
Anatomical Studies Evaluating Pediatric Regional Anesthesia: A Scoping Review

 , ,
, , 
 and
and 
Abstract
1. Introduction
2. Methods
2.1. Selection of Studies
2.2. Data Extraction
2.3. Data Analysis and Presentation
2.4. Secondary Analysis
3. Results
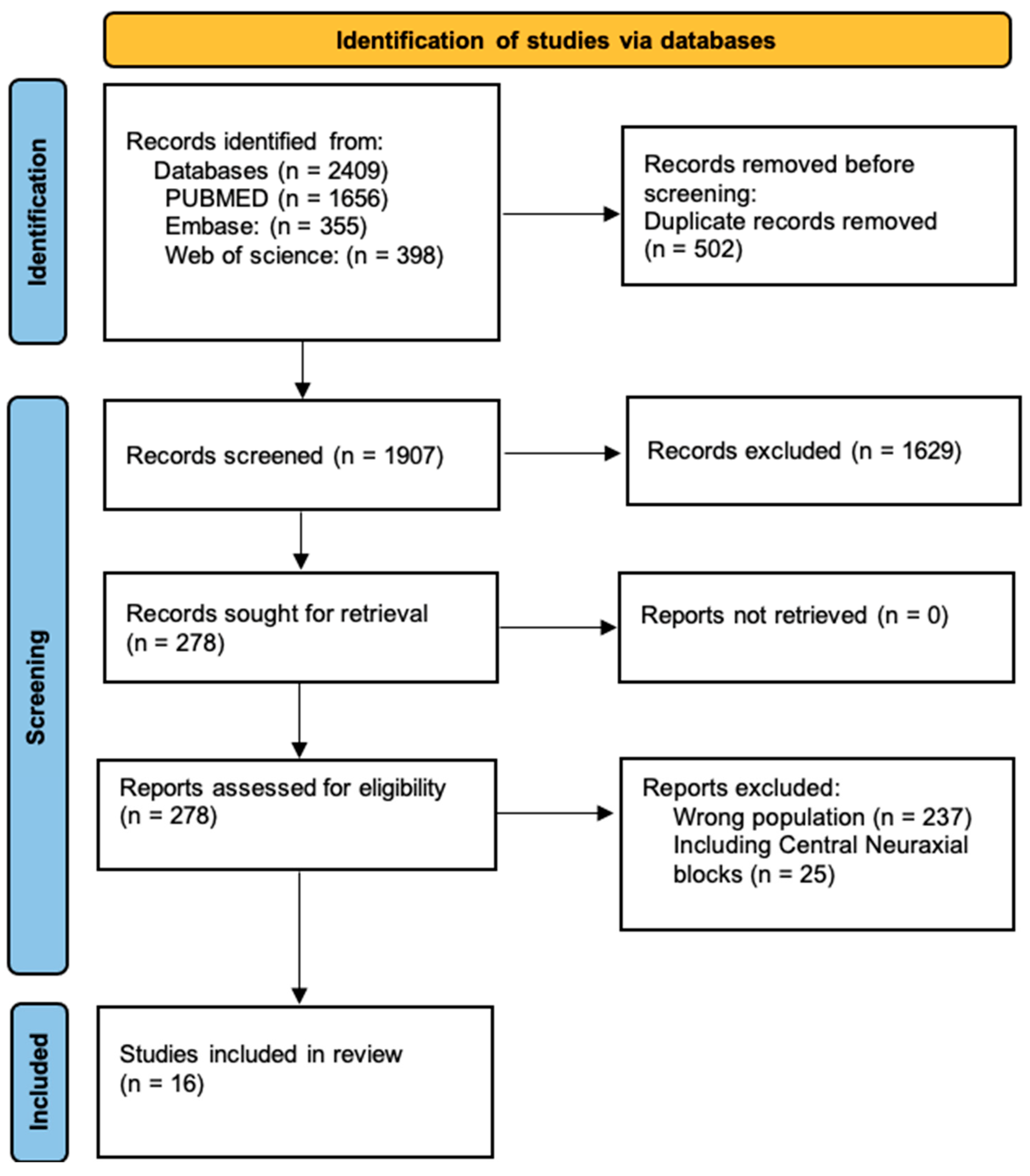
3.1. Search
3.2. Study Characteristics
4. Discussion
Issues Related to Cadaver Preservation/Preparation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heydinger, G.; Tobias, J.; Veneziano, G. Fundamentals and innovations in regional anaesthesia for infants and children. Anaesthesia 2021, 76 (Suppl. S1), 74–88. [Google Scholar] [CrossRef] [PubMed]
- Kendall, M.C.; Alves, L.J.C.; Suh, E.I.; McCormick, Z.L.; De Oliveira, G.S. Regional anesthesia to ameliorate postoperative analgesia outcomes in pediatric surgical patients: An updated systematic review of randomized controlled trials. Local. Reg. Anesth. 2018, 11, 91–109. [Google Scholar] [CrossRef]
- Walters, J.L.; Paule, M.G. Review of preclinical studies on pediatric general anesthesia-induced developmental neurotoxicity. Neurotoxicol Teratol. 2017, 60, 2–23. [Google Scholar] [CrossRef] [PubMed]
- Bier, A. Versuche über Cocainisirung des Rückenmarkes. Dtsch. Z. Chir. 1899, 51, 361–369. [Google Scholar] [CrossRef]
- Taylor, C.; Wilson, F.M.; Roesch, R.; Stoelting, V.K. Prevention of the Oculo-Cardiac Reflex in Children. Comparison of Retrobulbar Block and Intravenous Atropine. Anesthesiology 1963, 24, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Schaldenbrand, K.; Wallis, B.; De Oliveira, G.S., Jr. Regional anaesthesia to improve pain outcomes in paediatric surgical patients: A qualitative systematic review of randomized controlled trials. Br. J. Anaesth. 2014, 113, 375–390. [Google Scholar] [CrossRef]
- Suresh, S.; De Oliveira, G.S., Jr. Local anaesthetic dosage of peripheral nerve blocks in children: Analysis of 40 121 blocks from the Pediatric Regional Anesthesia Network database. Br. J. Anaesth. 2018, 120, 317–322. [Google Scholar] [CrossRef]
- Polaner, D.M.; Taenzer, A.H.; Walker, B.J.; Bosenberg, A.; Krane, E.J.; Suresh, S.; Wolf, C.; Martin, L.D. Pediatric Regional Anesthesia Network (PRAN): A Multi-Institutional Study of the Use and Incidence of Complications of Pediatric Regional Anesthesia. Anesth. Analg. 2012, 115, 1353–1364. [Google Scholar] [CrossRef]
- Taenzer, A.H.; Herrick, M.; Hoyt, M.; Ramamurthi, R.J.; Walker, B.; Flack, S.H.; Bosenberg, A.; Franklin, A.; Polaner, D.M. Variation in pediatric local anesthetic dosing for peripheral nerve blocks: An analysis from the Pediatric Regional Anesthesia Network (PRAN). Reg. Anesth. Pain Med. 2020, 45, 964–969. [Google Scholar] [CrossRef]
- McLeod, G.; McKendrick, M.; Taylor, A.; Lynch, J.; Ker, J.; Sadler, A.; Halcrow, J.; McKendrick, G.; Mustafa, A.; Seeley, J.; et al. Validity and reliability of metrics for translation of regional anaesthesia performance from cadavers to patients. Br. J. Anaesth. 2019, 123, 368–377. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Govender, S.; Mohr, D.; Bosenberg, A.; Van Schoor, A.N. A cadaveric study of the erector spinae plane block in a neonatal sample. Reg. Anesth. Pain Med. 2020, 45, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Govender, S.; Mohr, D.; Bosenberg, A.; Van Schoor, A.N. The anatomical features of an ultrasound-guided erector spinae fascial plane block in a cadaveric neonatal sample. Paediatr. Anaesth. 2020, 30, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Govender, S.; Mohr, D.; Van Schoor, A.N.; Bosenberg, A. The extent of cranio-caudal spread within the erector spinae fascial plane space using computed tomography scanning in a neonatal cadaver. Paediatr. Anaesth. 2020, 30, 667–670. [Google Scholar] [CrossRef]
- van Schoor, A.N.; Boon, J.M.; Bosenberg, A.T.; Abrahams, P.H.; Meiring, J.H. Anatomical considerations of the pediatric ilioinguinal/iliohypogastric nerve block. Paediatr. Anaesth. 2005, 15, 371–377. [Google Scholar] [CrossRef] [PubMed]
- van Schoor, A.N.; Bosman, M.C.; Bosenberg, A.T. Revisiting the anatomy of the ilio-inguinal/iliohypogastric nerve block. Paediatr. Anaesth. 2013, 23, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Reinoso-Barbero, F.; Saavedra, B.; Segura-Grau, E.; Llamas, A. Anatomical comparison of sciatic nerves between adults and newborns: Clinical implications for ultrasound guided block. J. Anat. 2014, 224, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Acar, A.A.; Bösenberg, A.T.; van Schoor, A.N. Anatomical description of the sciatic nerve block at the subgluteal region in a neonatal cadaver population. Paediatr. Anaesth. 2017, 27, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Prigge, L.; van Schoor, A.N.; Bosman, M.C.; Bosenberg, A.T. Clinical anatomy of the maxillary nerve block in pediatric patients. Paediatr. Anaesth. 2014, 24, 1120–1126. [Google Scholar] [CrossRef]
- Albokrinov, A.A.; Fesenko, U.A. Spread of dye after single thoracolumbar paravertebral injection in infants. A cadaveric study. Eur. J. Anaesthesiol. 2014, 31, 305–309. [Google Scholar] [CrossRef]
- Cihan, E.; Buyukmumcu, M.; Ayd1n-Kabakc1, A.D.; Ak1n, D.; Gungorer, S. A Guideline for Femoral Nerve Block with the Age-Related Formulas Obtained from the Distances Between the Femoral Nerve and Surface Anatomical Landmarks in Fetal Cadavers. Int. J. Morphol. 2022, 40, 62–67. [Google Scholar] [CrossRef]
- Gupta, R.; Aggarwal, A.; Sahni, D.; Harjeet, K.; Barnwal, M. Anatomical survey of terminal branching patterns of superficial branch of radial nerve in fetuses. Surg. Radiol. Anat. 2012, 34, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Prigge, L.; van Schoor, A.N.; Bosenberg, A.T. Anatomy of the greater occipital nerve block in infants. Paediatr. Anaesth. 2019, 29, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Yagmurkaya, U.; Uysal, I.I.; Kabakci, A. Definition of an Effective Site for Greater and Third Occipital Nerve Block in the Nuchal Region: A Fetal Cadaver Study. Turk. Neurosurg. 2023, 33, 535–540. [Google Scholar] [CrossRef]
- Bosenberg, A.T.; Van Schoor, A.N.; Bosman, M.C. Infraclavicular Brachial Plexus Blocks. Comparison of Neonatal and Adult Anatomy; UPSpace: West Chester, PA, USA, 2009. [Google Scholar]
- Bösenberg, A.T.; Kimble, F.W. Infraorbital nerve block in neonates for cleft lip repair: Anatomical study and clinical application. Br. J. Anaesth. 1995, 74, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Zadrazil, M.; Feigl, G.; Opfermann, P.; Marhofer, P.; Marhofer, D.; Schmid, W. Ultrasound-Guided Dorsal Penile Nerve Block in Children: An Anatomical-Based Observational Study of a New Anesthesia Technique. Children 2023, 11, 50. [Google Scholar] [CrossRef]
- Davidson, A.J. In search of the big question. Paediatr. Anaesth. 2012, 22, 613–615. [Google Scholar] [CrossRef] [PubMed]
- Naik, V.M.; Fabila, T.S. Practicing pediatric regional anesthesia: Children are not small adults. J. Anaesthesiol. Clin. Pharmacol. 2023, 39, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, F.H. The challenges of research participation by children. Pediatr. Res. 2015, 78, 109–110. [Google Scholar] [CrossRef]
- Behr, A.U.; Chan, V.W.S.; Stecco, C. Living versus cadaver fascial plane injection. Reg. Anesth. Pain Med. 2019, 45, 156. [Google Scholar] [CrossRef]
- Sondekoppam, R.V.; Tsui, B.C.H. “Minimally invasive” regional anesthesia and the expanding use of interfascial plane blocks: The need for more systematic evaluation. Can. J. Anaesth. 2019, 66, 855–863. [Google Scholar] [CrossRef]
- Pavan, P.G.; Stecco, A.; Stern, R.; Stecco, C. Painful connections: Densification versus fibrosis of fascia. Curr. Pain Headache Rep. 2014, 18, 441. [Google Scholar] [CrossRef]
- Elsharkawy, H.; Pawa, A.; Mariano, E.R. Interfascial Plane Blocks: Back to Basics. Reg. Anesth. Pain Med. 2018, 43, 341–346. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Year | Authors | Country | Block Studied | Population | Cadaver Characteristics |
|---|---|---|---|---|---|
| 2020 | Govender et al. [12] | South Africa | ESP Block | 2 neonates | Fresh unembalmed preterm neonatal cadavers subject to cryopreservation; cadaver 1: 1.6 kg, cadaver 2: 0.6 kg. |
| 2020 | Govender et al. [13] | South Africa | ESP Block | 9 neonates | Fresh unembalmed preterm neonatal cadavers subject to cryopreservation. Weight: 0.7 kg, 1.2 kg, 1.35 kg, 1.7 kg, 1.8 kg, 2 kg, 2.6 kg, 2.95 kg, 3.4 kg. |
| 2020 | Govender et al. [14] | South Africa | ESP Block | 1 neonate | Fresh unembalmed preterm neonatal cadaver subject to cryopreservation. Weight: 2.3 kg. |
| 2005 | van Schoor et al. [15] | South Africa | Ilioinguinal iliohypogastric block | 25 infants and neonates | Embalmed cadavers (mean weight = 2.2 kg; mean height = 45.6 cm). |
| 2013 | Van Schoor et al. [16] | South Africa | Ilioinguinal iliohypogastric block | 54 neonates | Embalmed cadavers (mean length: 43 cm; mean weight: 1.9 kg). |
| 2014 | Reinoso-Barbero et al. [17] | Spain | Sciatic nerve block | 13 adults and 11 newborns | Embalmed cadavers in a solution of phenol and glycerin (mean age = 6 days; mean weight = 3.3 kg; mean height = 48.4 cm). |
| 2017 | Acar et al. [18] | South Africa | Sciatic nerve block | 20 neonates | Formalin-fixed preterm and full-term cadavers (mean weight = 1.2 kg; mean height = 40 cm). |
| 2014 | Prigge et al. [19] | South Africa | Maxillary nerve block | 30 pediatrics | 10 dried pediatric skulls and 30 formalin-fixed pediatric cadavers. Group 1—Neonate cadavers; Group 2—28 days to 1 year. |
| 2014 | Albokrinov et al. [20] | Ukraine | Paravertebral block | 20 infants | Fresh, unembalmed infant cadavers (median age = 7 months; median body mass 4550 g). |
| 2022 | Cihan et al. [21] | Turkey | Femoral nerve block | 30 newborns | Formalin-fixed cadavers, ranging in age from 9 to 40 weeks. |
| 2012 | Gupta et al. [22] | India | Radial nerve block | 30 newborns | Spontaneously aborted fetuses with age between 32 and 40 weeks. |
| 2019 | Prigge et al. [23] | South Africa | Greater occipital nerve block | 6 pediatrics | Pediatric formalin-fixed cadavers (mean age 51.4 days and one cadaver of 2 years). |
| 2023 | Yagmurkaya et al. [24] | Turkey | Greater occipital nerve and the third occipitalnerve extend block | 15 fetal cadavers (3rd trimester) | The immersion method used 10% formalin, and the gestational ages were determined depending on the crown–rump length. |
| 2009 | Bosenberg et al. [25] | South Africa | Infraclavicular brachial plexus block | 52 neonates and 81 adults | Mean weight −1.94 kg ± 1.62; mean height—0.43 m ± 0.08. |
| 1995 | Bosenberg et al. [26] | South Africa | Infraorbital nerve block | 15 neonates | Fresh stillborn cadavers (mean weight = 2.85 kg. |
| 2024 | Zadrazil et al. [27] | Austria | Dorsal penile nerve block | 3 pediatric cadaveric specimens | Fixed with Thiel’s method. |
| Year | Authors | Block Studied | Assessment of the Block | Results | Conclusion |
|---|---|---|---|---|---|
| 2020 | Govender et al. [12] | ESP block | The block was replicated using methylene blue dye at vertebral levels T5 using 0.5 mL in cadaver 1 and in T8 using 0.2 mL in cadaver 2. The spread of dye was tracked on the ultrasound and confirmed on dissection. | Cadaver 1—spread from vertebral levels T3 to T6. Cadaver 2—spread from vertebral levels T7 to T11. Methylene blue was found in the paravertebral and epidural spaces, staining both dorsal and ventral rami of spinal nerves T2 to T12. | The dye injected spread to the paravertebral, epidural, and intercostal spaces and over multiple dermatomal levels from T2 to T12. More studies are needed to compare ESP over paravertebral and epidural spaces in this population. |
| 2020 | Govender et al. [13] | ESP block | The block was performed ultrasound-guided bilaterally using 0.1 mL/kg of iodinated contrast dye at vertebral levels T5 and T8. Dissections were performed 30 min after injection. | 14 blocks were successful, and 4 blocks were incomplete or failed. The contrast was found in paravertebral, intercostal, and epidural spaces, including over the neural foramina. The needle direction or entry side did not influence the spread. | The contrast injected was found in the paravertebral, intercostal, and epidural spaces over an average of 5 dermatomal levels using 0.1 mL/kg of solution. |
| 2020 | Govender et al. [14] | ESP block | The ultrasound-guided block was performed bilaterally using 2.3 mL (1 mL/kg) of iodinated contrast dye. It was carried out at vertebral levels T8 on the right-hand side and T10 on the left-hand side, followed by a CT scan after 20 min. | The contrast was observed to spread over three dermatomal levels from T6 to T9 on the right side and over four dermatomal levels from T9 to T12 on the left side. Additionally, it spread over the costotransverse ligament into the paravertebral space, with no spread detected in the epidural space. | The contrast dye was found in the paravertebral space at four dermatomal levels, suggesting an approximate volume of 0.5–0.6 mL per dermatome. |
| 2005 | van Schoor et al. [15] | Ilioinguinal iliohypogastric block | The aim of the study was to use dissection to determine the precise anatomical position of the nerves relative to the ASIS. | The distance from left ilioinguinal nerve—1.9 ± 0.9 mm; Right ilioinguinal nerve—2.0 ± 0.7 mm. Left iliohypogastric nerves to the ASIS—3.3 ± 0.8 mm; right iliohypogastric nerves—3.9 ± 1.0 mm. | It is suggested that the high failure rate of the nerve block in this population could be attributed to a lack of knowledge of the anatomy of these nerves. The insertion point is approximately 2.5 mm from the ASIS, on a line connecting the ASIS to the umbilicus. |
| 2012 | van Schoor et al. [16] | Ilioinguinal iliohypogastric block | The position of the ilioinguinal and iliohypogastric nerves in relation to the ASIS was studied by dissecting neonate cadavers. | - Distance from the ilioinguinal nerve to ASIS: 2.2 ± 1.2 mm. - Distance from the iliohypogastric nerve to ASIS: 3.8 ± 1.3 mm. The recommended needle insertion site is 3.0 mm from ASIS. There is a strong correlation between the needle insertion point and the neonate’s weight. | A linear regression formula was determined to calculate the needle insertion distance (mm) based on the weight (kg): distance (mm) = 0.6 × weight (kg) + 1.8. This formula serves as a guideline for the position of the ilioinguinal and iliohypogastric nerves. |
| 2014 | Reinoso-Barbero et al. [17] | Sciatic nerve block | The SN, TN, and CPN were dissected, and the distances were measured from the origin of the SN to its division and from there to the popliteal crease. The aim was to clarify the anatomical variability. | The distance from the popliteal crease to the sciatic nerve division was shorter in neonates than in adults (1.04 ± 0.9 cm vs. 5.6 ± 5.1 cm). The sciatic nerve divided proportionally farther down the leg in neonates compared to adults (86 ± 13 vs. 74 ± 15). | The site of the SN division shows high variation from birth, being much closer to the popliteal fossa in newborns than in adults. Its position still varies, so ultrasound guidance for this block is highly recommended. |
| 2017 | Acar et al. [18] | SN block | Neonatal cadavers were dissected to locate the sciatic nerve (SN) and measure the distances from the nerve to the greater trochanter of the femur and the tip of the coccyx. | The SN was located 14.9 ± 2.4 mm to the side of the coccyx tip, and the distance from the greater trochanter to the coccyx tip was 27.3 ± 4.0 mm. There was a weak correlation between these distances and the weight and height of the population. | In neonates, the sciatic nerve is typically located midway between the greater trochanter of the femur and the tip of the coccyx. These findings may assist in guiding ultrasound visualization. |
| 2014 | Prigge et al. [19] | Maxillary nerve block | To determine the best approach for blocking the maxillary nerve within the pterygopalatine fossa, this study evaluated the needle course to block the nerve as it exits the skull at the foramen rotundum and compared it with two techniques. | The suprazygomatic approach to the pterygopalatine fossa did not show any statistical significance. However, there were statistically significant differences between the suprazygomatic approach, which enters from the midpoint on the lateral border of the orbit, and the infrazygomatic approach, which enters at a point on a vertical line along the lateral orbit wall. | The suprazygomatic approach from the frontozygomatic angle yields the most consistent results in pediatric cadavers. The needle can be advanced horizontally for approximately 20 mm in neonates and 30 mm for infants younger than one year. |
| 2014 | Albokrinov et al. [20] | PVB | To assess the dispersion of dye in the paravertebral space of infants, evaluate the effectiveness of a single-injection paravertebral block, and determine the ideal volume needed to cover the paravertebral segments by injecting methylene blue dye at the T12 vertebral level and dissecting the cadaver. | The volume and number of segments are strongly correlated. In all cadavers, the T11, T12, and L1 nerve roots were stained. An optimal volume of 0.2 to 0.3 mL per kg was found to involve the T10-L1 segments. We observed an anterior and contralateral spread of dye, and the incidence correlated with the volume of dye. | A single thoracolumbar paravertebral injection can be administered for lower abdominal anesthesia using 0.2 to 0.3 mL/kg of local anesthetic for a single injection. |
| 2022 | Cihan et al. [21] | FN block | To determine an adequate area for safe blocking. The exit point of the femoral nerve block and two measurements were taken: the level of the FN division (high-level division—proximal of the IL; mid-level division—on the level of the IL; and lower-level division—distal of the IL) and its relationship with surrounding structures. | In the study, a strong correlation was found between fetal development and limb division. The researchers observed high-level limb division in 6 fetal cadavers, mid-level division in 33 cadavers, and lower-level division in 21 cadavers. Additionally, two formulas were developed based on the findings. Formula 1 calculates the distance between the FN and the ASIS as −1.221 + 0.408 × gestational age (weeks), while Formula 2 computes the distance between the FN and the PT as −1.321 + 0.621 × gestational age (weeks). | Gestational age-based regression equations from the study indicated that the block site could be effectively identified using palpable bone structures to increase the success of the blockade. |
| 2012 | Gupta et al. [22] | Radial nerve block | To explore the terminal branches of the SBRN in fetuses, 30 cadavers were dissected, and measurements were made of the relationship of cephalic veins and their tributaries, as well as the branching patterns found. | Three distinct patterns of innervation were observed: Type 1 (66.7%): SBRN innervated the lateral two-and-a-half digits. Type 2 (23.3%): SBRN innervated the lateral three digits. Type 3 (10%): SBRN innervated the lateral three-and-a-half digits. Additionally, the cephalic vein intersected more than twice along its course. | This detailed branching pattern will improve the success rate of radial nerve blocks and minimize postoperative complications associated with injuries. |
| 2019 | Prigge et al. [23] | Greater occipital nerve block | Developing a technique to block the greater occipital nerve in children by evaluating the anatomy of the nerve and the occipital artery. Obtaining measurements between the nerve and selected landmarks. | The occipital nerve was located, on average, 22.6 ± 5.6 mm from the external occipital protuberance. The average distance of the medial three fingers measured at the proximal interphalangeal joint was 20.4 ± 4.0 mm, and there was a strong correlation between these measurements. In 83.3% of cases, the occipital artery was positioned laterally to the nerve at the trapezius muscle hiatus. | The greater occipital nerve can be blocked around 23 mm from the external occipital protuberance, medially to the occipital artery. This distance is equivalent to the width of the three middle fingers at the proximal interphalangeal joint. |
| 2023 | Yagmurkaya et al. [24] | Greater occipital nerve and the third occipital nerve extend block | Palpation identified bone landmarks for reference, and measurements were taken prior to dissection. The location, relationship, and variation of the nerves and muscles were observed. | The greater occipital nerve (GON) was observed to pass through the aponeurosis of the trapezius on the superficial plane in all fetal cadavers. In the deep plane, it was noted that the nerve only extended from the medial 1/3 of the semispinalis capitis on the right side without piercing the muscle in 3.3% of cases, while it pierced the muscle in 96.7% of cases in the total fetal cadavers studied. | The effective area for nerve block and other invasive approaches in the suboccipital region was approximately 2–2.5 cm below the RL and 0.5–1 cm lateral to the midline. |
| 2009 | Bosenberg et al. [25] | Infraclavicular brachial plexus block | To determine the relationship between the brachial plexus in the axilla and the coracoid process (CP) and an improved needle insertion site for the infraclavicular block using the CP and the xiphoid process (XS) as landmarks. | - Mean distance between the CP and the lateral cord of the brachial plexus: 5.26 mm - Mean distance between the CP and the medial cord of the brachial plexus: 10.05 mm - Mean distance between CP and needle insertion: 7.66 mm. The distance between CP and the needle insertion point revealed a strong correlation. | Lack of knowledge about differences in distances from bony landmarks and the relative depth of the brachial plexus can lead to complications or failed blocks. |
| 1995 | Bosenberg et al. [26] | Infraorbital nerve block | To determine the location of the infraorbital nerve in neonatal cadavers and identify landmarks for the infraorbital nerve. Measurements were taken from the infraorbital foramen to the base of the alae nasi, palpebral fissure, and the angle of the mouth. | The average distance from the infraorbital nerve to the alae nasi was 7.7 mm (SD 1.3) on the left and 7.5 mm (SD 0.8) on the right. The nerve was located halfway along a line from the angle of the mouth to the midpoint of the palpebral fissure, approximately 15.5 ± 1.5 mm from the angle of the mouth. | The described landmarks are easily identifiable, and we have successfully applied them in clinical situations. Additional studies are necessary to validate this point. |
| 2024 | Zadrazil et al. [27] | Dorsal penile nerve block | To examine the anatomy of the dorsal penile nerve block, dissections were performed to analyze the relevant structures. | The anatomical studies on the three dissected cadaveric specimens gave us the confidence and anatomical knowledge to position the needle tip near the deep neurovascular bundle of the penis. | The feasibility of pediatric penile surgical interventions in spontaneously breathing patients is ensured by precise execution of the penile root block and a thorough understanding of all anatomical structures and potential challenges. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, L.F.G.; Carlos, R.V.; van Schoor, A.; Bosenberg, A.; Luna, N.M.S.; da Costa Silva, R.; de Fátima Bertanha, B.; Carmona, M.J.C.; Quintão, V.C. Anatomical Studies Evaluating Pediatric Regional Anesthesia: A Scoping Review. Children 2024, 11, 733. https://doi.org/10.3390/children11060733
Pereira LFG, Carlos RV, van Schoor A, Bosenberg A, Luna NMS, da Costa Silva R, de Fátima Bertanha B, Carmona MJC, Quintão VC. Anatomical Studies Evaluating Pediatric Regional Anesthesia: A Scoping Review. Children. 2024; 11(6):733. https://doi.org/10.3390/children11060733
Chicago/Turabian StylePereira, Lucas Ferreira Gomes, Ricardo Vieira Carlos, Albert van Schoor, Adrian Bosenberg, Natália Mariana Silva Luna, Rebeca da Costa Silva, Bianca de Fátima Bertanha, Maria José Carvalho Carmona, and Vinícius Caldeira Quintão. 2024. "Anatomical Studies Evaluating Pediatric Regional Anesthesia: A Scoping Review" Children 11, no. 6: 733. https://doi.org/10.3390/children11060733
APA StylePereira, L. F. G., Carlos, R. V., van Schoor, A., Bosenberg, A., Luna, N. M. S., da Costa Silva, R., de Fátima Bertanha, B., Carmona, M. J. C., & Quintão, V. C. (2024). Anatomical Studies Evaluating Pediatric Regional Anesthesia: A Scoping Review. Children, 11(6), 733. https://doi.org/10.3390/children11060733