

Pediatric Inflammatory Bowel Disease in Romania: The First Epidemiological Study of the North-West Region (2000–2020)

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
2.3. Methods
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramos, G.P.; Papadakis, K.A. Mechanisms of Disease: Inflammatory Bowel Diseases. Mayo Clin. Proc. 2019, 94, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; de Carpi, J.M.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of Paediatric Ulcerative Colitis, Part 1: Ambulatory Care-An Evidence-based Guideline From European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 257–291. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ruemmele, F.M.; Orlanski-Meyer, E.; Griffiths, A.M.; de Carpi, J.M.; Bronsky, J.; Veres, G.; Aloi, M.; Strisciuglio, C.; Braegger, C.P.; et al. Management of Paediatric Ulcerative Colitis, Part 2: Acute Severe Colitis-An Evidence-based Consensus Guideline From the European Crohn’s and Colitis Organization and the European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 292–310. [Google Scholar] [CrossRef]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef]
- Spinelli, A.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Surgical Treatment. J. Crohns Colitis 2022, 16, 179–189. [Google Scholar] [CrossRef]
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J. Crohns Colitis 2022, 16, 2–17. [Google Scholar] [CrossRef]
- Gordon, H.; Minozzi, S.; Kopylov, U.; Verstockt, B.; Chaparro, M.; Buskens, C.; Warusavitarne, J.; Agrawal, M.; Allocca, M.; Atreya, R.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohns Colitis 2024, 18, 1531–1555. [Google Scholar] [CrossRef]
- Adamina, M.; Minozzi, S.; Warusavitarne, J.; Buskens, C.J.; Chaparro, M.; Verstockt, B.; Kopylov, U.; Yanai, H.; Vavricka, S.R.; Sigall-Boneh, R.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. J. Crohns Colitis 2024, 18, 1556–1582. [Google Scholar] [CrossRef]
- Melton, S.L.; Day, A.S.; Bryant, R.V.; Halmos, E.P. Revolution in diet therapy for inflammatory bowel disease. JGH Open 2024, 8, e13097. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Windsor, J.W. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Alvisi, P.; Labriola, F.; Scarallo, L.; Gandullia, P.; Knafelz, D.; Bramuzzo, M.; Zuin, G.; Pastore, M.R.; Illiceto, M.T.; Miele, E.; et al. Epidemiological trends of pediatric IBD in Italy: A 10-year analysis of the Italian society of pediatric gastroenterology, hepatology and nutrition registry. Dig. Liver Dis. 2022, 54, 469–476. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Fortinsky, K.J.; Gozdyra, P.; Van den Heuvel, M.; Van Limbergen, J.; Griffiths, A.M. Epidemiology of pediatric inflammatory bowel disease: A systematic review of international trends. Inflamm. Bowel Dis. 2011, 17, 423–439. [Google Scholar] [CrossRef] [PubMed]
- Van Limbergen, J.; Russell, R.K.; Drummond, H.E.; Aldhous, M.C.; Round, N.K.; Nimmo, E.R.; Smith, L.; Gillett, P.M.; McGrogan, P.; Weaver, L.T.; et al. Definition of phenotypic characteristics of childhood-onset inflammatory bowel disease. Gastroenterology 2008, 135, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Carroll, M.W.; Kuenzig, M.E.; Mack, D.R.; Otley, A.R.; Griffiths, A.M.; Kaplan, G.G.; Bernstein, C.N.; Bitton, A.; Murthy, S.K.; Nguyen, G.C.; et al. The Impact of Inflammatory Bowel Disease in Canada 2018: Children and Adolescents with IBD. J. Can. Assoc. Gastroenterol. 2019, 2, S49–S67. [Google Scholar] [CrossRef]
- Kelsen, J.; Baldassano, R.N. Inflammatory bowel disease: The difference between children and adults. Inflamm. Bowel Dis. 2008, 14 (Suppl. S2), S9–S11. [Google Scholar] [CrossRef]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Kuenzig, M.E.; Fung, S.G.; Marderfeld, L.; Mak, J.W.Y.; Kaplan, G.G.; Ng, S.C.; Wilson, D.C.; Cameron, F.; Henderson, P.; Kotze, P.G.; et al. Twenty-first Century Trends in the Global Epidemiology of Pediatric-Onset Inflammatory Bowel Disease: Systematic Review. Gastroenterology 2022, 162, 1147–1159.e1144. [Google Scholar] [CrossRef]
- Sykora, J.; Pomahacova, R.; Kreslova, M.; Cvalinova, D.; Stych, P.; Schwarz, J. Current global trends in the incidence of pediatric-onset inflammatory bowel disease. World J. Gastroenterol. 2018, 24, 2741–2763. [Google Scholar] [CrossRef]
- Roberts, S.E.; Thorne, K.; Thapar, N.; Broekaert, I.; Benninga, M.A.; Dolinsek, J.; Mas, E.; Miele, E.; Orel, R.; Pienar, C.; et al. A Systematic Review and Meta-analysis of Paediatric Inflammatory Bowel Disease Incidence and Prevalence Across Europe. J. Crohns Colitis 2020, 14, 1119–1148. [Google Scholar] [CrossRef]
- Levine, A.; Koletzko, S.; Turner, D.; Escher, J.C.; Cucchiara, S.; de Ridder, L.; Kolho, K.L.; Veres, G.; Russell, R.K.; Paerregaard, A.; et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 795–806. [Google Scholar] [CrossRef]
- TEMPO Online. Available online: http://statistici.insse.ro:8077/tempo-online/#/pages/tables/insse-table (accessed on 9 September 2021).
- Eurostat (European Comission) Publications Office. Available online: https://ec.europa.eu/eurostat/web/products-manuals-and-guidelines/-/KS-RA-13–028 (accessed on 7 October 2021).
- Shivashankar, R.; Tremaine, W.J.; Harmsen, W.S.; Loftus, E.V., Jr. Incidence and Prevalence of Crohn’s Disease and Ulcerative Colitis in Olmsted County, Minnesota From 1970 Through 2010. Clin. Gastroenterol. Hepatol. 2017, 15, 857–863. [Google Scholar] [CrossRef]
- Zagorowicz, E.; Walkiewicz, D.; Kucha, P.; Perwieniec, J.; Maluchnik, M.; Wieszczy, P.; Regula, J. Nationwide data on epidemiology of inflammatory bowel disease in Poland between 2009 and 2020. Pol. Arch. Intern. Med. 2022, 132, 16194. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.M.; Zoega, H.; Shah, S.A.; Bright, R.M.; Mallette, M.; Moniz, H.; Grabert, S.A.; Bancroft, B.; Merrick, M.; Flowers, N.T.; et al. Incidence of Crohn’s Disease and Ulcerative Colitis in Rhode Island: Report from the Ocean State Crohn’s and Colitis Area Registry. Inflamm. Bowel Dis. 2016, 22, 1456–1461. [Google Scholar] [CrossRef]
- Virta, L.J.; Saarinen, M.M.; Kolho, K.L. Inflammatory Bowel Disease Incidence is on the Continuous Rise Among All Paediatric Patients Except for the Very Young: A Nationwide Registry-based Study on 28-Year Follow-up. J. Crohns Colitis 2017, 11, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Malmborg, P.; Grahnquist, L.; Lindholm, J.; Montgomery, S.; Hildebrand, H. Increasing incidence of paediatric inflammatory bowel disease in northern Stockholm County, 2002–2007. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Lovasz, B.D.; Lakatos, L.; Horvath, A.; Pandur, T.; Erdelyi, Z.; Balogh, M.; Szipocs, I.; Vegh, Z.; Veres, G.; Muller, K.E.; et al. Incidence rates and disease course of paediatric inflammatory bowel diseases in Western Hungary between 1977 and 2011. Dig. Liver Dis. 2014, 46, 405–411. [Google Scholar] [CrossRef]
- Perminow, G.; Brackmann, S.; Lyckander, L.G.; Franke, A.; Borthne, A.; Rydning, A.; Aamodt, G.; Schreiber, S.; Vatn, M.H.; Group, I.-I. A characterization in childhood inflammatory bowel disease, a new population-based inception cohort from South-Eastern Norway, 2005–07, showing increased incidence in Crohn’s disease. Scand. J. Gastroenterol. 2009, 44, 446–456. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Bernstein, C.N.; Bitton, A.; Carroll, M.W.; Singh, H.; Otley, A.R.; Vutcovici, M.; El-Matary, W.; Nguyen, G.C.; Griffiths, A.M.; et al. Trends in Epidemiology of Pediatric Inflammatory Bowel Disease in Canada: Distributed Network Analysis of Multiple Population-Based Provincial Health Administrative Databases. Am. J. Gastroenterol. 2017, 112, 1120–1134. [Google Scholar] [CrossRef]
- Adamiak, T.; Walkiewicz-Jedrzejczak, D.; Fish, D.; Brown, C.; Tung, J.; Khan, K.; Faubion, W., Jr.; Park, R.; Heikenen, J.; Yaffee, M.; et al. Incidence, clinical characteristics, and natural history of pediatric IBD in Wisconsin: A population-based epidemiological study. Inflamm. Bowel Dis. 2013, 19, 1218–1223. [Google Scholar] [CrossRef]
- Burgess, C.; Henderson, P.; Chalmers, I.; Harris, R.; Hansen, R.; Russell, R.; Wilson, D. DOP84 Nationwide incidence and prevalence of paediatric inflammatory bowel disease in Scotland 2015–2017 demonstrates the highest paediatric prevalence rate recorded worldwide. J. Crohn’s Colitis 2019, 13, S081. [Google Scholar] [CrossRef]
- Wilson, J.; Hair, C.; Knight, R.; Catto-Smith, A.; Bell, S.; Kamm, M.; Desmond, P.; McNeil, J.; Connell, W. High incidence of inflammatory bowel disease in Australia: A prospective population-based Australian incidence study. Inflamm. Bowel Dis. 2010, 16, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Urlep, D.; Blagus, R.; Orel, R. Incidence Trends and Geographical Variability of Pediatric Inflammatory Bowel Disease in Slovenia: A Nationwide Study. Biomed. Res. Int. 2015, 2015, 921730. [Google Scholar] [CrossRef]
- Larsen, M.D.; Baldal, M.E.; Nielsen, R.G.; Nielsen, J.; Lund, K.; Norgard, B.M. The incidence of Crohn’s disease and ulcerative colitis since 1995 in Danish children and adolescents < 17 years—Based on nationwide registry data. Scand. J. Gastroenterol. 2016, 51, 1100–1105. [Google Scholar] [CrossRef]
- Kern, I.; Schoffer, O.; Kiess, W.; Henker, J.; Laass, M.W.; Winkler, U.; Quietzsch, J.; Wenzel, O.; Zurek, M.; Buttner, K.; et al. Incidence trends of pediatric onset inflammatory bowel disease in the years 2000–2009 in Saxony, Germany-first results of the Saxon Pediatric IBD Registry. PLoS ONE 2021, 16, e0243774. [Google Scholar] [CrossRef]
- Petritsch, W.; Fuchs, S.; Berghold, A.; Bachmaier, G.; Hogenauer, C.; Hauer, A.C.; Weiglhofer, U.; Wenzl, H.H. Incidence of inflammatory bowel disease in the province of Styria, Austria, from 1997 to 2007: A population-based study. J. Crohns Colitis 2013, 7, 58–69. [Google Scholar] [CrossRef]
- Ghione, S.; Sarter, H.; Fumery, M.; Armengol-Debeir, L.; Savoye, G.; Ley, D.; Spyckerelle, C.; Pariente, B.; Peyrin-Biroulet, L.; Turck, D.; et al. Dramatic Increase in Incidence of Ulcerative Colitis and Crohn’s Disease (1988–2011): A Population-Based Study of French Adolescents. Am. J. Gastroenterol. 2018, 113, 265–272. [Google Scholar] [CrossRef]
- Ashton, J.J.; Wiskin, A.E.; Ennis, S.; Batra, A.; Afzal, N.A.; Beattie, R.M. Rising incidence of paediatric inflammatory bowel disease (PIBD) in Wessex, Southern England. Arch. Dis. Child. 2014, 99, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Hope, B.; Shahdadpuri, R.; Dunne, C.; Broderick, A.M.; Grant, T.; Hamzawi, M.; O’Driscoll, K.; Quinn, S.; Hussey, S.; Bourke, B. Rapid rise in incidence of Irish paediatric inflammatory bowel disease. Arch. Dis. Child. 2012, 97, 590–594. [Google Scholar] [CrossRef]
- Burisch, J. Crohn’s disease and ulcerative colitis. Occurrence, course and prognosis during the first year of disease in a European population-based inception cohort. Dan. Med. J. 2014, 61, B4778. [Google Scholar]
- Martin-de-Carpi, J.; Rodriguez, A.; Ramos, E.; Jimenez, S.; Martinez-Gomez, M.J.; Medina, E.; SPIRIT-IBD Working Group of Sociedad Española de Gastroenterología, Hepatología y Nutricion Pediátrica. Increasing incidence of pediatric inflammatory bowel disease in Spain (1996–2009): The SPIRIT Registry. Inflamm. Bowel Dis. 2013, 19, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.J.; Cho, S.M.; Choe, B.H.; Jang, H.J.; Choi, K.H.; Kang, B.; Kim, J.E.; Hwang, J.H. Characteristics and Incidence Trends for Pediatric Inflammatory Bowel Disease in Daegu-Kyungpook Province in Korea: A Multi-Center Study. J. Korean Med. Sci. 2018, 33, e132. [Google Scholar] [CrossRef]
- Salkic, N.N.; Pavlovic-Calic, N.; Gegic, A.; Jovanovic, P.; Basic, M. Ulcerative colitis in the Tuzla region of Bosnia and Herzegovina between 1995 and 2006: Epidemiological and clinical characteristics. Eur. J. Gastroenterol. Hepatol. 2010, 22, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Pavlovic-Calic, N.; Salkic, N.N.; Gegic, A.; Smajic, M.; Alibegovic, E. Crohn’s disease in Tuzla region of Bosnia and Herzegovina: A 12-year study (1995–2006). Int. J. Colorectal Dis. 2008, 23, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Wittig, R.; Albers, L.; Koletzko, S.; Saam, J.; von Kries, R. Pediatric Chronic Inflammatory Bowel Disease in a German Statutory Health INSURANCE-Incidence Rates From 2009 to 2012. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 244–250. [Google Scholar] [CrossRef]
- Ivkovic, L.; Hojsak, I.; Trivic, I.; Sila, S.; Hrabac, P.; Konjik, V.; Senecic-Cala, I.; Palcevski, G.; Despot, R.; Zaja, O.; et al. Incidence and Geographical Variability of Pediatric Inflammatory Bowel Disease in Croatia: Data From the Croatian National Registry for Children With Inflammatory Bowel Disease. Clin. Pediatr. 2020, 59, 1182–1190. [Google Scholar] [CrossRef]
- Studd, C.; Cameron, G.; Beswick, L.; Knight, R.; Hair, C.; McNeil, J.; Desmond, P.; Wilson, J.; Connell, W.; Bell, S. Never underestimate inflammatory bowel disease: High prevalence rates and confirmation of high incidence rates in Australia. J. Gastroenterol. Hepatol. 2016, 31, 81–86. [Google Scholar] [CrossRef]
- Choe, J.Y.; Choi, S.; Song, K.H.; Jang, H.J.; Choi, K.H.; Yi, D.Y.; Hong, S.J.; Hwang, J.H.; Cho, S.M.; Kim, Y.J.; et al. Incidence and Prevalence Trends of Pediatric Inflammatory Bowel Disease in the Daegu-Kyungpook Province From 2017 to 2020. Front. Pediatr. 2021, 9, 810173. [Google Scholar] [CrossRef]
- Lopez, R.N.; Evans, H.M.; Appleton, L.; Bishop, J.; Chin, S.; Mouat, S.; Gearry, R.B.; Day, A.S. Prospective Incidence of Paediatric Inflammatory Bowel Disease in New Zealand in 2015: Results From the Paediatric Inflammatory Bowel Disease in New Zealand (PINZ) Study. J. Pediatr. Gastroenterol. Nutr. 2018, 66, e122–e126. [Google Scholar] [CrossRef]
- Krzesiek, E.; Kofla-Dlubacz, A.; Akutko, K.; Stawarski, A. The Incidence of Inflammatory Bowel Disease in the Paediatric Population in the District of Lower Silesia, Poland. J. Clin. Med. 2021, 10, 3994. [Google Scholar] [CrossRef]
- Tulumovic, E.; Salkic, N.; Tulumovic, D. Inflammatory bowel disease in Tuzla Canton, Bosnia-Herzegovina: A prospective 10-year follow-up. World J. Gastroenterol. 2021, 27, 2630–2642. [Google Scholar] [CrossRef] [PubMed]
- Vicentin, R.; Wagener, M.; Pais, A.B.; Contreras, M.; Orsi, M. One-year prospective registry of inflammatory bowel disease in the Argentine pediatric population. Arch. Argent. Pediatr. 2017, 115, 533–540. [Google Scholar] [CrossRef]
- EUROSTAT. Available online: https://ec.europa.eu/eurostat/web/nuts (accessed on 5 January 2025).
- Dalzell, A.M.; Ba’Ath, M.E. Paediatric inflammatory bowel disease: Review with a focus on practice in low- to middle-income countries. Paediatr. Int. Child. Health 2019, 39, 48–58. [Google Scholar] [CrossRef]
- Gheorghe, C.; Pascu, O.; Gheorghe, L.; Iacob, R.; Dumitru, E.; Tantau, M.; Vadan, R.; Goldis, A.; Balan, G.; Iacob, S.; et al. Epidemiology of inflammatory bowel disease in adults who refer to gastroenterology care in Romania: A multicentre study. Eur. J. Gastroenterol. Hepatol. 2004, 16, 1153–1159. [Google Scholar] [CrossRef]
- Muller, K.E.; Lakatos, P.L.; Arato, A.; Kovacs, J.B.; Varkonyi, A.; Szucs, D.; Szakos, E.; Solyom, E.; Kovacs, M.; Polgar, M.; et al. Incidence, Paris classification, and follow-up in a nationwide incident cohort of pediatric patients with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Lakatos, L.; Kiss, L.S.; David, G.; Pandur, T.; Erdelyi, Z.; Mester, G.; Balogh, M.; Szipocs, I.; Molnar, C.; Komaromi, E.; et al. Incidence, disease phenotype at diagnosis, and early disease course in inflammatory bowel diseases in Western Hungary, 2002–2006. Inflamm. Bowel Dis. 2011, 17, 2558–2565. [Google Scholar] [CrossRef]
- Sjoberg, D.; Holmstrom, T.; Larsson, M.; Nielsen, A.L.; Holmquist, L.; Ekbom, A.; Ronnblom, A. Incidence and clinical course of Crohn’s disease during the first year—Results from the IBD Cohort of the Uppsala Region (ICURE) of Sweden 2005–2009. J. Crohns Colitis 2014, 8, 215–222. [Google Scholar] [CrossRef]
- Sjoberg, D.; Holmstrom, T.; Larsson, M.; Nielsen, A.L.; Holmquist, L.; Ekbom, A.; Ronnblom, A. Incidence and natural history of ulcerative colitis in the Uppsala Region of Sweden 2005–2009—Results from the IBD cohort of the Uppsala Region (ICURE). J. Crohns Colitis 2013, 7, e351–e357. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.; Sykora, J.; Cvalinova, D.; Pomahacova, R.; Kleckova, J.; Kryl, M.; Vcelak, P. Inflammatory bowel disease incidence in Czech children: A regional prospective study, 2000–2015. World J. Gastroenterol. 2017, 23, 4090–4101. [Google Scholar] [CrossRef]
- Jabandziev, P.; Pinkasova, T.; Kunovsky, L.; Papez, J.; Jouza, M.; Karlinova, B.; Novackova, M.; Urik, M.; Aulicka, S.; Slaby, O.; et al. Regional Incidence of Inflammatory Bowel Disease in a Czech Pediatric Population: 16 Years of Experience (2002–2017). J. Pediatr. Gastroenterol. Nutr. 2020, 70, 586–592. [Google Scholar] [CrossRef]
- Nambu, R.; Warner, N.; Mulder, D.J.; Kotlarz, D.; McGovern, D.P.B.; Cho, J.; Klein, C.; Snapper, S.B.; Griffiths, A.M.; Iwama, I.; et al. A Systematic Review of Monogenic Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 20, e653–e663. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.M.; Manuc, T.; Chifulescu, A.; Istratescu, D.; Louis, E.; Baicus, C.; Sandra, I.; Diculescu, M.M.; Reenaers, C.; van Kemseke, C.; et al. Diet as an environmental trigger in inflammatory bowel disease: A retrospective comparative study in two European cohorts. Rev. Esp. Enferm. Dig. 2020, 112, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Marion-Letellier, R.; Amamou, A.; Savoye, G.; Ghosh, S. Inflammatory Bowel Diseases and Food Additives: To Add Fuel on the Flames! Nutrients 2019, 11, 1111. [Google Scholar] [CrossRef]
- Narula, N.; Wong, E.C.L.; Dehghan, M.; Mente, A.; Rangarajan, S.; Lanas, F.; Lopez-Jaramillo, P.; Rohatgi, P.; Lakshmi, P.V.M.; Varma, R.P.; et al. Association of ultra-processed food intake with risk of inflammatory bowel disease: Prospective cohort study. BMJ 2021, 374, n1554. [Google Scholar] [CrossRef]
- Raoul, P.; Cintoni, M.; Palombaro, M.; Basso, L.; Rinninella, E.; Gasbarrini, A.; Mele, M.C. Food Additives, a Key Environmental Factor in the Development of IBD through Gut Dysbiosis. Microorganisms 2022, 10, 167. [Google Scholar] [CrossRef]
- Raygoza Garay, J.A.; Turpin, W.; Lee, S.H.; Smith, M.I.; Goethel, A.; Griffiths, A.M.; Moayyedi, P.; Espin-Garcia, O.; Abreu, M.; Aumais, G.L.; et al. Gut Microbiome Composition Is Associated With Future Onset of Crohn’s Disease in Healthy First-Degree Relatives. Gastroenterology 2023, 165, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Adolph, T.E.; Zhang, J. Diet fuelling inflammatory bowel diseases: Preclinical and clinical concepts. Gut 2022, 71, 2574–2586. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.; Chan, S.S.M.; Touvier, M.; Julia, C.; Tjonneland, A.; Kyro, C.; Dahm, C.C.; Katzke, V.A.; Schulze, M.B.; Tumino, R.; et al. Inflammatory Potential of the Diet and Risk of Crohn’s Disease and Ulcerative Colitis. Aliment. Pharmacol. Ther. 2025, 61, 1032–1042. [Google Scholar] [CrossRef]
- Gerasimidis, K.; Russell, R.K.; Giachero, F.; Gkikas, K.; Tel, B.; Assa, A.; Bronsky, J.; de Ridder, L.; Hojsak, I.; Jenke, A.; et al. Precision nutrition in pediatric IBD: A position paper from the ESPGHAN special interest group for basic science and translational research, the IBD Porto group, and allied health professionals. J. Pediatr. Gastroenterol. Nutr. 2024, 78, 428–445. [Google Scholar] [CrossRef]
- Sigall Boneh, R.; Westoby, C.; Oseran, I.; Sarbagili-Shabat, C.; Albenberg, L.G.; Lionetti, P.; Manuel Navas-Lopez, V.; Martin-de-Carpi, J.; Yanai, H.; Maharshak, N.; et al. The Crohn’s Disease Exclusion Diet: A Comprehensive Review of Evidence, Implementation Strategies, Practical Guidance, and Future Directions. Inflamm. Bowel Dis. 2024, 30, 1888–1902. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Bager, P.; Escher, J.; Forbes, A.; Hebuterne, X.; Hvas, C.L.; Joly, F.; Klek, S.; Krznaric, Z.; Ockenga, J.; et al. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease. Clin. Nutr. 2023, 42, 352–379. [Google Scholar] [CrossRef] [PubMed]
- Kikut, J.; Konecka, N.; Zietek, M.; Kulpa, D.; Szczuko, M. Diet supporting therapy for inflammatory bowel diseases. Eur. J. Nutr. 2021, 60, 2275–2291. [Google Scholar] [CrossRef] [PubMed]
- Marild, K.; Lerchova, T.; Ostensson, M.; Imberg, H.; Stordal, K.; Ludvigsson, J. Early-Life Infections, Antibiotics and Later Risk of Childhood and Early Adult-Onset Inflammatory Bowel Disease: Pooled Analysis of Two Scandinavian Birth Cohorts. Aliment. Pharmacol. Ther. 2025, 61, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Faye, A.S.; Allin, K.H.; Iversen, A.T.; Agrawal, M.; Faith, J.; Colombel, J.F.; Jess, T. Antibiotic use as a risk factor for inflammatory bowel disease across the ages: A population-based cohort study. Gut 2023, 72, 663–670. [Google Scholar] [CrossRef]
- Klein, E.Y.; Impalli, I.; Poleon, S.; Denoel, P.; Cipriano, M.; Van Boeckel, T.P.; Pecetta, S.; Bloom, D.E.; Nandi, A. Global trends in antibiotic consumption during 2016–2023 and future projections through 2030. Proc. Natl. Acad. Sci. USA 2024, 121, e2411919121. [Google Scholar] [CrossRef]
- Thacker, N.; Duncanson, K.; Eslick, G.D.; Dutt, S.; O’Loughlin, E.V.; Hoedt, E.C.; Collins, C.E. Antibiotics, passive smoking, high socioeconomic status and sweetened foods contribute to the risk of paediatric inflammatory bowel disease: A systematic review with meta-analysis. J. Pediatr. Gastroenterol. Nutr. 2024, 79, 610–621. [Google Scholar] [CrossRef]
- Narula, N.; Wong, E.C.L.; Pray, C.; Marshall, J.K.; Rangarajan, S.; Islam, S.; Bahonar, A.; Alhabib, K.F.; Kontsevaya, A.; Ariffin, F.; et al. Associations of Antibiotics, Hormonal Therapies, Oral Contraceptives, and Long-Term NSAIDS With Inflammatory Bowel Disease: Results From the Prospective Urban Rural Epidemiology (PURE) Study. Clin. Gastroenterol. Hepatol. 2023, 21, 2649–2659.e2616. [Google Scholar] [CrossRef]
- Alperen, C.C.; Soydas, B.; Serin, E.; Erbayrak, M.; Savas, N.A.; Unler, G.K.; Meral, C.E.; Toprak, U.; Boyacioglu, A.S.; Dagli, U. Role of Environmental Risk Factors in the Etiology of Inflammatory Bowel Diseases: A Multicenter Study. Dig. Dis. Sci. 2024, 69, 2927–2936. [Google Scholar] [CrossRef]
- Xue, M.; Leibovitzh, H.; Jingcheng, S.; Neustaeter, A.; Dong, M.; Xu, W.; Espin-Garcia, O.; Griffiths, A.M.; Steinhart, A.H.; Turner, D.; et al. Environmental Factors Associated With Risk of Crohn’s Disease Development in the Crohn’s and Colitis Canada—Genetic, Environmental, Microbial Project. Clin. Gastroenterol. Hepatol. 2024, 22, 1889–1897.e12. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | 0 to <6 Years | 6 to <10 Years | 10 to <18 Years | Age Group | 0 to <6 Years | 6 to <10 Years | 10 to <18 Years | Age Group | 0 to <6 Years | 6 to <10 Years | 10 to <18 Years | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | Disease | F | M | F | M | F | M | Year | Disease | F | M | F | M | F | M | Year | Disease | F | M | F | M | F | M | ||
| 2000 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2007 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2014 | CD | 0 | 0 | 0 | 0 | 1 | 2 | ||
| UC | 0 | 0 | 0 | 0 | 0 | 0 | UC | 0 | 0 | 0 | 0 | 0 | 0 | UC | 0 | 0 | 1 | 0 | 2 | 0 | |||||
| pIBD | 0 | 0 | 0 | 0 | 0 | 0 | pIBD | 0 | 0 | 0 | 0 | 0 | 0 | pIBD | 0 | 0 | 1 | 0 | 3 | 2 | |||||
| 2001 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2008 | CD | 0 | 0 | 0 | 1 | 1 | 0 | 2015 | CD | 0 | 0 | 0 | 0 | 2 | 4 | ||
| UC | 0 | 0 | 0 | 0 | 0 | 0 | UC | 0 | 0 | 0 | 0 | 0 | 0 | UC | 1 | 0 | 1 | 0 | 2 | 5 | |||||
| pIBD | 0 | 0 | 0 | 0 | 0 | 0 | pIBD | 0 | 0 | 0 | 1 | 1 | 0 | pIBD | 1 | 0 | 1 | 0 | 4 | 9 | |||||
| 2002 | CD | 0 | 0 | 0 | 0 | 1 | 0 | 2009 | CD | 0 | 0 | 0 | 0 | 2 | 0 | 2016 | CD | 0 | 0 | 0 | 1 | 2 | 3 | ||
| UC | 0 | 0 | 0 | 0 | 0 | 0 | UC | 0 | 0 | 0 | 0 | 1 | 0 | UC | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| pIBD | 0 | 0 | 0 | 0 | 1 | 0 | pIBD | 0 | 0 | 0 | 0 | 3 | 0 | pIBD | 0 | 1 | 0 | 1 | 2 | 3 | |||||
| 2003 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2010 | CD | 0 | 0 | 0 | 0 | 1 | 1 | 2017 | CD | 0 | 0 | 1 | 0 | 2 | 1 | ||
| UC | 1 | 0 | 0 | 0 | 1 | 1 | UC | 0 | 0 | 0 | 2 | 0 | 4 | UC | 0 | 0 | 0 | 0 | 2 | 1 | |||||
| pIBD | 1 | 0 | 0 | 0 | 1 | 1 | pIBD | 0 | 0 | 0 | 2 | 1 | 5 | pIBD | 0 | 0 | 1 | 0 | 4 | 4 | |||||
| 2004 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2011 | CD | 0 | 0 | 0 | 0 | 0 | 1 | 2018 | CD | 0 | 0 | 0 | 0 | 3 | 0 | ||
| UC | 0 | 0 | 0 | 0 | 1 | 0 | UC | 0 | 0 | 0 | 0 | 0 | 1 | UC | 0 | 0 | 0 | 0 | 1 | 1 | |||||
| pIBD | 0 | 0 | 0 | 0 | 1 | 0 | pIBD | 0 | 0 | 0 | 0 | 1 | 2 | pIBD | 0 | 0 | 0 | 0 | 4 | 1 | |||||
| 2005 | CD | 0 | 0 | 0 | 0 | 0 | 0 | 2012 | CD | 0 | 0 | 0 | 0 | 2 | 2 | 2019 | CD | 0 | 0 | 0 | 0 | 0 | 3 | ||
| UC | 0 | 0 | 0 | 0 | 1 | 0 | UC | 0 | 0 | 1 | 0 | 0 | 0 | UC | 0 | 0 | 1 | 1 | 1 | 1 | |||||
| pIBD | 0 | 0 | 0 | 0 | 1 | 0 | pIBD | 0 | 0 | 1 | 0 | 2 | 2 | pIBD | 0 | 0 | 1 | 1 | 2 | 4 | |||||
| 2006 | CD | 0 | 0 | 0 | 0 | 0 | 1 | 2013 | CD | 0 | 0 | 0 | 0 | 0 | 2 | 2020 | CD | 0 | 0 | 0 | 0 | 0 | 8 | ||
| UC | 0 | 0 | 0 | 0 | 0 | 1 | UC | 1 | 0 | 0 | 0 | 1 | 0 | UC | 0 | 0 | 0 | 0 | 2 | 0 | |||||
| pIBD | 0 | 0 | 0 | 0 | 0 | 2 | pIBD | 1 | 0 | 0 | 0 | 1 | 2 | pIBD | 0 | 1 | 0 | 0 | 2 | 8 | |||||
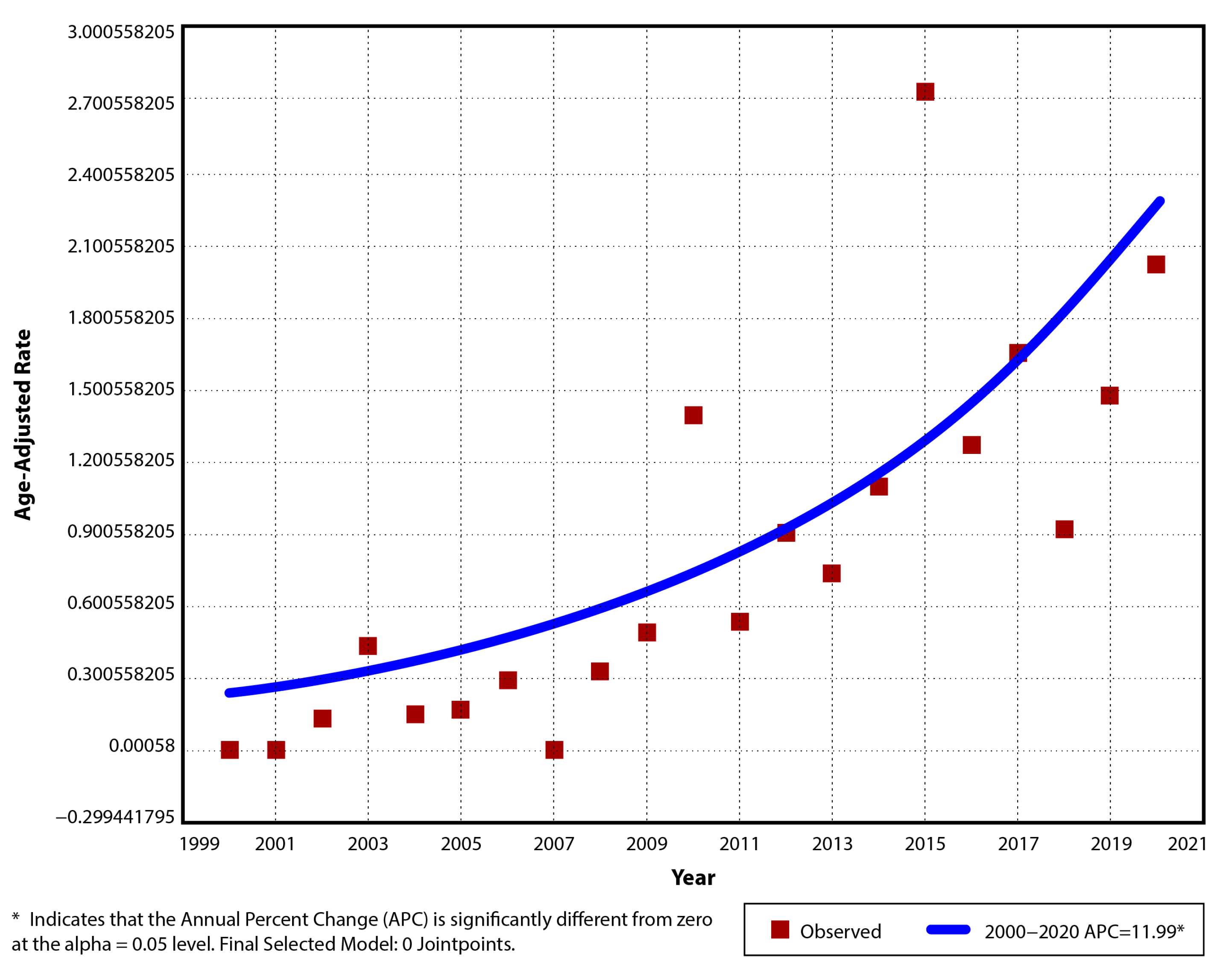
| Year | Cases | Population | Crude Rate (CR) | Age-Adjusted Rate (AAR) | Standard Error (SE) | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|---|---|---|
| 2000 | 0 | 673,805 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2001 | 0 | 664,082 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2002 | 1 | 650,872 | 0.15 | 0.13 | 0.13 | −0.12 | 0.38 |
| 2003 | 3 | 635,385 | 0.47 | 0.43 | 0.25 | −0.06 | 0.92 |
| 2004 | 1 | 620,138 | 0.16 | 0.14 | 0.14 | −0.13 | 0.41 |
| 2005 | 1 | 603,003 | 0.17 | 0.16 | 0.16 | −0.15 | 0.47 |
| 2006 | 2 | 587,201 | 0.34 | 0.29 | 0.21 | −0.12 | 0.70 |
| 2007 | 0 | 570,654 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2008 | 2 | 554,887 | 0.36 | 0.32 | 0.23 | −0.13 | 0.77 |
| 2009 | 3 | 547,296 | 0.55 | 0.48 | 0.28 | −0.07 | 1.03 |
| 2010 | 8 | 541,912 | 1.48 | 1.4 | 0.49 | 0.44 | 2.36 |
| 2011 | 3 | 537,399 | 0.56 | 0.53 | 0.31 | −0.08 | 1.14 |
| 2012 | 5 | 531,879 | 0.94 | 0.9 | 0.4 | 0.12 | 1.68 |
| 2013 | 4 | 528,155 | 0.76 | 0.73 | 0.36 | 0.02 | 1.44 |
| 2014 | 6 | 524,351 | 1.14 | 1.09 | 0.45 | 0.21 | 1.97 |
| 2015 | 15 | 524,824 | 2.86 | 2.73 | 0.71 | 1.34 | 4.12 |
| 2016 | 7 | 523,828 | 1.34 | 1.26 | 0.48 | 0.32 | 2.20 |
| 2017 | 9 | 522,578 | 1.72 | 1.64 | 0.55 | 0.56 | 2.72 |
| 2018 | 5 | 521,722 | 0.96 | 0.91 | 0.41 | 0.11 | 1.71 |
| 2019 | 8 | 519,134 | 1.54 | 1.47 | 0.52 | 0.45 | 2.49 |
| 2020 | 11 | 515,232 | 2.13 | 2.01 | 0.61 | 0.81 | 3.21 |
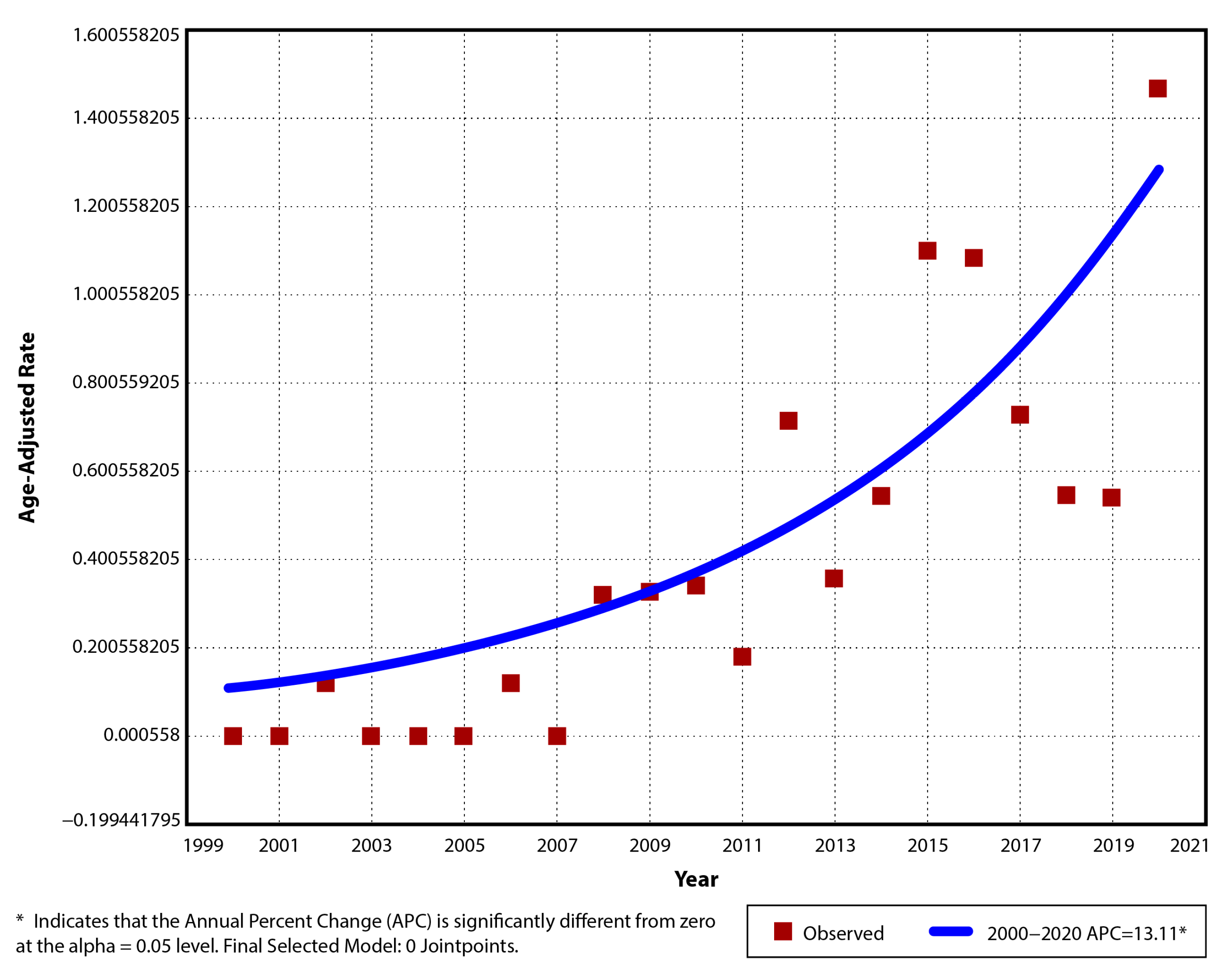
| Year | Cases | Population | Crude Rate (CR) | Age-Adjusted Rate (AAR) | Standard Error (SE) | Lower 95%CI | Upper 95%CI |
|---|---|---|---|---|---|---|---|
| 2000 | 0 | 673,805 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2001 | 0 | 664,082 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2002 | 0 | 650,872 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2003 | 3 | 635,385 | 0.47 | 0.43 | 0.25 | −0.06 | 0.92 |
| 2004 | 1 | 620,138 | 0.16 | 0.14 | 0.14 | −0.13 | 0.41 |
| 2005 | 1 | 603,003 | 0.17 | 0.16 | 0.16 | −0.15 | 0.47 |
| 2006 | 1 | 587,201 | 0.17 | 0.17 | 0.16 | −0.14 | 0.48 |
| 2007 | 0 | 570,654 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2008 | 0 | 554,887 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2009 | 1 | 547,296 | 0.18 | 0.15 | 0.15 | −0.14 | 0.44 |
| 2010 | 6 | 541,912 | 1.11 | 1.05 | 0.43 | 0.21 | 1.89 |
| 2011 | 2 | 537,399 | 0.37 | 0.35 | 0.25 | −0.14 | 0.84 |
| 2012 | 1 | 531,879 | 0.19 | 0.18 | 0.18 | −0.17 | 0.53 |
| 2013 | 2 | 528,155 | 0.38 | 0.36 | 0.26 | −0.15 | 0.87 |
| 2014 | 3 | 524,351 | 0.57 | 0.54 | 0.31 | −0.07 | 1.15 |
| 2015 | 9 | 524,824 | 1.71 | 1.63 | 0.54 | 0.57 | 2.69 |
| 2016 | 0 | 523,828 | 0.00 | 0 | 0.01 | −0.02 | 0.02 |
| 2017 | 3 | 522,578 | 0.57 | 0.55 | 0.32 | −0.08 | 1.18 |
| 2018 | 2 | 521,722 | 0.38 | 0.37 | 0.26 | −0.14 | 0.88 |
| 2019 | 4 | 519,134 | 0.77 | 0.75 | 0.37 | 0.02 | 1.48 |
| 2020 | 2 | 515,232 | 0.39 | 0.37 | 0.26 | −0.14 | 0.88 |
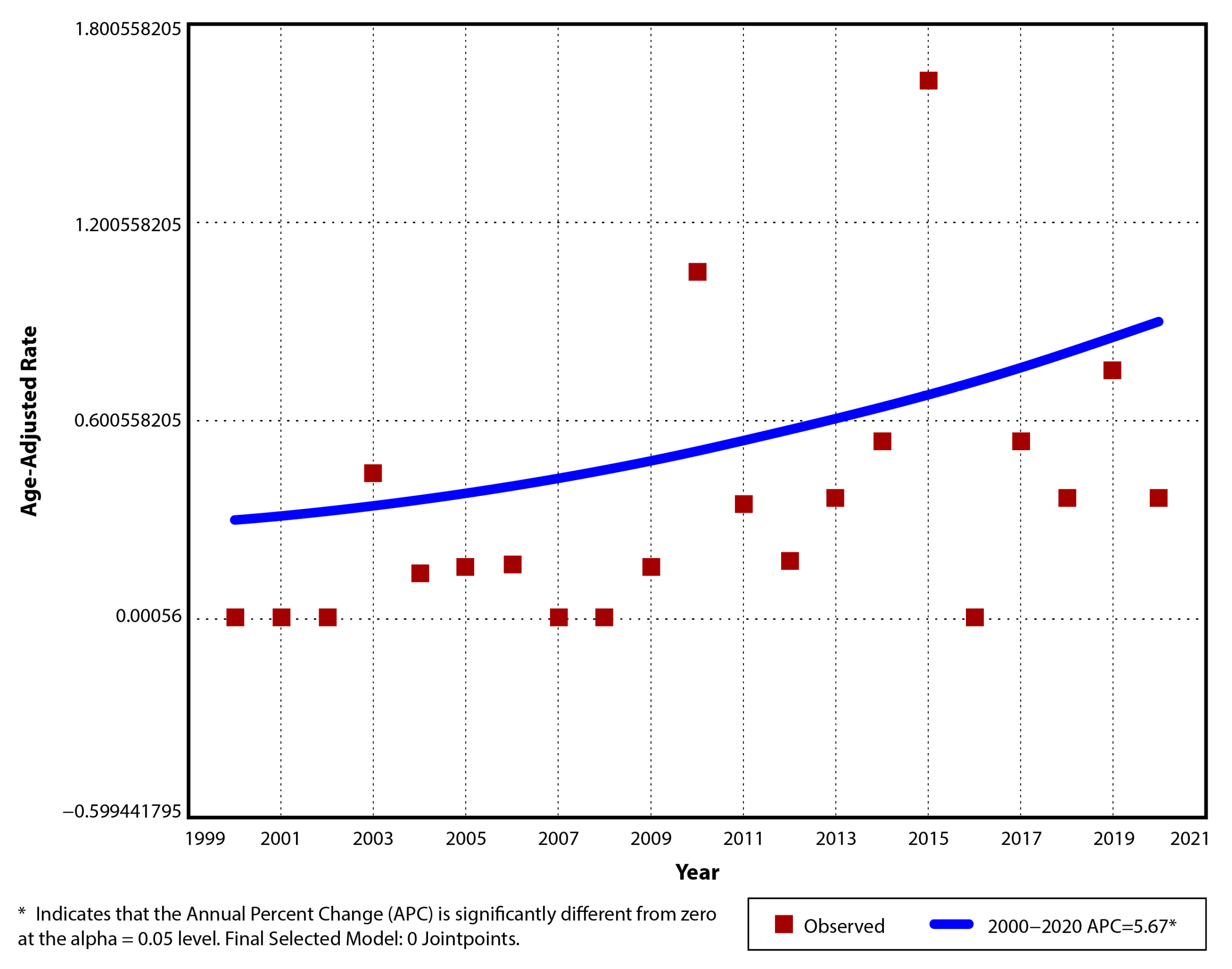
| Year | Cases | Population | Crude Rate (CR) | Age-Adjusted Rate (AAR) | Standard Error (SE) | Lower 95%CI | Upper 95%CI |
|---|---|---|---|---|---|---|---|
| 2000 | 0 | 673,805 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2001 | 0 | 664,082 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2002 | 0 | 650,872 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2003 | 3 | 635,385 | 0.47 | 0.43 | 0.25 | −0.06 | 0.92 |
| 2004 | 1 | 620,138 | 0.16 | 0.14 | 0.14 | −0.13 | 0.41 |
| 2005 | 1 | 603,003 | 0.17 | 0.16 | 0.16 | −0.15 | 0.47 |
| 2006 | 1 | 587,201 | 0.17 | 0.17 | 0.16 | −0.14 | 0.48 |
| 2007 | 0 | 570,654 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2008 | 0 | 554,887 | 0 | 0 | 0.01 | −0.02 | 0.02 |
| 2009 | 1 | 547,296 | 0.18 | 0.15 | 0.15 | −0.14 | 0.44 |
| 2010 | 6 | 541,912 | 1.11 | 1.05 | 0.43 | 0.21 | 1.89 |
| 2011 | 2 | 537,399 | 0.37 | 0.35 | 0.25 | −0.14 | 0.84 |
| 2012 | 1 | 531,879 | 0.19 | 0.18 | 0.18 | −0.17 | 0.53 |
| 2013 | 2 | 528,155 | 0.38 | 0.36 | 0.26 | −0.15 | 0.87 |
| 2014 | 3 | 524,351 | 0.57 | 0.54 | 0.31 | −0.07 | 1.15 |
| 2015 | 9 | 524,824 | 1.71 | 1.63 | 0.54 | 0.57 | 2.69 |
| 2016 | 0 | 523,828 | 0.00 | 0 | 0.01 | −0.02 | 0.02 |
| 2017 | 3 | 522,578 | 0.57 | 0.55 | 0.32 | −0.08 | 1.18 |
| 2018 | 2 | 521,722 | 0.38 | 0.37 | 0.26 | −0.14 | 0.88 |
| 2019 | 4 | 519,134 | 0.77 | 0.75 | 0.37 | 0.02 | 1.48 |
| 2020 | 2 | 515,232 | 0.39 | 0.37 | 0.26 | −0.14 | 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tartamus, G.V.; Serban, D.E.; Fogas, C.R.; Tantau, M.V. Pediatric Inflammatory Bowel Disease in Romania: The First Epidemiological Study of the North-West Region (2000–2020). Children 2025, 12, 403. https://doi.org/10.3390/children12040403
Tartamus GV, Serban DE, Fogas CR, Tantau MV. Pediatric Inflammatory Bowel Disease in Romania: The First Epidemiological Study of the North-West Region (2000–2020). Children. 2025; 12(4):403. https://doi.org/10.3390/children12040403
Chicago/Turabian StyleTartamus (Tita), Georgia Valentina, Daniela Elena Serban, Cristina Rebeca Fogas, and Marcel Vasile Tantau. 2025. "Pediatric Inflammatory Bowel Disease in Romania: The First Epidemiological Study of the North-West Region (2000–2020)" Children 12, no. 4: 403. https://doi.org/10.3390/children12040403
APA StyleTartamus, G. V., Serban, D. E., Fogas, C. R., & Tantau, M. V. (2025). Pediatric Inflammatory Bowel Disease in Romania: The First Epidemiological Study of the North-West Region (2000–2020). Children, 12(4), 403. https://doi.org/10.3390/children12040403