenting or the airway, left bronchial compression during left pulmonary artery stenting after Fontan palliation), and rarely death.
- ii.
- In the intermediate and long-term, vascular stenosis secondary to neointimal proliferation, acquired stenosis secondary to somatic growth, and unintentional stent fracture are relevant clinical problems. Unintentional stent fracture results from cyclical loading imposed by the dynamic cardiovascular milieu at the implantation site and can be clinically silent or can result in stent collapse and vascular stenosis.
- iii.
- Fortunately, most stents can be safely dilated beyond manufacturer-recommended maximum diameter to accommodate for somatic growth (note that self-expanding stents cannot be dilated beyond nominal diameter). To accomplish this, serial incremental dilation is necessary. All stents dilated beyond the nominal diameter shorten longitudinally, with the degree of shortening being stent-specific and widely variable.
- iv.
- Small children are frequently treated with pre-mounted small and medium diameter stents owing to the necessity for a smaller crossing profile and flexibility. Here the only option for increasing stent diameter is surgical intervention or intentional stent fracture followed by placement of a larger stent. While feasibility has been shown on the bench and in some clinical studies, the generalizability of this approach is awaiting real world clinical data.
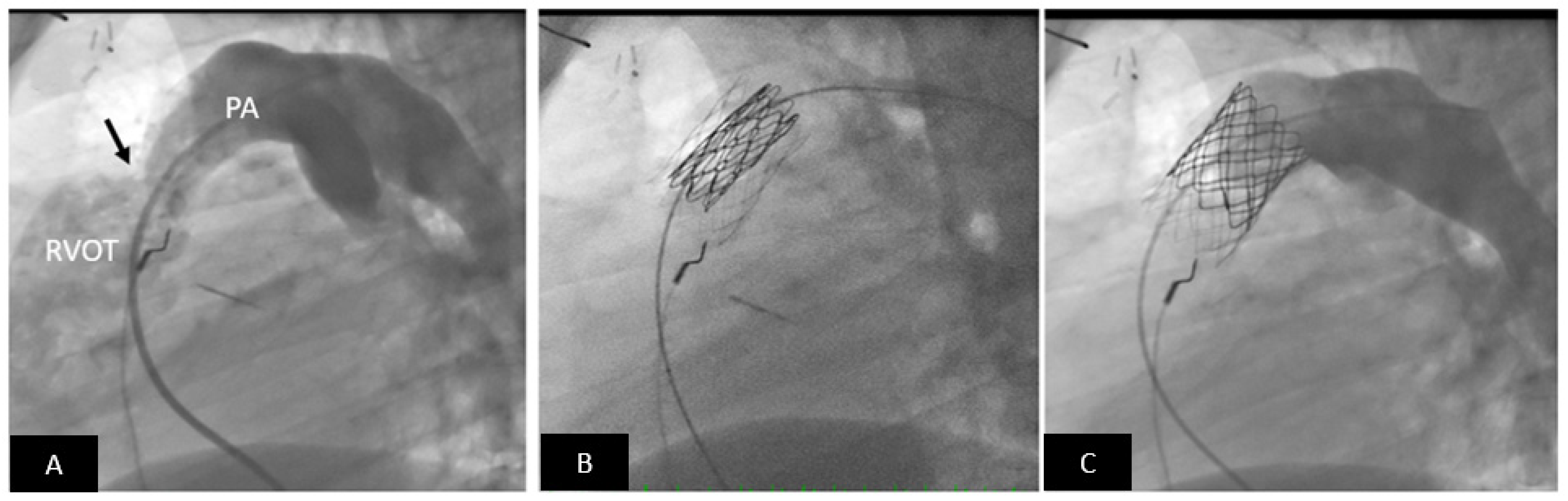
2.3. Transcatheter Valve Therapies
- i.
- Endocarditis: The risk of endocarditis is highest with the Melody valve and lowest with the Sapien valves [82]. To date endocarditis has not been reported in Harmony TPV and Alterra pre-stent implants [82,83,84,85]. All TPVs have risk of endocarditis and therefore life-long endocarditis prophylaxis is recommended. Longer term data will be necessary to define patient- and device-related risk factors.
- ii.
- Growth strategies: For successful TPVR, defined as low resting gradient, the landing zone in conduits and bioprosthetic valves may not be of an adequate diameter. The ability to dilate the conduit beyond the nominal implant size and fracturing of the bioprosthetic valve ring can allow “growth” in some patients. The minimum diameter necessary and safety of this approach needs to be studied.
- iii.
- Anticoagulation: There is increasing recognition that valve function and possibly endocarditis risk are at least partly determined by thrombosis of the valve leaflets/housing. Optimal strategies for each valve have not yet been defined. Lifelong aspirin is increasingly used; some patients require dual anti-platelet therapy and/or anticoagulation.
- iv.
- Stent fractures: Prior to routine pre-stenting, Melody valve frame fractures were common. Fortunately, the incidence decreases with pre-stenting and adequate preparation of the conduit. The structural frame of the Sapien valve is stronger and frame fractures are rare. It is too early to know the risk for the new self-expanding valves.
- v.
- Pulmonary regurgitation: While the short and intermediate term freedom from reintervention for PR is generally good, longer-term data is necessary. For the larger self-expanding valves, the additional risk of perivalvular leak will require investigation. Currently, the incidence of significant perivalvular leak is small.
- vi.
- Arrhythmias: There appears to be a higher incidence of ventricular arrhythmia after TPVR especially with the larger self-expanding valves. Fortunately, a majority of the reported arrhythmias are benign (PVCs, non-sustained VT), respond to medications, and resolve in a majority of patients after several weeks [80]. We will need longer term data to understand the mechanism, risks, and treatment paradigm.
2.4. Vascular Occlusion Devices
- i.
- ii.
- Coils and vascular plugs cause artifact during subsequent clinically necessary cross-sectional imaging. Fortunately, most of the devices are MR conditional and when appropriate care is taken can be safely imaged.
- iii.
- Recanalization after occlusion of aortopulmonary collaterals especially with coils and plugs is common. Recanalized vessels pose difficulty for repeat occlusion especially when significant. The optimal method to prevent recanalization remains currently undetermined [95].
3. Review the Role of Advanced Imaging and Its Integration in the Current Management of CHD
3.1. Echocardiography
3.2. Three-Dimensional Imaging
3.2.1. Pre-Procedural Guidance
3.2.2. Three-Dimensional Printing
3.2.3. Virtual Reality
3.3. Intraoperative/Intraprocedural Guidance
3.3.1. Echocardiography-Fluoroscopy Fusion
CT/cMRI Overlay
3.3.2. Augmented Reality Real-Time Guidance
3.3.3. Future Directions
4. Current Regulatory Framework within the United States for Device Approval
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharfi, M.H.; Alghamdi, A.H.; Mashali, M.H.; Helel, A.M.; Arfi, M.A. Current Advances in Transcatheter Intervention for Children Born with Congenital Heart Defects: A Review of Literature. J. Biosci. Med. 2021, 9, 219–230. [Google Scholar] [CrossRef]
- Levi, D.S.; Kusnezov, N.; Carman, G.P. Smart Materials Applications for Pediatric Cardiovascular Devices. Pediatr. Res. 2008, 63, 552–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexy, R.D.; Levi, D.S. Materials and manufacturing technologies available for production of a pediatric bioabsorbable stent. Biomed. Res. Int. 2013, 2013, 137985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schievano, S.; Taylor, A.M.; Capelli, C.; Lurz, P.; Nordmeyer, J.; Migliavacca, F.; Bonhoeffer, P. Patient specific finite element analysis results in more accurate prediction of stent fractures: Application to percutaneous pulmonary valve implantation. J. Biomech. 2010, 43, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Schievano, S.; Capelli, C.; Young, C.; Lurz, P.; Nordmeyer, J.; Owens, C.; Bonhoeffer, P.; Taylor, A.M. Four-dimensional computed tomography: A method of assessing right ventricular outflow tract and pulmonary artery deformations throughout the cardiac cycle. Eur. Radiol. 2011, 21, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, M.J.; Benson, L.N.; Bergersen, L.; Bacha, E.A.; Cheatham, S.L.; Crean, A.M.; Eicken, A.; Ewert, P.; Geva, T.; Hellenbrand, W.E.; et al. Patient Selection Process for the Harmony Transcatheter Pulmonary Valve Early Feasibility Study. Am. J. Cardiol. 2017, 120, 1387–1392. [Google Scholar] [CrossRef]
- Capelli, C.; Biglino, G.; Petrini, L.; Migliavacca, F.; Cosentino, D.; Bonhoeffer, P.; Taylor, A.M.; Schievano, S. Finite element strategies to satisfy clinical and engineering requirements in the field of percutaneous valves. Ann. Biomed. Eng. 2012, 40, 2663–2673. [Google Scholar] [CrossRef]
- Heyden, C.M.; Brock, J.E.; Ratnayaka, K.; Moore, J.W.; El-Said, H.G. Intravascular Ultrasound (IVUS) Provides the Filling for the Angiogram’s Crust: Benefits of IVUS in Pediatric Interventional Cardiology. J. Invasive Cardiol. 2021, 33, E978–E985. [Google Scholar]
- Arar, Y.; Dimas, V.V.; Nugent, A.W.; Hussain, T.; Kasraie, N.; Reddy, S.R.V.; Zellers, T.M.; Herbert, C. Pre-procedural CT imaging aids neonatal PDA stenting for ductal-dependent pulmonary blood flow with reduction in overall procedural morbidity. Cardiol. Young 2021, 1–6. [Google Scholar] [CrossRef]
- Divekar, A. Mustard Transcatheter Pulmonary Venous Baffle Intervention—A Pictorial essay. Congenit. Cardiol. Today 2015, 13, 1–24. [Google Scholar]
- Arar, Y.; Reddy, S.R.V.; Kim, H.; Dimas, V.V.; Zellers, T.M.; Abou Zahr, R.; Vamsee, R.; Greer, J.S.; Tandon, A.; Pontiki, A.; et al. 3D advanced imaging overlay with rapid registration in CHD to reduce radiation and assist cardiac catheterisation interventions. Cardiol. Young 2020, 30, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Mathis, C.; Romans, R.; Divekar, A. Variation in the outer diameter of vascular sheaths commonly used in infant cardiac catheterization. Catheter. Cardiovasc. Interv. 2020, 96, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.; Gillette, N.; Patel, H.; Peiris, V. Regulatory Science, and How Device Regulation Will Shape Our Future. Pediatr. Cardiol. 2020, 41, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Peiris, V.; Xu, K.; Agler, H.L.; Chen, E.A.; Gopal-Srivastava, R.; Lappin, B.M.; Lewis, D.Y.; Rao, G.R. Children and Adults with Rare Diseases Need Innovative Medical Devices. J. Med. Devices 2018, 12, 034701. [Google Scholar] [CrossRef]
- Takahashi, S.; Ibrahim, N.; Yasukochi, S.; Ringel, R.; Ing, F.; Tomita, H.; Sugiyama, H.; Yamagishi, M.; Forbes, T.J.; Kim, S.H.; et al. Partnership between Japan and the United States for Early Development of Pediatric Medical Devices-Harmonization by Doing for Children. Circ. J. 2020, 84, 786–791. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M. Natural history of atrial septal defect. Br. Heart J. 1970, 32, 820–826. [Google Scholar] [CrossRef]
- Saxena, A.; Divekar, A.; Soni, N.R. Natural history of secundum atrial septal defect revisited in the era of transcatheter closure. Indian Heart J. 2005, 57, 35–38. [Google Scholar]
- Murphy, J.G.; Gersh, B.J.; McGoon, M.D.; Mair, D.D.; Porter, C.J.; Ilstrup, D.M.; McGoon, D.C.; Puga, F.J.; Kirklin, J.W.; Danielson, G.K. Long-term outcome after surgical repair of isolated atrial septal defect. Follow-up at 27 to 32 years. N. Engl. J. Med. 1990, 323, 1645–1650. [Google Scholar] [CrossRef]
- Mills, N.L.; King, T.D. Nonoperative closure of left-to-right shunts. J. Thorac. Cardiovasc. Surg. 1976, 72, 371–378. [Google Scholar] [CrossRef]
- Amedro, P.; Bayburt, S.; Assaidi, A.; Kreitmann, B.; Habib, G.; Fouilloux, V.; Fraisse, A. Should transcatheter closure of atrial septal defects with inferior-posterior deficient rim still be attempted? J. Thorac. Dis. 2019, 11, 708–716. [Google Scholar] [CrossRef]
- O’Byrne, M.L.; Levi, D.S. State-of-the-Art Atrial Septal Defect Closure Devices for Congenital Heart. Interv. Cardiol. Clin. 2019, 8, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, H.A.M.; Alsalkhi, H.A.; Khalid, K.A. Transcatheter closure of sinus venosus atrial septal defect with anomalous pulmonary venous drainage: Innovative technique with long-term follow-up. Catheter. Cardiovasc. Interv. 2020, 95, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.; Qureshi, S.A.; Jones, M.; Butera, G.; Sivakumar, K.; Boudjemline, Y.; Hijazi, Z.M.; Almaskary, S.; Ponder, R.D.; Salem, M.M.; et al. Correction of sinus venosus atrial septal defects with the 10 zig covered Cheatham-platinum stent—An international registry. Catheter. Cardiovasc. Interv. 2021, 98, 128–136. [Google Scholar] [CrossRef]
- Divekar, A.; Gaamangwe, T.; Shaikh, N.; Raabe, M.; Ducas, J. Cardiac perforation after device closure of atrial septal defects with the Amplatzer septal occluder. J. Am. Coll. Cardiol. 2005, 45, 1213–1218. [Google Scholar] [CrossRef] [Green Version]
- McElhinney, D.B.; Quartermain, M.D.; Kenny, D.; Alboliras, E.; Amin, Z. Relative Risk Factors for Cardiac Erosion following Transcatheter Closure of Atrial Septal Defects. Circulation 2016, 133, 1738–1746. [Google Scholar] [CrossRef] [Green Version]
- Guelker, J.-E.; Jansen, R.; Sievert, K.; Sievert, H.; Bertog, S. Very late erosion of Amplatzer occluder device resulting in Cardiac tamponade after 15 years. Clin. Res. Cardiol. 2018, 107, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Orford, J.L.; Tobis, J.M. Two cases of pericardial tamponade due to nitinol wire fracture of a gore septal occluder. Catheter. Cardiovasc. Interv. 2020, 96, 219–224. [Google Scholar] [CrossRef] [PubMed]
- El-Said, H.G.; Moore, J.W. Erosion by the Amplatzer Septal Occluder: Experienced Operator Opinions at Odds with Manufacturer Recommendations? Catheter. Cardiovasc. Interv. 2009, 73, 925–930. [Google Scholar] [CrossRef]
- Kitano, M.; Yazaki, S.; Sugiyama, H.; Ohtsuki, S.-I.; Tomita, H. Risk Factors and Predictors of Cardiac Erosion Discovered from 12 Japanese Patients Who Developed Erosion after Atrial Septal Defect Closure Using Amplatzer Septal Occluder. Pediatr. Cardiol. 2020, 41, 297–308. [Google Scholar] [CrossRef]
- Ikeda, S.; Imai, M.; Yoshizawa, K.; Miyamoto, T.; Fujiwara, K.; Sato, Y. Cardiac erosion causing an aortic dissection after a catheter closure of an atrial septal defect: First late erosion case with the Figulla Flex II septal occluder. Cardiovasc. Interv. Ther. 2021, 36, 270–272. [Google Scholar] [CrossRef]
- Auriau, J.; Bouvaist, H.; Aaberge, L.; Abe, T.; Dähnert, I.; Panzer, J.; Santoro, G.; Khalil, M.; Hijazi, Z.M.; Fraisse, A. Cardiac Erosions after Transcatheter Atrial Septal Defect Closure with the Occlutech Figulla Flex Device. JACC Cardiovasc. Interv. 2019, 12, 1397–1399. [Google Scholar] [CrossRef] [PubMed]
- Asakai, H.; Weskamp, S.; Eastaugh, L.; D’Udekem, Y.; Pflaumer, A. Atrioventricular block after ASD closure. Heart Asia 2016, 8, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bink-Boelkens, M.T.; Bergstra, A.; Landsman, M.L. Functional abnormalities of the conduction system in children with an atrial septal defect. Int. J. Cardiol. 1988, 20, 263–272. [Google Scholar] [CrossRef]
- Xu, Y.-J.; Qiu, X.-B.; Yuan, F.; Shi, H.-Y.; Xu, L.; Hou, X.-M.; Qu, X.-K.; Liu, X.; Huang, R.-T.; Xue, S.; et al. Prevalence and spectrum of NKX2.5 mutations in patients with congenital atrial septal defect and atrioventricular block. Mol. Med. Rep. 2017, 15, 2247–2254. [Google Scholar] [CrossRef] [Green Version]
- Al-Anani, S.J.; Weber, H.; Hijazi, Z.M. Atrioventricular block after transcatheter ASD closure using the Amplatzer septal occluder: Risk factors and recommendations. Catheter. Cardiovasc. Interv. 2010, 75, 767–772. [Google Scholar] [CrossRef]
- Figueras-Coll, M.; Sabaté-Rotés, A.; Roguera-Sopena, M.; Betrián-Blasco, P. Reversible atrioventricular block after atrial septal defect closure with a Gore Cardioform Septal Occluder. Arch. Cardiol. Méx. 2020, 90, 90–92. [Google Scholar] [CrossRef]
- Thanopoulos, B.V.D.; Soendergaard, L.; Ngugen, H.L.; Marasini, M.; Giannopoulos, A.; Bompotis, G.C.; Thonghong, T.; Krishnamoorthy, K.M.; Placid, S.; Deleanou, D.; et al. International experience with the use of Cocoon septal occluder for closure of atrial septal defects. Hell. J. Cardiol. 2021, 62, 206–211. [Google Scholar] [CrossRef]
- Roymanee, S.; Promphan, W.; Tonklang, N.; Wongwaitaweewong, K. Comparison of the Occlutech® Figulla® Septal Occluder and Amplatzer® Septal Occluder for Atrial Septal Defect Device Closure. Pediatr. Cardiol. 2015, 36, 935–941. [Google Scholar] [CrossRef]
- Astarcioglu, M.A.; Kalcik, M.; Sen, T.; Aykan, A.C.; Gokdeniz, T.; Gursoy, O.M.; Karakoyun, S.; Kulahcioglu, S.; Gunduz, S.; Kilit, C.; et al. Ceraflex versus Amplatzer occluder for secundum atrial septal defect closure. Herz 2015, 40, 146–150. [Google Scholar] [CrossRef]
- Sievert, K.; Bertog, S.; Söderberg, B.; Gafoor, S.; Hofmann, I.; Grunwald, I.; Schnelle, N.; Sievert, H. Transcatheter closure of atrial septal defect and patent foramen ovale with Carag bioresorbable septal occluder: First-in-man experience with 24-month follow-up. EuroIntervention 2021. [Google Scholar] [CrossRef]
- Hoffman, J.I.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef] [Green Version]
- Holzer, R.; Balzer, D.; Cao, Q.L.; Lock, K.; Hijazi, Z.M. Device closure of muscular ventricular septal defects using the Amplatzer muscular ventricular septal defect occluder: Immediate and mid-term results of a U.S. registry. J. Am. Coll. Cardiol. 2004, 43, 1257–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hijazi, Z.M.; Hakim, F.; Al-Fadley, F.; Abdelhamid, J.; Cao, Q.L. Transcatheter closure of single muscular ventricular septal defects using the amplatzer muscular VSD occluder: Initial results and technical considerations. Catheter. Cardiovasc. Interv. 2000, 49, 167–172. [Google Scholar] [CrossRef]
- Bacha, E.A.; Cao, Q.-L.; Starr, J.P.; Waight, D.; Ebeid, M.R.; Hijazi, Z.M. Perventricular device closure of muscular ventricular septal defects on the beating heart: Technique and results. J. Thorac. Cardiovasc. Surg. 2003, 126, 1718–1723. [Google Scholar] [CrossRef] [Green Version]
- Ng, L.Y.; Al-Alawi, K.; Breatnach, C.; Nolke, L.; Redmond, M.; McCrossan, B.; Oslizlok, P.; Walsh, K.P.; McGuinness, J.; Kenny, D. Hybrid Subxiphoid Perventricular Approach as an Alternative Access in Neonates and Small Children Undergoing Complex Congenital Heart Interventions. Pediatr. Cardiol. 2021, 42, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Sadiq, M.; Qureshi, A.U.; Younas, M.; Arshad, S.; Hyder, S.N. Percutaneous closure of ventricular septal defect using LifeTechTM Konar-MF VSD Occluder: Initial and short-term multi-institutional results. Cardiol. Young 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.; Germann, C.P.; Nordmeyer, J.; Peters, B.; Berger, F.; Schubert, S. Short- and Long-term Outcome after Interventional VSD Closure: A Single-Center Experience in Pediatric and Adult Patients. Pediatr. Cardiol. 2021, 42, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Trezzi, M.; Kavarana, M.N.; Hlavacek, A.M.; Bradley, S.M. Left ventricular pseudoaneurysm after perventricular ventricular septal defect device closure. J. Card. Surg. 2014, 29, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Tzikas, A.; Ibrahim, R.; Velasco-Sanchez, D.; Freixa, X.; Alburquenque, M.; Khairy, P.; Bass, J.L.; Ramirez, J.; Aguirre, D.; Miro, J. Transcatheter closure of perimembranous ventricular septal defect with the Amplatzer®membranous VSD occluder 2: Initial world experience and one-year follow-up. Catheter. Cardiovasc. Interv. 2014, 83, 571–580. [Google Scholar] [CrossRef]
- Mijangos-Vázquez, R.; El-Sisi, A.; Sandoval Jones, J.P.; García-Montes, J.A.; Hernández-Reyes, R.; Sobhy, R.; Abdelmassih, A.; Soliman, M.M.; Ali, S.; Molina-Sánchez, T.; et al. Transcatheter Closure of Perimembranous Ventricular Septal Defects Using Different Generations of Amplatzer Devices: Multicenter Experience. J. Interv. Cardiol. 2020, 2020, 8948249. [Google Scholar] [CrossRef] [Green Version]
- Singhi, A.K.; Sivakumar, K. Echocardiographic Classification of Perimembranous Ventricular Septal Defect Guides Selection of the Occluder Design for Their Transcatheter Device Closure. J. Cardiovasc. Imaging 2021, 29, 316. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhang, W.; Li, J.; Wang, S.; Qian, M.; Shi, J.; Xie, Y.; Zhang, Z. Transcatheter Closure of Perimembranous and Intracristal Ventricular Septal Defects Using Amplatzer Duct Occluder II in Children. J. Interv. Cardiol. 2021, 2021, 4091888. [Google Scholar] [CrossRef] [PubMed]
- Porstmann, W.; Wierny, L.; Warnke, H. Closure of persistent ductus arteriosus without thoracotomy. Ger. Med. Mon. 1967, 12, 259–261. [Google Scholar]
- Gałeczka, M.; Szkutnik, M.; Białkowski, J.; Litwin, L.; Smerdziński, S.; Knop, M.; Głowacki, J.; Fiszer, R. Transcatheter patent ductus arteriosus closure: What have we learned after over 25 years? A single-center experience with 1036 patients. Kardiol. Pol. 2021, 79, 287–293. [Google Scholar] [CrossRef]
- Sathanandam, S.K.; Gutfinger, D.; O’Brien, L.; Forbes, T.J.; Gillespie, M.J.; Berman, D.P.; Armstrong, A.K.; Shahanavaz, S.; Jones, T.K.; Morray, B.H.; et al. Amplatzer Piccolo Occluder clinical trial for percutaneous closure of the patent ductus arteriosus in patients ≥700 grams. Catheter. Cardiovasc. Interv. 2020, 96, 1266–1276. [Google Scholar] [CrossRef]
- Rao, P.S.; Sideris, E.B.; Haddad, J.; Rey, C.; Hausdorf, G.; Wilson, A.D.; Smith, P.A.; Chopra, P.S. Transcatheter occlusion of patent ductus arteriosus with adjustable buttoned device. Initial clinical experience. Circulation 1993, 88, 1119–1126. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, D.; Salem, M.M.; Forbes, T.J.; Gordon, B.M.; Soriano, B.D.; Dimas, V.; Goldstein, B.H.; Owada, C.; Javois, A.; Bass, J.; et al. Results of the combined U.S. multicenter postapproval study of the Nit-Occlud PDA device for percutaneous closure of patent ductus arteriosus. Catheter. Cardiovasc. Interv. 2019, 93, 645–651. [Google Scholar] [CrossRef]
- Heyden, C.M.; El-Said, H.G.; Moore, J.W.; Guyon, P.W., Jr.; Katheria, A.C.; Ratnayaka, K. Early experience with the Micro Plug Set for preterm patent ductus arteriosus closure. Catheter. Cardiovasc. Interv. 2020, 96, 1439–1444. [Google Scholar] [CrossRef]
- Sathanandam, S.; Justino, H.; Waller, B.R., 3rd; Radtke, W.; Qureshi, A.M. Initial clinical experience with the Medtronic Micro Vascular Plug™ in transcatheter occlusion of PDAs in extremely premature infants. Catheter. Cardiovasc. Interv. 2017, 89, 1051–1058. [Google Scholar] [CrossRef]
- Wang-Giuffre, E.W.; Breinholt, J.P. Novel use of the medtronic micro vascular plug for PDA closure in preterm infants. Catheter. Cardiovasc. Interv. 2017, 89, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Peters, B.; Ewert, P.; Berger, F. The role of stents in the treatment of congenital heart disease: Current status and future perspectives. Ann. Pediatr. Cardiol. 2009, 2, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Trant, C.A.; O’Laughlin, M.P.; Ungerleider, R.M.; Garson, A. Cost-Effectiveness Analysis of Stents, Balloon Angioplasty, and Surgery for the Treatment of Branch Pulmonary Artery Stenosis. Pediatr. Cardiol. 1997, 18, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Glatz, A.C.; Petit, C.J.; Goldstein, B.H.; Kelleman, M.S.; McCracken, C.E.; McDonnell, A.; Buckey, T.; Mascio, C.E.; Shashidharan, S.; Ligon, R.A.; et al. Comparison between Patent Ductus Arteriosus Stent and Modified Blalock-Taussig Shunt as Palliation for Infants with Ductal-Dependent Pulmonary Blood Flow. Circulation 2018, 137, 589–601. [Google Scholar] [CrossRef] [PubMed]
- Bauser-Heaton, H.; Qureshi, A.M.; Goldstein, B.H.; Glatz, A.C.; Ligon, R.A.; Gartenberg, A.; Aggarwal, V.; Shashidharan, S.; McCracken, C.E.; Kelleman, M.S.; et al. Comparison of Patent Ductus Arteriosus Stent and Blalock–Taussig Shunt as Palliation for Neonates with Sole Source Ductal-Dependent Pulmonary Blood Flow: Results from the Congenital Catheterization Research Collaborative. Pediatr. Cardiol. 2022, 43, 121–131. [Google Scholar] [CrossRef]
- Eilers, L.; Qureshi, A.M. Advances in Pediatric Ductal Intervention: An Open or Shut Case? Curr. Cardiol. Rep. 2020, 22, 14. [Google Scholar] [CrossRef]
- Nicholson, G.T.; Glatz, A.C.; Qureshi, A.M.; Petit, C.J.; Meadows, J.J.; McCracken, C.; Kelleman, M.; Bauser-Heaton, H.; Gartenberg, A.J.; Ligon, R.A.; et al. Impact of Palliation Strategy on Interstage Feeding and Somatic Growth for Infants with Ductal-Dependent Pulmonary Blood Flow: Results from the Congenital Catheterization Research Collaborative. J. Am. Heart Assoc. 2020, 9, e013807. [Google Scholar] [CrossRef]
- Schranz, D.; Zartner, P.; Michel-Behnke, I.; Akinturk, H. Bioabsorbable metal stents for percutaneous treatment of critical recoarctation of the aorta in a newborn. Catheter. Cardiovasc. Interv. 2006, 67, 671–673. [Google Scholar] [CrossRef]
- Herbert, C.E.; Veeram Reddy, S.; Welch, T.R.; Wang, J.; Richardson, J.A.; Forbess, J.M.; Nugent, A.W. Bench and initial preclinical results of a novel 8 mm diameter double opposed helical biodegradable stent. Catheter. Cardiovasc. Interv. 2016, 88, 902–911. [Google Scholar] [CrossRef]
- Shibbani, K.; De Lima, E.S.B.L.; Poulin, M.F.; Matella, T.; Diab, K.; Kavinsky, C.; Ramesh, N.; Bhat, V.; Hijazi, Z.M.; Kenny, D. Preclinical comparative assessment of a dedicated pediatric poly-L-lactic-acid-based bioresorbable scaffold with a low-profile bare metal stent. Catheter. Cardiovasc. Interv. 2020, 96, 878–888. [Google Scholar] [CrossRef]
- Ewert, P.; Riesenkampff, E.; Neuss, M.; Kretschmar, O.; Nagdyman, N.; Lange, P.E. Novel growth stent for the permanent treatment of vessel stenosis in growing children: An experimental study. Catheter. Cardiovasc. Interv. 2004, 62, 506–510. [Google Scholar] [CrossRef]
- Zahn, E.M.; Abbott, E.; Tailor, N.; Sathanandam, S.; Armer, D. Preliminary testing and evaluation of the renata minima stent, an infant stent capable of achieving adult dimensions. Catheter. Cardiovasc. Interv. 2021, 98, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Quandt, D.; Knirsch, W.; Michel-Behnke, I.; Kitzmuller, E.; Obradovic, M.; Uhlemann, F.; Kretschmar, O. First-in-man pulmonary artery stenting in children using the Bentley(R) BeGrow stent system for newborns and infants. Int. J. Cardiol. 2019, 276, 107–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boudjemline, Y.; Massih, T.A.; Bonhoeffer, P. Transcatheter reconstruction of the right heart. Cardiol. Young 2003, 13, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Holzer, R.J.; Hijazi, Z.M. Transcatheter pulmonary valve replacement: State of the art. Catheter. Cardiovasc. Interv. 2016, 87, 117–128. [Google Scholar] [CrossRef]
- Sinha, S.; Aboulhosn, J.; Asnes, J.; Bocks, M.; Zahn, E.; Goldstein, B.H.; Zampi, J.; Hellenbrand, W.; Salem, M.; Levi, D. Initial results from the off-label use of the SAPIEN S3 valve for percutaneous transcatheter pulmonary valve replacement: A multi-institutional experience. Catheter. Cardiovasc. Interv. 2019, 93, 455–463. [Google Scholar] [CrossRef]
- Shahanavaz, S.; Zahn, E.M.; Levi, D.S.; Aboulhousn, J.A.; Hascoet, S.; Qureshi, A.M.; Porras, D.; Morgan, G.J.; Bauser Heaton, H.; Martin, M.H.; et al. Transcatheter Pulmonary Valve Replacement with the Sapien Prosthesis. J. Am. Coll. Cardiol. 2020, 76, 2847–2858. [Google Scholar] [CrossRef]
- Benson, L.N.; Gillespie, M.J.; Bergersen, L.; Cheatham, S.L.; Hor, K.N.; Horlick, E.M.; Weng, S.; McHenry, B.T.; Osten, M.D.; Powell, A.J.; et al. Three-Year Outcomes from the Harmony Native Outflow Tract Early Feasibility Study. Circ. Cardiovasc. Interv. 2020, 13, e008320. [Google Scholar] [CrossRef]
- Shahanavaz, S.; Balzer, D.; Babaliaros, V.; Kim, D.; Dimas, V.; Veeram Reddy, S.R.; Leipsic, J.; Blanke, P.; Shirali, G.; Parthiban, A.; et al. Alterra Adaptive Prestent and SAPIEN 3 THV for Congenital Pulmonic Valve Dysfunction: An Early Feasibility Study. JACC Cardiovasc. Interv. 2020, 13, 2510–2524. [Google Scholar] [CrossRef]
- Zahn, E.M.; Chang, J.C.; Armer, D.; Garg, R. First human implant of the Alterra Adaptive Prestent™: A new self-expanding device designed to remodel the right ventricular outflow tract. Catheter. Cardiovasc. Interv. 2018, 91, 1125–1129. [Google Scholar] [CrossRef] [Green Version]
- Bergersen, L.; Benson, L.N.; Gillespie, M.J.; Cheatham, S.L.; Crean, A.M.; Hor, K.N.; Horlick, E.M.; Lung, T.H.; McHenry, B.T.; Osten, M.D.; et al. Harmony Feasibility Trial: Acute and Short-Term Outcomes with a Self-Expanding Transcatheter Pulmonary Valve. JACC Cardiovasc. Interv. 2017, 10, 1763–1773. [Google Scholar] [CrossRef]
- Stout, K.K.; Daniels, C.J.; Aboulhosn, J.A.; Bozkurt, B.; Broberg, C.S.; Colman, J.M.; Crumb, S.R.; Dearani, J.A.; Fuller, S.; Gurvitz, M.; et al. 2018 AHA/ACC Guideline for the Management of Adults with Congenital Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e698–e800. [Google Scholar] [CrossRef] [PubMed]
- Lehner, A.; Haas, N.A.; Dietl, M.; Jakob, A.; Schulze-Neick, I.; Dalla Pozza, R.; Rodriguez, S.F.; Fischer, M. The risk of infective endocarditis following interventional pulmonary valve implantation: A meta-analysis. J. Cardiol. 2019, 74, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Hascoet, S.; Mauri, L.; Claude, C.; Fournier, E.; Lourtet, J.; Riou, J.Y.; Brenot, P.; Petit, J. Infective Endocarditis Risk after Percutaneous Pulmonary Valve Implantation with the Melody and Sapien Valves. JACC Cardiovasc. Interv. 2017, 10, 510–517. [Google Scholar] [CrossRef] [PubMed]
- McElhinney, D.B.; Sondergaard, L.; Armstrong, A.K.; Bergersen, L.; Padera, R.F.; Balzer, D.T.; Lung, T.H.; Berger, F.; Zahn, E.M.; Gray, R.G.; et al. Endocarditis after Transcatheter Pulmonary Valve Replacement. J. Am. Coll. Cardiol. 2018, 72, 2717–2728. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, M.J.; Bergersen, L.; Benson, L.N.; Weng, S.; Cheatham, J.P. 5-Year Outcomes from the Harmony Native Outflow Tract Early Feasibility Study. JACC Cardiovasc. Interv. 2021, 14, 816–817. [Google Scholar] [CrossRef]
- Sivakumar, K.; Sagar, P.; Qureshi, S.; Promphan, W.; Sasidharan, B.; Awasthy, N.; Kappanayil, M.; Suresh, P.V.; Koneti, N.R. Outcomes of Venus p-valve for dysfunctional right ventricular outflow tracts from Indian Venus p-valve database. Ann. Pediatr. Cardiol. 2021, 14, 281–292. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, G.B.; Kim, S.H.; Jang, S.I.; Choi, J.Y.; Kang, I.S.; Kim, Y.H. Mid-term outcomes of the Pulsta transcatheter pulmonary valve for the native right ventricular outflow tract. Catheter. Cardiovasc. Interv. 2021, 98, E724–E732. [Google Scholar] [CrossRef]
- Zhang, X.; Puehler, T.; Seiler, J.; Gorb, S.N.; Sathananthan, J.; Sellers, S.; Haneya, A.; Hansen, J.-H.; Uebing, A.; Müller, O.J.; et al. Tissue Engineered Transcatheter Pulmonary Valved Stent Implantation: Current State and Future Prospect. Int. J. Mol. Sci. 2022, 23, 723. [Google Scholar] [CrossRef]
- Kalfa, D. Novel Valve Choices for Pulmonary Valve Replacement. In Seminars in Thoracic and Cardiovascular Surgery; 2022. Available online: https://pubmed.ncbi.nlm.nih.gov/35032644/ (accessed on 1 February 2022). [CrossRef]
- McElhinney, D.B.; Marx, G.R.; Newburger, J.W. Congenital Portosystemic Venous Connections and Other Abdominal Venous Abnormalities in Patients with Polysplenia and Functionally Univentricular Heart Disease: A Case Series and Literature Review. Congenit. Heart Dis. 2011, 6, 28–40. [Google Scholar] [CrossRef]
- Glatz, A.C.; Harrison, N.; Small, A.J.; Dori, Y.; Gillespie, M.J.; Harris, M.A.; Fogel, M.A.; Rome, J.J.; Whitehead, K.K. Factors associated with systemic to pulmonary arterial collateral flow in single ventricle patients with superior cavopulmonary connections. Heart 2015, 101, 1813–1818. [Google Scholar] [CrossRef]
- Whitehead, K.K.; Harris, M.A.; Glatz, A.C.; Gillespie, M.J.; Dimaria, M.V.; Harrison, N.E.; Dori, Y.; Keller, M.S.; Rome, J.J.; Fogel, M.A. Status of Systemic to Pulmonary Arterial Collateral Flow after the Fontan Procedure. Am. J. Cardiol. 2015, 115, 1739–1745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammad Nijres, B.; Aregullin, E.O.; Al-Khatib, Y.; Samuel, B.P.; Abdulla, R.-I.; Hijazi, Z.M.; Vettukattil, J.J. Aortopulmonary Collaterals in Single Ventricle Physiology: Variation in Understanding Occlusion Practice among Interventional Cardiologists. Pediatr. Cardiol. 2020, 41, 1608–1616. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, M.; Breuer, J.; Steger, V.; Steil, E.; Sieverding, L.; Ziemer, G. Incidence and Impact of Systemic Venous Collateral Development after Glenn and Fontan Procedures. Thorac. Cardiovasc. Surg. 2001, 49, 172–178. [Google Scholar] [CrossRef] [PubMed]
- O’Byrne, M.L.; Schidlow, D.N. Durable Benefit of Particle Occlusion of Systemic to Pulmonary Collaterals in Select Patients after Superior Cavopulmonary Connection. Pediatr. Cardiol. 2018, 39, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Poterucha, J.T.; Johnson, J.N.; Taggart, N.W.; Cabalka, A.K.; Hagler, D.J.; Driscoll, D.J.; Cetta, F. Embolization of Veno-venous Collaterals after the Fontan Operation Is Associated with Decreased Survival. Congenit. Heart Dis. 2015, 10, E230–E236. [Google Scholar] [CrossRef] [PubMed]
- Prakash, A.; Rathod, R.H.; Powell, A.J.; McElhinney, D.B.; Banka, P.; Geva, T. Relation of Systemic-to-Pulmonary Artery Collateral Flow in Single Ventricle Physiology to Palliative Stage and Clinical Status. Am. J. Cardiol. 2012, 109, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Ait Ali, L.; Cadoni, A.; Rossi, G.; Keilberg, P.; Passino, C.; Festa, P. Effective Cardiac Index and Systemic-Pulmonary Collaterals Evaluated by Cardiac Magnetic Resonance Late after Fontan Palliation. Am. J. Cardiol. 2017, 119, 2069–2072. [Google Scholar] [CrossRef]
- Goldstein, B.H.; Aiyagari, R.; Bocks, M.L.; Armstrong, A.K. Hydrogel Expandable Coils for Vascular Occlusion in Congenital Cardiovascular Disease: A Single Center Experience. Congenit. Heart Dis. 2012, 7, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Zhang, F.; Ouyang, W.; Zhao, G.; Lu, W.; Zou, M.; Pan, X. Transcatheter Closure of Patent Ductus Arteriosus under Echocardiography Guidance: A Randomized Controlled Noninferiority Trial. J. Interv. Cardiol. 2020, 2020, 4357017. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, W.; Wu, Q.; Gao, L.; Jin, W.; Zhao, T. Transcatheter closure of atrial septal defects without fluoroscopy: A well-established procedure for alternative use in children. EuroIntervention 2016, 12, e652–e657. [Google Scholar] [CrossRef]
- Bu, H.; Yang, Y.; Wu, Q.; Jin, W.; Zhao, T. Echocardiography-guided percutaneous closure of perimembranous ventricular septal defects without arterial access and fluoroscopy. BMC Pediatr. 2019, 19, 302. [Google Scholar] [CrossRef] [PubMed]
- Medford, B.A.; Taggart, N.W.; Cabalka, A.K.; Cetta, F.; Reeder, G.S.; Hagler, D.J.; Johnson, J.N. Intracardiac echocardiography during atrial septal defect and patent foramen ovale device closure in pediatric and adolescent patients. J. Am. Soc. Echocardiogr. 2014, 27, 984–990. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Cao, Q.-L.; Koenig, P.R.; Hijazi, Z.M. Intracardiac echocardiography to guide closure of atrial septal defects in children less than 15 kilograms. Catheter. Cardiovasc. Interv. 2006, 68, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Valsangiacomo Buechel, E.R.; Grosse-Wortmann, L.; Fratz, S.; Eichhorn, J.; Sarikouch, S.; Greil, G.F.; Beerbaum, P.; Bucciarelli-Ducci, C.; Bonello, B.; Sieverding, L.; et al. Indications for cardiovascular magnetic resonance in children with congenital and acquired heart disease: An expert consensus paper of the Imaging Working Group of the AEPC and the Cardiovascular Magnetic Resonance Section of the EACVI. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 281–297. [Google Scholar] [CrossRef]
- Pushparajah, K.; Duong, P.; Mathur, S.; Babu-Narayan, S.V. Educational Series in Congenital Heart Disease: Cardiovascular MRI and CT in congenital heart disease. Echo Res. Pract. 2019, 6, R121–R138. [Google Scholar] [CrossRef] [Green Version]
- Illmann, C.F.; Hosking, M.; Harris, K.C. Utility and Access to 3-Dimensional Printing in the Context of Congenital Heart Disease: An International Physician Survey Study. CJC Open 2020, 2, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Batteux, C.; Meliani, A.; Brenot, P.; Hascoet, S. Multimodality fusion imaging to guide percutaneous sinus venosus atrial septal defect closure. Eur. Heart J. 2020, 41, 4444–4445. [Google Scholar] [CrossRef]
- Cantinotti, M.; Valverde, I.; Kutty, S. Three-dimensional printed models in congenital heart disease. Int. J. Cardiovasc. Imaging 2017, 33, 137–144. [Google Scholar] [CrossRef]
- Moore, R.A.; Riggs, K.W.; Kourtidou, S.; Schneider, K.; Szugye, N.; Troja, W.; D’Souza, G.; Rattan, M.; Bryant, R., 3rd; Taylor, M.D.; et al. Three-dimensional printing and virtual surgery for congenital heart procedural planning. Birth Defects Res. 2018, 110, 1082–1090. [Google Scholar] [CrossRef]
- Forte, M.N.V.; Hussain, T.; Roest, A.; Gomez, G.; Jongbloed, M.; Simpson, J.; Pushparajah, K.; Byrne, N.; Valverde, I. Living the heart in three dimensions: Applications of 3D printing in CHD. Cardiol. Young 2019, 29, 733–743. [Google Scholar] [CrossRef]
- Thakkar, A.N.; Chinnadurai, P.; Breinholt, J.P.; Lin, C.H. Transcatheter closure of a sinus venosus atrial septal defect using 3D printing and image fusion guidance. Catheter. Cardiovasc. Interv. 2018, 92, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasco Forte, M.N.; Byrne, N.; Valverde, I.; Gomez Ciriza, G.; Hermuzi, A.; Prachasilchai, P.; Mainzer, G.; Pushparajah, K.; Henningsson, M.; Hussain, T.; et al. Interventional Correction of Sinus Venosus Atrial Septal Defect and Partial Anomalous Pulmonary Venous Drainage: Procedural Planning Using 3D Printed Models. JACC Cardiovasc. Imaging 2018, 11, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Valverde, I.; Gomez, G.; Coserria, J.F.; Suarez-Mejias, C.; Uribe, S.; Sotelo, J.; Velasco, M.N.; Santos De Soto, J.; Hosseinpour, A.R.; Gomez-Cia, T. 3D printed models for planning endovascular stenting in transverse aortic arch hypoplasia. Catheter. Cardiovasc. Interv. 2015, 85, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Pluchinotta, F.R.; Sturla, F.; Caimi, A.; Giugno, L.; Chessa, M.; Giamberti, A.; Votta, E.; Redaelli, A.; Carminati, M. 3-Dimensional personalized planning for transcatheter pulmonary valve implantation in a dysfunctional right ventricular outflow tract. Int. J. Cardiol. 2020, 309, 33–39. [Google Scholar] [CrossRef]
- Velasco Forte, M.N.; Byrne, N.; Valverde Perez, I.; Bell, A.; Gómez-Ciriza, G.; Krasemann, T.; Sievert, H.; Simpson, J.; Pushparajah, K.; Razavi, R.; et al. 3D printed models in patients with coronary artery fistulae: Anatomical assessment and interventional planning. EuroIntervention 2017, 13, e1080–e1083. [Google Scholar] [CrossRef]
- Kern, M.C.; Janardhanan, R.; Kelly, T.; Fox, K.A.; Klewer, S.E.; Seckeler, M.D. Multimodality imaging for diagnosis and procedural planning for a ruptured sinus of Valsalva aneurysm. J. Cardiovasc. Comput. Tomogr. 2020, 14, e139–e142. [Google Scholar] [CrossRef]
- Davies, R.R.; Hussain, T.; Tandon, A. Using virtual reality simulated implantation for fit-testing pediatric patients for adult ventricular assist devices. JTCVS Tech. 2021, 6, 134–137. [Google Scholar] [CrossRef]
- Tandon, A.; Burkhardt, B.E.U.; Batsis, M.; Zellers, T.M.; Velasco Forte, M.N.; Valverde, I.; McMahan, R.P.; Guleserian, K.J.; Greil, G.F.; Hussain, T. Sinus Venosus Defects: Anatomic Variants and Transcatheter Closure Feasibility Using Virtual Reality Planning. JACC Cardiovasc. Imaging 2019, 12, 921–924. [Google Scholar] [CrossRef]
- Ghosh, R.M.; Mascio, C.E.; Rome, J.J.; Jolley, M.A.; Whitehead, K.K. Use of Virtual Reality for Hybrid Closure of Multiple Ventricular Septal Defects. JACC Case Rep. 2021, 3, 1579–1583. [Google Scholar] [CrossRef]
- Jone, P.N.; Ross, M.M.; Bracken, J.A.; Mulvahill, M.J.; Di Maria, M.V.; Fagan, T.E. Feasibility and Safety of Using a Fused Echocardiography/Fluoroscopy Imaging System in Patients with Congenital Heart Disease. J. Am. Soc. Echocardiogr. 2016, 29, 513–521. [Google Scholar] [CrossRef]
- Jone, P.N.; Haak, A.; Ross, M.; Wiktor, D.M.; Gill, E.; Quaife, R.A.; Messenger, J.C.; Salcedo, E.E.; Carroll, J.D. Congenital and Structural Heart Disease Interventions Using Echocardiography-Fluoroscopy Fusion Imaging. J. Am. Soc. Echocardiogr. 2019, 32, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Hadeed, K.; Hascoët, S.; Karsenty, C.; Ratsimandresy, M.; Dulac, Y.; Chausseray, G.; Alacoque, X.; Fraisse, A.; Acar, P. Usefulness of echocardiographic-fluoroscopic fusion imaging in children with congenital heart disease. Arch. Cardiovasc. Dis. 2018, 111, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Grant, E.K.; Kanter, J.P.; Olivieri, L.J.; Cross, R.R.; Campbell-Washburn, A.; Faranesh, A.Z.; Cronin, I.; Hamann, K.S.; O’Byrne, M.L.; Slack, M.C.; et al. X-ray fused with MRI guidance of pre-selected transcatheter congenital heart disease interventions. Catheter. Cardiovasc. Interv. 2019, 94, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Fagan, T.E.; Truong, U.T.; Jone, P.N.; Bracken, J.; Quaife, R.; Hazeem, A.A.; Salcedo, E.E.; Fonseca, B.M. Multimodality 3-dimensional image integration for congenital cardiac catheterization. Methodist Debakey Cardiovasc. J. 2014, 10, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Ehret, N.; Alkassar, M.; Dittrich, S.; Cesnjevar, R.; Rüffer, A.; Uder, M.; Rompel, O.; Hammon, M.; Glöckler, M. A new approach of three-dimensional guidance in paediatric cath lab: Segmented and tessellated heart models for cardiovascular interventions in CHD. Cardiol. Young 2018, 28, 661–667. [Google Scholar] [CrossRef]
- Sumdani, H.; Aguilar-Salinas, P.; Avila, M.J.; Barber, S.R.; Dumont, T. Utility of Augmented Reality and Virtual Reality in Spine Surgery: A Systematic Review of the Literature. World Neurosurg. 2021. [Google Scholar] [CrossRef]
- Currie, M.E.; McLeod, A.J.; Moore, J.T.; Chu, M.W.A.; Patel, R.; Kiaii, B.; Peters, T.M. Augmented Reality System for Ultrasound Guidance of Transcatheter Aortic Valve Implantation. Innov. Technol. Tech. Cardiothorac. Vasc. Surg. 2016, 11, 31–39. [Google Scholar] [CrossRef]
- Opolski, M.P.; Michałowska, I.M.; Borucki, B.A.; Nicińska, B.; Szumowski, Ł.; Sterliński, M. Augmented-reality computed tomography-guided transcatheter pacemaker implantation in dextrocardia and congenitally corrected transposition of great arteries. Cardiol. J. 2018, 25, 412–413. [Google Scholar] [CrossRef]
- Fischer, G.A.; Wells, S.M.; Rebuffoni, J.F.; Peterson, B.M.; LeBien, T.W. A model for overcoming challenges in academic pediatric medical device innovation. J. Clin. Transl. Sci. 2019, 3, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Section on Cardiology and Cardiac Surgery; Section on Orthopaedics; Jenkins, K.J.; Beekman, R.H.; Vitale, M.G.; Hennrikus, W.; Minich, L.L.; Ackerman, M.J.; Berger, S.; Jaquiss, R.D.B.; et al. Off-Label Use of Medical Devices in Children. Pediatrics 2017, 139, e20163439. [Google Scholar] [CrossRef] [Green Version]
- Kaushik, A.; Saini, K.; Anil, B.; Rambabu, S. Harmonized Medical Device Regulation: Need, Challenges, and Risks of not Harmonizing the Regulation in Asia. J. Young Pharm. 2010, 2, 101–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Divekar, A.A.; Arar, Y.M.; Clark, S.; Tandon, A.; Zellers, T.M.; Veeram Reddy, S.R. Transcatheter Device Therapy and the Integration of Advanced Imaging in Congenital Heart Disease. Children 2022, 9, 497. https://doi.org/10.3390/children9040497
Divekar AA, Arar YM, Clark S, Tandon A, Zellers TM, Veeram Reddy SR. Transcatheter Device Therapy and the Integration of Advanced Imaging in Congenital Heart Disease. Children. 2022; 9(4):497. https://doi.org/10.3390/children9040497
Chicago/Turabian StyleDivekar, Abhay A., Yousef M. Arar, Stephen Clark, Animesh Tandon, Thomas M. Zellers, and Surendranath R. Veeram Reddy. 2022. "Transcatheter Device Therapy and the Integration of Advanced Imaging in Congenital Heart Disease" Children 9, no. 4: 497. https://doi.org/10.3390/children9040497
APA StyleDivekar, A. A., Arar, Y. M., Clark, S., Tandon, A., Zellers, T. M., & Veeram Reddy, S. R. (2022). Transcatheter Device Therapy and the Integration of Advanced Imaging in Congenital Heart Disease. Children, 9(4), 497. https://doi.org/10.3390/children9040497