

Tibial Spine Avulsion Fractures in Paediatric Patients: A Systematic Review and Meta-Analysis of Surgical Management


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Collection Process and Data Items
2.5. Study Risk of Bias Assessment
2.6. Data Synthesis and Measures of Effect
2.7. Heterogeneity and Subgroup Analysis
3. Results
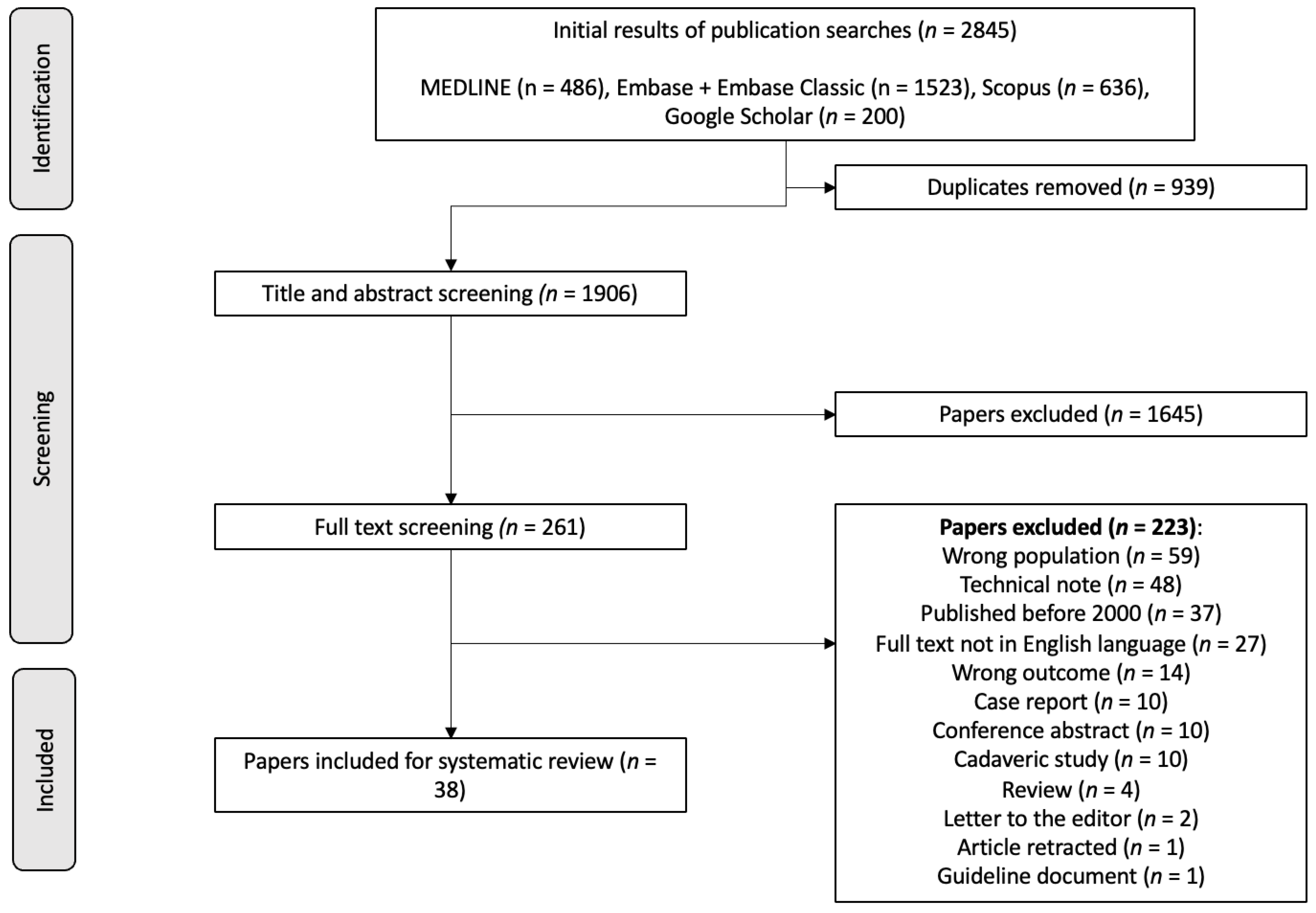
3.1. Search Results and Study Characteristics
3.2. Critical Appraisal
3.3. Population Characteristics
3.4. Screw vs. Suture Fixation
3.5. Screw vs. Suture Risk of Arthrofibrosis
3.6. Screw vs. Suture Risk of Reoperation
3.7. Screw vs. Suture Risk of Post-Operative Pain
3.8. Screw vs. Suture Risk of Instability
3.9. ORIF vs. ARIF Risk of Arthrofibrosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

| Tibial Spine Avulsion Fracture AND | Surgical Management AND | Paediatric Patients |
|---|---|---|
| (Tibial OR Tibia) AND (spine OR eminence OR inter?condylar OR inter?condyle) AND fracture OR avulsion Tibial eminence avulsion Tibial eminence fracture Intercondylar fracture Intercondylar avulsion Anterior cruciate ligament avulsion ACL avulsion | Surgery Surgical treatment Surgical management Operative treatment Operative management Surgical technique Management Treatment Fracture fixation Surgical fixation | Paediatric * Child * Youth High school Adolescent * Paediatric surgery Juvenile |
References
- Poncet, A. Arrachement de l’epine du tibia a l’insertion du ligament croise anterieur. Bull Mem. Soc. Chir. Paris. 1875, 883–884. [Google Scholar]
- Kendall, N.; Hsu, S.; Chan, K. Fracture of the tibial spine in adults and children. A review of 31 cases. J. Bone Joint Surg. Br. 1992, 74-B, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Sapre, V.; Bagari, V. Tibial Spine Avulsion Fractures: Current Concepts and Technical Note on Arthroscopic Techniques Used in Management of These Injuries. In Regional Arthroscopy; InTech: London, UK, 2013. [Google Scholar] [CrossRef]
- Meyers, M.H.; McKeever, F.M. Fracture of the Intercondylar Eminence of the Tibia. J. Bone Jt. Surg. 1959, 41, 209–222. [Google Scholar] [CrossRef]
- Zaricznyj, B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg. Am. 1977, 59, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Tuca, M.; Luderowski, E.; Gausden, E.; Goodbody, C.; Konin, G. A new, MRI-based classification system for tibial spine fractures changes clinical treatment recommendations when compared to Myers and Mckeever. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Meyers, A.L.; Tiwari, V.; Nelson, R. Tibial Eminence Fractures; StatPearls: St. Petersburg, FL, USA, 2024. [Google Scholar]
- Coyle, C.; Jagernauth, S.; Ramachandran, M. Tibial eminence fractures in the paediatric population: A systematic review. J. Child Orthop. 2014, 8, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies (MINORS): Development and Validation of A New Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Abdelkafy, A.; Said, H.G. Neglected ununited tibial eminence fractures in the skeletally immature: Arthroscopic management. Int. Orthop. 2014, 38, 2525–2532. [Google Scholar] [CrossRef]
- Brunner, S.; Vavken, P.; Kilger, R.; Vavken, J.; Rutz, E.; Brunner, R.; Camathias, C. Absorbable and non-absorbable suture fixation results in similar outcomes for tibial eminence fractures in children and adolescents. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 723–729. [Google Scholar] [CrossRef]
- Çağlar, C.; Yagar, H.; Emre, F.; Ugurlu, M. Mid-term Outcomes of Arthroscopic Suture Fixation Technique in Tibial Spine Fractures in the Pediatric Population. Turk. J. Trauma Emerg. Surg. 2020, 27, 571–576. [Google Scholar] [CrossRef]
- Callanan, M.; Allen, J.; Flutie, B.; Tepolt, F.; Miller, P.E.; Kramer, D.; Kocher, M.S. Suture Versus Screw Fixation of Tibial Spine Fractures in Children and Adolescents: A Comparative Study. Orthop. J. Sports Med. 2019, 7, 232596711988196. [Google Scholar] [CrossRef] [PubMed]
- Casalonga, A.; Bourelle, S.; Chalencon, F.; De Oliviera, L.; Gautheron, V.; Cottalorda, J. Tibial intercondylar eminence fractures in children: The long-term perspective. Orthop. Traumatol. Surg. Res. 2010, 96, 525–530. [Google Scholar] [CrossRef]
- Chalopin, A.; Geffroy, L.; Decante, C.; Noailles, T.; Hamel, A. Arthroscopic suture-fixation of anterior tibial intercondylar eminence fractures by retensioning of the ACL and hollowing of the tibial footprint: Objective and subjective clinical results in a paediatric population. Orthop. Traumatol. Surg. Res. 2022, 108, 103270. [Google Scholar] [CrossRef]
- Chotel, F.; Raux, S.; Accadbled, F.; Gouron, R.; Pfirrmann, C.; Bérard, J.; Seil, R. Cartilaginous tibial eminence fractures in children: Which recommendations for management of this new entity? Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 688–696. [Google Scholar] [CrossRef] [PubMed]
- D’Ambrosio, A.; Schneider, L.; Bund, L.; Gicquel, P. Anatomical fixation of tibial intercondylar eminence fractures in children using a threaded pin with an adjustable lock. Orthop. Traumatol. Surg. Res. 2022, 108, 103021. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, E.W.; Fornari, E.D.; Dashe, J.; Roocroft, J.H.; King, M.M.; Pennock, A.T. Results of Displaced Pediatric Tibial Spine Fractures: A Comparison Between Open, Arthroscopic, and Closed Management. J. Pediatr. Orthop. 2015, 35, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Furlan, D.; Pogorelic, Z.; Biocic, M.; Juric, I.; Mestrovic, J. Pediatric tibial eminence fractures: Arthroscopic treatment using K-wire. Scand. J. Surg. 2010, 99, 38–44. [Google Scholar] [CrossRef]
- Hirschmann, M.T.; Mayer, R.R.; Kentsch, A.; Friederich, N.F. Physeal sparing arthroscopic fixation of displaced tibial eminence fractures: A new surgical technique. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 741–747. [Google Scholar] [CrossRef]
- Jääskelä, M.; Turati, M.; Lempainen, L.; Bremond, N.; Courvoisier, A.; Henri, A.; Accadbled, F.; Sinikumpu, J. Long-term Outcomes of Tibial Spine Avulsion Fractures After Open Reduction with Osteosuturing Versus Arthroscopic Screw Fixation: A Multicenter Comparative Study. Orthop. J. Sports Med. 2023, 11, 23259671231176991. [Google Scholar] [CrossRef]
- Kieser, D.C.; Gwynne-Jones, D.; Dreyer, S. Displaced tibial intercondylar eminence fractures. J. Orthop. Surg. 2011, 19, 292–298. [Google Scholar] [CrossRef]
- Kim, K.T.; Shon, S.K.; Kim, S.S.; Song, C.G.; Ha, I.S. Arthroscopic Internal Fixation of Displaced Tibial Eminence Fracture Using Cannulated Screw. J. Korean Orthop. Assoc. 2007, 42, 659–664. [Google Scholar] [CrossRef]
- Kristinsson, J.; Elsoe, R.; Jensen, H.P.; Larsen, P. Satisfactory outcome following arthroscopic fixation of tibial intercondylar eminence fractures in children and adolescents using bioabsorbable nails. Arch. Orthop. Trauma Surg. 2021, 141, 1945–1951. [Google Scholar] [CrossRef]
- Liljeros, K.; Werner, S.; Janarv, P.-M. Arthroscopic Fixation of Anterior Tibial Spine Fractures with Bioabsorbable Nails in Skeletally Immature Patients. Am. J. Sports Med. 2009, 37, 923–928. [Google Scholar] [CrossRef]
- Marie-Laure, L.; Jean-Marc, G.; Franck, L.; Christophe, T.; Jean-Luc, J.; Gérard, B. Surgical management of type II tibial intercondylar eminence fractures in children. J. Pediatr. Orthop. B 2008, 17, 231–235. [Google Scholar]
- Memisoglu, K.; Muezzinoglu, U.S.; Atmaca, H.; Sarman, H.; Kesemenli, C.C. Arthroscopic fixation with intra-articular button for tibial intercondylar eminence fractures in skeletally immature patients. J. Pediatr. Orthop. B 2016, 25, 31–36. [Google Scholar] [CrossRef]
- Momaya, A.M.; Read, C.; Steirer, M.; Estes, R. Outcomes after arthroscopic fixation of tibial eminence fractures with bioabsorbable nails in skeletally immature patients. J. Pediatr. Orthop. B 2018, 27, 8–12. [Google Scholar] [CrossRef]
- Najdi, H.; Thévenin-lemoine, C.; Sales de gauzy, J.; Accadbled, F. Arthroscopic treatment of intercondylar eminence fractures with intraepiphyseal screws in children and adolescents. Orthop. Traumatol. Surg. Res. 2016, 102, 447–451. [Google Scholar] [CrossRef]
- Perugia, D.; Basiglini, L.; Vadalà, A.; Ferretti, A. Clinical and radiological results of arthroscopically treated tibial spine fractures in childhood. Int. Orthop. 2009, 33, 243–248. [Google Scholar] [CrossRef]
- Russu, O.M.; Pop, T.S.; Ciorcila, E.; Gergely, I.; Zuh, S.-G.; Trâmbițaș, C.; Borodi, P.G.; Incze-Bartha, Z.; Feier, A.M.; Georgeanu, V.A. Arthroscopic Repair in Tibial Spine Avulsion Fractures Using Polyethylene Terephthalate Suture: Good to Excellent Results in Pediatric Patients. J. Pers. Med. 2021, 11, 434. [Google Scholar] [CrossRef]
- Scrimshire, A.B.; Gawad, M.; Davies, R.; George, H. Management and outcomes of isolated paediatric tibial spine fractures. Injury 2018, 49, 437–442. [Google Scholar] [CrossRef]
- Sharma, A.; Lakshmannan, P.; Peehal, J.; David, H. An analysis of different types of surgical fixation for avulsion fractures of the anterior tibial spine. Acta Orthop. Belg. 2008, 74, 90–97. [Google Scholar]
- Shimberg, J.L.; Leska, T.M.; Cruz, A.I.; Patel, N.M.; Ellis, H.B.; Ganley, T.J.; Johnson, B.; Milbrandt, T.A.; Yen, Y.-M.; Mistovich, R.J. A Multicenter Comparison of Open Versus Arthroscopic Fixation for Pediatric Tibial Spine Fractures. J. Pediatr. Orthop. 2022, 42, 195–200. [Google Scholar] [CrossRef]
- Shin, C.H.; Lee, D.J.; Choi, I.H.; Cho, T.-J.; Yoo, W.J. Clinical and radiological outcomes of arthroscopically assisted cannulated screw fixation for tibial eminence fracture in children and adolescents. BMC Musculoskelet. Disord. 2018, 19, 41. [Google Scholar] [CrossRef]
- Sinha, S.; Meena, D.; Naik, A.K.; Selvamari, M.; Arya, R.K. Arthroscopic Fixation of Tibial Spine Avulsion in Skeletally Immature: The Technique. J. Orthop. Case Rep. 2017, 7, 80–84. [Google Scholar]
- Tudisco, C.; Giovarruscio, R.; Febo, A.; Savarese, E.; Bisicchia, S. Intercondylar eminence avulsion fracture in children: Long-term follow-up of 14 cases at the end of skeletal growth. J. Pediatr. Orthop. B 2010, 19, 403–408. [Google Scholar] [CrossRef]
- Uboldi, F.M.; Trezza, P.; Panuccio, E.; Memeo, A. Arthroscopic treatment of tibial intercondylar eminence fractures in skeletally immature patients with bioabsorbable nails. La Pediatr. Medica E Chir. 2022, 44. [Google Scholar] [CrossRef]
- Vega, J.R.; Irribarra, L.A.; Baar, A.K.; Iñiguez, M.; Salgado, M.; Gana, N. Arthroscopic Fixation of Displaced Tibial Eminence Fractures: A New Growth Plate–Sparing Method. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 1239–1243. [Google Scholar] [CrossRef]
- Watts, C.D.; Larson, A.N.; Milbrandt, T.A. Open Versus Arthroscopic Reduction for Tibial Eminence Fracture Fixation in Children. J. Pediatr. Orthop. 2016, 36, 437–439. [Google Scholar] [CrossRef]
- Wiegand, N.; Naumov, I.; Vámhidy, L.; Nöt, L.G. Arthroscopic treatment of tibial spine fracture in children with a cannulated Herbert screw. Knee 2014, 21, 481–485. [Google Scholar]
- Wiktor, Ł.; Tomaszewski, R. Results of Anterior Cruciate Ligament Avulsion Fracture by Treatment Using Bioabsorbable Nails in Children and Adolescents. Children 2022, 9, 1897. [Google Scholar] [CrossRef] [PubMed]
- Wouters, D.B.; de Graaf, J.S.; Hemmer, P.H.; Burgerhof, J.G.M.; Kramer, W.L.M. The arthroscopic treatment of displaced tibial spine fractures in children and adolescents using Meniscus Arrows®. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 736–739. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, Z.; Wen, H.; Pan, X. Arthroscopic fixation of pediatric tibial eminence fractures using suture anchors: A mid-term follow-up. Arch. Orthop. Trauma Surg. 2017, 137, 1409–1416. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, L.; Zheng, J.; Ren, B.; Kang, X.; Zhang, X.; Dang, X. Arthroscopic tri-pulley Technology reduction and internal fixation of pediatric Tibial Eminence fracture: A retrospective analysis. BMC Musculoskelet. Disord. 2020, 21, 408. [Google Scholar] [CrossRef]
- Zheng, C.; Han, H.; Cao, Y. Arthroscopically Assisted Cannulated Screw Fixation for Treating Type III Tibial Intercondylar Eminence Fractures: A Short-Term Retrospective Controlled Study. Front. Surg. 2021, 8, 639270. [Google Scholar] [CrossRef]
- Zhou, Y.; Deng, G.; She, H.; Zhou, Y.; Xiang, B.; Bai, F. Arthroscopic percutaneous pullout suture transverse tunnel technique repair for tibial spine fractures in skeletally immature patients. Int. Orthop. 2023, 47, 1353–1360. [Google Scholar] [CrossRef]
- Vannabouathong, C.; Ayeni, O.R.; Bhandari, M. A Narrative Review on Avulsion Fractures of the Upper and Lower Limbs. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2018, 11, 1179544118809050. [Google Scholar] [CrossRef]
- Shimberg, J.L.; Aoyama, J.T.; Leska, T.M.; Ganley, T.J.; Fabricant, P.D.; Patel, N.M.; Cruz, A.I.; Ellis, H.B.; Schmale, G.A.; Green, D.W.; et al. Tibial Spine Fractures: How Much Are We Missing Without Pretreatment Advanced Imaging? A Multicenter Study. Am. J. Sports Med. 2020, 48, 3208–3213. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Micheli, L.J.; Zurakowski, D.; Luke, A. Partial Tears of the Anterior Cruciate Ligament in Children and Adolescents. Am. J. Sports Med. 2002, 30, 697–703. [Google Scholar] [CrossRef]
- Dawkins, B.J.; Kolin, D.A.; Park, J.; Fabricant, P.D.; Gilmore, A.; Seeley, M.; Mistovich, R.J. Sensitivity and Specificity of MRI in Diagnosing Concomitant Meniscal Injuries with Pediatric and Adolescent Acute ACL Tears. Orthop. J. Sports Med. 2022, 10, 232596712210793. [Google Scholar] [CrossRef]
- Bouju, Y.; Carpentier, E.; Bergerault, F.; De Courtivron, B.; Bonnard, C.; Garaud, P. The concordance of MRI and arthroscopy in traumatic meniscal lesions in children. Orthop. Traumatol. Surg. Res. 2011, 97, 712–718. [Google Scholar] [CrossRef]
- Samora, W.P.; Palmer, R.; Klingele, K.E. Meniscal Pathology Associated with Acute Anterior Cruciate Ligament Tears in Patients with Open Physes. J. Pediatr. Orthop. 2011, 31, 272–276. [Google Scholar] [CrossRef]
- Gans, I.; Baldwin, K.D.; Ganley, T.J. Treatment and Management Outcomes of Tibial Eminence Fractures in Pediatric Patients. Am. J. Sports Med. 2014, 42, 1743–1750. [Google Scholar] [CrossRef]
- Munger, A.M.; Gonsalves, N.R.; Sarkisova, N.; Clarke, E.; VandenBerg, C.D.; Pace, J.L. Confirming the Presence of Unrecognized Meniscal Injuries on Magnetic Resonance Imaging in Pediatric and Adolescent Patients with Anterior Cruciate Ligament Tears. J. Pediatr. Orthop. 2019, 39, e661–e667. [Google Scholar] [CrossRef]
- Cirrincione, P.M.; Salvato, D.; Chipman, D.E.; Mintz, D.N.; Fabricant, P.D.; Green, D.W. Extension of Tibial Spine Fractures Beyond the Tibial Spine: An MRI Analysis of 54 Patients. Am. J. Sports Med. 2023, 51, 2085–2090. [Google Scholar] [CrossRef] [PubMed]
- Kushare, I.; Lee, R.J.; Ellis, H.B.; Fabricant, P.D.; Ganley, T.J.; Green, D.W.; McKay, S.; Patel, N.M.; Schmale, G.A.; Weber, M.; et al. Tibial Spine Fracture Management—Technical Tips and Tricks from the Tibial Spine Fracture Research Interest Group. J. Pediatr. Orthop. Soc. N. Am. 2020, 2, 68. [Google Scholar] [CrossRef]
- Salvato, D.; Green, D.W.; Accadbled, F.; Tuca, M. Tibial spine fractures: State of the art. J. ISAKOS 2023, 8, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Eggers, A.K.; Becker, C.; Weimann, A.; Herbort, M.; Zantop, T.; Raschke, M.J.; Petersen, W. Biomechanical Evaluation of Different Fixation Methods for Tibial Eminence Fractures. Am. J. Sports Med. 2007, 35, 404–410. [Google Scholar]
- Osti, L.; Buda, M.; Soldati, F.; Del Buono, A.; Osti, R.; Maffulli, N. Arthroscopic treatment of tibial eminence fracture: A systematic review of different fixation methods. Br. Med. Bull. 2016, 118, 77–94. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Description |
|---|---|
| Type 1 | Non- or minimally displaced (<3 mm) |
| Type 2 | Minimally displaced with intact posterior hinge |
| Type 3a | Completely displaced involving a small portion of the eminence |
| Type 3b | Completely displaced involving the majority of the tibial spine |
| Type 4 | Completely displaced, rotated, and comminuted |
| (Author, Year of Publication) | Title of Paper | Country of Origin | Journal of Publication | Level of Evidence |
|---|---|---|---|---|
| (Abdelkafy and Said, 2014) [11] | Neglected ununited tibial eminence fractures in the skeletally immature: arthroscopic management | Egypt | International Orthopaedics | 4 |
| (Brunner et al., 2016) [12] | Absorbable and non-absorbable suture fixation results in similar outcomes for tibial eminence fractures in children and adolescents | Switzerland | Knee Surgery, Sports Traumatology, Arthroscopy | 3 |
| (Caglar et al., 2021) [13] | Mid-term outcomes of arthroscopic suture fixation technique in tibial spine fractures in the paediatric population | Turkey | Ulusal Travma va Acil Cerrahi Dergisi | 4 |
| (Callanan et al., 2019) [14] | Suture Versus Screw Fixation of Tibial Spine Fractures in Children and Adolescents: A Comparative Study | USA | The Orthopaedic Journal of Sports Medicine | 3 |
| (Casalonga et al., 2010) [15] | Tibial intercondylar eminence fractures in children: The long-term perspective | France | Orthopaedics and Traumatology: Surgery and Research | 4 |
| (Chalopin et al., 2022) [16] | Arthroscopic suture-fixation of anterior tibial intercondylar eminence fractures by retensioning of the ACL and hollowing of the tibial footprint: Objective and subjective clinical results in a paediatric population | France | Orthopaedics and Traumatology: Surgery and Research | 4 |
| (Chotel et al., 2016) [17] | Cartilaginous tibial eminence fractures in children: which recommendations for management of this new entity? | France | Knee Surgery, Sports Traumatology, Arthroscopy | 4 |
| (D’ambrosio et al., 2022) [18] | Anatomical fixation of tibial intercondylar eminence fractures in children using a threaded pin with an adjustable lock | France | Orthopaedics and Traumatology: Surgery and Research | 4 |
| (Edmonds et al., 2015) [19] | Results of Displaced Paediatric Tibial Spine Fractures: A Comparison Between Open, Arthroscopic, and Closed Management | USA | Journal of Paediatric Orthopedics | 3 |
| (Furlan et al., 2010) [20] | Paediatric Tibial Eminence Fractures: Arthroscopic Treatment using K-Wire | Croatia | Scandinavian Journal of Surgery | 4 |
| (Hirschmann et al., 2009) [21] | Physeal sparing arthroscopic fixation of displaced tibial eminence fractures: a new surgical technique | Switzerland | Knee Surgery, Sports Traumatology, Arthroscopy | 4 |
| (Jaaskela et al., 2023) [22] | Long-term Outcomes of Tibial Spine Avulsion Fractures after Open Reduction with Osteosuturing Versus Arthroscopic Screw Fixation: A Multicenter Comparative Study | Italy | The Orthopaedic Journal of Sports Medicine | 3 |
| (Kieser et al., 2011) [23] | Displaced tibial intercondylar eminence fractures | New Zealand | Journal of Orthopaedic Surgery | 4 |
| (Kim et al., 2007) [24] | Arthroscopic Internal Fixation of Displaced Tibial Eminence Fracture Using Cannulated Screw | Republic of Korea | The Journal of The Korean Orthopaedic Association | 4 |
| (Kristinsson et al., 2021) [25] | Satisfactory outcomes following arthroscopic fixation of tibial intercondylar eminence fractures in children and adolescents using bioabsorbable nails | Denmark | Archives of Orthopaedic and Trauma Surgery | 4 |
| (Liljeros et al., 2009) [26] | Arthroscopic Fixation of Anterior Tibial Spine Fractures with Bioabsorbable Nails in Skeletally Immature Patients | Sweden | The American Journal of Sports Medicine | 4 |
| (Marie-Laure et al., 2008) [27] | Surgical management of type II tibial intercondylar eminence fractures in children | France | Journal of Paediatric Orthopaedics B | 4 |
| (Memisoglu et al., 2016) [28] | Arthroscopic fixation with intra-articular button for tibial intercondylar eminence fractures in skeletally immature patients | Turkey | Journal of Paediatric Orthopaedics B | 4 |
| (Momaya et al., 2017) [29] | Outcomes after arthroscopic fixation of tibial eminence fractures with bioabsorbable nails in skeletally immature patients | USA | Journal of Paediatric Orthopaedics B | 4 |
| (Najdi et al., 2016) [30] | Arthroscopic treatment of intercondylar eminence fractures with intraepiphyseal screws in children and adolescents | France | Orthopaedics and Traumatology: Surgery and Research | 4 |
| (Perugia et al., 2009) [31] | Clinical and radiological results of arthroscopically treated tibial spine fractures in childhood | Italy | International Orthopaedics (SICOT) | 4 |
| (Russu et al., 2021) [32] | Arthroscopic Repair in Tibial Spine Avulsion Fractures Using Polyethylene Terephthalate Suture: Good to Excellent Results in Paediatric Patients | Romania | Journal of Personalized Medicine | 4 |
| (Scrimshire et al., 2018) [33] | Management and outcomes of isolated paediatric tibial spine fractures | UK | Injury: International Journal of the Care of the Injured | 4 |
| (Sharma et al., 2008) [34] | An analysis of different types of surgical fixation for avulsion fractures of the anterior tibial spine | UK | Acta Orthopaedica Belgica | 4 |
| (Shimberg et al., 2022) [35] | A Multicenter Comparison of Open Versus Arthroscopic Fixation for Paediatric Tibial Spine Fractures | USA | Journal of Paediatric Orthopedics | 3 |
| (Shin et al., 2018) [36] | Clinical and radiological outcomes of arthroscopically assisted cannulated screw fixation for tibial eminence fracture in children and adolescents | Republic of Korea | BMC Musculoskeletal Disorders | 4 |
| (Sinha et al., 2017) [37] | Arthroscopic Fixation of Tibial Spine Avulsion in Skeletally Immature: The Technique | India | Journal of Orthopaedic Case Reports | 4 |
| (Tudisco et al., 2010) [38] | Intercondylar eminence avulsion fracture in children: long-term follow-up of 14 cases at the end of skeletal growth | Italy | Journal of Paediatric Orthopaedics B | 4 |
| (Uboldi et al., 2022) [39] | Arthroscopic treatment of tibial intercondylar eminence fractures in skeletally immature patients with bioabsorbable nails | Italy | La Pediatria Medica e Chirugica | 4 |
| (Vega et al., 2008) [40] | Arthroscopic Fixation of Displaced Tibial Eminence Fractures: A New Growth Plate-Sparing Method | Chile | Arthroscopy: The Journal of Arthroscopic and Related Surgery | 4 |
| (Watts et al., 2016) [41] | Open Versus Arthroscopic Reduction for Tibial Eminence Fracture Fixation in Children | USA | Journal of Paediatric Orthopedics | 3 |
| (Wiegand et al., 2014) [42] | Arthroscopic treatment of tibial spine fracture in children with a cannulated Herbert screw | Hungary | The Knee | 4 |
| (Wiktor and Tomaszewski, 2022) [43] | Results of Anterior Cruciate Ligament Avulsion Fracture by Treatment Using Bioabsorbable Nails in Children and Adolescents | Poland | Children | 4 |
| (Wouters et al., 2010) [44] | The arthroscopic treatment of displaced tibial spine fractures in children and adolescents using Mensicus Arrows® | The Netherlands | Knee Surgery, Sports Traumatology, Arthroscopy | 4 |
| (Xu et al., 2017) [45] | Arthroscopic fixation of paediatric tibial eminence fractures using suture anchors: A mid-term follow-up | China | Archives of Orthopaedic and Trauma Surgery | 4 |
| (Zhang et al., 2020) [46] | Arthroscopic tri-pulley Technology reduction and internal fixation of paediatric Tibial Eminence: a retrospective analysis | China | BMC Musculoskeletal Disorders | 4 |
| (Zheng et al., 2021) [47] | Arthroscopically Assisted Cannulated Screw Fixation for Treating Type III Tibial Intercondylar Eminence Fractures: A Short-Term Retrospective Controlled Study | China | Frontiers in Surgery | 3 |
| (Zhou et al., 2023) [48] | Arthroscopic percutaneous pullout suture transverse tunnel technique repair for tibial spine fractures in skeletally immature patients | China | International Orthopaedics | 3 |
| (Author, Year of Publication) | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 1 | Item 10 1 | Item 11 1 | Item 12 1 | Total 2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Abdelkafy and Said, 2014) [11] | 2 | 1 | 2 | 2 | 0 | 2 | 2 | 0 | NA 3 | NA | NA | NA | 11 |
| (Brunner et al., 2016) [12] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 15 |
| (Caglar et al., 2021) [13] | 2 | 1 | 0 | 1 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 7 |
| (Callanan et al., 2019) [14] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 19 |
| (Casalonga et al., 2010) [15] | 1 | 1 | 0 | 2 | 1 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Chalopin et al., 2022) [16] | 2 | 1 | 0 | 2 | 1 | 2 | 1 | 0 | NA | NA | NA | NA | 9 |
| (Chotel et al., 2016) [17] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (D’ambrosio et al., 2022) [18] | 2 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | NA | NA | NA | NA | 8 |
| (Edmonds et al., 2015) [19] | 2 | 1 | 1 | 1 | 0 | 2 | 2 | 0 | 2 | 2 | 1 | 2 | 16 |
| (Furlan et al., 2010) [20] | 1 | 2 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Hirschmann et al., 2009) [21] | 2 | 0 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 8 |
| (Jaaskela et al., 2023) [22] | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 20 |
| (Kieser et al., 2011) [23] | 1 | 0 | 0 | 1 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 5 |
| (Kim et al., 2007) [24] | 2 | 0 | 0 | 2 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 7 |
| (Kristinsson et al., 2021) [25] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 11 |
| (Liljeros et al., 2009) [26] | 2 | 2 | 1 | 2 | 0 | 0 | 1 | 0 | NA | NA | NA | NA | 8 |
| (Marie-Laure et al., 2008) [27] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Memisoglu et al., 2016) [28] | 2 | 0 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 8 |
| (Momaya et al., 2017) [29] | 2 | 1 | 1 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 10 |
| (Najdi et al., 2016) [30] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Perugia et al., 2009) [31] | 2 | 0 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 8 |
| (Russu et al., 2021) [32] | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | NA | NA | NA | NA | 12 |
| (Scrimshire et al., 2018) [33] | 2 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | NA | NA | NA | NA | 8 |
| (Sharma et al., 2008) [34] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Shimberg et al., 2022) [35] | 2 | 2 | 1 | 2 | 0 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| (Shin et al., 2018) [36] | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 10 |
| (Sinha et al., 2017) [37] | 1 | 0 | 0 | 2 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 6 |
| (Tudisco et al., 2010) [38] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | 1 | 2 | 0 | 0 | 12 |
| (Uboldi et al., 2022) [39] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Vega et al., 2008) [40] | 2 | 1 | 0 | 2 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 8 |
| (Watts et al., 2016) [41] | 2 | 2 | 1 | 2 | 0 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 18 |
| (Wiegand et al., 2014) [42] | 2 | 1 | 1 | 2 | 0 | 1 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Wiktor and Tomaszewski, 2022) [43] | 2 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 9 |
| (Wouters et al., 2010) [44] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 11 |
| (Xu et al., 2017) [45] | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | NA | NA | NA | NA | 12 |
| (Zhang et al., 2020) [46] | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 0 | NA | NA | NA | NA | 12 |
| (Zheng et al., 2021) [47] | 1 | 1 | 0 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 8 |
| (Zhou et al., 2023) [48] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 0 | NA | NA | NA | NA | 11 |
| (Author, Year of Publication) | Number of Participants | Mean Age | Meyers and McKeever Classification | Surgical Approach | Fixation Method | Mean Follow-Up Time |
|---|---|---|---|---|---|---|
| (Abdelkafy and Said, 2014) [11] | 13 | 10 ± 2.6 | I: 0 II: 0 III: 13 IV: 0 | Arthroscopic: 13 Open: 0 | Screw: 0 Suture: 13 | 10.8 ± 6.8 months |
| (Brunner et al., 2016) [12] | 25 | Group A: 11.1 ± 3.3 Group B: 11.7 ± 3.3 | I: 0 II: 11 III: 14 IV: 0 | Arthroscopic: 25 Open: 0 | Screw: 10 (non-absorbable suture with screw; Group B) Suture: 15 (absorbable with transosseus fixation; Group A) | Group A: 28.1 ± 4.6 months Group B: 47.4 ± 20.7 months |
| (Caglar et al., 2021) [13] | 28 | 14.2 (8–18) | I: 0 II: 16 III: 10 IV: 2 | Arthroscopic: 28 Open: 0 | Screw: 0 Suture: 28 | 4.64 years |
| (Callanan et al., 2019) [14] | 68 | 11.8 ± 2.99 | I: 0 II: 14 III: 50 IV: 0 | Arthroscopic: 68 Open: 0 | Screw: 35 Suture: 33 | 26 (17–47) months |
| (Casalonga et al., 2010) [15] | 32 | 12.0 | I: 8 II: 17 III: 5 IV: 2 | Arthroscopic: 0 Open: 7 Conservative: 25 | Screw: 3 Suture: 4 | 14 years and 11 months (5–21 years) |
| (Chalopin et al., 2022) [16] | 17 | 12 (7–15) | I: 0 II: 5 III: 9 IV: 3 | Arthroscopic: 17 Open: 0 | Screw: 0 Suture: 17 (Single sutures: 11, Double sutures: 6) | 28 months (16–48 months) |
| (Chotel et al., 2016) [17] | 15 | 6.5 ± 1.4 | I: 0 II: 3 III: 6 IV: 6 | Arthroscopic: 6 Open: 0 Mixed: 4 Conservative: 2 | Screw: 0 Suture: 8 | 4.6 years (1–18.5) |
| (D’ambrosio et al., 2022) [18] | 34 | 11.5 ± 2.7 | I: 0 II: 19 III: 12 IV: 3 | Arthroscopic: 34 Open: 0 | Screw: 34 Suture: 0 | 8.8 ± 6 years |
| (Edmonds et al., 2015) [19] | 18 | Arthroscopic: 18.3 ± 2.0 Open: 18.2 ± 3.0 Conservative: 17.4 ± 5.0 | NR | Arthroscopic: 5 Open: 7 Conservative: 6 | Screw: 0 Suture: 12 | Arthroscopic: 5.6 ± 2.0 years Open: 6.8 ± 2.0 years Conservative: 5.8 ± 2.0 years |
| (Furlan et al., 2010) [20] | 10 | 15 (12–17) | I: 0 II: 5 III: 4 IV: 1 | Arthroscopic: 10 Open: 0 | NR (K-wire fixation) | 42 (9–78) months |
| (Hirschmann et al., 2009) [21] | 6 | 14 ± 2 | I: 0 II: 2 III: 3 IV: 1 | Arthroscopic: 6 Open: 0 | Screw: 6 Suture: 0 | 5 ± 2 years |
| (Jaaskela et al., 2023) [22] | 61 | 11.2 ± 2.6 | I: 1 II: 26 III: 34 IV: 0 | Arthroscopic: 29 Open: 32 | Screw: 29 Suture: 32 | 87.0 ± 47.1 months |
| (Kieser et al., 2011) [23] | 9 | 12 (6–15) | I: 0 II: 2 III: 7 IV: 0 | Arthroscopic: 2 Open: 7 | Screw: 2 Suture: 6 | 45 (6–260) weeks |
| (Kim et al., 2007) [24] | 10 | 10.5 (7–13) | I: 0 II: 4 III: 6 IV: 0 | Arthroscopic: 10 Open: 0 | Screw: 10 Suture: 0 | 22.4 (12–81) months |
| (Kristinsson et al., 2021) [25] | 13 | 11 (4–15) | I: 0 II: 9 III: 2 IV: 2 | Arthroscopic: 13 Open: 0 | Screw: 13 Suture: 0 | 6.5 (1–10) years |
| (Liljeros et al., 2009) [26] | 13 | 11 (7–15) | I: 0 II: 1 III: 12 IV: 0 | Arthroscopic: 13 Open: 0 | Screw: 13 Suture: 0 | NR |
| (Marie-Laure et al., 2008) [27] | 17 | 12.1 (6–16) | I: 0 II: 17 III: 0 IV: 0 | Arthroscopic: 0 Open: 17 | NR | 3 (0.5–7) years |
| (Memisoglu et al., 2016) [28] | 11 | 12.2 (10–16) | I: 0 II: 1 III: 9 (A), 1 (B) IV: 1 | Arthroscopic: 11 Open: 0 | Screw: 0 Suture: 0 Both: 11 (+ Endobutton) | 69 (60–84) months |
| (Momaya et al., 2017) [29] | 7 | 11.6 (8–15) | I: 0 II: 1 III: 6 IV: 0 | Arthroscopic: 7 Open: 0 | Screw: 7 Suture: 0 | 31 (24–36) months |
| (Najdi et al., 2016) [30] | 24 | 11 (6–15) | I: 0 II: 15 III: 9 IV: 0 | Arthroscopic: 24 Open: 0 | Screw: 24 Suture: 0 | 2 (1.5–3) years |
| (Perugia et al., 2009) [31] | 10 | 13.5 (12–15) | I: 0 II: 3 III: 7 IV: 0 | Arthroscopic: 10 Open: 0 | Screw: 0 Suture: 10 | 85.8 (20–188) months |
| (Russu et al., 2021) [32] | 12 | 14.3 ± 2.1 | I: 0 II: 0 III: 12 IV: 0 | Arthroscopic: 12 Open: 0 | Screw: 0 Suture: 12 | 6 months |
| (Scrimshire et al., 2018) [33] | 40 | 11.8 | I: 3 II: 13 III: 24 IV: 0 | Arthroscopic: 0 Open: 30 Conservative: 10 | Screw: 30 Suture: 0 | 36 months |
| (Sharma et al., 2008) [34] | 14 (children), 11 (adults) | 13 (8–16) | I: 0 II: 0 III: 19 IV: 6 | Arthroscopic: 0 Open: 24 | Screw: 7 (children), 6 (adults) Suture: 6 (children), 3 (adults) Stainless steel loop: 2 (children), 2 (adults) | 44 months |
| (Shimberg et al., 2022) [35] | 477 | Arthroscopic: 12.1 Open: 12.5 | I: 14 II: 211 III: 252 IV: 0 | Arthroscopic: 420 Open: 57 | NR | 1.12 years |
| (Shin et al., 2018) [36] | 27 | 10.1 ± 2.2 | I: 0 II: 12 III: 13 IV: 2 | Arthroscopic: 27 Open: 0 | Screw: 27 Suture: 0 | 3.9 ± 2.2 years |
| (Sinha et al., 2017) [37] | 10 | 12.1 ± 1.9 | NR | Arthroscopic: 10 Open: 0 | Screw: 0 Suture: 10 | 12 months |
| (Tudisco et al., 2010) [38] | 14 | 12.25 (7–16) | I: 4 II: 3 III: 7 IV: 0 | Arthroscopic: 6 Open: 1 Conservative: 7 | Screw: 0 Suture: 14 | 29 (12–42) years |
| (Uboldi et al., 2022) [39] | 19 | 10 (6–13) | I: 0 II: 5 III: 14 IV: 0 | Arthroscopic: 19 Open: 0 | Screw: 19 Suture: 0 | 27 (6–60) months |
| (Vega et al., 2008) [40] | 7 | 11.8 | I: 0 II: 0 III: 5 IV: 2 | Arthroscopic: 7 Open: 0 | Screw: 0 Suture: 0 Both: 7 | 6 (6–24) months |
| (Watts et al., 2016) [41] | 31 | Arthroscopic group: 12.9 (7–18) Open group: 11.5 (7–16) | NR | Arthroscopic: 18 Open: 13 | Screw: 17 Suture: 11 Both: 3 | Arthroscopic: 13.9 (3–33) months Open: 12.7 (3–50) months |
| (Wiegand et al., 2014) [42] | 8 (+4 treated conservatively) | 12.5 | I: 4 II: 3 III: 5 IV: 0 | Arthroscopic: 8 Open: 0 Conservative: 4 | Screw: 8 Suture: 0 | 1 year |
| (Wiktor and Tomaszewski, 2022) [43] | 17 | 10.1 (5–15.2) | I: 0 II: 5 III: 10 IV: 2 | Arthroscopic: 10 Open: 7 | Screw: 17 Suture: 0 | 28 ± 21.9 months |
| (Wouters et al., 2010) [44] | 12 | 12.0 (6–15) | NR | Arthroscopic: 12 Open: 0 | NR | 3–10 years |
| (Xu et al., 2017) [45] | 20 | 15.3 (13–17) | I: 0 II: 10 III: 6 IV: 4 | Arthroscopic: 20 Open: 0 | Screw: 0 Suture: 20 | 43.4 (40–47) months |
| (Zhang et al., 2020) [46] | 21 | 12.5 (8–16) | I: 0 II: 14 III: 3 (A), 4 (B) IV: 0 | Arthroscopic: 21 Open: 0 | Screw: 0 Suture: 21 | 28.4 ± 5.6 months |
| (Zheng et al., 2021) [47] | Group 1 (arthroscopically assisted cannulated screw fixation) = 12 Group 2 (open reduction and cannulated screw internal fixation) = 10 | Group 1: 10.94 ± 2.00 Group 2: 10.85 ± 1.53 | I: 0 II: 12 III: 22 IV: 0 | Arthroscopic: 12 Open: 10 | Screw: 22 Suture: 0 | 27.5 (12–58) months |
| (Zhou et al., 2023) [48] | Group 1 (transtibial pullout suture technique) = 21 Group 2 (percutaneous pullout suture transverse tunnel) = 20 | Group 1: 12.5 ± 2.6 Group 2: 11.3 ± 2.9 | I: 0 II: 19 III: 22 IV: 0 | Arthroscopic: 41 Open: 0 | Screw: 0 Suture: 41 | Group 1: 33.27 ± 4.18 months Group 2: 34.15 ± 3.65 months |
| (Author, Year of Publication) | Pre-Surgery IKDC Score | Post-Surgery IKDC Score | Pre-Surgery Lysholm Score | Post-Surgery Lysholm Score | Other Outcomes | |
|---|---|---|---|---|---|---|
| Pre-Surgery | Post-Surgery | |||||
| (Abdelkafy and Said, 2014) [11] | Objective: Grade B (1), Grade C (10), Grade D (2) Subjective: 15.4 ± 4.2 | Objective: Grade A (12), Grade B (1) Subjective: 80.5 ± 16.7 | 3.8 ± 2.5 | 91.2 ± 8.9 | VAS: 8.5 ± 1.2 (pain) | VAS: 9.6 ± 0.5 (operation satisfaction), 0.4 ± 0.5 (pain) |
| (Brunner et al., 2016) [12] | NR | Objective Group A: Grade A (10), Grade B (5) Objective Group B: Grade A (7), Grade B (3) Subjective: NA | NR | Group A: 94.1 ± 8.1 Group B: 90.1 ± 10.2 | NR | Rollimeter difference to ipsilateral knee (mm): Group A: 0.5 ± 0.8 Group B: 0.5 ± 0.7 |
| (Caglar et al., 2021) [13] | NR | Objective: NR Subjective: 6 months: 82.3 (68–91); 12 months: 91.4 (81–100); 24 months: 95.7 (89–100) | NR | NR | NR | NR |
| (Callanan et al., 2019) [14] | NR | NR | NR | NR | NR | Time to radiographic union: 2.1 years (suture); 4.3 years (screw) |
| (Casalonga et al., 2010) [15] | NR | Objective: Grade A (4), Grade B (4), Grade C (4), Grade D (1) Subjective: 91 (mailed, n = 10), 81 (at follow-up, n = 13) | NR | NR | NR | ARPEGE Score: 8.3 |
| (Chalopin et al., 2022) [16] | NR | Objective: Grade A (14), Grade B (3) Subjective: 97 ± 2.46 | NR | 99.1 ± 1.62 | NR | NR |
| (Chotel et al., 2016) [17] | NR | Objective: Grade A (9), Grade B (3), Grade C (1) Subjective: 97 (91–100) | NR | 97.36 (94–100) | NR | NR |
| (D’ambrosio et al., 2022) [18] | NR | Objective: NR Subjective: 93.8 ± 6.4 | NR | 93.1 ± 9.8 | NR | Average return to sport time: 9.1 ± 9.5 months Average Tegner Score: 5.6 ± 1.5 |
| (Edmonds et al., 2015) [19] | NR | NR | NR | Arthroscopic: 95 Open: 97.4 Conservative: 86 | NR | Pain (0–10): Arthroscopic: 0.2 Open: 0.7 Conservative: 2.7 |
| (Furlan et al., 2010) [20] | NR | Objective: Grade A (8), Grade B (2) Subjective: 96 (85–100) | NR | NR | NR | NR |
| (Hirschmann et al., 2009) [21] | NR | Objective: Grade A (5), Grade B (1) Subjective: 197 ± 4 | NR | 97 ± 3 | Tegner Score: 8 (6–9) | VAS: 0.5 ± 0.8 (pain), 9.5 ± 1.5 (satisfaction) Tegner Score: 8 (6–9) |
| (Jaaskela et al., 2023) [22] | NR | Objective: NR Subjective: 93.1 ± 13.5 (open osteosuture), 90.4 ± 14.5 (arthroscopic screw) | NR | NR | NR | Time to return to sport (weeks): 8.0 (8–12) (open osteosuture), 21.0 (12–36.3) (arthroscopic screw) |
| (Kieser et al., 2011) [23] | NR | NR | NR | NR | NR | NR |
| (Kim et al., 2007) [24] | NR | NR | NR | 96.3 (92.6–99.0) | NR | NR |
| (Kristinsson et al., 2021) [25] | NR | NR | NR | NR | NR | KOOS Scores:
EQ5D-5L VAS–92.0 (50–100) |
| (Liljeros et al., 2009) [26] | NR | NR | NR | 93.69 | Activity Level (1–3): 2 (1–3) | Activity Level (1–3): 2 (1–3) |
| (Marie-Laure et al., 2008) [27] | NR | NR | NR | 99.7 (95–100) | NR | NR |
| (Memisoglu et al., 2016) [28] | NR | Objective: Grade A (7), Grade B (4) Subjective: 94.3 (85–100) | NR | 95.7 ± 6.6 | NR | NR |
| (Momaya et al., 2017) [29] | NR | Objective: NR Subjective: 97.3 ± 3.5 | NR | 95.6 ± 5.2 | NR | NR |
| (Najdi et al., 2016) [30] | NR | NR | NR | 99.1 ± 1.9 | NR | NR |
| (Perugia et al., 2009) [31] | NR | Objective: Grade A (3), Grade B (4), Grade C (3) Subjective: 92.4 ± 3.3 | NR | 95.9 ± 2.9 | NR | NR |
| (Russu et al., 2021) [32] | Objective: NR Subjective: 33.4 ± 23.3 | Objective: NR Subjective: 84.2 ± 14.3 | 53.7 ± 17.3 | 87.7 ± 9.9 | Tegner Score: 3.8 ± 1.1 | Tegner Score: 6.7 ± 2.2 |
| (Scrimshire et al., 2018) [33] | NR | NR | NR | Operative: 94 (washer used = 92, no washer used = 96) Non-operative: 95 | NR | Cincinnati Score: Operative: 96 Non-operative: 96 |
| (Sharma et al., 2008) [34] | NR | NR | NR | Screw and wire (non-absorbable): 89 (69–100) Suture (absorbable): 100 (85–100) | NR | NR |
| (Shimberg et al., 2022) [35] | NR | NR | NR | NR | NR | NR |
| (Shin et al., 2018) [36] | NR | NR | NR | 94.8 ± 6.8 | NR | NR |
| (Sinha et al., 2017) [37] | NR | NR | 50.8 ± 1.4 | 96.3 ± 2.9 | NR | NR |
| (Tudisco et al., 2010) [38] | NR | Objective: Grade A (2), Grade B (11), Grade C (1) Subjective: NR | NR | NR | NR | NR |
| (Uboldi et al., 2022) [39] | NR | Objective: Grade A (18), Grade B (19) Subjective: 88.45 (80–95) | NR | NR | Tegner Activity Scale: 5.51 (3–7) | Tegner Activity Scale: 5.61 (4–7) |
| (Vega et al., 2008) [40] | NR | Objective: Grade A (4), Grade B (3) Subjective: 92 (86–98) | 29 | 94 | NR | NR |
| (Watts et al., 2016) [41] | NR | NR | NR | NR | NR | NR |
| (Wiegand et al., 2014) [42] | NR | NR | NR | Conservative (Type I): 97.00 Arthroscopic (Type II): 94.97 Arthroscopic (Type III): 94.20 | NR | NR |
| (Wiktor and Tomaszewski, 2022) [43] | NR | Objective: NR Subjective: 84.64 ± 3.10 | NR | 96.64 ± 4.54 | NR | NR |
| (Wouters et al., 2010) [44] | NR | NR | NR | NR | NR | NR |
| (Xu et al., 2017) [45] | Objective: Grade C (15), Grade D (5) Subjective: NR | Objective: Grade A (13), Grade B (7) Subjective: NR | 57.5 ± 11.2 | 91.0 ± 7.2 | Tegner Score: 4.6 ± 1.4 | Tegner Score: 8.0 ± 1.7 |
| (Zhang et al., 2020) [46] | Objective: NR Subjective: 43.1 ± 13.2 | Objective: NR Subjective: 83.8 ± 6.3 | 48.3 ± 6.21 | 87.1 ± 9.8 | NR | NR |
| (Zheng et al., 2021) [47] | NR | Objective: NR Subjective: Group 1: 92.06 ± 3.55 Group 2: 86.07 ± 5.81 | NR | Group 1: 93.33 ± 3.55 Group 2: 86.20 ± 4.52 | NR | Tegner Score: Group 1: 7.75 ± 0.87 Group 2: 6.40 ± 0.52 |
| (Zhou et al., 2023) [48] | Objective: NR Subjective: Group 1: 46.16 ± 12.57 Group 2: 47.27 ± 11.87 | Objective: NR Subjective: Group 1: 90.15 ± 8.12 Group 2: 92.14 ± 7.89 | Group 1: 43.23 ± 9.54 Group 2: 41.62 ± 10.15 | Group 1: 91.08 ± 7.65 Group 2: 92.54 ± 9.17 | Tegner Score: Group 1: 3.26 ± 1.54 Group 2: 3.02 ± 1.34 VAS Score: Group 1: 4.86 ± 0.53 Group 2: 5.13 ± 0.71 | Tegner Score: Group 1: 5.76 ± 1.12 Group 2: 5.52 ± 1.01 VAS Score: Group 1: 1.23 ± 0.41 Group 2: 1.31 ± 0.51 |
| (Author, Year of Publication) | Wound Infection | Post-Surgical Pain | Stiffness | Instability | Arthrofibrosis | Reoperation | Leg Length Discrepancy | Deep Venous Thrombosis |
|---|---|---|---|---|---|---|---|---|
| (Abdelkafy and Said, 2014) [11] | 1 (superficial) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Brunner et al., 2016) [12] | 0 | Group B: 8 (pain around screw) | 0 | 0 | Group A: 3 Group B: 1 | 0 | 0 | 0 |
| (Caglar et al., 2021) [13] | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 |
| (Callanan et al., 2019) [14] | 0 | 0 | Suture: 8 Screw: 11 | Suture: 3 Screw: 22 | Suture: 8 Screw: 11 | Suture: 13 Screw: 23 | 0 | 0 |
| (Casalonga et al., 2010) [15] | 0 | 0 | 3 (Type II) | 0 | 0 | 1 | 0 | 1 |
| (Chalopin et al., 2022) [16] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Chotel et al., 2016) [17] | 0 | 0 | 1 | 0 | 0 | 4 | 6 | 0 |
| (D’ambrosio et al., 2022) [18] | 0 | 0 | 0 | 5 | 0 | 0 | 0 | 0 |
| (Edmonds et al., 2015) [19] | 0 | Conservative: 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Furlan et al., 2010) [20] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Hirschmann et al., 2009) [21] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Jaaskela et al., 2023) [22] | 0 | Arthroscopic screw: 3 | 0 | Arthroscopic screw: 2 | 0 | Arthroscopic screw: 6 Open osteosuture: 3 | 0 | 0 |
| (Kieser et al., 2011) [23] | 0 | 0 | 0 | 0 | 1 | 2 | 0 | 0 |
| (Kim et al., 2007) [24] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Kristinsson et al., 2021) [25] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Liljeros et al., 2009) [26] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 |
| (Marie-Laure et al., 2008) [27] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Memisoglu et al., 2016) [28] | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| (Momaya et al., 2017) [29] | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| (Najdi et al., 2016) [30] | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| (Perugia et al., 2009) [31] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Russu et al., 2021) [32] | NR | NR | NR | NR | NR | NR | NR | NR |
| (Scrimshire et al., 2018) [33] | 0 | 1 | 5 | 0 | 0 | 9 | 0 | 0 |
| (Sharma et al., 2008) [34] | 1 | 0 | 0 | 6 | 0 | 1 | 0 | 0 |
| (Shimberg et al., 2022) [35] | Arthroscopic: 2 (0.5%) | 0 | 0 | 0 | Arthroscopic: 29 (6.9%) Open: 4 (7.0%) | Arthroscopic: 90 (21%) Open: 18 (32%) | Arthroscopic: 6 (1.4%) | 0 |
| (Shin et al., 2018) [36] | 0 | 0 | 1 | 0 | 0 | 0 | 10 | 0 |
| (Sinha et al., 2017) [37] | NR | NR | NR | NR | NR | NR | NR | NR |
| (Tudisco et al., 2010) [38] | 0 | 0 | 0 | Conservative: 1 | 2 | Conservative: 1 | 0 | 0 |
| (Uboldi et al., 2022) [39] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Vega et al., 2008) [40] | NR | NR | NR | NR | NR | NR | NR | NR |
| (Watts et al., 2016) [41] | 0 | 0 | 0 | 0 | Arthroscopic: 7 Open: 1 | 10 | 0 | 0 |
| (Wiegand et al., 2014) [42] | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| (Wiktor and Tomaszewski, 2022) [43] | 0 | 0 | 4 | 0 | 0 | 0 | 0 | 0 |
| (Wouters et al., 2010) [44] | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| (Xu et al., 2017) [45] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Zhang et al., 2020) [46] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Zheng et al., 2021) [47] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| (Zhou et al., 2023) [48] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandanani, M.; Jaibaji, R.; Jaibaji, M.; Volpin, A. Tibial Spine Avulsion Fractures in Paediatric Patients: A Systematic Review and Meta-Analysis of Surgical Management. Children 2024, 11, 345. https://doi.org/10.3390/children11030345
Chandanani M, Jaibaji R, Jaibaji M, Volpin A. Tibial Spine Avulsion Fractures in Paediatric Patients: A Systematic Review and Meta-Analysis of Surgical Management. Children. 2024; 11(3):345. https://doi.org/10.3390/children11030345
Chicago/Turabian StyleChandanani, Mehak, Raian Jaibaji, Monketh Jaibaji, and Andrea Volpin. 2024. "Tibial Spine Avulsion Fractures in Paediatric Patients: A Systematic Review and Meta-Analysis of Surgical Management" Children 11, no. 3: 345. https://doi.org/10.3390/children11030345
APA StyleChandanani, M., Jaibaji, R., Jaibaji, M., & Volpin, A. (2024). Tibial Spine Avulsion Fractures in Paediatric Patients: A Systematic Review and Meta-Analysis of Surgical Management. Children, 11(3), 345. https://doi.org/10.3390/children11030345