Highlights
What are the main findings?
- Psychosocial burden, including impaired body image, social anxiety, and low quality of life, is significant in adolescents and young adults with pectus excavatum and pectus carinatum, often manifesting as social avoidance, concealment behaviors, and emotional distress.
- Surgical and non-surgical correction of chest wall deformities markedly improves body image, self-esteem, social participation, and mental health scores, with benefits sustained long-term.
What are the implications of the main findings?
- Routine psychosocial screening and incorporation of psychologists into chest wall deformity clinics are essential for optimizing outcomes.
- Expansion of insurance coverage beyond anatomic criteria to include psychological indications can help mitigate long-term emotional distress.
Abstract
Progression of pectus excavatum and carinatum coincides with adolescence, a critical period for identity and self-esteem development. While clinical decision-making and insurance coverage have historically emphasized anatomic severity and cardiopulmonary functioning, increasing evidence suggests that psychosocial burden and quality of life (QoL) impairment represent central components of disease impact. A narrative review was conducted using the PubMed database to synthesize the current literature on the psychological impact of these deformities in adolescents and young adults, including body image distress, social functioning, and mental health effects before and after surgical and non-surgical correction, focusing on validated tools and qualitative studies. Across multiple cohorts, adolescents and young adults with chest wall deformities consistently report impaired body image, reduced self-esteem, social avoidance, and diminished QoL, even in the absence of diagnosable psychiatric disorders. Surgical and non-surgical corrections have positive effects in these domains. Psychological burden, therefore, represents a clinically meaningful component of chest wall deformities and should be considered alongside anatomic and physiologic criteria. Current evidence advocates for the integration of standardized psychosocial screening and support into evaluation and follow-up, which is essential for providing comprehensive, patient-centered care. Greater recognition of psychosocial outcomes may inform advocacy for broader treatment criteria, increasing accessibility among affected individuals.
1. Introduction
Congenital chest wall deformities encompass a broad spectrum of disorders, including thoracic ectopia cordis, sternal clefts, Poland syndrome, Jeune syndrome, and the two most common deformities—pectus excavatum (PE) and pectus carinatum (PC) [1]. The pathophysiology of chest wall deformities is poorly established, with proposed mechanisms related to impairments in the costal hyaline cartilage structure and function, and progression is commonly seen during periods of rapid vertical growth, such as puberty [1,2,3]. Patients often present with a range of physical symptoms during this time, including dyspnea, exercise intolerance, and chest pain, or with psychological distress related to body-image concerns [1,4,5]. Current insurance-approved indications for repair in the United States focus on these physical symptoms and the severity of the chest wall deformity, typically measured by the Haller Index (HI), which is calculated as the ratio of the transverse chest diameter to the anterior–posterior distance between the sternum and spine. However, there is a growing body of literature to support the impact of chest wall deformities on patients’ body image, mental health, and quality of life (QoL).
The progression of PE and PC coincides with adolescence, a critical period for identity and self-esteem development. Feelings of dissatisfaction with one’s appearance often emerge during this time as comparison with peers violates their desire to fit in and appear “normal”. As a result, body image scores in adolescents with chest wall deformities have been shown to be consistently reduced compared to healthy controls and are correlated with impaired QoL [6,7]. Distress related to self-image manifests in social avoidance, concealment behaviors, and social anxiety disorders [7,8,9]. Given the significant psychosocial impact of chest wall deformities, the treatment of PE and PC (surgical repair or bracing) has a positive effect on body image, self-confidence, and overall QoL [6,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28].
This narrative review synthesizes the current literature on the psychological impact of PE and PC in adolescent and young adult patients, the validated assessments available to understand both patient and parental concerns, and the impact of chest wall correction on patient and parental well-being.
2. Methods
A narrative review was conducted to identify relevant studies published between January 1990 and November 2025 using the PubMed database. Search terms included the following combinations: “pectus excavatum”, “pectus carinatum”, “chest wall deformity”, “quality of life”, “psychological”, “psychosocial”, “mental health”, “body image”, “adolescent”, and “pediatric”. Additional articles were identified by a manual search of the cited references, including those referenced in systematic reviews. A reference librarian was consulted to supplement the search, and 21 relevant articles were identified, with 7 of them being new. Titles and abstracts were screened for relevance to the scope of this review. The selected studies are comprised of observational studies, systematic reviews, and validated instrument development studies that evaluate psychosocial outcomes in patients with PE or PC with an average age ≤ 25 years. Case reports, purely technical surgical descriptions, and studies without psychosocial endpoints were excluded. Abstracts without available full-text manuscripts and non-English language availability were also excluded.
3. Anatomic Basis of Chest Wall Deformities
PE is characterized by depression of the anterior chest wall and is the most common chest wall deformity, accounting for approximately 65–95% of all cases [1,5]. Although incidence and prevalence rates vary due to differences in diagnostic methods, it is estimated to occur in up to 8 per 1000 live births. Historically, PE was thought to have a male predominance as seen in clinical studies; however, a recent radiographic study demonstrated a female predominance [5,29]. While the exact mechanism of PE is not completely understood, there is consensus that the defect is present at birth but may not manifest until years later during the prepubertal period of rapid skeletal growth [1,3]. Proposed mechanisms relate to abnormalities in the costal hyaline cartilage structure and function, resulting in weakness or overgrowth and subsequent chest wall collapse. PE can occur independently or in association with other conditions, including scoliosis, Marfan syndrome, Ehlers–Danlos syndrome, Noonan syndrome, and neurofibromatosis [1,2,3,5]. Symptoms range from shortness of breath, exercise intolerance, lack of endurance, and chest pain to body image concerns [1,4,5]. Surgical management by the Nuss procedure, or less frequently the Ravitch procedure, is offered for patients with a Haller Index ≥ 3.25 in the U.S. [30]. Alternative therapies include an emerging external traction system to elevate the chest, called the taulinoplasty or Pectus Up procedure, and pectus implants, which correct the appearance but not the sternal depression of the chest wall, with a subpectoral silicone implant [31,32].
PC is the second most common chest wall deformity, characterized by protrusion of the anterior chest wall. Similar to PE, incidence and prevalence rates are difficult to establish, but PC is estimated to occur in 1 per 2500 live births, with a male predominance [33]. Symptoms are generally milder than in PE, oftentimes limited to psychological distress but sometimes also including thoracic pain, decreased endurance, or exertional dyspnea related to the fixed anterior–posterior diameter of the chest wall [1,5,34]. Orthotic bracing to apply compressive anterior-to-posterior force to depress the sternum is the first-line therapy, with reported success rates of 65–85% [1,5]. Surgical correction via the modified Ravitch procedure or a minimally invasive repair of pectus carinatum (known as an Abramson procedure or reverse Nuss procedure) is reserved for patients who fail conservative management [25,33,35,36].
5. Quality of Life (QoL) Assessment Tools
Assessing QoL in children with PE and PC is essential as psychosocial burden often exceeds physiologic impairment. While surgical criteria traditionally rely on anatomic severity (e.g., Haller Index), patient-reported outcomes provide a more nuanced understanding of functional limitations, emotional well-being, and social participation. Over the past two decades, several validated instruments, including generic and condition-specific questionnaires, have been employed to capture these dimensions.
5.1. Validated Questionnaires
Studies evaluating the psychosocial impact of PE and PC often rely on generic QoL and health-related quality of life (HRQoL) instruments, such as the Pediatric Quality of Life Inventory (PedsQL) or Short Form 36 (SF-36), to understand functional impacts (Table 1). These tools are valuable, as they allow for benchmarking against normative data and can track global health improvements post-intervention. However, they often fail to capture the appearance-related distress that has been shown to lead many adolescents to seek surgical intervention [6,22,40]. Condition-specific instruments like the Pectus Excavatum Evaluation Questionnaire (PEEQ) and Single Step Questionnaire (SSQ) provide critical insight into body image and perceived physical ability, domains that are strongly associated with psychosocial well-being (Table 1). Most commonly, studies employ a variety of assessment tools for a comprehensive understanding of the impact of chest wall deformities on QoL.
5.1.1. Pectus Excavatum Specific Assessment Tools
The Pectus Excavatum Evaluation Questionnaire (PEEQ) was the original PE-specific questionnaire developed by Lawson et al. in 2003 [11]. The PEEQ focuses on the domains of psychosocial well-being and physical functioning related to the individual’s chest appearance and concavity. Responses are given on a four-point Likert scale to reflect either the happiness or frequency of each component. Many studies using the PEEQ have shown the Nuss procedure to have a positive impact [11,15,19,45,46,47]. The tool has also been applied to patients with PC, both with and without adaptations [48,49]. Since its development, the PEEQ and its adaptations have been widely used to understand the QoL implications of chest wall deformities and how QoL is influenced by disease management, thereby increasing visibility of the psychological impacts of PE and PC.
The Nuss Questionnaire modified for Adults (NQ-mA) was adapted from the PEEQ by Krasopoulos et al. for use in adults through minor wording changes [13]. The NQ-mA also reverses the scoring of the first three questions to allow for summation of scoring, with higher scores indicating a better QoL. The questionnaire has also been used in the PC population, with one study renaming the survey to NQ-mP while keeping the questions and scoring the same [50]. Similar to the PEEQ, many studies using the NQ-mA have demonstrated a positive impact of surgical intervention on QoL for both PE and PC [13,14,23,40,50,51,52].
The Single Step Questionnaire (SSQ) was developed by Krasopoulos et al. to provide a simpler assessment more relevant to young adults, covering both pre- and post-operative feelings and outcomes [13]. The assessment was derived from the PEEQ and consists of 16 questions, with its design intended to allow for the degree of satisfaction from surgical intervention to be assessed not only by a single question, but also through the overall score. The nine studies reviewed that have used the SSQ for adolescents and young adults have all shown high levels of satisfaction following surgery [13,14,20,21,23,24,48,53]. While the questionnaire was created and validated for use at a single post-operative timepoint, Zuidema et al. demonstrated improvements at four timepoints following the Nuss procedure, thus expanding its use [53].
5.1.2. Pectus Carinatum Specific Assessment Tools
The Pectus Carinatum Body Image Quality of Life (PeCBI-QOL) Questionnaire was created by Paulson et al. to address the gap of limited PC-specific assessment tools [54]. Following a development phase and refinement process, the final questionnaire for patients includes 18 items focused on four domains: body image disturbance, treatment motivation/engagement, physical limitations, and social disadvantage. The parent component includes 15 items on the same domains, except with the addition of social disadvantage. The initial study on PeCBI-QOL found that following treatment, there was a significant improvement in overall PeCBI-QOL scores, with moderate patient–parent concordance [54].
5.1.3. Generic Assessment Tools
Short Form 36 (SF-36) is a generic HRQoL instrument created for adults that consists of 36 questions across two broad health indicators, the Physical Component Score (PCS) and Mental Component Score (MCS), which are divided into eight sub-domains. Subscales and summary scores range from 0 to 100 points, and higher scores indicate better HRQoL [23,55]. The SF-36 has been applied to at least five studies examining chest wall deformities, and a shorter version consisting of 12 questions has also been utilized [23,40,42,48,56,57].
Child Health Questionnaire (CHQ) is a pediatric-focused generic HRQoL instrument that assesses physical, emotional, social, and family functioning through parent and self-reported formats [58]. There are a variety of survey lengths, including short forms CHQ-CF45 and CHQ-PF28, and full-length CHQ-CF87 and CHQ-PF28 for both children and parents. Responses are given on a four or five-point Likert scale, with higher scores indicating better HRQoL. Given its multi-dimensional focus for both children and parents, the questionnaire and adaptations have been used extensively in the chest wall deformity population [14,16,45,56,59].
The Symptom Checklist-90 (SCL-90) and its revised version (SCL-90-R) have been used to evaluate a broad range of psychological symptoms and mental health disorders. The tool assesses three global indices—Global Severity Index (GSI), Positive Symptom Distress Index (PSDI), and Positive Symptom Total (PST)—and nine primary symptom dimensions, including somatization, obsessive-compulsiveness, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The tool has been used in at least three studies on PE [21,22,44].
The Pediatric Quality of Life Inventory (PedsQL) is a pediatric HRQoL instrument that has been widely used in pediatric research. PedsQL covers the domains of physical, emotional, social, and school functioning and has been applied in at least two studies of PE and PC [7,8].
Several studies have utilized semi-structured interviews to gain a broader understanding of how chest wall deformities have impacted patients in their own words [6,10,12,41]. Themes of social belonging, well-being, self-esteem, satisfaction, and empowerment have been identified, which correlate with the themes seen in commonly utilized questionnaires.

Table 1.
Commonly utilized questionnaires in pediatric chest wall deformity research.
Table 1.
Commonly utilized questionnaires in pediatric chest wall deformity research.
| Instrument | Domains | Target Audience | Frequency of Use | Strengths | Limitations |
|---|---|---|---|---|---|
| Pectus-Specific Questionnaires | |||||
| Pectus Excavatum Evaluation Questionnaire (PEEQ) [11] | Psychosocial & Physical | Developed for PE; has parent form | 8 studies | Condition-specific, sensitive to cosmetic outcomes, short (12 questions), parental version | Limited mental health assessment |
| Nuss Assessment Questionnaire Modified for Adults (NQ-mA) [13] | Psychosocial & Physical | Adapted PEEQ for adult PE use | 7 studies | Allows for score summation | Limited mental health assessment |
| Single Step Questionnaire (SSQ) [13] | Physical, Psychosocial, Postoperative pain & satisfaction | Developed for PE | 9 studies | Comprehensive assessment including surgery-related questions, short (16 questions) | Limited to post-operative use |
| Pectus Carinatum Body Image Quality of Life Questionnaire (PeCBI-QOL) [54] | Body Image, Treatment Motivation, Physical Limitations, & Social Limitations | Developed for PC | 1 study | Condition-specific, sensitive to cosmetic outcomes, parental version | Limited mental health assessment |
| General Questionnaires | |||||
| Short-Form 36 (SF-36) | Physical, Social, Physical Role Limitations, Emotional Role Limitations, Mental Health, Vitality, Bodily Pain, & General Health | Adult validated; used in adolescents | 5 studies | Norm-based scoring, 36 questions | Not pediatric-specific |
| Child Health Questionnaire (CHQ) [58] | Physical & Psychosocial | Parent (PF50) and child forms (CF87) | 5 studies | Comprehensive domains, parental version | Lengthy, generic |
| Symptom Checklist 90 (SCL-90) | Psychological & Psychiatric Conditions | General | 3 studies | Captures key mental health symptoms and disorders | Not HRQoL, narrow focus |
| Pediatric Quality of Life Inventory (PedsQL) | Physical, Emotional, Social, & School | Pediatric patients | 2 studies | Broad pediatric HRQoL coverage | Lacks body image specificity |
6. Surgical and Non-Surgical Treatment: Psychological Outcomes
Psychosocial outcomes are central to the management of PE and PC, as body image concerns and emotional distress often outweigh physiologic limitations [23,51]. Both surgical and non-surgical interventions aim to not only correct the anatomic chest wall deformity but also improve mental health, self-esteem, and QoL.
6.1. Surgical Management
6.1.1. Motivations for Surgery
The motivation to undergo surgical intervention for chest wall deformities varies based on psychological burden and physical symptoms. Motivations for those with PC are predominantly related to physical appearance, with different studies finding that 64–100% of patients sought surgery solely for appearance-related reasons [23,40,50]. Although less commonly reported, physical functioning was still identified as a motivating factor when considering surgery [23,40]. Patients with PE are also concerned about appearance, with 11–100% of individuals, depending on the study, citing it as the primary motivator [6,24,40]. However, physical symptoms play a more substantial role in PE than PC, with 21–31% electing for surgery due to physical symptoms alone [6,24,40], and 51% for both appearance and physical symptoms [40]. Verbal reactions from others have also been reported as a meaningful driver for surgical intervention in 15% of patients in one study [6].
Patients who elect for surgery typically demonstrate more negative pre-operative body satisfaction scores in comparison to those who choose non-operative management, as found in one study comparing those with PE and PC by choice of management [18]. Many adolescents who desire surgery self-advocate for evaluation, with one study identifying 59% of patients who educated themselves regarding pectus-related clinics and surgery before approaching their parents [22]. Together, these findings underscore that surgery is often pursued in response to persistent appearance-related distress, with physical symptoms often contributing to a lesser degree.
6.1.2. Postoperative Improvements
Surgical correction of PE and PC leads to significant improvements in both psychosocial and physical domains, as demonstrated by qualitative studies and quantitatively over time through condition-specific assessments. Of the eight studies reviewed that used the PEEQ, two reported pre- and post-operative scores, and both demonstrated improvements across all domains (Figure 1) [11,46]. Similarly, four of the seven studies that used the NQ-mA had pre- and post-operative scores available, with improvements seen in each domain and overall (Figure 2A,B) [13,23,50,51]. As the SSQ is typically administered at one point in time, sufficient data on individual questions were included in five of the nine studies reviewed, and the studies showed post-operative improvements and high satisfaction (Figure 3) [13,20,23,24,53].
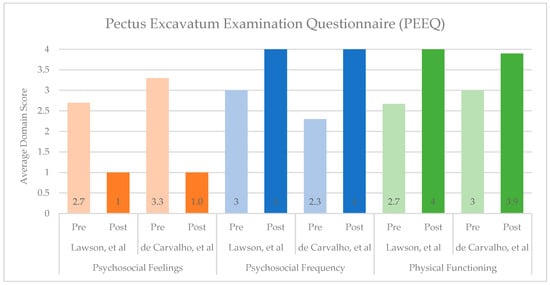
Figure 1.
Summary of Pectus Excavatum Examination Questionnaire (PEEQ) scores before and after surgical correction of Pectus Excavatum or Pectus Carinatum [11,46]. Psychosocial Feelings include questions 1–3, answered on a 4-point Likert scale, where 1 = very happy and 4 = very unhappy (lower scores indicate more desirable experiences). Psychosocial Frequency includes questions 4–9, and Physical Functioning includes questions 10–12; both sets are answered on a 4-point Likert scale, where 1 = very often and 4 = never (higher scores indicate more desirable experiences).

Figure 2.
Summary of Nuss Assessment Questionnaire Modified for Adults (NQ-mA) scores before and after surgical correction of Pectus Excavatum or Pectus Carinatum [13,23,50,51]. (A). Psychosocial and Physical Functioning Domains. Psychosocial Function includes questions 1–9, answered on a 4-point Likert scale, where 1 = very happy and 4 = very unhappy for questions 1–3 and 1 = very often and 4 = never for questions 4–9. Physical Functioning includes questions 10–12 answered on a 4-point Likert scale, where 1 = very often and 4 = never. Higher scores indicate more desirable experiences. (B). Total Scores. Summation of scores across the psychosocial and physical domains. Answers can range from 12 to 48. Higher scores indicate more desirable experiences.

Figure 3.
Single Step Questionnaire (SSQ) scores after surgical correction of Pectus Excavatum or Pectus Carinatum [13,20,23,24,53]. The survey is administered after treatment. However, two questions ask patients to recall their pre-operative self-assessment for comparison. Questions are scored on a 5-point Likert scale for chest appearance interfering with activity, general health, exercise capacity, chest improvement, and satisfaction. Self-esteem and the decision to have the operation again are scored on a scale of up to 10 points. Higher scores indicate more desirable experiences.
Body Image & Self-Esteem:
Across multiple studies, surgical correction of PE and PC provides marked improvements in body image and self-confidence [11,12,13,14,15,16,17]. Post-operatively, questionnaire scores show that between 97 and 99% of patients with PE, depending on the study, were improved and happy with their chest appearance [19,20,24,46]. Furthermore, 90–100% felt comfortable having their shirt off and were satisfied with spending the rest of their life with their updated chest appearance based upon PEEQ and NQ-mA assessments [15,46]. PC patients show similar benefits, with one cohort demonstrating that their satisfaction with their appearance without a shirt on improved from 29% to 85% following the modified Ravitch procedure, and acceptance of their chest appearance for the rest of their life improved from 4% to 93% [23]. Semi-structured interview studies reinforce these findings, with adolescents and young adults reporting increased confidence in social settings, improvements in self-acceptance, and decreased worries about the perceptions of others [12,14,22].
Interestingly, one study found that following the Nuss procedure, PE patients had scored higher in nine CHQ scales compared to healthy control peers, indicating better HRQoL [14]. One possible explanation is that due to their significantly impacted self-esteem and preoccupation with their chest appearance at baseline, surgical correction of PE may lead to a more robust sense of confidence. This theory is supported by the findings of other studies, where the attribution of QoL to their chest wall, the ownership to seek care to improve their appearance, and post-operative feelings of normalcy allow those with chest wall deformities to feel an inflated sense of self-confidence [10]. As a result, patients with both PE and PC engage less in concealment behaviors, feel less bothered by their chest appearance, and become more willing to engage in social interactions after surgical correction [6,10,23].
The timing of these improvements has been cited to be most significant from the pre-operative state to the six-week timepoint after surgery, with score stabilization at six months and beyond [53,59].
Social Functioning:
Improvements in body image and self-esteem following surgical correction translate into improvements in social belonging and empowerment. Consistently, studies have found increased participation in sports and peer activities, decreased concealment behaviors, and improved comfort taking off their shirt in the locker room, all of which were previously avoided due to chest exposure [6,10,14,20,21,24]. These findings have been affirmed by systematic reviews [17,25,26]. In semi-structured interviews following the Nuss procedure, adolescents reported that the cessation of concealment behaviors led to feelings of relief, as they felt comfortable being open with peers about their PE and surgery [10]. PC patients show similar post-operative improvements, with NQ-mA scores demonstrating less reluctance to wear clothes that expose the chest in public, as well as decreased teasing and feelings of isolation [50].
Mental Health:
While the mental health disturbances seen in adolescents and young adults with PE and PC may not consistently meet formal diagnostic thresholds, significant post-operative improvements have been observed on a variety of questionnaires. Generic HRQoL questionnaires, such as the CHQ, have shown improved scores on the mental health scale [16] while significant reductions in the domains of depression and interpersonal sensitivity have been seen on the SCL-90 following PE repair [22,44]. Furthermore, both depressive symptoms and overall mental health problems in those with PE decreased from 57% to 29% and from 61% to 30%, respectively, from before to after surgery [44]. These improvements were independent of the Haller Index, reinforcing that psychosocial benefit is not severity dependent. Similar improvements have been observed for those with PC on both generic and condition-specific QoL assessments regarding feelings of sadness, depression, and general mental health [23,50].
QoL & Satisfaction:
Overall QoL improvement and satisfaction with surgical intervention have been strongly observed following correction of both PE and PC deformities [12,18,19,20,21,22,23,24]. Satisfaction is independent of the procedure performed (Nuss vs. Ravitch), and for patients with PE who underwent the Nuss procedure, high satisfaction has been reported at both six months post-operatively and after bar removal [19,20]. Across several studies, 85–96% of patients with PE reported that they would choose to have the operation performed again [19,20,24]. This overall high level of satisfaction has been confirmed on all five systematic reviews conducted on chest wall deformities and QoL [17,25,26,27,28].
Long-term studies have demonstrated that patients with PE maintain high satisfaction and long-lasting positive effects on their psychological state years following bar removal [20,22,47]. A minority experience persistent distress or require surgical revision, often related to asymmetry or recurrence.
6.1.3. Parental Viewpoints
The distress felt by many adolescents does not go unnoticed by their parents, with a majority of studies identifying strong patient–parental score concordance [11,12,14,15,19,51,60]. Mirrored distress in parents is common, with 79% of parents expressing frequent concern about their child’s deformity pre-operatively, which drops to 16% post-operatively [19]. Parents also confirm marked improvements in their child’s psychosocial functioning, social self-consciousness, and overall confidence following surgical correction of both PE and PC [11,15,19,50,51]. Reduced concerns about the effects of PE on their child’s life, enhanced family dynamics, and fewer conflicts around concealment behaviors are common themes [11,14]. There appears to be no difference in parental perceptions based on surgical technique [19].
6.1.4. Impact of Pain
Post-operative pain is common following both open and minimally invasive repair of chest wall deformities, peaking in the first four to six weeks and impairing initial return to normal activities, and then improving significantly by six months [12,20,24,53]. Long-term pain following bar removal is rare [20,24]. Some adolescents have expressed that the surgical pain is preferable to the ongoing emotional distress of living with the deformity, with one interviewee stating that “any amount of pain would probably be better than the emotional pain” [10,12]. Predictors of persistent pain include pain-specific psychological variables (pain anxiety, hypervigilance), highlighting the need for targeted interventions [61]. Overall, patients and families have reported that the risks and pain associated with surgery are well worth the benefits [12].
Advances in multimodal analgesia have dramatically improved early recovery following chest wall deformity repair. Early post-operative strategies included regional anesthesia with thoracic epidurals, opioids, and non-steroidal anti-inflammatory medications. More recently, intercostal nerve cryoablation has been introduced as an ideal solution to mitigate post-operative pain. Cryoablation has been shown to provide considerable improvements in post-operative opioid consumption and length-of-stay after the Nuss procedure [62,63]. While many patients with severe and symptomatic PE previously chose surgical intervention despite the expected post-operative course, the successful introduction of cryoablation may further encourage patients to consider surgical intervention when they otherwise would not have, given the dramatically improved post-operative recovery enabled by the use of cryoablation.
Finally, another approach being explored is providing patients and their parents with pre-operative psychological coping strategies for pain and surgical-related worries, which was found to be beneficial in a recent study [64].
6.2. Non-Surgical Management
Non-operative management of PC through orthotic bracing has shown similar psychosocial improvements to surgical intervention. Successful bracing is dependent on patient motivation and adherence, with high attrition rates observed when expectations are not met [48,49]. Adolescents who complete bracing report significant improvements in body image, self-esteem, mental health, social participation, and physical functioning on both generic HRQoL tools and condition-specific questionnaires such as the modified PEEQ and PeCBI-QOL [48,49,54,56]. These improvements were most significant in the first six months after starting bracing and demonstrated stability in the two years following [56]. Individuals who failed bracing or were non-compliant with bracing had minimal psychosocial and overall QoL benefit, resulting in continued distress and dissatisfaction [48,56]. However, both studies comparing successful and unsuccessful bracing found that participants were interested in trying bracing again if it meant that their outcome could be improved. Family involvement enhances adherence and satisfaction. Similar to surgical correction, there is considerable parent–child concordance in QoL improvements, and supportive families facilitate coping with the demands of prolonged bracing [48].
There are limited data available regarding the psychological changes following non-operative management of PE with the vacuum bell technique, making it challenging to draw any definitive conclusions regarding its impacts [21].
Intervention of any variety may not be mandatory for all patients, with recent consensus guidelines suggesting that many deformities are well-tolerated and that supportive care is sufficient [32]. Limited data are available on the long-term psychological outcomes of those who elect conservative management, as psychological burden is a common reason for presenting to surgical evaluation and differs from those who choose non-operative management [18]. No studies have determined a level of psychological harm that indicates an operation would or would not be beneficial.
7. Health Policy and Insurance Considerations
7.1. Haller Index and Functional Criteria
In the United States, insurance coverage for surgical correction of chest wall deformities is largely restricted to anatomic and physiologic criteria. For PE, most payers require a Haller Index ≥ 3.25 and objective evidence of cardiopulmonary compromise, such as abnormal pulmonary function tests (PFTs), echocardiography, evidence of cardiac compression, or exercise intolerance [65,66,67,68]. Coverage for PC is typically more restrictive, as bracing and surgical repair are often categorized as “cosmetic” in the absence of demonstrable cardiac or pulmonary compromise expected to improve post-repair [65,66,67,68]. These criteria may exclude patients whose primary concern is psychosocial functioning, despite evidence that such factors can meaningfully affect quality of life.
International practices vary, with several centers reporting performing corrective surgery for appearance-related indications alone, with favorable satisfaction and mental health outcomes [6,15,23,24,40,50]. Other regions have adopted more restrictive criteria. In the United Kingdom (UK), the National Health Service (NHS) decommissioned routine surgical correction of chest wall deformities in 2019 [69]. Eligibility in England is closely aligned with anatomic and physiologic thresholds, and a multi-disciplinary review makes the final determination. No coverage is provided for bracing or surgical correction for PC. Scotland permits broader access, with patients under the age of 16 able to access a multi-disciplinary team that promotes a non-operative approach first. Following the decommissioning of surgical correction, joint specialist societies issued best-practice guidelines recommending that psychological impact, such as low self-esteem, depression, and social withdrawal, be evaluated when determining eligibility for intervention [32,51].
The distinction between “cosmetic” and reconstructive surgery is important, and mislabeling corrective surgery as cosmetic can be misleading and potentially harmful. While cosmetic is traditionally defined as modification of normal anatomy for aesthetic preference, chest wall deformity repair addresses a congenital structural abnormality and aims to restore normal thoracic contour and function [70]. Reliance on the Haller Index as a sole metric can be problematic, as studies show inconsistent associations between HI and psychosocial distress or surgical complexity. Patients with indices < 3.25 have reported substantial QoL impairment with post-operative benefit, and surgeons internationally do not agree that HI should be an indication for repair [6,7,8,9,15,17,30]. Alternative metrics, such as the correction index (CI), which accounts for the depth of the deformity as a proportion in terms of the most prominent portion of the chest wall, have been proposed to offer better discrimination of severity [71]. Furthermore, several studies indicate that psychosocial impairment often exceeds physical limitations among individuals seeking repair [23,51].
7.2. Surgeon Advocacy for Broader Coverage
Surgeons and professional societies increasingly call for policy reform to address coverage gaps in psychosocial indications for repair. A recent international survey found that 84% of chest wall surgeons agree that body image disturbances should be an indication for corrective surgery, even in the absence of physiologic compromise [30]. There is limited consensus regarding routine imaging as part of the pre-operative evaluation. Aside from clinical photography, no specific test, including CT, MRI, echocardiography, ECG, or PFTs, reached broad agreement, with many surgeons reserving relevant cardiopulmonary studies for symptomatic patients. One center has opted against pre-operative CT due to the hazards of radiation exposure in young patients, given that Haller Index measurements do not reliably predict outcomes [24]. Surgeons appear to agree that functional indices should be used as an adjunctive measure, rather than as the sole measure to assess severity for repair [15,27,72]. Patients and surgeons have also advocated for increasing multidisciplinary support through the inclusion of psychologists in chest wall deformity clinics to routinely support the psychological needs of these patients [21,22].
The age at which repair should occur remains an important aspect that has not been fully elucidated. Early intervention may prevent years of emotional suffering and social isolation that have accumulated during adolescence [41,44]; however, current surgical timing considerations often focus on anatomic and technical aspects of the operation, and it is unknown if this aligns with optimal timing for psychological benefits. Survey data suggest that the youngest age for pectus repair should be 12 years old, though earlier intervention may be considered on a case-by-case basis [30].
8. Limitations and Future Directions
While narrative methods enable an integrative approach to summarize the literature, the conclusions of this review may be limited by the absence of systematic approaches that quantify the quality and rigor of the analyzed data. However, all five systematic reviews identified on the topic were included and had concordant findings. Additionally, the literature on this topic frequently utilizes small sample sizes and heterogeneous outcome measures through predominantly observational designs, and there is a paucity of longitudinal data. This limitation is even more apparent for PC, where all but one study included <50 patients. While parallel psychosocial impacts have been observed between PE and PC, the underrepresentation of data on PC may not be representative of the true burden. Studies infrequently capture the formal diagnosis of mental health disorders and instead focus on symptom burden, limiting the conclusions that can be drawn regarding the impact on mental health.
Research has consistently demonstrated the psychological and QoL improvements following chest wall correction, yet insurance criteria have limited the number of individuals eligible for repair. Ongoing research should include individuals who do not meet the Haller Index threshold of ≥3.25 to better establish mental health criteria for repair. This research can support advocacy for expanding insurance coverage criteria to include psychosocial impairments and aligning reimbursement with evidence-based, patient-centered care. While many studies recognize that earlier correction can improve psychosocial outcomes, future research can better elucidate the optimal age for repair. In clinics, surgeons can implement standardized psychosocial screening with age-appropriate and deformity-specific assessment tools to understand their patients’ psychological risk. The integration of psychologists within multidisciplinary chest wall clinics can further support those at risk and provide pre-operative counseling, coping strategies, and post-operative support.
9. Conclusions
Chest wall deformities impose a significant psychosocial burden on adolescents and young adults, often disproportionate to their physiologic impairments. Perceived chest appearance, rather than anatomic severity, is the strongest predictor of psychological risk. While patients’ anxiety and depression do not always meet formal diagnostic thresholds, they have substantial impacts on daily functioning and QoL. Treatment of PE and PC through surgical and non-surgical approaches has positive effects on body image, self-confidence, and overall QoL and has led surgeons to advocate for these domains to be considered core measures in chest wall evaluations. Early psychosocial evaluation and psychological support are important components of a holistic care model aimed at mitigating long-term emotional distress and optimizing patient outcomes.
Author Contributions
Conceptualization, E.A.B. and K.J.V.A.; literature review, E.A.B. and B.B.M.; writing—original draft preparation, E.A.B.; writing—review and editing, E.A.B., B.B.M., S.A.M. and K.J.V.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
We would like to thank the Nationwide Children’s Reference Librarians for assistance with the literature search.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PE | Pectus Excavatum |
| PC | Pectus Carinatum |
| QoL | Quality of Life |
| HRQoL | Health-Related Quality of Life |
| HI | Haller Index |
References
- Obermeyer, R.J.; Goretsky, M.J. Chest wall deformities in pediatric surgery. Surg. Clin. N. Am. 2012, 92, 669–684. [Google Scholar] [CrossRef]
- Notrica, D.M.; McMahon, L.E.; Jaroszewski, D.E. Pectus Disorders: Excavatum, Carinatum and Arcuatum. Adv. Pediatr. 2024, 71, 181–194. [Google Scholar] [CrossRef]
- David, V.L. Current Concepts in the Etiology and Pathogenesis of Pectus Excavatum in Humans—A Systematic Review. J. Clin. Med. 2022, 11, 1241. [Google Scholar] [CrossRef] [PubMed]
- Colombani, P.M. Preoperative assessment of chest wall deformities. Semin. Thorac. Cardiovasc. Surg. 2009, 21, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.; Coorens, N.A.; Franssen, A.; Daemen, J.H.T.; Michels, I.L.; Hulsewé, K.W.E.; Vissers, Y.L.J.; de Loos, E.R. Pectus excavatum and carinatum: A narrative review of epidemiology, etiopathogenesis, clinical features, and classification. J. Thorac. Dis. 2024, 16, 1687–1701. [Google Scholar] [CrossRef]
- Morshuis, W.J.; Mulder, H.; Wapperom, G.; Folgering, H.T.; Assman, M.; Cox, A.L.; van Lier, H.J.; Vincent, J.G.; Lacquet, L.K. Pectus excavatum. A clinical study with long-term postoperative follow-up. Eur. J. Cardiothorac. Surg. 1992, 6, 318–328; discussion 319–328. [Google Scholar] [CrossRef]
- Sutyak, K.M.; Hebballi, N.B.; Bidart, Y.; Joly, J.M.; Broussard, M.; Christensen, H.; Mendenhall, J.; Jayarajan, N.; Anderson, I.; Young, Y.; et al. Is it time to expand the surgical criteria? The psychosocial impact of pectus excavatum in pediatrics. Surgery 2025, 185, 109546. [Google Scholar] [CrossRef]
- Alaca, N.; Yüksel, M. Comparison of physical functions and psychosocial conditions between adolescents with pectus excavatum, pectus carinatum and healthy controls. Pediatr. Surg. Int. 2021, 37, 765–775. [Google Scholar] [CrossRef]
- Ji, Y.; Liu, W.; Chen, S.; Xu, B.; Tang, Y.; Wang, X.; Yang, G.; Cao, L. Assessment of psychosocial functioning and its risk factors in children with pectus excavatum. Health Qual. Life Outcomes 2011, 9, 28. [Google Scholar] [CrossRef]
- Roberts, J.; Macmath, S.; English, M.; Martin, J.; Hayashi, A.; Sigalet, D.L. Body Disfigurement and the Quality of Life of Adolescents with Pectus Excavatum: Effects of the Nuss Procedure. Phys. Disabil. Educ. Relat. Serv. 2006, 25, 21–46. [Google Scholar]
- Lawson, M.L.; Cash, T.F.; Akers, R.; Vasser, E.; Burke, B.; Tabangin, M.; Welch, C.; Croitoru, D.P.; Goretsky, M.J.; Nuss, D.; et al. A pilot study of the impact of surgical repair on disease-specific quality of life among patients with pectus excavatum. J. Pediatr. Surg. 2003, 38, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.; Hayashi, A.; Anderson, J.O.; Martin, J.M.; Maxwell, L.L. Quality of life of patients who have undergone the Nuss procedure for pectus excavatum: Preliminary findings. J. Pediatr. Surg. 2003, 38, 779–783. [Google Scholar] [CrossRef]
- Krasopoulos, G.; Dusmet, M.; Ladas, G.; Goldstraw, P. Nuss procedure improves the quality of life in young male adults with pectus excavatum deformity. Eur. J. Cardio-Thorac. Surg. 2006, 29, 1–5. [Google Scholar] [CrossRef]
- Jacobsen, E.B.; Thastum, M.; Jeppesen, J.H.; Pilegaard, H.K. Health-related quality of life in children and adolescents undergoing surgery for pectus excavatum. Eur. J. Pediatr. Surg. 2010, 20, 85–91. [Google Scholar] [CrossRef]
- Gibreel, W.; Zendejas, B.; Joyce, D.; Moir, C.R.; Zarroug, A.E. Minimally Invasive Repairs of Pectus Excavatum: Surgical Outcomes, Quality of Life, and Predictors of Reoperation. J. Am. Coll. Surg. 2016, 222, 245–252. [Google Scholar] [CrossRef]
- Lomholt, J.J.; Jacobsen, E.B.; Thastum, M.; Pilegaard, H. A prospective study on quality of life in youths after pectus excavatum correction. Ann. Cardiothorac. Surg. 2016, 5, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, J.S.; Tan, J.W.; Tam, J.K.C. Quality of life with minimally invasive repair of pectus excavatum: A systematic review and meta-analysis. Ann. Transl. Med. 2023, 11, 407. [Google Scholar] [CrossRef]
- Bahadir, A.T.; Kuru Bektaşoğlu, P.; Çakiroğlu Eser, A.; Afacan, C.; Yüksel, M. Psychosocial functioning in pediatric patients with pectus excavatum and pectus carinatum. Turk. J. Med. Sci. 2017, 47, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.E., Jr.; Cash, T.F.; Shamberger, R.C.; Mitchell, K.K.; Mellins, R.B.; Lawson, M.L.; Oldham, K.; Azizkhan, R.G.; Hebra, A.V.; Nuss, D.; et al. Surgical repair of pectus excavatum markedly improves body image and perceived ability for physical activity: Multicenter study. Pediatrics 2008, 122, 1218–1222. [Google Scholar] [CrossRef]
- Metzelder, M.L.; Kuebler, J.F.; Leonhardt, J.; Ure, B.M.; Petersen, C. Self and parental assessment after minimally invasive repair of pectus excavatum: Lasting satisfaction after bar removal. Ann. Thorac. Surg. 2007, 83, 1844–1849. [Google Scholar] [CrossRef]
- Habelt, S.; Korn, S.; Berger, A.; Bielek, J. Psychological distress in patients with pectus excavatum as an indication for therapy. Int. J. Clin. Med. 2011, 2, 295–300. [Google Scholar] [CrossRef]
- Hadolt, B.; Wallisch, A.; Egger, J.W.; Höllwarth, M.E. Body-image, self-concept and mental exposure in patients with pectus excavatum. Pediatr. Surg. Int. 2011, 27, 665–670. [Google Scholar] [CrossRef]
- Knudsen, M.V.; Grosen, K.; Pilegaard, H.K.; Laustsen, S. Surgical correction of pectus carinatum improves perceived body image, mental health and self-esteem. J. Pediatr. Surg. 2015, 50, 1472–1476. [Google Scholar] [CrossRef] [PubMed]
- Hanna, W.C.; Ko, M.A.; Blitz, M.; Shargall, Y.; Compeau, C.G. Thoracoscopic Nuss procedure for young adults with pectus excavatum: Excellent midterm results and patient satisfaction. Ann. Thorac. Surg. 2013, 96, 1033–1036; discussion 1037–1038. [Google Scholar] [CrossRef]
- Johnstone, A.D.; Davis, C.; Roberts, N.J.; Sharp, K. Quality of life of children and young people with anterior chest wall deformity: A systematic review of the literature. Arch. Dis. Child. 2023, 108, 678–683. [Google Scholar] [CrossRef]
- Fortmann, C.; Petersen, C. Surgery for Deformities of the Thoracic Wall: No More than Strengthening the Patient’s Self-Esteem? Eur. J. Pediatr. Surg. 2018, 28, 355–360. [Google Scholar] [CrossRef]
- Walsh, J.; Walsh, R.; Redmond, K. Systematic review of physiological and psychological outcomes of surgery for pectus excavatum supporting commissioning of service in the UK. BMJ Open Respir. Res. 2023, 10, e001665. [Google Scholar] [CrossRef]
- Alqadi, G.O.; Saxena, A.K. Analysis of Psychological Assessments Affecting Patients Undergoing Treatment for Chest Wall Deformities. Am. Surg. 2023, 89, 1923–1929. [Google Scholar] [CrossRef] [PubMed]
- Biavati, M.; Kozlitina, J.; Alder, A.C.; Foglia, R.; McColl, R.W.; Peshock, R.M.; Kelly, R.E., Jr.; Kim Garcia, C. Prevalence of pectus excavatum in an adult population-based cohort estimated from radiographic indices of chest wall shape. PLoS ONE 2020, 15, e0232575. [Google Scholar] [CrossRef]
- Janssen, N.; Daemen, J.H.T.; van Polen, E.J.; Coorens, N.A.; Jansen, Y.J.L.; Franssen, A.; Hulsewé, K.W.E.; Vissers, Y.L.J.; Haecker, F.M.; Milanez de Campos, J.R.; et al. Pectus Excavatum: Consensus and Controversies in Clinical Practice. Ann. Thorac. Surg. 2023, 116, 191–199. [Google Scholar] [CrossRef]
- Bardají, C.; Cassou, L. Taulinoplasty: The traction technique-a new extrathoracic repair for pectus excavatum. Ann. Cardiothorac. Surg. 2016, 5, 519–522. [Google Scholar] [CrossRef]
- Dunning, J.; Burdett, C.; Child, A.; Davies, C.; Eastwood, D.; Goodacre, T.; Haecker, F.M.; Kendall, S.; Kolvekar, S.; MacMahon, L.; et al. The pectus care guidelines: Best practice consensus guidelines from the joint specialist societies SCTS/MF/CWIG/BOA/BAPS for the treatment of patients with pectus abnormalities. Eur. J. Cardiothorac. Surg. 2024, 66, ezae166. [Google Scholar] [CrossRef]
- Blanco, F.C.; Elliott, S.T.; Sandler, A.D. Management of congenital chest wall deformities. Semin. Plast. Surg. 2011, 25, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Robicsek, F.; Watts, L.T. Pectus carinatum. Thorac. Surg. Clin. 2010, 20, 563–574. [Google Scholar] [CrossRef]
- Abramson, H.; D’Agostino, J.; Wuscovi, S. A 5-year experience with a minimally invasive technique for pectus carinatum repair. J. Pediatr. Surg. 2009, 44, 118–123; discussion 114–123. [Google Scholar] [CrossRef]
- Buziashvili, D.; Gopman, J.M.; Weissler, H.; Bodenstein, L.; Kaufman, A.J.; Taub, P.J. An Evidence-Based Approach to Management of Pectus Excavatum and Carinatum. Ann. Plast. Surg. 2019, 82, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Vannucci, A.; Ohannessian, C.M. Body Image Dissatisfaction and Anxiety Trajectories During Adolescence. J. Clin. Child. Adolesc. Psychol. 2018, 47, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, H.; Patalay, P.; Choo, T.H.; Wall, M.; Mason, S.M.; Goldschmidt, A.B.; Neumark-Sztainer, D. Bidirectional associations between body dissatisfaction and depressive symptoms from adolescence through early adulthood. Dev. Psychopathol. 2018, 30, 1447–1458. [Google Scholar] [CrossRef]
- Elkind, D. Egocentrism in adolescence. Child. Dev. 1967, 38, 1025–1034. [Google Scholar] [CrossRef]
- Steinmann, C.; Krille, S.; Mueller, A.; Weber, P.; Reingruber, B.; Martin, A. Pectus excavatum and pectus carinatum patients suffer from lower quality of life and impaired body image: A control group comparison of psychological characteristics prior to surgical correction. Eur. J. Cardiothorac. Surg. 2011, 40, 1138–1145. [Google Scholar] [CrossRef]
- Norlander, L.; Anderzén-Carlsson, A.; Vidlund, M.; Sundqvist, A.S. Experiences of living with funnel chest prior to corrective surgery: An interview study. PLoS ONE 2024, 19, e0304968. [Google Scholar] [CrossRef]
- Matsuda, K.; Fujisawa, D.; Masai, K.; Miyazaki, N.; Suzuki, S.; Okubo, Y.; Kaseda, K.; Asakura, K.; Hishida, T.; Asamura, H. Quality of life, psychological states, and personality traits in patients with pectus excavatum. JTCVS Open 2024, 19, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Krille, S.; Müller, A.; Steinmann, C.; Reingruber, B.; Weber, P.; Martin, A. Self- and social perception of physical appearance in chest wall deformity. Body Image 2012, 9, 246–252. [Google Scholar] [CrossRef]
- Luo, L.; Xu, B.; Wang, X.; Tan, B.; Zhao, J. Intervention of the Nuss Procedure on the Mental Health of Pectus Excavatum Patients. Ann. Thorac. Cardiovasc. Surg. 2017, 23, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.W.; Klassen, A.F.; Montgomery, C.J.; LeBlanc, J.G.; Skarsgard, E.D. Quality-of-life outcomes after surgical correction of pectus excavatum: A comparison of the Ravitch and Nuss procedures. J. Pediatr. Surg. 2008, 43, 819–825. [Google Scholar] [CrossRef] [PubMed]
- de Carvalho, R.L.C.; Tedde, M.L.; de Campos, J.R.M.; Hamilton, N.N.; Guilherme, G.F.; Sousa, V.M.; Junior, V.F.S.; Savazzi, F.H.; Pego-Fernandes, P.M. Quality of life outcomes after minimally invasive repair of pectus excavatum utilizing a new set of metallic bars and stabilizers. J. Pediatr. Surg. 2021, 56, 545–549. [Google Scholar] [CrossRef]
- Kelly, R.E., Jr.; Daniel, A. Outcomes, quality of life, and long-term results after pectus repair from around the globe. Semin. Pediatr. Surg. 2018, 27, 170–174. [Google Scholar] [CrossRef]
- Colozza, S.; Bütter, A. Bracing in pediatric patients with pectus carinatum is effective and improves quality of life. J. Pediatr. Surg. 2013, 48, 1055–1059. [Google Scholar] [CrossRef]
- Orrick, B.A.; Pierce, A.L.; McElroy, S.F. Changes in self-image after pectus carinatum brace treatment. J. Pediatr. Surg. 2022, 57, 1579–1583. [Google Scholar] [CrossRef]
- Bostanci, K.; Ozalper, M.H.; Eldem, B.; Ozyurtkan, M.O.; Issaka, A.; Ermerak, N.O.; Yuksel, M. Quality of life of patients who have undergone the minimally invasive repair of pectus carinatum. Eur. J. Cardiothorac. Surg. 2013, 43, 122–126. [Google Scholar] [CrossRef]
- Kuru, P.; Bostanci, K.; Ermerak, N.O.; Bahadir, A.T.; Afacan, C.; Yuksel, M. Quality of life improves after minimally invasive repair of pectus excavatum. Asian Cardiovasc. Thorac. Ann. 2015, 23, 302–307. [Google Scholar] [CrossRef]
- Norlander, L.; Sundqvist, A.S.; Anderzén-Carlsson, A.; Dreifaldt, M.; Andreasson, J.; Vidlund, M. Health-related quality of life after Nuss procedure for pectus excavatum: A cross-sectional study. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac031. [Google Scholar] [CrossRef]
- Zuidema, W.P.; van der Steeg, A.F.W.; van der Heide, S.; Zijp, G.W.; van Baren, R.; Oosterhuis, J.W.A.; van Heurn, E. The Outcome of the Single Step Questionnaire in Pectus Excavatum Patients is Phase Dependent. Eur. J. Pediatr. Surg. 2020, 30, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Paulson, J.F.; Ellis, K.; Obermeyer, R.J.; Kuhn, M.A.; Frantz, F.W.; McGuire, M.M.; Ortiz, E.; Kelly, R.E., Jr. Development and validation of the Pectus Carinatum Body Image Quality of Life (PeCBI-QOL) questionnaire. J. Pediatr. Surg. 2019, 54, 2257–2260. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef]
- van Braak, H.; de Beer, S.A.; Twisk, J.W.R.; Zwaveling, S.; Oomen, M.W.N.; de Jong, J.R.; Ernest van Heurn, L.W. Improving Quality of Life With Dynamic Compression Bracing in Patients With Pectus Carinatum. J. Pediatr. Surg. 2025, 60, 161975. [Google Scholar] [CrossRef]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- IQVIA. Child Health Questionnaire (CHQ). Available online: https://www.qualitymetric.com/health-surveys/child-health-questionnaire-chq/ (accessed on 30 November 2025).
- Zuidema, W.P.; Oosterhuis, J.W.A.; Zijp, G.W.; van der Heide, S.M.; van der Steeg, A.F.W.; van Heurn, L.W.E. Early Consequences of Pectus Excavatum Surgery on Self-Esteem and General Quality of Life. World J. Surg. 2018, 42, 2502–2506. [Google Scholar] [CrossRef] [PubMed]
- Kroczek, K.K.; Sebastian, J.; Szymkuć-Bukowska, I.; Pyskir, M.; Gałązka, P. Quality of life assessment after minimally invasive operative treatment in children with pectus excavatum: A single-center study and literature review. Adv. Clin. Exp. Med. 2025, 34, 1485–1492. [Google Scholar] [CrossRef]
- Horn-Hofmann, C.; Scheel, J.; Dimova, V.; Parthum, A.; Carbon, R.; Griessinger, N.; Sittl, R.; Lautenbacher, S. Prediction of persistent post-operative pain: Pain-specific psychological variables compared with acute post-operative pain and general psychological variables. Eur. J. Pain. 2018, 22, 191–202. [Google Scholar] [CrossRef]
- Arshad, S.A.; Garcia, E.I.; Bell, C.; Avritscher, E.B.C.; Kumar, M.; Brahmamdam, P.; Fraser, J.A.; St Peter, S.D.; Aranda, A.; Hill, M.; et al. Multicenter Assessment of Cryoanalgesia Use in Minimally Invasive Repair of Pectus Excavatum: A 20-center Retrospective Cohort Study. Ann. Surg. 2023, 277, e1373–e1379. [Google Scholar] [CrossRef] [PubMed]
- Lotakis, D.; Vernamonti, J.P.; Wright, T.N.; Van Arendonk, K.J.; Minneci, P.C.; Leys, C.M.; Landman, M.P.; St Peter, S.D.; Brown, R.L.; Mak, G.Z.; et al. Regional Anesthesia and Surgical Volume in Children Undergoing Nuss Repair: A Multicenter Review. J. Surg. Res. 2025, 305, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Brimeyer, C.; Czarnecki, M.L.; LiaBraaten, B.; Flynn, E.; Weisman, S.J.; Densmore, J.D.; Hainsworth, K.R. A Preoperative Psychosocial Intervention for Youth Undergoing Pectus Repair: Development and Initial Patient/Caregiver Experiences. Clin. Pract. Pediatr. Psychol. 2024, 12, 291–302. [Google Scholar] [CrossRef]
- Aetna. Pectus Excavatum and Poland’s Syndrome: Surgical Correction. Available online: https://www.aetna.com/cpb/medical/data/200_299/0272.html (accessed on 30 November 2025).
- Healthcare, C. Surgical Treatment of Chest Wall Deformities. Available online: https://static.cigna.com/assets/chcp/pdf/coveragePolicies/medical/mm_0309_coveragepositioncriteria_surgical_treatment_chest_wall_deformities.pdf (accessed on 30 November 2025).
- Healthcare, U. Pectus Deformity Repair. Available online: https://www.aapc.com/codes/webroot/upload/general_pages_docs/document/Pectus_Deformity_Repair_CD.pdf?msockid=0506c244a948661c1adad484a88d6700 (accessed on 30 November 2025).
- Permanente, K. Pectus Excavatum, Pectus Carinatum and Poland’s Syndrome: Surgical Correction Medical Coverage Policy. Available online: https://healthy.kaiserpermanente.org/content/dam/kporg/final/documents/health-plan-documents/notice/utilization-management/pectus-excavatum-sx-mas-en.pdf (accessed on 30 November 2025).
- Matters, P. Accessing Treatment in the UK. Available online: https://www.pectusmatters.co.uk/accessing-treatment-in-the-uk (accessed on 12 December 2025).
- Chrysopoulo, M. What’s the Difference Between Reconstructive and Cosmetic Procedures? Available online: https://www.plasticsurgery.org/news/blog/whats-the-difference-between-reconstructive-and-cosmetic-procedures (accessed on 5 December 2025).
- St Peter, S.D.; Juang, D.; Garey, C.L.; Laituri, C.A.; Ostlie, D.J.; Sharp, R.J.; Snyder, C.L. A novel measure for pectus excavatum: The correction index. J. Pediatr. Surg. 2011, 46, 2270–2273. [Google Scholar] [CrossRef]
- Ciriaco, P. Surgical Treatment of Pectus Excavatum: The Boundary Between Pathologic and Aesthetic Need. J. Clin. Med. 2025, 14, 231. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.