



Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study



Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Analysis
3. Results
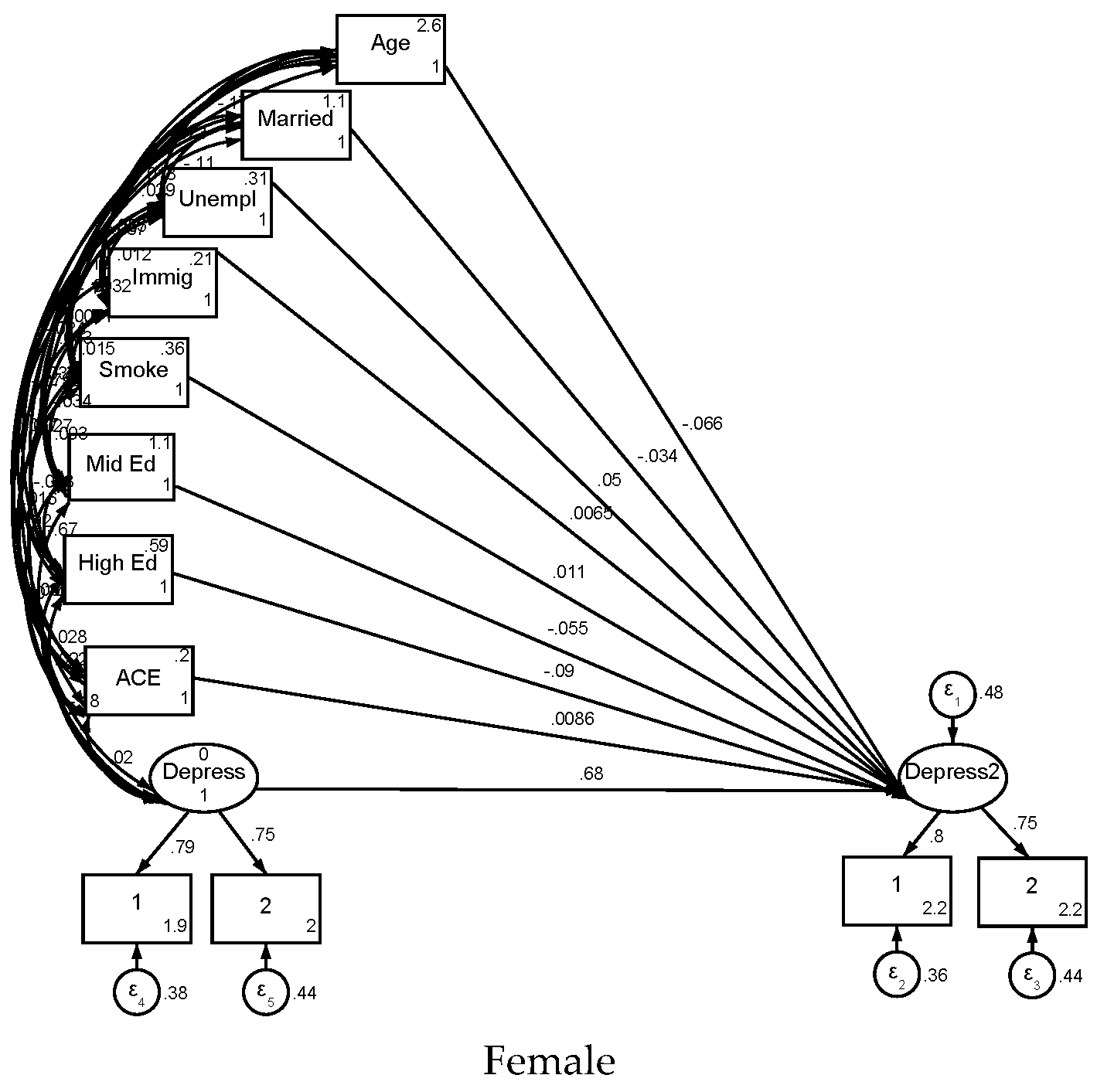
4. Structural Equation Modeling (SEM) in Females
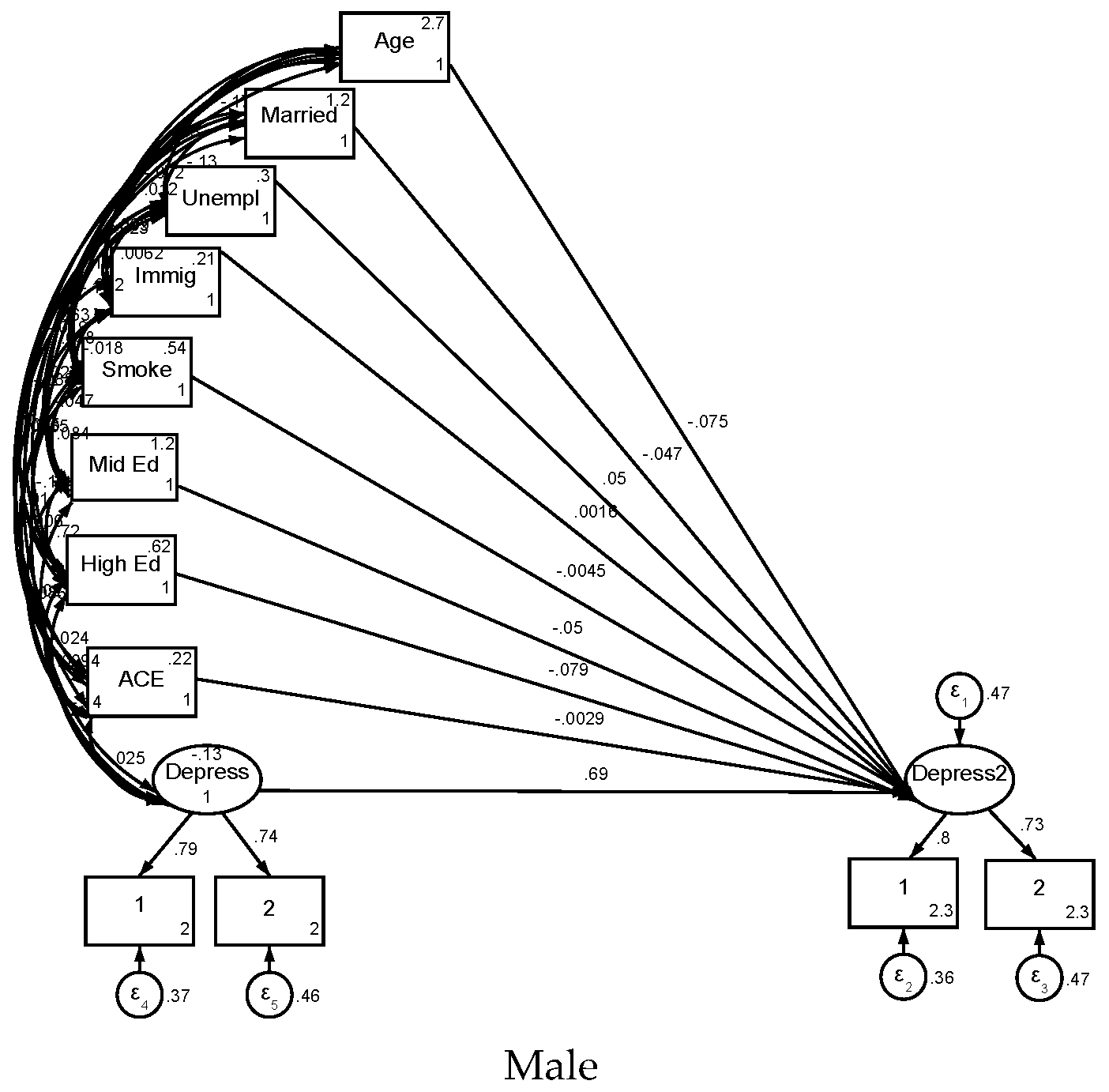
5. Structural Equation Modeling (SEM) in Males
6. Discussion
7. Policy and Practice Implications
8. Strengths and Limitations
9. Future Research Directions
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Pavlidi, P.; Kokras, N.; Dalla, C. Sex Differences in Depression and Anxiety. Curr. Top. Behav. Neurosci. 2023, 62, 103–132. [Google Scholar] [CrossRef]
- Felitti, V.J. The Relation Between Adverse Childhood Experiences and Adult Health: Turning Gold into Lead. Perm. J. 2002, 6, 44–47. [Google Scholar] [CrossRef]
- Chapman, D.P.; Whitfield, C.L.; Felitti, V.J.; Dube, S.R.; Edwards, V.J.; Anda, R.F. Adverse childhood experiences and the risk of depressive disorders in adulthood. J. Affect. Disord. 2004, 82, 217–225. [Google Scholar] [CrossRef]
- Sheffler, J.L.; Piazza, J.R.; Quinn, J.M.; Sachs-Ericsson, N.J.; Stanley, I.H. Adverse childhood experiences and coping strategies: Identifying pathways to resiliency in adulthood. Anxiety Stress Coping 2019, 32, 594–609. [Google Scholar] [CrossRef]
- Iob, E.; Lacey, R.; Giunchiglia, V.; Steptoe, A. Adverse childhood experiences and severity levels of inflammation and depression from childhood to young adulthood: A longitudinal cohort study. Mol. Psychiatry 2022, 27, 2255–2263. [Google Scholar] [CrossRef]
- McEwen, B.S.; Milner, T.A. Hippocampal formation: Shedding light on the influence of sex and stress on the brain. Brain Res. Rev. 2007, 55, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Sapienza, P.; Zingales, L.; Maestripieri, D. Gender differences in financial risk aversion and career choices are affected by testosterone. Proc. Natl. Acad. Sci. USA 2009, 106, 15268–15273. [Google Scholar] [CrossRef]
- Verma, R.; Balhara, Y.P.; Gupta, C.S. Gender differences in stress response: Role of developmental and biological determinants. Ind. Psychiatry J. 2011, 20, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Gan, A.K.X.; Gibb, B.E. Stress sensitivity in women with a history of recurrent versus first-episode major depression. Psychiatry Res. 2025, 345, 116382. [Google Scholar] [CrossRef] [PubMed]
- Eid, R.S.; Gobinath, A.R.; Galea, L.A.M. Sex differences in depression: Insights from clinical and preclinical studies. Prog. Neurobiol. 2019, 176, 86–102. [Google Scholar] [CrossRef] [PubMed]
- O’Shields, J.D.; Graves, B.D.; Mowbray, O.P. Sex differences in childhood maltreatment, inflammation, and adulthood depression: A network analysis. Brain Behav. Immun. Health 2023, 29, 100611. [Google Scholar] [CrossRef]
- Gronewold, J.; Duman, E.E.; Engel, M.; Engels, M.; Siegrist, J.; Erbel, R.; Jöckel, K.H.; Hermann, D.M. Association between life events and later depression in the population-based Heinz Nixdorf Recall study-The role of sex and optimism. PLoS ONE 2022, 17, e0271716. [Google Scholar] [CrossRef] [PubMed]
- An, X.; Guo, W.; Wu, H.; Fu, X.; Li, M.; Zhang, Y.; Li, Y.; Cui, R.; Yang, W.; Zhang, Z.; et al. Sex Differences in Depression Caused by Early Life Stress and Related Mechanisms. Front. Neurosci. 2022, 16, 797755. [Google Scholar] [CrossRef]
- Jarkas, D.A.; Villeneuve, A.H.; Daneshmend, A.Z.B.; Villeneuve, P.J.; McQuaid, R.J. Sex differences in the inflammation-depression link: A systematic review and meta-analysis. Brain Behav. Immun. 2024, 121, 257–268. [Google Scholar] [CrossRef]
- Wang, R.; Kogler, L.; Derntl, B. Sex differences in cortisol levels in depression: A systematic review and meta-analysis. Front. Neuroendocr. 2024, 72, 101118. [Google Scholar] [CrossRef]
- O’Shields, J.D.; Slavich, G.M.; Mowbray, O. Adverse childhood experiences, inflammation, and depression: Evidence of sex- and stressor specific effects in a nationally representative longitudinal sample of U.S. adolescents. Psychol. Med. 2025, 55, e140. [Google Scholar] [CrossRef]
- Donovan, A.; Assari, S.; Shaheen, M.; Grella, C.; Richter, L.; Friedman, T.C. 8256 Early Life Stress and Pubertal Predictors of Youth Substance Use Initiation: Does Sex Moderate the Relationship Between ELS, Puberty, and Substance Use Initiation? J. Endocr. Soc. 2024, 8, bvae163.1194. [Google Scholar] [CrossRef]
- Assari, S.; Sheikhattari, P. Sex Differences in the Relationship Between Nucleus Accumbens Volume and Youth Tobacco or Marijuana Use Following Stressful Life Events. J. Ment. Health Clin. Psychol. 2024, 8, 1–13. [Google Scholar] [CrossRef]
- Campioni, M.R.; Xu, M.; McGehee, D.S. Stress-induced changes in nucleus accumbens glutamate synaptic plasticity. J. Neurophysiol. 2009, 101, 3192–3198. [Google Scholar] [CrossRef]
- Magalhães, E.; Ferreira, C.; Antunes, C.; Jongenelen, I.; Castro, E. Stressful Events During Last Year, Violence and Anxiety and Depression: A Moderated Mediation Model by Sex. Violence Vict. 2022, 37, 610–624. [Google Scholar] [CrossRef] [PubMed]
- Donovan, A.; Assari, S.; Grella, C.; Shaheen, M.; Richter, L.; Friedman, T.C. Early life stress and pubertal predictors of subsequent substance use in a national diverse sample of adolescents: Sex and substance type matter. Drug Alcohol. Depend. 2025, 268, 112551. [Google Scholar] [CrossRef] [PubMed]
- Donovan, A.; Assari, S.; Grella, C.; Shaheen, M.; Richter, L.; Friedman, T.C. Neuroendocrine mechanisms in the links between early life stress, affect, and youth substance use: A conceptual model for the study of sex and gender differences. Front. Neuroendocrinol. 2024, 73, 101121. [Google Scholar] [CrossRef]
- Manoli, D.S.; Tollkuhn, J. Gene regulatory mechanisms underlying sex differences in brain development and psychiatric disease. Ann. N. Y. Acad. Sci. 2018, 1420, 26–45. [Google Scholar] [CrossRef] [PubMed]
- López-Cerdán, A.; Andreu, Z.; Hidalgo, M.R.; Soler-Sáez, I.; de la Iglesia-Vayá, M.; Mikozami, A.; Guerini, F.R.; García-García, F. An integrated approach to identifying sex-specific genes, transcription factors, and pathways relevant to Alzheimer’s disease. Neurobiol. Dis. 2024, 199, 106605. [Google Scholar] [CrossRef]
- Baker, T.; Mundell, N.; Koorts, H.; Pebole, M.; Rosenbaum, S.; Ganakas, E.; Teychenne, M. Targeting mental health and wellbeing in women who have experienced gender-based violence through moderate-vigorous physical activity: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2025, 22, 49. [Google Scholar] [CrossRef]
- Levin, J.; Bradshaw, M.; Johnson, B.R. Association between Jewish religious observance and mental health among Israeli adults: Findings from the Global Flourishing Study. Int. J. Psychiatry Med. 2025, 60, 338–355. [Google Scholar] [CrossRef] [PubMed]
- Lomas, T.; Bradshaw, M.; Case, B.; Cowden, R.G.; Crabtree, S.; English, C.; Fogleman, A.; Johnson, K.A.; Ritter, Z.; Johnson, B.R. The development of the Global Flourishing Study questionnaire: Charting the evolution of a new 109-Item inventory of human flourishing. BMC Glob. Public. Health 2025, 3, 30. [Google Scholar] [CrossRef]
- Johnson, B.R.; VanderWeele, T.J. The global flourishing study: A new era for the study of well-being. Int. Bull. Mission Res. 2022, 46, 272–275. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Johnson, B.R.; Bialowolski, P.T.; Bonhag, R.; Bradshaw, M.; Breedlove, T.; Case, B.; Chen, Y.; Chen, Z.J.; Counted, V. The Global Flourishing Study: Study profile and initial results on flourishing. Nat. Ment. Health 2025, 1–18. [Google Scholar] [CrossRef]
- Levin, J.; Bradshaw, M.; Johnson, B.R. Religious Differences in Physical and Mental Health among Israeli Jews: Findings from the Global Flourishing Study. J. Relig. Health 2024, 63, 2544–2558. [Google Scholar] [CrossRef] [PubMed]
- Padgett, R.N.; Cowden, R.G.; Chattopadhyay, M.; Han, Y.; Honohan, J.; Ritter, Z.; Srinivasan, R.; Johnson, B.R.; VanderWeele, T.J. Survey sampling design in wave 1 of the Global Flourishing Study. Eur. J. Epidemiol. 2025, 40, 391–406. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Ullman, J.B.; Bentler, P.M. Structural equation modeling. In Handbook of Psychology, 2nd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; Volume 2. [Google Scholar]
- Hair Jr, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.; Danks, N.P.; Ray, S.; Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. An introduction to structural equation modeling. In Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1–29. [Google Scholar]
- Mueller, R.O.; Hancock, G.R. Structural equation modeling. In The reviewer’s Guide to Quantitative Methods in the Social Sciences; Routledge: Oxford, UK, 2018; pp. 445–456. [Google Scholar]
- Bowen, N.K.; Guo, S. Structural Equation Modeling; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Velayutham, S.; Aldridge, J.M.; Fraser, B. Gender differences in student motivation and self-regulation in science learning: A multi-group structural equation modeling analysis. Int. J. Sci. Math. Educ. 2012, 10, 1347–1368. [Google Scholar] [CrossRef]
- Tu, Y.K.; Baelum, V.; Gilthorpe, M.S. A structural equation modelling approach to the analysis of change. Eur. J. Oral. Sci. 2008, 116, 291–296. [Google Scholar] [CrossRef]
- Lee, M.-A.; Song, R. Childhood abuse, personality traits, and depressive symptoms in adulthood. Child Abus. Negl. 2017, 65, 194–203. [Google Scholar] [CrossRef]
- Shapero, B.G.; Black, S.K.; Liu, R.T.; Klugman, J.; Bender, R.E.; Abramson, L.Y.; Alloy, L.B. Stressful life events and depression symptoms: The effect of childhood emotional abuse on stress reactivity. J. Clin. Psychol. 2014, 70, 209–223. [Google Scholar] [CrossRef]
- Van Dam, D.; van Nierop, M.; Viechtbauer, W.; Velthorst, E.; van Winkel, R.; Bruggeman, R.; Cahn, W.; De Haan, L.; Kahn, R.; Meijer, C. Childhood abuse and neglect in relation to the presence and persistence of psychotic and depressive symptomatology. Psychol. Med. 2015, 45, 1363–1377. [Google Scholar] [CrossRef]
- He, C.; Fan, D.; Liu, X.; Wang, Q.; Zhang, H.; Zhang, H.; Zhang, Z.; Xie, C. Insula network connectivity mediates the association between childhood maltreatment and depressive symptoms in major depressive disorder patients. Transl. Psychiatry 2022, 12, 89. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.; Linn, K.A.; Shinohara, R.T.; Oathes, D.J.; Cook, P.A.; Duprat, R.; Moore, T.M.; Oquendo, M.A.; Phillips, M.L.; McInnis, M. Childhood trauma history is linked to abnormal brain connectivity in major depression. Proc. Natl. Acad. Sci. USA 2019, 116, 8582–8590. [Google Scholar] [CrossRef]
- Wang, Q.; Qi, L.; He, C.; Fan, D.; Zhang, H.; Zhang, H.; Cheng, W.; Xie, C. Occipital connectivity networks mediate the neural effects of childhood maltreatment on depressive symptoms in major depressive disorder. Asian J. Psychiatry 2024, 97, 104093. [Google Scholar] [CrossRef]
- Lin, J.; Huang, J.; Wu, Y.; Zhou, L.; Qiao, C.; Xie, J.; Hu, C. Exploring the neural link between childhood maltreatment and depression: A default mode network rs-fMRI study. Front. Psychiatry 2024, 15, 1450051. [Google Scholar] [CrossRef] [PubMed]
- Weder, N.; Zhang, H.; Jensen, K.; Yang, B.Z.; Simen, A.; Jackowski, A.; Lipschitz, D.; Douglas-Palumberi, H.; Ge, M.; Perepletchikova, F. Child abuse, depression, and methylation in genes involved with stress, neural plasticity, and brain circuitry. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 417–424.e415. [Google Scholar] [CrossRef]
- Wu, Z.; Luo, Q.; Wu, H.; Wu, Z.; Zheng, Y.; Yang, Y.; He, J.; Ding, Y.; Yu, R.; Peng, H. Amplitude of low-frequency oscillations in major depressive disorder with childhood trauma. Front. Psychiatry 2021, 11, 596337. [Google Scholar] [CrossRef] [PubMed]
- Heck, A.L.; Handa, R.J. Sex differences in the hypothalamic–pituitary–adrenal axis’ response to stress: An important role for gonadal hormones. Neuropsychopharmacology 2019, 44, 45–58. [Google Scholar] [CrossRef]
- Oyola, M.G.; Handa, R.J. Hypothalamic–pituitary–adrenal and hypothalamic–pituitary–gonadal axes: Sex differences in regulation of stress responsivity. Stress 2017, 20, 476–494. [Google Scholar] [CrossRef]
- Obeidallah, D.A.; McHale, S.M.; Silbereisen, R.K. Gender role socialization and adolescents’ reports of depression: Why some girls and not others? J. Youth Adolesc. 1996, 25, 775–785. [Google Scholar] [CrossRef]
- Dedovic, K.; Wadiwalla, M.; Engert, V.; Pruessner, J.C. The role of sex and gender socialization in stress reactivity. Dev. Psychol. 2009, 45, 45. [Google Scholar] [CrossRef]
- Christiansen, D.M.; McCarthy, M.M.; Seeman, M.V. Where sex meets gender: How sex and gender come together to cause sex differences in mental illness. Front. Psychiatry 2022, 13, 856436. [Google Scholar] [CrossRef] [PubMed]
- Rincón-Cortés, M.; Herman, J.P.; Lupien, S.; Maguire, J.; Shansky, R.M. Stress: Influence of sex, reproductive status and gender. Neurobiol. Stress. 2019, 10, 100155. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.; Mendenhall, S.; Myers, C.A. The effects of sex and gender role identity on perceived stress and coping among traditional and nontraditional students. J. Am. Coll. Health 2016, 64, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Young, E.; Korszun, A. Sex, trauma, stress hormones and depression. Mol. Psychiatry 2010, 15, 23–28. [Google Scholar] [CrossRef]
- Mengelkoch, S.; Slavich, G.M. Sex differences in stress susceptibility as a key mechanism underlying depression risk. Curr. Psychiatry Rep. 2024, 26, 157–165. [Google Scholar] [CrossRef]
- Guo, L.; Chen, Y.-X.; Hu, Y.-T.; Wu, X.-Y.; He, Y.; Wu, J.-L.; Huang, M.-L.; Mason, M.; Bao, A.-M. Sex hormones affect acute and chronic stress responses in sexually dimorphic patterns: Consequences for depression models. Psychoneuroendocrinology 2018, 95, 34–42. [Google Scholar] [CrossRef]
- Marrocco, J.; McEwen, B.S. Sex in the brain: Hormones and sex differences. Dialogues Clin. Neurosci. 2016, 18, 373–383. [Google Scholar] [CrossRef]
- McEwen, B.S.; Milner, T.A. Understanding the broad influence of sex hormones and sex differences in the brain. J. Neurosci. Res. 2017, 95, 24–39. [Google Scholar] [CrossRef]
- Sinclair, D.; Purves-Tyson, T.D.; Allen, K.M.; Weickert, C.S. Impacts of stress and sex hormones on dopamine neurotransmission in the adolescent brain. Psychopharmacology 2014, 231, 1581–1599. [Google Scholar] [CrossRef]
- Liddon, L.; Kingerlee, R.; Barry, J.A. Gender differences in preferences for psychological treatment, coping strategies, and triggers to help-seeking. Br. J. Clin. Psychol. 2018, 57, 42–58. [Google Scholar] [CrossRef]
- Gibbons, S.W.; Barnett, S.D.; Hickling, E.J.; Herbig-Wall, P.L.; Watts, D.D. Stress, coping, and mental health-seeking behaviors: Gender differences in OEF/OIF health care providers. J. Trauma. Stress 2012, 25, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Bennett, K.M. “No sissy stuff”: Towards a theory of masculinity and emotional expression in older widowed men. J. Aging Stud. 2007, 21, 347–356. [Google Scholar] [CrossRef]
- Jakupcak, M.; Tull, M.T.; Roemer, L. Masculinity, Shame, and Fear of Emotions as Predictors of Men’s Expressions of Anger and Hostility. Psychol. Men Masculinity 2005, 6, 275. [Google Scholar] [CrossRef]
- De Boise, S.; Hearn, J. Are men getting more emotional? Critical sociological perspectives on men, masculinities and emotions. Sociol. Rev. 2017, 65, 779–796. [Google Scholar] [CrossRef]
- Lee, C. Social context, depression and the transition to motherhood. Br. J. Health Psychol. 1997, 2, 93–108. [Google Scholar] [CrossRef]
- Schwartz, S. Women and depression: A Durkheimian perspective. Soc. Sci. Med. 1991, 32, 127–140. [Google Scholar] [CrossRef]
- Shors, T.J.; Millon, E.M.; Chang, H.Y.M.; Olson, R.L.; Alderman, B.L. Do sex differences in rumination explain sex differences in depression? J. Neurosci. Res. 2017, 95, 711–718. [Google Scholar] [CrossRef]
- Papadakis, A.A.; Prince, R.P.; Jones, N.P.; Strauman, T.J. Self-regulation, rumination, and vulnerability to depression in adolescent girls. Dev. Psychopathol. 2006, 18, 815–829. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Country | n | % | SE | 95% | CI |
|---|---|---|---|---|---|
| Argentina | 2884 | 2.31 | 0.04 | 2.23 | 2.39 |
| Australia | 2557 | 2.05 | 0.04 | 1.97 | 2.13 |
| Brazil | 4196 | 3.36 | 0.05 | 3.26 | 3.46 |
| Egypt | 3028 | 2.42 | 0.04 | 2.34 | 2.51 |
| Germany | 5476 | 4.38 | 0.06 | 4.27 | 4.50 |
| India | 6023 | 4.82 | 0.06 | 4.70 | 4.94 |
| Indonesia | 2664 | 2.13 | 0.04 | 2.05 | 2.21 |
| Japan | 13,841 | 11.07 | 0.09 | 10.90 | 11.25 |
| Kenya | 7660 | 6.13 | 0.07 | 6.00 | 6.26 |
| Mexico | 2229 | 1.78 | 0.04 | 1.71 | 1.86 |
| Nigeria | 3116 | 2.49 | 0.04 | 2.41 | 2.58 |
| Philippines | 2677 | 2.14 | 0.04 | 2.06 | 2.22 |
| Poland | 6419 | 5.14 | 0.06 | 5.01 | 5.26 |
| South Africa | 967 | 0.77 | 0.02 | 0.73 | 0.82 |
| Spain | 2880 | 2.30 | 0.04 | 2.22 | 2.39 |
| Tanzania | 5551 | 4.44 | 0.06 | 4.33 | 4.56 |
| Türkiye | 495 | 0.40 | 0.02 | 0.36 | 0.43 |
| United Kingdom | 3568 | 2.85 | 0.05 | 2.76 | 2.95 |
| United States | 31,970 | 25.58 | 0.12 | 25.34 | 25.82 |
| Sweden | 11,539 | 9.23 | 0.08 | 9.07 | 9.39 |
| Hong Kong | 704 | 0.56 | 0.02 | 0.52 | 0.61 |
| China | 4538 | 3.63 | 0.05 | 3.53 | 3.74 |
| Mean | Std. err. | [95% conf. | Interval] | |
|---|---|---|---|---|
| Age (Years) | 49.04 | 0.05 | 48.94 | 49.13 |
| Depressed Baseline | 1.73 | 0.00 | 1.73 | 1.74 |
| Depressed Follow Up | 1.75 | 0.00 | 1.74 | 1.75 |
| Anhedonia Baseline | 1.84 | 0.00 | 1.84 | 1.85 |
| Anhedonia Follow Up | 1.86 | 0.00 | 1.86 | 1.87 |
| Gender/Sex | ||||
| Female | 51.09 | 0.14 | 50.82 | 51.37 |
| Male | 48.91 | 0.14 | 48.63 | 49.18 |
| ACE | ||||
| No | 85.89 | 0.10 | 85.69 | 86.08 |
| Yes | 14.11 | 0.10 | 13.92 | 14.31 |
| Education | ||||
| Low | 14.40 | 0.10 | 14.20 | 14.59 |
| Mid | 54.93 | 0.14 | 54.65 | 55.21 |
| High | 30.67 | 0.13 | 30.42 | 30.93 |
| Married | ||||
| No | 42.17 | 0.14 | 41.89 | 42.44 |
| Yes | 57.83 | 0.14 | 57.56 | 58.11 |
| Unemployed | ||||
| No | 92.98 | 0.07 | 92.83 | 93.12 |
| Yes | 7.02 | 0.07 | 6.88 | 7.17 |
| B | SE | 95% | CI | p | ||
|---|---|---|---|---|---|---|
| Structural | ||||||
| Depression (Follow Up) | ||||||
| Mid Education (Baseline) | −0.055 | 0.005 | −0.066 | −0.045 | <0.001 | |
| High Education (Baseline) | −0.090 | 0.005 | −0.100 | −0.079 | <0.001 | |
| Smoker (Baseline) | 0.011 | 0.004 | 0.002 | 0.019 | 0.011 | |
| Immigrant (Baseline) | 0.006 | 0.004 | −0.001 | 0.014 | 0.098 | |
| Age (Yr) (Baseline) | −0.066 | 0.004 | −0.073 | −0.059 | <0.001 | |
| Unemployed (Baseline) | 0.050 | 0.004 | 0.042 | 0.059 | <0.001 | |
| Married (Baseline) | −0.034 | 0.004 | −0.042 | −0.027 | <0.001 | |
| ACE | 0.009 | 0.004 | 0.000 | 0.017 | 0.044 | |
| Depression (Baseline) | 0.677 | 0.004 | 0.669 | 0.684 | <0.001 | |
| Measurement | ||||||
| Depressed (Follow Up) | ||||||
| Depression (Follow Up) | 0.800 | 0.003 | 0.795 | 0.805 | <0.001 | |
| Intercept | 2.209 | 0.011 | 2.188 | 2.230 | <0.001 | |
| Anhedonia (Follow Up) | ||||||
| Depression (Follow Up) | 0.749 | 0.002 | 0.744 | 0.754 | <0.001 | |
| Intercept | 2.237 | 0.010 | 2.217 | 2.258 | <0.001 | |
| Depressed (Baseline) | ||||||
| Depression (Baseline) | 0.788 | 0.002 | 0.784 | 0.793 | <0.001 | |
| Intercept | 1.905 | 0.005 | 1.895 | 1.914 | <0.001 | |
| Anhedonia (Baseline) | ||||||
| Depression (Baseline) | 0.750 | 0.002 | 0.746 | 0.754 | <0.001 | |
| Intercept | 1.952 | 0.005 | 1.942 | 1.962 | <0.001 | |
| B | SE | 95% | CI | p | ||
|---|---|---|---|---|---|---|
| Structural | ||||||
| Depression (Follow Up) | ||||||
| Mid Education (Baseline) | −0.050 | 0.006 | −0.061 | −0.039 | <0.001 | |
| High Education (Baseline) | −0.079 | 0.006 | −0.090 | −0.068 | <0.001 | |
| Smoker (Baseline) | −0.005 | 0.004 | −0.013 | 0.004 | 0.279 | |
| Immigrant (Baseline) | 0.002 | 0.004 | −0.006 | 0.009 | 0.685 | |
| Age (Yr) (Baseline) | −0.075 | 0.004 | −0.082 | −0.067 | <0.001 | |
| Unemployed (Baseline) | 0.050 | 0.004 | 0.042 | 0.059 | <0.001 | |
| Married (Baseline) | −0.047 | 0.004 | −0.055 | −0.039 | <0.001 | |
| ACE | −0.003 | 0.004 | −0.012 | 0.006 | 0.524 | |
| Depression (Baseline) | 0.688 | 0.004 | 0.680 | 0.696 | <0.001 | |
| Measurement | ||||||
| Depressed (Follow Up) | ||||||
| Depression (Follow Up) | 0.801 | 0.003 | 0.796 | 0.806 | <0.001 | |
| Intercept | 2.295 | 0.011 | 2.274 | 2.317 | <0.001 | |
| Anhedonia (Follow Up) | ||||||
| Depression (Follow Up) | 0.730 | 0.003 | 0.725 | 0.735 | <0.001 | |
| Intercept | 2.263 | 0.010 | 2.242 | 2.283 | <0.001 | |
| Depressed (Baseline) | ||||||
| Depression (Baseline) | 0.794 | 0.002 | 0.789 | 0.799 | <0.001 | |
| Intercept | 1.976 | 0.005 | 1.965 | 1.986 | <0.001 | |
| Anhedonia (Baseline) | ||||||
| Depression (Baseline) | 0.735 | 0.002 | 0.731 | 0.740 | <0.001 | |
| Intercept | 1.971 | 0.005 | 1.961 | 1.981 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assari, S.; Najand, B.; Donovan, A. Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study. Children 2025, 12, 754. https://doi.org/10.3390/children12060754
Assari S, Najand B, Donovan A. Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study. Children. 2025; 12(6):754. https://doi.org/10.3390/children12060754
Chicago/Turabian StyleAssari, Shervin, Babak Najand, and Alexandra Donovan. 2025. "Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study" Children 12, no. 6: 754. https://doi.org/10.3390/children12060754
APA StyleAssari, S., Najand, B., & Donovan, A. (2025). Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study. Children, 12(6), 754. https://doi.org/10.3390/children12060754