Abstract
Currently, there is no intervention model for autism spectrum disorder (ASD) that addresses all levels and factors of the International Classification of Functioning, Disability and Health (ICF, WHO). The most researched programs focus on naturalistic, developmental and behavioral approaches to socio-communication. Less attention has been paid to motor and environmental reactivity aspects (behavior/interest restriction and sensory reactivity). The evidence rationale for the Global Integration Method (MIG, “Método de Integração Global”), a model addressing sensorimotor reactivity in addition to socio-communication, is presented. MIG is an integrative, interdisciplinary, family-oriented intervention and naturalistic program that addresses all levels and moderating factors of ASD’s impact. MIG’s theoretical rationale is based on the predictive coding impairment and embodied cognition hypotheses. MIG incorporates both bottom-up (flexible therapeutic suit, social-motor synchronization) and top-down (schematic social information processing, narratives, imagery) strategies to promote the building and use of accurate, flexible and context-sensitive internal predictive models. MIG is based on the premises that predictive coding improves both socio-communication and environmental reactivity, and that the postural stabilization provided by the flexible therapeutic suit frees information processing resources for socio-cognitive learning. MIG builds on interdisciplinary, professionally and parentally mediated work based on behavioral principles of intensive training in a situated environment.
1. Introduction
Autism spectrum disorder (ASD) is usually a lifelong neurodevelopmental disorder with presumed genetic, environmental and epigenetic causes that influences socialization and communication, in addition to exhibiting restricted, repetitive and stereotyped behavior patterns [1]. People with ASD may have limited involvement in social interactions with peers and restrictions in participation at home, school and in the community. Children and adolescents with ASD may present higher prevalence of intellectual disability, self-injurious behavior, sensory/perceptual difficulties and emotional problems compared to those with typical development [2]. The current literature also highlights the presence of motor abnormalities in ASD, with approximately 80% of children presenting manifestations in different aspects of the motor system [3,4]. Generally, ASD manifests before the age of 3 and results in lifelong challenges for an individual. ASD can manifest in individuals from different ethnic and socioeconomic groups and is more likely to occur in males than females [5]. ASD challenges families and professionals to find effective interventions that can improve functionality and quality of life for individuals throughout their lifespan.
Several interventions have been proposed to help people with ASD and their families [6,7]. In general, the main evidence-based interventions focus on socio-behavioral symptoms [2]. Most children with ASD undergo interventions based on the applied behavioral analysis approach—ABA [4]. Some examples include Naturalistic Developmental Behavioral Interventions—NDBI [8] and Treatment and Education of Autistic and Related Communication Disabilities Children—TEACCH [9]. Data from a large USA study involving 11.814 children with ASD (SPARK study) [10] showed that 67.8% of people with ASD received ABA-based behavioral therapies and 47.7% received social skills interventions. Only 32% of children in the SPARK study received physical therapy for motor dysfunction. An intervention model that strictly emphasizes behavioral or social changes may limit access to interventions necessary to comprehensively meet the needs of children and adolescents with ASD. Therefore, integrated, interdisciplinary and intensive interventions are still needed to address all domains relevant for this population.
The present article aims to introduce and explain the theoretical–methodological bases that guide the Global Integration Method (Método de Integração Global, MIG), an interdisciplinary and intensive intervention program for autism spectrum disorder (ASD, or autism hereinafter). MIG was developed at TREINITEC Ltda. (Ribeirão das Neves, Brazil) based on the work of physical therapist Renato Loffi and his team. The MIG framework was developed mainly considering the needs of children and adolescents requiring levels 2 and 3 of support [1], that is, children with a higher probability of presenting intellectual disability and associated medical conditions. The present text emphasizes the distinguishing features of the MIG program, discussing in depth the theoretical bases and evidence for the specific interventions, mainly motor, that make up the program. The text is divided into eight sections: clinical epidemiology of autism; biopsychosocial impacts of autism; neuropsychological profile of the population with autism; interventions for ASD; characterization of the Global Integration Method; flexible therapeutic suit based on myofascial rails (called MIG Flex) based on myofascial trains supporting complex motor synergies; evaluation of the results of the intervention; strengths and limitations and final considerations. MIG is an important step towards a more comprehensive and integrated approach to intervention. A salient characteristic of the proposed approach is that it adds interventions for sensorimotor issues based on newer concepts of neuropsychological mechanisms implicated in autism, i.e., the predictive coding and embodied cognitive perspectives (the definition of these and other medical and psychological terms is available in Supplementary Materials S1). As MIG integrates several new approaches from multiple disciplines, and considering space limitation intrinsic to a journal article, an appendix with recommended further readings is provided.
2. Clinical Epidemiology of Autism
Autism results from neurodevelopmental diversity, with onset in early childhood and diagnostic stability throughout the lifespan [11,12,13,14,15]. Autism manifests through widely varying behavioral characteristics in three domains of functioning: sociability, communication and environmental reactivity.
From a nosological point of view, autism can be characterized as a disorder or syndrome, with etiological and phenotypic heterogeneity [16]. Autism has become an important public health issue due to the increase in the number of diagnoses in recent decades. A recent meta-analysis showed the worldwide prevalence of ASD to be 0.6% (95% confidence interval: 0.4–1%) [17]. In school-age children, this prevalence is even higher, around 3% to 4% [18,19,20]. There is also evidence that the prevalence is 3 times greater in males [21]. The increase in the number of diagnoses may reflect both changes in diagnostic criteria and greater knowledge of autism, as well as a real increase in its incidence, probably caused by environmental influences [22,23,24,25].
The etiology of autism can be conceptualized in two large groups [26,27]. In a group of individuals, the etiology is more specific and identifiable, being associated with rare genetic variants with low familial recurrence or specific environmental agents. Many of the rare genetic variants are exemplified by genetic syndromes such as Rett, Cornelia de Lange, Tuberous Sclerosis, Angelman and Down syndromes, etc. [28]. Specific etiologies may also be environmental, exemplified by fetal alcohol and fetal cocaine syndromes [29,30,31,32,33], by maternal–fetal immune activation [29], or by exposure to high levels of fetal testosterone [34,35,36,37,38]. Cases with specific etiologies and syndromic characteristics correspond to 10–20% of the cases, and are more likely to present intellectual disability and less likely to have familial recurrence [26,27].
Around 80% to 90% of autism cases do not have a specific etiology, and these are characterized as idiopathic, probably multifactorial [24,26,27]. Cases of multifactorial etiology arising from the interaction between common genetic variants and environmental influences present a greater probability of familial recurrence or the occurrence of cases with an extended or milder autistic phenotype in the family. Multifactorial autism can be characterized as a psychological trait in itself, since it is not possible to identify a specific etiological agent [39,40,41,42].
The therapeutic challenge of autism is to meet the multiple demands imposed by the complexity of its manifestations and biopsychosocial impacts. This is discussed in the next section.
3. Biopsychosocial Impacts of Autism
The phenotypic variability in cases of both syndromic and non-syndromic autism is enormous, potentially expressed at all levels of impact of the World Health Organization’s (WHO) biopsychosocial health model [43,44,45,46] (Figure 1). The impacts on the five levels of the biopsychosocial model are described below.
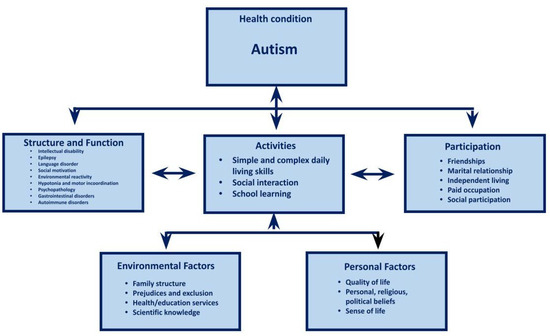
Figure 1.
Biopsychosocial impacts of autism according to the WHO’s biopsychosocial model [46]. Explanation in the text.
3.1. Body Structure and Function
Dysfunctions in the epigenetic regulation of development and neuroplasticity allow us to understand not only the genesis of autism manifestations, but also the pattern of associated comorbidities. Current population estimates indicate that 30% of individuals with autism have intellectual disability [18,19,47]. However, the most recent estimates show that 25% to 30% of children with autism have borderline intelligence [18,19,48]. That is, around 55% to 60% of children with autism have cognitive changes which make their social and academic learning, as well as the acquisition of functional skills in daily life, difficult, constituting a risk factor for several associated conditions [49].
Difficulties with oral language are highly prevalent in autism. Fifty-seven percent of verbal children with autism present structural disorders in the acquisition of oral language [50], in addition to the social–pragmatic difficulties characteristic of autism [51]. Around 27% of children with autism do not acquire oral language skills [52,53]. Autism is associated with an increased risk of school learning disabilities, such as dyslexia and dyscalculia [54,55,56].
Motor manifestations in autism are a relatively neglected aspect [3], and there are few interdisciplinary and intensive models of autism care, including motor physical therapy [57]. Virtually all levels of the motor system are compromised in autism [58,59,60]. More than half of children with autism present hypotonia, and changes in balance, gait, appendicular motor coordination and motor planning are also common [61].
There is evidence that motor function is significantly associated with social skills in autism [58,59,60,62,63,64]. The knowledge about brain and neuropsychological development in the first year of life indicates that sensorimotor difficulties are among the first manifestations of autism, observable in a pre-clinical phase, suggesting that sensorimotor difficulties interfere with social interaction and can contribute to the development of autism manifestations [3,65,66,67,68]. The evidence indicates that there is basic instability in postural mechanisms in autism, which potentially interferes with socio-cognitive learning mechanisms. The understanding that early sensorimotor difficulties may play a role in the development of autism manifestations has been guiding the development of conceptual models of early, presymptomatic intervention [69]. One of the hallmarks of MIG is that it also intervenes in the motor difficulties of autism. This is discussed below.
The manifestations associated with autism at the body structure and function level illustrate the complexity of care demands, which need to be met by different professionals in the health and education areas. Impacts at the activity level are discussed below.
3.2. Activities
The cognitive, linguistic, motor and environmental reactivity peculiarities experienced by children with autism are expressed as difficulties at the activity level. The main difficulties are associated with atypicalities in social learning [13,70]. Autism is usually regarded as an atypicality in social learning, in that most of children’s learning occurs through interaction with adults and peers. Children with autism present difficulties in motivation for social contact as well as peculiar patterns of social reinforcement (e.g., smiles, hugs, speech, gestures), which make it difficult to acquire skills in the diverse situations of daily and social life [68].
In general, many children with autism may be characterized by: (a) apparent attenuated response to social stimuli (e.g., eye contact); (b) difficulty sharing attention and intention; (c) greater interest in objects than in people; (d) preference for solitary activities; (e) apparent reduced interest in social interaction; (f) reduction in initiative and maintenance of conversation; (g) manifest reduced pleasure from social interaction; (h) reduction in the search for social comfort; (i) difficulty in interpreting social stimuli; (j) peculiar reinforcers; (k) peculiar social interaction; etc. [11,12,13,14,15,26].
The social learning difficulties characteristic of autism also have repercussions at the activities level regarding the development of autonomy and functional occupational skills. In autistic children with intellectual disabilities, functional abilities are directly associated with IQ [71,72,73]. However, in autistic children without intellectual disabilities, the level of functional performance is around one standard deviation below IQ [74,75,76].
Next, the impacts of autism at the level of participation are discussed.
3.3. Participation
Participation may be impacted in autism in several ways. Children with autism tend to be lonely, facing difficulties in establishing and maintaining friendships [77,78]. Many children with autism do not have a clear idea of what friendship is, and the degree of intimacy and reciprocity involved [79,80]. Children with autism are infrequently mentioned in sociometric studies carried out in school classes, indicating a certain social “invisibility” [77]. Individuals with autism find it difficult to initiate and maintain sexual and marital relationships [81]. Furthermore, important restrictions on social participation, such as leisure activities, are observed. In adulthood, only 14% of individuals with autism are able to maintain a paid occupation and 49% need to live with their family [82]. The impacts of autism at the body structure and function and activities and participation levels are moderated by environmental and personal factors. Next, environmental factors are discussed.
3.4. Environmental Factors
Environmental factors can represent barriers or facilitators to the individual’s development. The main environments experienced by children with autism are the family, the clinics where they receive care and the schools.
3.4.1. Family
While they depend on good family structure and functioning to develop, children with autism play a significant role in increasing family stress. Of all the neurodevelopmental disorders, autism has the greatest potential impact on the family [82,83,84,85,86,87,88,89,90,91,92]. Families having children with autism are more susceptible to disruption [93], and they present a lower quality of life [94,95,96] and a higher incidence of stress [92,97,98] as well as psychopathologies [99]. After the initial difficulties with the diagnosis, families face difficulties in obtaining the necessary therapies and in finding a school that meets their children’s needs. Difficulties in adolescence can be illustrated by the high incidence of gender dysphoria [100,101]. In adulthood, the family needs to make provisions to support persons with autism if they are unable to lead an independent life. Some autistic children present behavioral characteristics, such as strict adherence to routines, sensory reactivity, food selectivity, hyperactivity, sleep disorders, etc., that require such drastic accommodations from the family that the family becomes maladaptive [102,103]. The quality of health and education services directly affects the structure and well-being of families [94,95].
3.4.2. Health Services
The complexity of the biopsychosocial impacts associated with autism requires a team of multiple health professionals. Treatments need to start early and to be intensive. The costs associated with treatments are enormous, not only from a financial point of view but also in terms of time, energy and affection [103,104]. Multiple treatments carried out by different professionals working independently or maintaining sporadic contact are extremely exhausting. There is also a risk that different professionals act in conflicting manners, pursuing different objectives. Ideally, health services should be provided in an interdisciplinary manner by a coordinated team, giving opportunities for the family to actively participate. Family participation may occur in the decision-making process or in acting as co-therapists and generalizing therapeutic practices from the clinic to the home environment [105,106]. Access to healthcare is associated with quality of life for families of children with autism [96,107].
3.4.3. Educational Services
Attending regular schools and classes is an ideal and a right, hard won by families with children with autism over decades of political mobilization [14]. However, the results of inclusive education are still far from what is desired [14,108]. Most children with autism have difficulty following the curriculum, and schools have difficulty making the necessary curricular adaptations. Often, schools emphasize an academic curriculum that is beyond the ability of many children with autism, while neglecting a functional curriculum that promotes autonomy and independence [14]. The difficulties encountered with inclusion in regular classes have sparked interest in alternative models. As children with autism have difficulties with social learning, imitation and collaboration in groups [13,109], simply being together with typical peers is not enough to promote their learning and social inclusion. Interdisciplinary interventions are necessary to make inclusion effective.
The discussion about the impacts of autism at the environmental factors level demonstrates the complexity of the health and educational needs associated with autism. Next, impacts at the personal factors level are discussed.
3.5. Personal Factors
People with autism have reduced perceptions of quality of life compared to typical individuals [6]. Their perceptions of quality of life reflect the multiple impacts associated with autism, mainly with participation [110]. Individual characteristics, such as intelligence and beliefs (personal, religious and political), constitute important moderators of the perceptions of quality of life in individuals with autism [111]. Difficulties are worsened by loneliness and lack of financial and decision-making autonomy [78,79,80,81,82]. In addition to other psychiatric problems, the risk of suicide is high in persons with autism [112,113]. In Brazil, practically the only community resources available after the age of 18 are support networks for people with intellectual disabilities or multiple disabilities, such as the Associação de Pais e Amigos dos Excepcionais (APAE) [114].
4. Neuropsychological Profile of the Population with Autism
The profound epidemiological changes that have occurred in recent decades have caused a change in the neuropsychological profile of the population with autism. As the prevalence of autism increased, the prevalence of people with autism and intellectual disabilities decreased from around 70% to 30% [18,19,47]. At the same time that this was occurring, the magnitudes of effects of neuropsychological markers that differentiated samples of individuals with and without autism decreased from up to two standard deviations to fewer than 0.5 standard deviations in many cases [115]. This suggests that the increase in prevalence is at least partially related to the increasing identification of autistic traits in individuals without intellectual disability.
The change in the neuropsychological profile of individuals with autism may partially explain the emergence of a new perspective, the identity theory of autism as neurodiversity [12,14]. This perspective proposes that: (a) autism should be considered as a collective identity; (b) autism is not related to any pathology, but simply to a different type of brain, constituting a diversity that characterizes a neurominority; (c) the autistic neurominority is socially and politically stigmatized and oppressed; (d) as it is an identity, it is most appropriate to refer to autistic people not to people “with autism”, since this reifies and makes autism more normal; (e) autism needs to be defined in terms of its advantages and not in terms of deficits, contributing to the development of autistic pride; (f) autism is a valid mode of existence that needs to be recognized and to which society and not the autistic individual needs to adapt; (g) education should not be “special” or “inclusive”, but rather accessible; (h) self-identification as autistic takes precedence over diagnosis by specialists; (i) as there is no disease or deficiency to be “cured”, the neurodiversity identity movement discourages research into neurogenetic bases; and (j) as individuals with autism have the right to self-determination and as, strictly speaking, only they have authority to speak, their participation in the formulation of public discourse and policies must be predominant.
A neurodiverse perspective certainly meets the rights and needs of a growing contingent of individuals with autism, especially adults with higher intelligence or requiring level 1 support in DSM-5 terminology [1]. However, it may conflict with the rights and needs of individuals with associated patterns of comorbidities, such as intellectual disabilities and genetic syndromes, corresponding to levels 2 and 3 of support. It is also necessary to consider that: (a) although the number of people with autism and normal intelligence has substantially increased in recent years, around 55% of children with autism in demographic representative samples have an IQ below 85 [48]; (b) the variability in the prevalence of autism diagnosis without intellectual disability from one research center to another is three times greater than the variability in the prevalence of autism diagnosis with intellectual disability [18,19], indicating that the diagnosis of autism without intellectual disability may be more complex and with lower inter-examiner reliability; (c) studies with clinical samples show a higher prevalence (around 50% to 55%) of intellectual disability in autism [21,116] compared to a prevalence of 30% in population samples [18,19,47], indicating that children with autism associated with intellectual disability may have greater or different assistance needs; (d) a sampling bias towards high intelligence was identified in research published in leading journals since 94% of participants did not present intellectual disability [117], suggesting that the needs for research on autism in association with intellectual disability may not be receiving due consideration; and, finally, (e) a fourfold increase in the risk of dementia occurring between 30 and 64 years of age has been identified for individuals with autism compared to the general population [110], indicating that persons with autism are neurologically vulnerable and require specific healthcare. MIG was designed considering the health and education needs of more vulnerable individuals with autism.
Phenotypic heterogeneity is the hallmark of autism. It has been notoriously difficult to characterize endophenotypes that bridge between the multifactorial etiologic influences and the autistic phenotype [16]. Evidence is emerging, however, that at least two fuzzy prototypes may be identified [26,27]. On the one hand, a growing contingent of individuals with autism do not present intellectual disability. In these cases, there is a stronger preponderance of occurrence in males, the family recurrence of the broad phenotype is higher, genetic markers are represented by common alleles, the association with parental age is low, there is an association with longer intergestational intervals and macroencephaly is more frequent. On the other hand, some individuals with autism present intellectual disability or some degree of cognitive change. In these cases, there is a weaker preponderance of occurrence in males, the family recurrence of the broad phenotype is lower, genetic markers are represented by rare alleles or new mutations, the association with parental age is higher, there is an association with shorter intergestational intervals and brain size is variable. These two prototypes may represent extremes of a continuum, reflecting the heterogeneity of the autistic phenotype. An intervention program for autism must consider the entire, or at least the largest possible, range of phenotypic variations, meeting the needs of those children with more severe conditions, including those associated with intellectual disabilities and/or genetic syndromes. The price to be paid may be the irrelevance or even offensiveness of this approach for people with autism who are cognitively more fortunate.
5. Interventions for ASD
The last few decades have witnessed remarkable progress in interventions for autism, with cumulative evidence regarding their validity, especially studies with single-subject experimental designs. Most of these interventions are based on the hypothesis that autism consists primarily of an atypicality in social learning. In general, four trends can be identified in the literature. The first studies evaluated applied behavior analysis in relatively limited clinical settings using discrete trial training (DTT). DTT has been used successfully both to manage behavior problems and to develop abilities in preschool children participating in intensive intervention programs ranging from 20 to 40 h/week [118]. Behavioral principles have also been applied in the school setting using the TEACCH approach [9]. More recently, the behavioral approach has benefited from integration with evidence on the trajectory of children’s social development in naturalistic settings. This has given rise to naturalistic developmental behavioral interventions (NDBIs) such as the Early Start Denver Model [119], Joint Attention, Symbolic Play, Engagement and Regulation (JASPER [120]) and Pivotal Response Training [121]. Criteria for establishing intervention validity have been established [122]. As these programs require intensive intervention for several hours per week, the costs are extremely high. One way to reduce costs, while maintaining the treatment intensity, is to work with parents as co-therapists. This has been proposed in programs such as Project ImPACT (Improving Parents as Communication Teachers [123]). Working with parents as co-therapists may eventually improve generalization as the treatment is implemented in the home.
While it is important to recognize the effectiveness of behavioral programs, it is also necessary to recognize their limitations. Behavioral interventions for autism focus on maladaptive behaviors and the development of social communication abilities. An important phenotypic dimension of autism, consisting of impairments of environmental reactivity such as stereotypies, restricted repertoires of behaviors and interests, resistance to change and insistence on sameness, hypo- and/or hyper-sensory reactivity, anxiety symptoms, etc., remains unaddressed or unexplained.
As will be seen in the next section, recent theoretical developments related to the predictive coding deficit hypothesis and embodied cognition impairments have important explanatory and intervention implications.
6. Global Integration Method (Método de Integração Global–MIG)
Considerations of the complexity and potential severity of the biopsychosocial impacts associated with autism support the need for integrative and intensive intervention programs, which should begin as early as possible [124]. These programs should be delivered in an interdisciplinary manner by a well-trained and cohesive team [105,106], working in a single location and in concert with the family in the pursuit of common goals [125,126].
The MIG does not consist of just a single intervention method, but rather an integrated and interdisciplinary program of multiple intervention strategies which seek to consider the greatest possible number of levels of impact, according to the WHO’s biopsychosocial model and its complex interactions [48]. The main characteristics of MIG, its theoretical–methodological foundation and the respective references are described in Table 1.

Table 1.
Characteristics of the Global Integration Method (MIG—Método de integração Global).
Table 2 describes the units of the City of Tomorrow, a naturalistic environment where many of the activities are developed with the child. The City of Tomorrow is an immersive therapeutic space that provides greater involvement of children and adolescents, has reward systems (based on applied behavior analysis [148]) and uses structured cognitive models of learning (based on the theory of cognitive overload, which bases learning on the development of cognitive schemes [138,139]). The City of Tomorrow is composed of units called naturalistic learning environments, in which the child has the opportunity to carry out activities relevant to life in situations that resemble their natural environment (i.e., home and school) in a playful way and using concrete materials.
Table 2.
City of Tomorrow’s naturalistic learning units.
In each City of Tomorrow unit, children have the opportunity to develop intrinsically reinforcing activities while developing powerful cognitive schemes, and learning to use them in a concrete and contextualized way that is relevant to life. The use of cognitive schemas is based on the cognitive load theory [138,139]. Working memory constitutes the locus of learning [181]. As processing capacity is limited in working memory, overload needs to be avoided for any learning to take place. The construction of complex knowledge structures called schemas contributes to information processing by reducing working memory overload [139].
The main cognitive schemes worked on and which underlie the City of Tomorrow units are: (a) social information processing theory [148,163]; (b) self-instruction in problem solving [155,156,157]; (c) story grammar [168,169,170,171]; (d) autobiographical memory [154,155,170]; (e) trajectory model of number concept development [161,162]; (f) cognitive–neuropsychological models of oral lexical processing [164,167] and the reading and writing of words [165,167] and numbers [166,182]; and (g) cognitive–neuropsychological models of drawing [172,175].
The use of cognitive schemes in the City of Tomorrow can be illustrated through the Supermarket (“Mercadinho”) Unit. The Supermarket Unit simulates two important scripts of daily life: going to the supermarket and a children’s party. The children receive a visit from a little Martian friend and plan to have a welcome party for which they need to go shopping at the supermarket. Children are invited to reflect on the scripts for going to the supermarket and organizing parties, explaining how everything works to another child without any prior experience. The visit to the Supermarket offers the opportunity to reflect on the causal–temporal structure of these itineraries, on the essential and accessory components, etc. At the same time, the child can develop vocabulary and functional and taxonomic categorization skills of items available in the supermarket, as well as develop elementary numerical–arithmetic skills related to quantities, numerical representations and operations with small sets. Planning skills are developed through the self-instruction schema for problem solving [156,158].
Some children with neurodevelopmental disorders present more serious difficulties in organizing their behavior and attention. Problems with executive functioning are exemplified by difficulties in concentrating, sustaining and dividing attention; maintaining and processing information in working memory; inhibiting inappropriate responses to the current context; and planning to monitor and implement problem-solving strategies flexibly that allow behavior to be organized according to objectives, etc. [183]. These difficulties are accentuated in children with intellectual disabilities, autism and attention deficit hyperactivity disorder. The Intuitive Learning Desk, which is used to work on attention and executive function and to develop work routines, aims to offer physical support that enables the organization of behavior to promote more effective learning for children with the greatest need for support.
The desk has raised edges to make it easier to understand the division of the space, as well as to prevent materials from falling to the floor. The desk allows height and inclination adjustment, and is spatially organized into a central top (task execution) area with a concave cut at the bottom, which allows the student to be closer to the desk, and two foldable side flaps. The divisions “Left Side Flap”, “Execution Area” and “Right Side Flap” allude to the processes of starting, executing and ending the proposed task, respectively (Figure 2). Tasks are offered and performed from left to right, just like the Western reading and writing pattern.
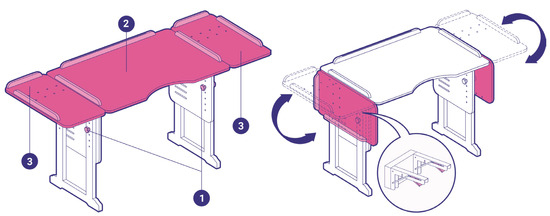
Figure 2.
The Intuitive Learning Desk. Legend: 1 = handles for height (allowing height variation from 52 to 70.7 cm) and inclination adjustment; 2 = task execution area (75 × 50 cm); 3 = side flaps (47 × 33 cm each).
In the next section, the basis of MIG in evidence is discussed.
6.1. Evidence Rationale for MIG
MIG is a complex program of interventions with the following hallmarks: (a) intensive interdisciplinary care by a single team working in an integrated manner in a single location; (b) coverage of all impact levels of the International Classification of Functioning, Disability and Health (ICF–Body Structure and Function; Activities and Participation; Environmental and Personal Factors); (c) specific physical therapeutic and cognitive interventions for socio-motor manifestations, using both bottom-up (flexible therapeutic suit based on myofascial trails and development of cognitive schemas) and top-down (socio-motor synchronization, motor planning through imagery, self-instruction in problem solving, etc.) strategies; (d) decisions shared with the family, and parents acting as co-therapists in managing behavioral problems and promoting social learning skills; (e) manualization, continuing training and supervision of the professionals involved; and (f) management through application.
MIG was developed from a broad literature review of original and secondary research (systematic reviews and meta-analyses) [2,184,185,186,187]. Each of the MIG components is supported by empirical evidence, presented in Table 1. Each of the characteristics and interventions that compose MIG was selected based on the availability of evidence regarding its effectiveness. Established clinical guidelines, results of original empirical studies, systematic reviews and meta-analyses from randomized, controlled clinical trials as well as quasi-experimental studies with single-subject designs were considered. Each of the components in Table 1 is based on an empirical–theoretical–methodological rationale and available evidence [25,184,185]. The strength of the MIG is that it integrates all these components into a comprehensive program, implemented by professionals who are trained and supervised. The principles of applied behavior analysis embodied by MIG are described below.
6.2. Applied Behavior Analysis
In the 1970s, Ole Ivar Lovaas began a series of studies of interventions based on applied behavior analysis for individuals with autism, finding favorable results for the practice [188,189]. Since then, other intervention modalities based on applied behavior analysis (ABA), such as discrete trial training (DTT), pivotal response treatment and naturalistic and developmental behavioral interventions (NDBIs) have been developed.
The most widespread practices using evidence-based interventions for ASD are based on ABA [2], which is considered a science in itself and not just a method or type of intervention. ABA is the science that applies knowledge from the assumptions of Skinner’s radical behaviorism to contribute to issues of social relevance, such as education and health [190]. The method developed by Lovaas [118,188,189], based on applied behavior analysis, is known as DTT.
An important advancement in the psychological therapies for autism was the advent of naturalistic, developmental behavioral interventions, or NDBIs [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123]. NDBI programs add naturalistic and developmental considerations to the traditional behavioral methods developed under ABA. The naturalistic–developmental behavioral approach emphasizes the involvement of parents as co-therapists [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123]. MIG follows this trend in that it emphasizes activities in naturalistic environments with relevance to practical and social everyday life, as well as parental involvement. MIG also uses conceptual tools from cognitive psychology [140,141] based on the assumption that children with autism have difficulties with anticipating events, which originates from inaccurate predictive models, rigidities or difficulties in handling prediction errors [191]. This will be discussed in the Relevance of Predictive Coding for Autism section.
MIG is characterized as an interdisciplinary intervention proposal for ASD, based not only on the principles of ABA science, but also on principles of cognitive neuropsychology and evidence-based practices, such as those mentioned above. The concepts and techniques of behavior analysis are implemented in MIG through a double strategy. On the one hand, professionals from different specialties are trained to use naturalistic–developmental behavioral strategies. The various therapeutic activities provide an opportunity for professionals to manage inappropriate behaviors in a non-coercive way and to develop prosocial and occupational skills in the child. This is implemented following the child’s lead through a playful and narrative context in a naturalistic environment, the City of Tomorrow. The strategies are based on differential reinforcement with natural reinforcers, shaping and chaining with cues and cue fading, organization of the environment and structuring of routines, child-initiated learning, shared control and reciprocity in activities, expansion of attentional focus, playful imitation of the child by the adult, modeling and managing the level of stress and emotions, etc. [8]. On the other hand, parents receive one hour per week of individualized counseling on parent training based on the same principles [123]. At least three parent training curricula are offered, each lasting 15 weeks. In the first semester, parents learn the basics of child social development and applied behavior analysis, learning how to use non-coercive problem management strategies. In the second semester, parents work on the development of social skills (shared attention, imitation, play, shared intention, etc.) and occupational skills (nutrition, personal hygiene, etc.) according to need. From the third semester of intervention, families begin to receive individualized parent training programs, focusing on specific issues on demand.
Therefore, the program proposes an intensive and comprehensive treatment covering a wide range of characteristics associated with autism, going beyond difficulties in socio-communication and encompassing sensorimotor aspects, language and daily life skills, among others.
MIG recommends that the evidence base for non-pharmacological interventions for autism not depend only on the application of Protocol A or B, but that it include the clinical reasoning of professionals working as a team and collaborating with families in the development and monitoring of therapeutic goals. Decisions need to be made as a team, working together with the family to establish goals, formulate hypotheses regarding the causes of certain problems and systematically test these hypotheses through specific interventions. The evidence-based healthcare philosophy underlying MIG can only be implemented at the expense of the ongoing training and supervision of the professionals involved.
Having thus far discussed the characteristics of the main components of MIG and its evidence base, the following sections discuss the theoretical–methodological foundation of one of the main hallmarks of MIG, precisely the interventions at the body structure and function level, which are mainly related to motor manifestations. The evidentiary basis for this approach comes from evidence regarding the importance that predictive coding dysfunctions play in autism [15,191] and the embodied basis of socio-cognition [192]. First, however, the traditional psychological approach that considers autism basically as a social learning atypicality is discussed.
6.3. Relevance of Social Learning for Autism
According to Siegel (2018) [14], autism can be considered a learning disorder comprising three important domains: (a) social interaction, (b) communication and (c) environmental reactivity. Social learning is essential for a child’s cognitive, communicational and affective development. Children learn from observing the consequences of their interactions with others and from observing the behavior of others in different contexts, through direct and vicarious learning mechanisms.
Many children with autism pay more attention to details and objects than to social situations and people, presenting difficulties in learning from interaction. Children with autism tend to be more responsive to instrumental reinforcement than to social reinforcement. Children with autism experience difficulties with cognitively mediated imitation, as well as with symbolic and social play, which are essential for development and learning.
The most effective intervention approaches for autism are based on applied behavior analysis, seeking to make the child more sensitive to social reinforcement and using social reinforcement to develop skills of shared attention and intention, cognitively mediated imitation and symbolic and social play [8].
One of the limitations of more traditional theories and interventions for autism is their substantial focus on the socio-communicational dimension to the detriment of environmental reactivity [15,193]. An important group of autism traits relates to environmental reactivity: (a) children with autism tend to be hyper- and hypo-reactive to sensory stimulation; (b) children with autism tend to self-stimulate and present stereotypies as a way of controlling their level of excitability; (c) children with autism tend to present neophobia, adhering rigidly to routines and showing resistance to change; (d) children with autism tend to show hyperfocus of attention on details, restricting their repertoire of interests and behaviors; and (e) children with autism tend to present instability in motor and postural regulation mechanisms, which manifests as excessive micromovement, difficulties with static and dynamic balance and difficulties with appendicular coordination and motor planning.
Two alternative theoretical approaches, based on the ideas of predictive coding [15,191] and embodied cognition [192], allow for an understanding of both the socio-communicational difficulties and the environmental reactivity observed in autism. Theories of deficits in predictive coding and embodied cognition in autism underlie the use of flexible therapeutic suits based on myofascial trails, which constitute a hallmark of MIG. This is discussed in the next two sections.
6.4. Relevance of Predictive Coding for Autism
The social learning deficit hypothesis does not adequately explain symptoms related to atypicalities in environmental reactivity [13]. A hypothesis with the potential to explain the three dimensions of autism (social, communicational and reactivity) is that the basic difficulty in autism may be related to a deficit in predictive coding [15,194]. The acronym PIA, derived from “prediction impairment in autism”, was proposed to refer to this hypothesis.
The predictive coding hypothesis originates from considerations that the brain processes and interprets sensory information so that it can be used to construct the phenomenological experience and regulate the decision-making processes [15,194]. The brain constantly builds predictions concerning the state of the world and seeks to minimize any discrepancies between these predictions and sensory inputs.
The brain is structured hierarchically [194]. The lower levels of the hierarchy represent specific details of the sensory input. The higher levels of the hierarchy represent interpretations at increasing levels of abstraction and generalization. At each level of the hierarchy, predictions are generated about the nature of the sensory input based on previously acquired experiences and knowledge. A discrepancy between predictions and sensory input constitutes a predictive error, and the main objective of hierarchical brain organization is to minimize predictive errors. Minimizing errors can occur through updating predictions, building new internal models (schemas) or through action to transform reality so that sensory inputs align with predictions.
Predictions represent top-down processing mechanisms, that is, a descending flow of control [194]. Prediction errors constitute bottom-up processing mechanisms, that is, an upward flow of control. The learning process consists of updating internal models or schemas based on prediction errors. The brain learns from its mistakes, adapts to changes and is able to make increasingly more credible predictions. The construction of internal models or schemes is based on bottom-up mechanisms of statistical learning, or Bayesian inference [193].
Predictive coding in autism can be compromised in at least three main ways: (a) deficits in the statistical learning processes in the form of difficulties with prototypical categorization and formation of cognitive schemes, resulting in poorly predictive internal models; (b) deficits in the statistical learning processes or neglect of context, resulting in the construction of rigid and inflexible internal models; and (c) deficits in the descending control mechanisms, corresponding to the impairments in executive functioning observed in autism. Empirical evidence is still insufficient to decide among these alternatives [191]. Most likely, these three hypotheses are complementary.
The hypothesis that deficits in predictive coding occur in autism has important implications for intervention. The emphasis on autism adopted in MIG is justified by the demographic prominence of this condition. At the same time, the implications of the predictive coding hypothesis are important not only for autism, but also for other conditions such as intellectual disability, ADHD, anxiety and even lack of stimulation. The main intervention strategies basically consist of explicit instruction based on error-free learning to develop more credible and flexible internal predictive models, involving the child in playful and concrete activities in a naturalistic environment. Both bottom-up and top-down strategies are used.
The bottom-up strategy consists of providing experiences and reflection that encourage the development of cognitive schemas, which give meaning to subjective and objective reality. Narratives constitute one of the most powerful cognitive schemas, as they allow for thematizing of conceptual, factual, procedural, social and practical aspects of learning. In this context, strategies based on feedback from the brain to the lower-lying parts of the brain hierarchy (top-down strategies) are important to allow the brain to check the value of its own predictions about the environment. In other words, information originating from senses is sent to the brain, and then the brain responds by selecting the information that is useful for its comprehension of the environment. Thus, an important strategy is to reduce processing overload in working memory, and consequently, more resources are available for processing novelty and contextual idiosyncrasies.
Autism presents motor manifestations at multiple levels. There are also manifestations of the axial and appendicular muscles, computational mechanisms (planning, feed-forward control and execution), functional mechanisms (e.g., intention, goal, neuromotricity, kinematics), the level of neural integration (e.g., cortex, basal ganglia, cerebellum), etc. The motor skills of people with autism may be compromised at different levels. At a very basic level, autistic people present instability in postural mechanisms, which manifests itself in the form of exaggerated micro-movements. Most likely, the exaggeration of micro-movements is related to a deficit in reafference mechanisms (efferent copies or corollary discharges) [195].
Evidence suggests that motor alterations may play an important role in the development of social skills in autism [4,58]. The two main mechanisms implicated are resonance and interference [58]. The mirror neuron system is one of the neural mechanisms enabling the activity of an individual’s neuromotor system to resonate with the motor activity of other individuals. This socio-motor resonance is essential for all psychological, social, cognitive, socio-emotional, etc., development. Resonance is a computational property of complex systems, such as the brain, that function in an oscillatory way. Whenever two systems come into oscillatory-phase synchrony, they resonate. That is, phase transitions, i.e., qualitative changes in information processing and development, occur. Individuals with autism have difficulties with motor synchronization mechanisms. In a finger tapping task, the phase anticipation of autistic people is always greater. This difficulty is not related to an intrinsic deficit in the internal generation of rhythms, but rather to a difficulty in synchronization caused by detecting invariance in the environment. Evidence suggests difficulties with socio-motor synchronization.
Socio-motor synchronization is essential for social, affective, cognitive, etc., development. These psychomotor synchronizations begin in the womb and continue in the baby’s first bodily interactions with the mother. Difficulties in socio-motor synchronization in autism are complicated by the fact that difficulties in statistical learning and in detecting invariances lead to a deficit in detecting biological motion. If typical people need to make a gesture at the same time as they watch another person making the opposite gesture, a cognitive conflict arises and people become confused. Autistic people do not experience this conflict because they are less affected by “biological movement”. Autistic people may find socio-motor synchronization easier with robots [196,197]. The other mechanism by which motor changes influence socio-cognition is mutual interference, discussed in the next section on the relevance of embodied cognition for autism.
6.5. Relevance of Embodied Cognition for Autism
Embodied cognition considers that mental activity in general, and cognitive activity in particular, have origins in bodily action mechanisms [192]. Illustrative examples of the embodied origin of cognitive activity are verbal working memory and the development of syntax and arithmetic skills.
The first arithmetic activity performed by children is counting. The use of fingers to count and solve arithmetic operations during a child’s development is practically universal. Finger counting plays the important role of reducing the processing burden on working memory as the child learns to coordinate the dual tasks of reciting the number series and making the correspondence between the recited numbers and the objects counted [198]. Over time, children begin to count without using their fingers, counting only verbally until they develop conceptual and mnemonic problem-solving strategies.
The examples above illustrate how bodily sensorimotor activity forms the foundation for the development of progressively more abstract cognitive skills. Most children with neurodevelopmental disorders present sensorimotor changes [199], ranging from basic disorders of postural tone reflected in excessive micro-movements to changes in static and dynamic balance and various forms of appendicular coordination [135].
Sensorimotor instability consumes energy and information processing resources, which are scarce [135]. Motor action and social interaction share internal regulatory mechanisms [137]. Therefore, the energy and attention that the child spends to stabilize the motor system drains resources that should be applied to other areas of learning, such as sociability and cognition. This creates a dual-task situation in which the need for voluntary control over sensorimotor stabilization competes with socio-cognitive activities related to learning for processing resources [130,132,134,136].
Sensorimotor action is fundamental for affective and social development [68,200]. The exchange of affect, as well as social interaction in general, depend on different forms of synchronization of an individual’s bodily activity, such as gaze, with the activities of other people [200]. Sensorimotor interactions compromised early in autism [201] are important precursors of language and socio-emotional development [202,203,204], constituting therapeutic targets of naturalistic–developmental behavioral interventions [2,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204]. Use of MIG Flex is based on the empirical–theoretical assumption that motor stabilization facilitates social, emotional and cognitive development.
Bidirectional interference between motor and cognitive activities occurs in dual-task paradigms, such as bouncing a ball (or walking) or solving a math problem at the same time [132]. Motor–cognitive interference is frequently observed in the elderly [205]; in neurological diseases, such as multiple sclerosis [206]; and in neurodevelopmental conditions such as Down syndrome [130], cerebral palsy [133] and autism [131,133]. The individual needs to spend scarce working memory resources to regulate motor activity. As these processing resources are limited, there are fewer resources left to process socio-cognitive information. If the individual is absorbed with maintaining their posture, they are less able to pay attention and absorb what is happening in their environment, especially their social environment, which is the most dynamic. MIG Flex, which is based on dynamic myofascial geometry, fulfills the dual purpose of: (a) reducing the effects of interference between motor and socio-cognitive activity and (b) providing opportunities for the child to acquire control over their physical and social environment through activities in which they learn to regulate and use body action for exploring visual space, for recognizing and using objects, and for social interaction. The next section discusses the theoretical foundation of MIG Flex.
7. Flexible Therapeutic Suit (MIG Flex) Based on Myofascial Trains
Different technologies have been developed to enhance the results of rehabilitation for children with developmental disorders. Among these technological innovations, for example, therapeutic suits are very popular in different countries and with various models aiming at promoting improvement in gross motor and postural function, increasing speed and gait cadence and improving trunk control [205,207,208].
The therapeutic suits were inspired by the “Penguin Suit” developed for the Soviet space program in the late 1960s [209]. This first model of the suit was designed to offer resistance to body movements and promote tissue and biomechanical adaptation of astronauts in conditions of reduced gravity in space, minimize adverse effects such as muscular atrophy and osteopenia and maintain neuromuscular fitness [209]. Following this, other suits were developed to be associated with intensive and specific treatment protocols for neurofunctional rehabilitation, for example, the Adeli Suit®, the TheraSuit® and the PediaSuit®. These models have hooks that anchor a system of individually fixed elastic tubes to exert traction between the trunk and the pelvis and between the pelvis and the lower limbs. The action mechanism, proposed to explain the effects provided by these therapeutic suits, is that of continuous compression exerted by the elastic elements of the clothing on the child’s musculoskeletal system [210].
However, the mechanical model of structural stability, based on continuous compressive forces, has limitations in terms of explaining the stability of joints in the human body [211]. Given the limitations of compressive models to explain the inherent stability of the musculoskeletal system, the tensional integrity (tensegrity) model was proposed [211,212,213]. A tensegrity system consists of an intrinsically stable system that contains a group of components in compression, within a network of interconnected components under continuous tension [212]. Applying this model to the musculoskeletal system, the bones represent the discontinuous compressive elements, and the soft tissues—fascia, ligaments, muscles and tendons—form the continuous network of tensional elements in which the bones are intrinsically connected [212,213]. It is believed that the organization of the musculoskeletal system is consistent with that of tensegrity structures, with the pre-stress present in the connective tissues of the musculoskeletal system.
The study of these continuous networks of tensional elements began in the 1940s, with different studies on “muscle chains” [214]. Based on this concept of muscle chains, and from the perspective of the tensegrity model, Myers (2001) and Stecco (2006, 2009) [215,216,217] describe models explaining “trains” that comprise the myofascial connections that cross the entire body. These “trains” are based not only on functional connections (as described by muscle chains), but also on anatomic connections between muscles and fascial tissue. The authors further postulate that these “trains” are involved directly in the organization of movement and in the transmission of muscular force [215,216,217,218,219]. Furthermore, the study on the innervation of fascial tissue also demonstrates its role in proprioception [220].
Fascial tissue can be divided into superficial fascia, visceral fascia and deep fascia, with the latter subdivided into aponeurotic fascia and epimysial fascia [221]. With the development of new studies and methodological advances in research, it has been seen that different fasciae have different types of innervations [220,221,222,223]. The superficial fascia has mechanical and thermal receptors that play an important role in thermoregulation, exteroception and pain perception [222,223]. The two types of deep fascia, aponeurotic and epimysial, have distinct mechanical functions and mechanisms. The aponeurotic fascia surrounds several muscles, holds them in place and connects them. The epimysial fascia is specific to each muscle and is tightly attached to them, defining their shape and volume. Histological studies on the deep fascia (in animals and humans), in turn, show its role in proprioception, with neuromuscular spindles and Golgi tendon organs observed in tissue analyses [220,223]. Furthermore, the connection between the capsule of the neuromuscular spindles and the connective tissue has been verified, which means that the function of the neuromuscular spindles has shown a direct relationship with the quality of the intramuscular and surrounding connective tissue [150]. Thus, changes in myofascial tissue can distort the information sent by the spindles to the central nervous system and, therefore, can interfere with the appropriate regulation of muscle tone and the quality of movements performed.
In addition to being innovative regarding neurodevelopmental disorders, this theoretical foundation is extremely important for the development of interventions and technologies for people with autism. This is because the correct planning and execution of movements require both a correct efferent motor stimulus and good motor control, based on appropriate proprioceptive stimuli. The MIG Flex was developed based on myofascial lines and general geometric patterns, also considering the changes in motor control, feedforward and feedback, as well as muscular hypotonia presented by children with autism [224,225] and the role of the quality of myofascial tissue on feedforward and feedback to the central nervous system, leading to the regulation of muscle tone.
Based on the above, the MIG Flex is based on the dynamic myofascial lines [149] with structural frameworks that simultaneously allow for stabilization, movement and body perception. Myofascial geometry is composed of rails that connect the different layers of connective tissue and muscle fibers of the body, including the fascia, aponeurosis, tendons and muscles. The transmission of tension through the myofascial rails reproduced by the MIG Flex allows for the implementation of more complex motor synergies, integrating different joints and segments of the body in a complex, organized gesture.
MIG Flex is made up of a base suit, two anchors (also called “nodes”) and six viscoelastic straps (or myofascial straps). The base garment is made of polyamide (84%) and elastane (16%) and has adjustment systems with Velcro on the shoulders, chest, abdomen and thigh. In the navel region and lumbosacral region (L5–S1) there are anchors made of nylon that allow for the passage of the viscoelastic strip (represented by the green color in Figure 3). The viscoelastic strip is a non-toxic polymer (silicone) which has connection systems with the clips located on the side of the suit and which has paths similar to the myofascial lines (lateral line, spiral line and anterior and posterior functional lines). Accordingly, MIG Flex is a therapeutic suit made with flexible material which ensures that the child can carry out their activities without any mobility restrictions. MIG Flex is one of the components of the MIG program. Therefore, non-tolerance of the child’s use of clothing does not constitute a contraindication to intervention with the MIG program. The child can benefit from the other components of the program, such as skills training in the different units of the City of Tomorrow. The initial adjustment of MIG Flex to the child’s body is carried out gradually, according to tolerance. Furthermore, if the child demonstrates intolerance to the clothing, not only through oral language, but also through significant changes in behavior, adjustments to MIG Flex can be made gradually, until the child becomes accustomed to the clothing. Figure 3 illustrates MIG Flex.

Figure 3.
Therapeutic suit—MIG Flex.
In addition to the role of fascia in regulating movement, it is also important to highlight the role of interventions that engage both the superficial fascia (through the stimulation of their mechanical receptors) and the deep fascia (through the execution of movements) [223]. Active fascial training aims at elasticity and resilience, which provides effective muscle function with a greater degree of injury prevention [218]. An appropriate exercise load, applied regularly, can also favor a collagen architecture with a more “wavy” or crimped arrangement of fibers [226], resulting in a significant increase in elastic energy storage capacity [227]. Failure to exercise causes a loss of fiber elasticity and reduced slippage between them, forming tissue adhesions and even tangled, poorly organized arrangements [218,226]. This also impacts the quality of proprioceptive information sent to the central nervous system.
Fascial training, through movements in multiple ranges of extension and elasticity, aims to stimulate fibroblasts to maintain the architecture of collagen fibers with the potential for elastic storage [218]. Furthermore, as the fascia is rich in proprioceptive receptors, in the absence of tissue adhesions, the deep fascia is sensitive to both small joint movements and multi-joint movements [218]. It is believed that fascial sensitivity is greater than joint capsule sensitivity, as the receptors in the joint capsules are generally stimulated only in the extreme joint ranges and not during physiological movements, as occurs with fascial proprioceptive receptors [218,219,220].
Thus, in addition to postural stabilization, activities carried out with MIG Flex in a naturalistic space (City of Tomorrow) optimize functional postures as well as active and exploratory movement in the environment with enhanced muscle strength. The stability, postural compensation and active movement with enhanced muscle strength provided by the MIG Flex are provided by distributing stimulation along the functional, superficial, lateral, spiral and deep myofascial lines. The stimulation of these lines, carried out in a naturalistic environment, plays both mechanical and perceptual roles [219,220,221], thus contributing to the motricity and naturalistic environmental exploration carried out in the units that make up the City of Tomorrow. In the long term, the benefits of using the MIG Flex include sending correct proprioceptive information to the central nervous system and favoring the adjustment of muscle tone. Adjusting tone and promoting constant motor control leads to the patient executing correct movements. This correct execution of active movements provides greater quality to the fascial tissue, thus generating a positive cycle in the patient’s motor function.
To estimate the amount of time for the effects of using MIG Flex to result in permanent structural changes in the connective tissue, and, consequently, in the improvement of tissue quality, the period of tissue remodeling of collagen fibers must be considered. Connective tissue adapts to regularly imposed physiological tensions, whereas fibroblasts adjust their tissue matrices by adapting activity to favor demand. Thus, upon tension, fibroblasts adapt the arrangement of the collagen fiber network [228]. It is estimated that half of the collagen fibrils are replaced annually [229]. Extrapolating from these data, in six months, there will be a renewal of 30% of the collagen fibers, and in two years, there will be a renewal of 75% [218]. Therefore, an MIG Flex usage duration equivalent to three years is considered ideal. During this period, the renewal of collagen fibers would be completed, with tissue being adapted and effective in sending accurate proprioceptive information.
8. Intervention Results Assessment Strategy
The MIG approach is currently serving 206 children aged 1.8 years to 18.25 years with autism and their families in interdisciplinary clinics across Brazil. The support levels required by the children are: Level 1: 23.2%; Level 2: 37.4%; and Level 3: 30.5%. A substantial proportion of children present autism associated with genetic syndromes and other neurological conditions, such as cerebral palsy. Care is funded by private health insurance companies in accordance with Brazilian legislation [230]. Similar programs are beginning to be implemented by public health services, albeit in an incipient manner. Children receive physical, occupational and speech therapy in the same institution. Therapeutic goals are defined, and their implementation is collaboratively assessed with the families using the Canadian Occupational Performance Measure (COPM) [231]. The MIG program lasts for at least three years. Children receive 20 weekly hours of care, and parents participate in one weekly session of parent training. Psychological care is available for children and parents as needed. Some families experience such an overwhelming burden that they are unable to participate in the parent training program. In these cases, parents receive other forms of psychotherapy, usually individual. Children use the MIG Flex for 20 h of the week, as they are participating at the clinic. A new model of using the MIG Flex at home coupled with parent training is currently being investigated. The MIG Flex is well-accepted by most children, resulting in improvements in balance, gait, stereotypies and aggressive behaviors.
In the current manuscript, we present the theoretical and methodological foundations of MIG. The next research step is to empirically assess the program’s validity. Table 3 describes the instruments that are being used for the initial assessment as well as for the evaluation of the results. The instruments listed in Table 3 are the main outcome measures. Additional instruments may be necessary, as appropriate in each case.
Table 3.
Assessment instruments.
The validity of the program is currently being assessed through a series of single-subject, quasi-experimental studies using the ABAB design with triplets of participants. The next step is a randomized controlled trial.
9. Strengths and Limitations
The main strength of the present article is the addition of interventions, specifically focusing on motor manifestations in autism, from a predictive coding and embodied cognition perspective. At the same time that it adds specific interventions for motor manifestations, MIG preserves components that have been proven effective in other approaches, especially in naturalistic–developmental–behavioral ones. One limitation of this article is that it is restricted to presenting the theoretical–methodological framework of a new approach. Examination of the validity of this approach is ongoing. Another limitation is that the process of creating MIG was not based on a systematic review of the literature, but rather on the clinical and research expertise accumulated by authors with over 20 years in the rehabilitation of children with neurodevelopmental disorders and neurodevelopment, as well as 40 years in neuropsychological assessment and counseling, respectively.
10. Final Considerations
MIG was created in response to the different needs of people with autism. It consists of an integrated and interdisciplinary program of intervention strategies, considering the greatest possible number of levels of disability and functionality proposed by the WHO biopsychosocial model, as well as their interactions. MIG’s theoretical foundation is based on the analysis of behavior, cognitive neuropsychology and motor function, as well as motor cognition guiding the practice of professionals from different areas of healthcare and education. MIG’s entire theoretical foundation has resulted in the development of exclusive ingredients such as the City of Tomorrow and therapeutic suit MIG Flex. These ingredients favor environmental exploration by people with autism in a structured, naturalistic, active way, and are mediated by the MIG Flex. The support offered by therapeutic suit MIG Flex increases the ability to focus attention and understand what is happening in the environment, especially the social environment, favoring both motor and cognitive aspects related to social skills.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/children11020191/s1.
Author Contributions
Conceptualization, R.G.L., T.K.F.C., G.M.P., D.O.S., S.R.B., P.A.N.S., A.A.A.C.N., F.R.M.C., E.B.C. and V.G.H.; methodology, V.G.H.; writing—original draft preparation, V.G.H. and T.K.F.C.; writing—review and editing, V.G.H., T.K.F.C., S.R.B., G.M.P. and E.B.C.; supervision, V.G.H.; project administration, R.G.L. and V.G.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
Renato Guimarães Loffi is the owner of TREINITEC Ltda. and developed the MIG program. The other authors are consultants and researchers at the company TREINITEC Ltda.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Publishing, Inc.: Arlington VA, USA, 2022. [Google Scholar]
- Hume, K.; Steinbrenner, J.R.; Odom, S.L.; Morin, K.L.; Nowell, S.W.; Tomaszewski, B.; Szendrey, S.; McIntyre, N.S.; Yücesoy-Özkan, S.; Savage, M.N. Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review. J. Autism Dev. Disord. 2021, 51, 4013–4032, Erratum in J. Autism Dev. Disord. 2023, 53, 514. [Google Scholar] [CrossRef]
- Bhat, A.N. Fewer children with autism spectrum disorder with motor challenges receive physical and recreational therapies compared to standard therapies: A SPARK data set analysis. Autism 2023. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.A.L.; Petrulla, V.; Zampella, C.J.; Waller, R.; Schultz, R.T. Gross motor impairment and its relation to social skills in autism spectrum disorder: A systematic review and two meta-analyses. Psychol. Bull. 2022, 148, 273–300. [Google Scholar] [CrossRef] [PubMed]
- Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators; Centers for Disease Control and Prevention (CDC). Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill. Summ. 2014, 63, 1–21. [Google Scholar]
- Rayan, A.; Ahmad, M. Effectiveness of mindfulness-based interventions on quality of life and positive reappraisal coping among parents of children with autism spectrum disorder. Res. Dev. Disabil. 2016, 55, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Odom, S.L.; Hume, K.A.; Cox, A.W.; Fettig, A.; Kucharczyk, S.; Brock, M.E.; Plavnick, J.B.; Fleury, V.P.; Schultz, T.R. Evidence-Based Practices for Children, Youth, and Young Adults with Autism Spectrum Disorder: A Comprehensive Review. J. Autism Dev. Disord. 2015, 45, 1951–1966. [Google Scholar] [CrossRef] [PubMed]
- Bruinsma, Y.E.M.; Minjarez, M.B.; Schreibman, L.; Stahmer, A.C. Naturalistic Developmental Behavioral Interventions for Autism Spectrum Disorder; Brookes Publishing Company: Baltimore, MD, USA, 2020. [Google Scholar]
- Mesibov, G.B.; Shea, V.; Schopler, E. The TEACCH Approach to Autism Spectrum Disorders; Springer Science & Business Media: Berlin, Germany, 2005. [Google Scholar]
- Bhat, A.N. Is Motor Impairment in Autism Spectrum Disorder Distinct from Developmental Coordination Disorder? A Report from the SPARK Study. Phys. Ther. 2020, 100, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Jones, E.J.H.; Jones, R.M.; Pickles, A.; State, M.W.; et al. Autism spectrum disorder. Nat. Rev. Dis. Prim. 2020, 6, 5. [Google Scholar] [CrossRef]
- Russell, G. The Rise of Autism: Risk and Resistance in the Age of Diagnosis; Taylor & Francis: Didcot, UK, 2021; Available online: https://library.oapen.org/ (accessed on 25 November 2023).
- Siegel, B. Helping Children with Autism Learn: Treatment Approaches for Parents and Professionals; Oxford University Press: Oxford, UK, 2003; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=F-mdBwbAHg0C&oi=fnd&pg=PR7&dq=Siegel (accessed on 24 January 2024).
- Siegel, D.B. The Politics of Autism; Oxford University Press: Oxford, UK, 2018; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=iWFmDwAAQBAJ&oi=fnd&pg=PP1&dq=Siegel (accessed on 24 January 2024).
- Vermeulen, P. Autism and The Predictive Brain: Absolute Thinking in a Relative World; Taylor & Francis: Didcot, UK, 2022; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=J5eSEAAAQBAJ&oi=fnd&pg=PT8&dq=Vermeulen (accessed on 24 January 2024).
- Waterhouse, L. Heterogeneity thwarts autism explanatory power: A proposal for endophenotypes. Front. Psychiatry 2022, 13, 947653. [Google Scholar] [CrossRef]
- Salari, N.; Rasoulpoor, S.; Shohaimi, S.; Jafarpour, S.; Abdoli, N.; Khaledi-Paveh, B.; Mohammadi, M. The global prevalence of autism spectrum disorder: A comprehensive systematic review and meta-analysis. Ital. J. Pediatr. 2022, 48, 112. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2020, 69, 1–12, Erratum in MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 503. [Google Scholar] [CrossRef]
- Maenner, M.J.; Warren, Z.; Williams, A.R.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR. Surveill. Summ. 2023, 72, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Shenouda, J.; Barrett, E.; Davidow, A.L.; Sidwell, K.; Lescott, C.; Halperin, W.; Silenzio, V.M.B.; Zahorodny, W. Prevalence and Disparities in the Detection of Autism without Intellectual Disability. Pediatrics 2023, 151, e2022056594. [Google Scholar] [CrossRef] [PubMed]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Crespi, B.J. Autism as a Disorder of High Intelligence. Front. Neurosci. 2016, 10, 300. [Google Scholar] [CrossRef] [PubMed]
- Lundström, S.; Reichenberg, A.; Anckarsäter, H.; Lichtenstein, P.; Gillberg, C. Autism phenotype versus registered diagnosis in Swedish children: Prevalence trends over 10 years in general population samples. BMJ 2015, 350, h1961. [Google Scholar] [CrossRef] [PubMed]
- Polimanti, R.; Gelernter, J. Widespread signatures of positive selection in common risk alleles associated to autism spectrum disorder. PLoS Genet. 2017, 13, e1006618. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Collishaw, S.; Golding, J.; Kelly, S.E.; Ford, T. Changes in diagnosis rates and behavioural traits of autism spectrum disorder over time. BJPsych Open 2015, 1, 110–115. [Google Scholar] [CrossRef]
- Giudice, M.D. Evolutionary Psychopathology: A Unified Approach; Oxford University Press: Oxford, UK, 2018; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=aiRjDwAAQBAJ&oi=fnd&pg=PP1&dq=Del+Giudice (accessed on 24 January 2024).
- Toma, C. Genetic Variation across Phenotypic Severity of Autism. Trends Genet. 2020, 36, 228–231. [Google Scholar] [CrossRef]
- Richards, C.; Jones, C.; Groves, L.; Moss, J.; Oliver, C. Prevalence of autism spectrum disorder phenomenology in genetic disorders: A systematic review and meta-analysis. Lancet Psychiatry 2015, 2, 909–916. [Google Scholar] [CrossRef]
- Carpita, B.; Migli, L.; Chiarantini, I.; Battaglini, S.; Montalbano, C.; Carmassi, C.; Cremone, I.M.; Dell’osso, L. Autism Spectrum Disorder and Fetal Alcohol Spectrum Disorder: A Literature Review. Brain Sci. 2022, 12, 792. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, C.; McCarthy, F.P.; Ryan, R.M.; Khashan, A.S. Maternal Alcohol Consumption During Pregnancy and the Risk of Autism Spectrum Disorders in Offspring: A Retrospective Analysis of the Millennium Cohort Study. J. Autism Dev. Disord. 2018, 48, 3773–3782. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Rehm, J.; Anagnostou, E.; Popova, S. Prevalence of externalizing disorders and Autism Spectrum Disorders among children with Fetal Alcohol Spectrum Disorder: Systematic review and meta-analysis. Biochem. Cell Biol. 2018, 96, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Ornoy, A.; Weinstein-Fudim, L.; Ergaz, Z. Prenatal factors associated with autism spectrum disorder (ASD). Reprod. Toxicol. 2015, 56, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Singer, A.B.; Aylsworth, A.S.; Cordero, C.; Croen, L.A.; DiGuiseppi, C.; Fallin, M.D.; Herring, A.H.; Hooper, S.R.; Pretzel, R.E.; Schieve, L.A.; et al. Prenatal Alcohol Exposure in Relation to Autism Spectrum Disorder: Findings from the Study to Explore Early Development (SEED). Paediatr. Périnat. Epidemiol. 2017, 31, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Auyeung, B.; Baron-Cohen, S. Hormonal Influences in Typical Development: Implications for Autism. In Chapter the Neuroscience of Autism Spectrum Disorders; Buxbaum, J.D., Hof, P.R., Eds.; Academic Press: Oxford, UK, 2013; pp. 215–232. [Google Scholar]
- Auyeung, B.; Ashwin, E.; Knickmeyer, R.; Taylor, K.; Hackett, G.; Baron-Cohen, S. Fetal testosterone and autistic traits. Br. J. Psychol. 2009, 100, 1–22. [Google Scholar] [CrossRef]
- Cesta, C.E.; Månsson, M.; Palm, C.; Lichtenstein, P.; Iliadou, A.N.; Landén, M. Polycystic ovary syndrome and psychiatric disorders: Co-morbidity and heritability in a nationwide Swedish cohort. Psychoneuroendocrinology 2016, 73, 196–203. [Google Scholar] [CrossRef]
- Knickmeyer, R.; Baron-Cohen, S.; Fane, B.A.; Wheelwright, S.; Mathews, G.A.; Conway, G.S.; Brook, C.G.; Hines, M. Androgens and autistic traits: A study of individuals with congenital adrenal hyperplasia. Horm. Behav. 2006, 50, 148–153. [Google Scholar] [CrossRef]
- Kosidou, K.; Dalman, C.; Widman, L.; Arver, S.; Lee, B.K.; Magnusson, C.; Gardner, R.M. Maternal polycystic ovary syndrome and the risk of autism spectrum disorders in the offspring: A population-based nationwide study in Sweden. Mol. Psychiatry 2015, 21, 1441–1448. [Google Scholar] [CrossRef]
- Lilienfeld, S.O.; Marino, L. Mental disorder as a Roschian concept: A critique of Wakefield’s “harmful dysfunction” analysis. J. Abnorm. Psychol. 1995, 104, 411–420. [Google Scholar] [CrossRef]
- Wakefield, J.C. The concept of mental disorder: On the boundary between biological facts and social values. Am. Psychol. 1992, 47, 373–388. [Google Scholar] [CrossRef]
- Wakefield, J.C. The concept of mental disorder: Diagnostic implications of the harmful dysfunction analysis. World Psychiatry 2007, 6, 149–156. [Google Scholar]
- Crespi, B.J. The hallmarks of autism. Front. Psychiatry 2022, 13, 937163. [Google Scholar] [CrossRef]
- Bölte, S.; Mahdi, S.; De Vries, P.J.; Granlund, M.; Robison, J.E.; Shulman, C.; Swedo, S.; Tonge, B.; Wong, V.; Zwaigenbaum, L.; et al. The Gestalt of functioning in autism spectrum disorder: Results of the international conference to develop final consensus International Classification of Functioning, Disability and Health core sets. Autism 2019, 23, 449–467. [Google Scholar] [CrossRef] [PubMed]
- Schiariti, V.; Mahdi, S.; Bölte, S. International Classification of Functioning, Disability and Health Core Sets for cerebral palsy, autism spectrum disorder, and attention-deficit-hyperactivity disorder. Dev. Med. Child Neurol. 2018, 60, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.B.; Filipini, R.; Monteiro, C.B.d.M.E.; Valenti, V.; de Carvalho, S.M.F.; Wajnsztejn, R.; de Farias, M.D.C.A.D.; Macedo, C.C.; de Abreu, L.C. The biopsychosocial processes in autism spectrum disorder. Int. Arch. Med. 2013, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=SWFQDXyU-rcC&oi=fnd&pg=PR8&dq=+International+Classification+of+Functioning (accessed on 24 January 2024).
- Fombonne, E.; MacFarlane, H.; Salem, A.C.; Zuckerman, K.E. Epidemiological Surveys of ASD: Current Findings and New Directions. Autism and child psychopathology series. In Handbook of Autism and Pervasive Developmental Disorder: Assessment, Diagnosis, and Treatment; Springer International Publishing: Cham, Switzerland, 2022; pp. 135–184. [Google Scholar]
- Katusic, M.Z.; Myers, S.M.; Weaver, A.L.; Voigt, R.G. IQ in Autism Spectrum Disorder: A Population-Based Birth Cohort Study. Pediatrics 2021, 148, e2020049899. [Google Scholar] [CrossRef] [PubMed]
- Hassiotis, A.; Emerson, E.; Wieland, J.; Bertelli, M.O. Borderline Intellectual Functioning. In Textbook of Psychiatry for Intellectual Disability and Autism Spectrum Disorder; Springer International Publishing: Cham, Switzerland, 2022; pp. 95–106. [Google Scholar]
- Loucas, T.; Charman, T.; Pickles, A.; Simonoff, E.; Chandler, S.; Meldrum, D.; Baird, G. Autistic symptomatology and language ability in autism spectrum disorder and specific language impairment. J. Child Psychol. Psychiatry 2008, 49, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, J.; El-Raziq, M.A.; Castroviejo, E.; Durrleman, S.; Ferré, S.; Grama, I.; Hendriks, P.; Kissine, M.; Manenti, M.; Marinis, T.; et al. Language in autism: Domains, profiles and co-occurring conditions. J. Neural Transm. 2023, 130, 433–457. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.M.; Shaw, K.A.; DiRienzo, M.; Durkin, M.S.; Esler, A.; Hall-Lande, J.; Wiggins, L.; Zahorodny, W.; Singer, A.; Maenner, M.J. The Prevalence and Characteristics of Children with Profound Autism, 15 Sites, United States, 2000–2016. Public Heath Rep. 2023, 138, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Posar, A.; Visconti, P. Update about “minimally verbal” children with autism spectrum disorder. Rev. Paul. Pediatr. 2022, 40, e2020158. [Google Scholar] [CrossRef] [PubMed]
- Bullen, J.C.; Zajic, M.C.; McIntyre, N.; Solari, E.; Mundy, P. Patterns of math and reading achievement in children and adolescents with autism spectrum disorder. Res. Autism Spectr. Disord. 2022, 92, 101933. [Google Scholar] [CrossRef]
- Chen, L.; Abrams, D.A.; Rosenberg-Lee, M.; Iuculano, T.; Wakeman, H.N.; Prathap, S.; Chen, T.; Menon, V. Quantitative Analysis of Heterogeneity in Academic Achievement of Children with Autism. Clin. Psychol. Sci. 2018, 7, 362–380. [Google Scholar] [CrossRef] [PubMed]
- Oswald, T.M.; Beck, J.S.; Iosif, A.; McCauley, J.B.; Gilhooly, L.J.; Matter, J.C.; Solomon, M. Clinical and Cognitive Characteristics Associated with Mathematics Problem Solving in Adolescents with Autism Spectrum Disorder. Autism Res. 2015, 9, 480–490. [Google Scholar] [CrossRef] [PubMed]
- Atun-Einy, O.; Lotan, M.; Harel, Y.; Shavit, E.; Burstein, S.; Kempner, G. Physical Therapy for Young Children Diagnosed with Autism Spectrum Disorders–Clinical Frameworks Model in an Israeli Setting. Front. Pediatr. 2013, 1, 19. [Google Scholar] [CrossRef] [PubMed]
- Casartelli, L.; Molteni, M.; Ronconi, L. So close yet so far: Motor anomalies impacting on social functioning in autism spectrum disorder. Neurosci. Biobehav. Rev. 2016, 63, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Cook, J. From movement kinematics to social cognition: The case of autism. Philos. Trans. R. Soc. B Biol. Sci. 2016, 371, 20150372. [Google Scholar] [CrossRef]
- Ohara, R.; Kanejima, Y.; Kitamura, M.; Izawa, P.K. Association between Social Skills and Motor Skills in Individuals with Autism Spectrum Disorder: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2019, 10, 276–296. [Google Scholar] [CrossRef]
- Ming, X.; Brimacombe, M.; Wagner, G.C. Prevalence of motor impairment in autism spectrum disorders. Brain Dev. 2007, 29, 565–570. [Google Scholar] [CrossRef]
- Casartelli, L.; Federici, A.; Biffi, E.; Molteni, M.; Ronconi, L. Are We “Motorically” Wired to Others? High-Level Motor Computations and Their Role in Autism. Neuroscientist 2018, 24, 568–581. [Google Scholar] [CrossRef]
- Casartelli, L.; Chiamulera, C. The motor way: Clinical implications of understanding and shaping actions with the motor system in autism and drug addiction. Cogn. Affect. Behav. Neurosci. 2016, 16, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, M.W.; Sweeney, J.A. Sensorimotor dysfunctions as primary features of autism spectrum disorders. Sci. China Life Sci. 2015, 58, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Courchesne, E.; Pramparo, T.; Gazestani, V.H.; Lombardo, M.V.; Pierce, K.; Lewis, N.E. The ASD Living Biology: From cell proliferation to clinical phenotype. Mol. Psychiatry 2019, 24, 88–107. [Google Scholar] [CrossRef] [PubMed]
- Hazlett, H.C.; Gu, H.; Munsell, B.C.; Kim, S.H.; Styner, M.; Wolff, J.J.; Elison, J.T.; Swanson, M.R.; Zhu, H.; Botteron, K.N.; et al. Early brain development in infants at high risk for autism spectrum disorder. Nature 2017, 542, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.D.; Piven, J. Brain and behavior development in autism from birth through infancy. Dialog. Clin. Neurosci. 2017, 19, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Vivanti, G.; Nuske, H.J. Autism, attachment, and social learning: Three challenges and a way forward. Behav. Brain Res. 2017, 325, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Grzadzinski, R.; Lord, C.; Sanders, S.J.; Werling, D.; Bal, V.H. Children with autism spectrum disorder who improve with fever: Insights from the Simons Simplex Collection. Autism Res. 2018, 11, 175–184. [Google Scholar] [CrossRef]
- Vivanti, G.; Rogers, S.J.; Dwyer, P.; Rivera, S. Early Learning in Autism; Springer: Berlin/Heidelberg, Germany, 2016; pp. 1–12. [Google Scholar]
- Anderson, D.K.; Liang, J.W.; Lord, C. Predicting young adult outcome among more and less cognitively able individuals with autism spectrum disorders. J. Child Psychol. Psychiatry 2014, 55, 485–494. [Google Scholar] [CrossRef]
- Jones, R.M.; Pickles, A.; Lord, C. Evaluating the quality of peer interactions in children and adolescents with autism with the Penn Interactive Peer Play Scale (PIPPS). Mol. Autism 2017, 8, 28. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; DiLavore, P.S.; Shulman, C.; Thurm, A.; Pickles, A. Autism from 2 to 9 years of age. Arch. Gen. Psychiatry 2006, 63, 694–701. [Google Scholar] [CrossRef]
- Kanne, S.M.; Gerber, A.J.; Quirmbach, L.M.; Sparrow, S.S.; Cicchetti, D.V.; Saulnier, C.A. The Role of Adaptive Behavior in Autism Spectrum Disorders: Implications for Functional Outcome. J. Autism Dev. Disord. 2011, 41, 1007–1018. [Google Scholar] [CrossRef]
- Klin, A.; Saulnier, C.A.; Sparrow, S.S.; Cicchetti, D.V.; Volkmar, F.R.; Lord, C. Social and Communication Abilities and Disabilities in Higher Functioning Individuals with Autism Spectrum Disorders: The Vineland and the ADOS. J. Autism Dev. Disord. 2006, 37, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.; Flanagan, H.E.; Geier, J.D.; Freeman, N.L. Brief Report: The Vineland Adaptive Behavior Scales in Young Children with Autism Spectrum Disorders at Different Cognitive Levels. J. Autism Dev. Disord. 2009, 39, 1066–1078. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, J.L.; Gates, J.A.; Lerner, M.D. Friendship in school-age boys with autism spectrum disorders: A meta-analytic summary and developmental, process-based model. Psychol. Bull. 2016, 142, 601–622. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.M.; Shattuck, P.T.; Rast, J.E.; Rava, J.A.; Anderson, K. National Autism Indicators Report: Transition into Young Adulthood; Life Course Outcomes Research Program; A.J. Drexel Autism Institute, Drexel University: Philadelphia, PA, USA, 2015. [Google Scholar]
- Petrina, N.; Carter, M.; Stephenson, J. The nature of friendship in children with autism spectrum disorders: A systematic review. Res. Autism Spectr. Disord. 2014, 8, 111–126. [Google Scholar] [CrossRef]
- Płatos, M.; Pisula, E. Friendship understanding in males and females on the autism spectrum and their typically developing peers. Res. Autism Spectr. Disord. 2021, 81, 101716. [Google Scholar] [CrossRef]
- Pecora, L.A.; Hancock, G.I.; Hooley, M.; Demmer, D.H.; Attwood, T.; Mesibov, G.B.; Stokes, M.A. Gender identity, sexual orientation and adverse sexual experiences in autistic females. Mol. Autism 2020, 11, 57. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.M.; Rast, J.E.; Anderson, K.A.; Shattuck, P.T. National Autism Indicators Report: Developmental Disability Services and Outcomes in Adulthood; Life Course Outcomes Program; A.J. Drexel Autism Institute, Drexel University: Philadelphia, PA, USA, 2017. [Google Scholar]
- Rast, J.E.; Roux, A.M.; Anderson, K.A.; Croen, L.A.; Kuo, A.A.; Shea, L.L.; Shattuck, P.T. National Autism Indicators Report: Health and Health Care; Life Course Outcomes Program; A.J. Drexel Autism Institute, Drexel University: Philadelphia, PA, USA, 2020. [Google Scholar]
- Bitsika, V.; Sharpley, C.F. Stress, Anxiety and Depression Among Parents of Children with Autism Spectrum Disorder. Aust. J. Guid. Couns. 2004, 14, 151–161. [Google Scholar] [CrossRef]
- Bouma, R.; Schweitzer, R. The impact of chronic childhood illness on family stress: A comparison between autism and cystic fibrosis. J. Clin. Psychol. 1990, 46, 722–730. [Google Scholar] [CrossRef]
- Donenberg, G.; Baker, B.L. The impact of young children with externalizing behaviors on their families. J. Abnorm. Child Psychol. 1993, 21, 179–198. [Google Scholar] [CrossRef]
- Gray, D.E.; Holden, W.J. Psycho-social well-being among the parents of children with autism. Aust. N. Z. J. Dev. Disabil. 1992, 18, 83–93. [Google Scholar] [CrossRef]
- Gurney, J.G.; McPheeters, M.L.; Davis, M.M. Parental Report of Health Conditions and Health Care Use Among Children with and without Autism. Arch. Pediatr. Adolesc. Med. 2006, 160, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Kogan, M.D.; Strickland, B.B.; Blumberg, S.J.; Singh, G.K.; Perrin, J.M.; van Dyck, P.C. A National Profile of the Health Care Experiences and Family Impact of Autism Spectrum Disorder Among Children in the United States, 2005–2006. Pediatrics 2008, 122, e1149–e1158. [Google Scholar] [CrossRef]
- Liptak, G.S.; Stuart, T.; Auinger, P. Health Care Utilization and Expenditures for Children with Autism: Data from U.S. National Samples. J. Autism Dev. Disord. 2006, 36, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Schieve, L.A.; Boulet, S.L.; Kogan, M.D.; Yeargin-Allsopp, M.; Boyle, C.A.; Visser, S.N.; Blumberg, S.J.; Rice, C. Parenting aggravation and autism spectrum disorders: 2007 National Survey of Children’s Health. Disabil. Health J. 2011, 4, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Valicenti-McDermott, M.; Lawson, K.; Hottinger, K.; Seijo, R.; Schechtman, M.; Shulman, L.; Shinnar, S. Parental Stress in Families of Children with Autism and Other Developmental Disabilities. J. Child Neurol. 2015, 30, 1728–1735. [Google Scholar] [CrossRef] [PubMed]
- Hartley, S.L.; Barker, E.T.; Seltzer, M.M.; Floyd, F.; Greenberg, J.; Orsmond, G.; Bolt, D. The relative risk and timing of divorce in families of children with an autism spectrum disorder. J. Fam. Psychol. 2010, 24, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Musetti, A.; Manari, T.; Dioni, B.; Raffin, C.; Bravo, G.; Mariani, R.; Esposito, G.; Dimitriou, D.; Plazzi, G.; Franceschini, C.; et al. Parental Quality of Life and Involvement in Intervention for Children or Adolescents with Autism Spectrum Disorders: A Systematic Review. J. Pers. Med. 2021, 11, 894. [Google Scholar] [CrossRef] [PubMed]
- Vasilopoulou, E.; Nisbet, J. The quality of life of parents of children with autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2016, 23, 36–49. [Google Scholar] [CrossRef]
- Vohra, R.; Madhavan, S.; Sambamoorthi, U.; Peter, C.S. Access to services, quality of care, and family impact for children with autism, other developmental disabilities, and other mental health conditions. Autism 2014, 18, 815–826. [Google Scholar] [CrossRef]
- Enea, V.; Rusu, D.M. Raising a Child with Autism Spectrum Disorder: A Systematic Review of the Literature Investigating Parenting Stress. J. Ment. Health Res. Intellect. Disabil. 2020, 13, 283–321. [Google Scholar] [CrossRef]
- Gomes, P.T.; Lima, L.H.; Bueno, M.K.; Araújo, L.A.; Souza, N.M. Autism in Brazil: A systematic review of family challenges and coping strategies. J. Pediatr. 2015, 91, 111–121. [Google Scholar] [CrossRef]
- Schnabel, A.; Youssef, G.J.; Hallford, D.J.; Hartley, E.J.; McGillivray, J.A.; Stewart, M.; Forbes, D.; Austin, D.W. Psychopathology in parents of children with autism spectrum disorder: A systematic review and meta-analysis of prevalence. Autism 2020, 24, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Glidden, D.; Bouman, W.P.; Jones, B.A.; Arcelus, J. Gender Dysphoria and Autism Spectrum Disorder: A Systematic Review of the Literature. Sex. Med. Rev. 2016, 4, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Kallitsounaki, A.; Williams, D.M. Autism Spectrum Disorder and Gender Dysphoria/Incongruence. A systematic Literature Review and Meta-Analysis. J. Autism Dev. Disord. 2023, 53, 3103–3117. [Google Scholar] [CrossRef] [PubMed]
- Koller, J.; David, T.; Bar, N.; Lebowitz, E.R. The Role of Family Accommodation of RRBs in Disruptive Behavior Among Children with Autism. J. Autism Dev. Disord. 2022, 52, 2505–2511. [Google Scholar] [CrossRef] [PubMed]
- Buescher, A.V.S.; Cidav, Z.; Knapp, M.; Mandell, D.S. Costs of Autism Spectrum Disorders in the United Kingdom and the United States. JAMA Pediatr. 2014, 168, 721–728. [Google Scholar] [CrossRef]
- Croteau, C.; Mottron, L.; Dorais, M.; Tarride, J.-E.; Perreault, S. Use, costs, and predictors of psychiatric healthcare services following an autism spectrum diagnosis: Population-based cohort study. Autism 2019, 23, 2020–2030. [Google Scholar] [CrossRef]
- Bowman, K.S.; Suarez, V.D.; Weiss, M.J. Standards for Interprofessional Collaboration in the Treatment of Individuals with Autism. Behav. Anal. Pract. 2021, 14, 1191–1208. [Google Scholar] [CrossRef]
- Lustrea, A. Case management in autism spectrum disorders. In Perspective on Autistic Specturm Disorders; Al Ghazi, L., Zappaterra, T.T., Eds.; Edizioni ETS: Pisa, Italy, 2019; pp. 43–57. [Google Scholar]
- Zuckerman, K.E.; Lindly, O.J.; Bethell, C.D.; Kuhlthau, K. Family Impacts Among Children with Autism Spectrum Disorder: The Role of Health Care Quality. Acad. Pediatr. 2014, 14, 398–407. [Google Scholar] [CrossRef]
- Lawrence, C. Autism and Flexischooling A Shared Classroom and Homeschooling Approach; Jessica Kingsley: London, UK, 2012. [Google Scholar]
- Vivanti, G.; Bent, C.; Capes, K.; Upson, S.; Hudry, K.; Dissanayake, C. The Victorian ASELCC Team Characteristics of children on the autism spectrum who benefit the most from receiving intervention in inclusive versus specialised early childhood education settings. Autism Res. 2022, 15, 2200–2209. [Google Scholar] [CrossRef]
- Tobin, M.C.; Drager, K.D.; Richardson, L.F. A systematic review of social participation for adults with autism spectrum disorders: Support, social functioning, and quality of life. Res. Autism Spectr. Disord. 2014, 8, 214–229. [Google Scholar] [CrossRef]
- Sáez-Suanes, G.P.; Álvarez-Couto, M. Factors Associated with Quality of Life in Adults with Autism Spectrum Disorder: A Systematic Review. Rev. J. Autism Dev. Disord. 2021, 9, 1–13. [Google Scholar] [CrossRef]
- Cybulski, L.; Ashcroft, D.M.; Carr, M.J.; Garg, S.; Chew-Graham, C.A.; Kapur, N.; Webb, R.T. Risk factors for nonfatal self-harm and suicide among adolescents: Two nested case–control studies conducted in the UK Clinical Practice Research Datalink. J. Child Psychol. Psychiatry 2022, 63, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Hedley, D.; Uljarević, M. Systematic Review of Suicide in Autism Spectrum Disorder: Current Trends and Implications. Curr. Dev. Disord. Rep. 2018, 5, 65–76. [Google Scholar] [CrossRef]
- da Silva, J.H.; Hayashi, M.C.P.I. Estudo bibliométrico da produção científica sobre a associação de pais e amigos dos excepcionais. Rev. Educ. Espec. 2018, 31, 65. [Google Scholar] [CrossRef][Green Version]
- Mottron, L.; Bzdok, D. Autism spectrum heterogeneity: Fact or artifact? Mol. Psychiatry 2020, 25, 3178–3185. [Google Scholar] [CrossRef] [PubMed]
- Charman, T.; Pickles, A.; Simonoff, E.; Chandler, S.; Loucas, T.; Baird, G. IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychol. Med. 2011, 41, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Russell, G.; Mandy, W.; Elliott, D.; White, R.; Pittwood, T.; Ford, T. Selection bias on intellectual ability in autism research: A cross-sectional review and meta-analysis. Mol. Autism 2019, 10, 1–10. [Google Scholar] [CrossRef]
- Lovaas, O.I. The development of a treatment-research project for developmentally disabled and autistic children. J. Appl. Behav. Anal. 1993, 26, 617–630. [Google Scholar] [CrossRef]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, Controlled Trial of an Intervention for Toddlers with Autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef]
- Waddington, H.; Reynolds, J.E.; Macaskill, E.; Curtis, S.; Taylor, L.J.; Whitehouse, A.J. The effects of JASPER intervention for children with autism spectrum disorder: A systematic review. Autism 2021, 25, 2370–2385. [Google Scholar] [CrossRef]
- Pierce, K.; Schreibman, L. Increasing complex social behaviors in children with autism: Effects of peer-implemented pivotal response training. J. Appl. Behav. Anal. 1995, 28, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Odom, S.L.; Boyd, B.A.; Hall, L.J.; Hume, K. Evaluation of Comprehensive Treatment Models for Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2010, 40, 425–436, Erratum in J. Autism Dev. Disord. 2010, 40, 437. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B.; Wainer, A. Initial Efficacy of Project ImPACT: A Parent-Mediated Social Communication Intervention for Young Children with ASD. J. Autism Dev. Disord. 2013, 43, 2943–2952. [Google Scholar] [CrossRef] [PubMed]
- Estes, A.; Munson, J.; Rogers, S.J.; Greenson, J.; Winter, J.; Dawson, G. Long-Term Outcomes of Early Intervention in 6-Year-Old Children with Autism Spectrum Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 580–587. [Google Scholar] [CrossRef]
- Acar, S.; Chen, C.-I.; Xie, H. Parental involvement in developmental disabilities across three cultures: A systematic review. Res. Dev. Disabil. 2021, 110, 103861. [Google Scholar] [CrossRef] [PubMed]
- Movahedazarhouligh, S. Parent-implemented interventions and family-centered service delivery approaches in early intervention and early childhood special education. Early Child Dev. Care 2019, 191, 1–12. [Google Scholar] [CrossRef]
- Almasri, N.A.; An, M.; Palisano, R.J. Parents’ Perception of Receiving Family-Centered Care for Their Children with Physical Disabilities: A Meta-Analysis. Phys. Occup. Ther. Pediatr. 2018, 38, 427–443. [Google Scholar] [CrossRef] [PubMed]
- An, M.; Palisano, R.J.; Yi, C.-H.; Chiarello, L.A.; Dunst, C.J.; Gracely, E.J. Effects of a Collaborative Intervention Process on Parent Empowerment and Child Performance: A Randomized Controlled Trial. Phys. Occup. Ther. Pediatr. 2019, 39, 1–15. [Google Scholar] [CrossRef]
- An, M.; Palisano, R.J.; Yi, C.-H.; Chiarello, L.A.; Dunst, C.J.; Gracely, E.J. Effects of a Collaborative Intervention Process on Parent–Therapist Interaction: A Randomized Controlled Trial. Phys. Occup. Ther. Pediatr. 2019, 39, 259–275. [Google Scholar] [CrossRef] [PubMed]
- Borji, R.; Laatar, R.; Zarrouk, N.; Sahli, S.; Rebai, H. Cognitive-motor interference during standing stance across different postural and cognitive tasks in individuals with Down syndrome. Res. Dev. Disabil. 2023, 139, 104562. [Google Scholar] [CrossRef] [PubMed]
- Jabouille, F.; Billot, M.; Hermand, E.; Lemonnier, E.; Perrochon, A. Balance rehabilitation for postural control in children with Autism Spectrum Disorder: A two-case report study. Physiother. Theory Pract. 2023, 39, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Leone, C.; Feys, P.; Moumdjian, L.; D’amico, E.; Zappia, M.; Patti, F. Cognitive-motor dual-task interference: A systematic review of neural correlates. Neurosci. Biobehav. Rev. 2017, 75, 348–360. [Google Scholar] [CrossRef] [PubMed]
- Reilly, D.S.; Woollacott, M.H.; van Donkelaar, P.; Saavedra, S. The Interaction Between Executive Attention and Postural Control in Dual-Task Conditions: Children with Cerebral Palsy. Arch. Phys. Med. Rehabil. 2008, 89, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Simmons, T.L.; Snider, J.; Amit, M.; Ng, T.N.; Townsend, J.; Chukoskie, L. An Objective System for Quantifying the Effect of Cognitive Load on Movement in Individuals with Autism Spectrum Disorder. In Proceedings of the 2019 9th International IEEE/EMBS Conference on Neural Engineering (NER), San Francisco, CA, USA, 20–23 March 2019; pp. 1042–1045. [Google Scholar]
- Torres, E.B.; Denisova, K. Motor noise is rich signal in autism research and pharmacological treatments. Sci. Rep. 2016, 6, 37422. [Google Scholar] [CrossRef] [PubMed]
- Van Biesen, D.; Jacobs, L.; McCulloch, K.; Janssens, L.; Vanlandewijck, Y.C. Cognitive-motor dual-task ability of athletes with and without intellectual impairment. J. Sports Sci. 2018, 36, 513–521. [Google Scholar] [CrossRef]
- Wolpert, D.M.; Doya, K.; Kawato, M. A unifying computational framework for motor control and social interaction. Philos. Trans. R. Soc. B Biol. Sci. 2003, 358, 593–602. [Google Scholar] [CrossRef]
- Ahar, S.; Ghadiri, F. The Effect of Motor Imagery Training on Motor Proficiency of Children with Autism Spectrum Disorder: A Clinical Trial Study. J. Rafsanjan Univ. Med. Sci. 2021, 20, 801–816. [Google Scholar] [CrossRef]
- Kalyuga, S. Schema acquisition and sources of cognitive load. In Cognitive Load Theory; Cambridge University Press: Cambridge, UK, 2010; pp. 48–64. [Google Scholar]
- Sweller, J.; Ayres, P.; Kalyuga, S. Cognitive Load Theory; Springer: New York, NY, USA, 2011. [Google Scholar]
- Bleyenheuft, Y.; Ebner-Karestinos, D.; Surana, B.; Paradis, J.; Sidiropoulos, A.; Renders, A.; Friel, K.M.; Brandao, M.; Rameckers, E.; Gordon, A.M. Intensive upper- and lower-extremity training for children with bilateral cerebral palsy: A quasi-randomized trial. Dev. Med. Child Neurol. 2017, 59, 625–633. [Google Scholar] [CrossRef]
- Figueiredo, P.R.P.; Mancini, M.C.; Feitosa, A.M.; Teixeira, C.M.M.F.; Guerzoni, V.P.D.; Elvrum, A.G.; Ferre, C.L.; Gordon, A.M.; Brandão, M.B. Hand–arm bimanual intensive therapy and daily functioning of children with bilateral cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2020, 62, 1274–1282. [Google Scholar] [CrossRef]
- Hodgson, R.; Biswas, M.; Palmer, S.; Marshall, D.; Rodgers, M.; Stewart, L.; Simmonds, M.; Rai, D.; Le Couteur, A. Intensive behavioural interventions based on applied behaviour analysis (ABA) for young children with autism: A cost-effectiveness analysis. PLoS ONE 2022, 17, e0270833. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child Neurol. 2021, 64, 536–549. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, F.; Feldman, I.; Lavelle, T.A.; Skokauskas, N. The cost-effectiveness of treatments for attention deficit-hyperactivity disorder and autism spectrum disorder in children and adolescents: A systematic review. Eur. Child Adolesc. Psychiatry 2022, 31, 1655–1670. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B.; Dvortcsak, A. Teaching Social Communication to Children with Autism and Other Developmental Delays (2-Book Set): The Project ImPACT Guide to Coaching Parents and The Project ImPACT Manual for Parents, 2nd ed.; Guilford Press: New York, NY, USA, 2019. [Google Scholar]
- Fenning, R.M.; Butter, E.M.; Macklin, E.A.; Norris, M.; Hammersmith, K.J.; McKinnon-Bermingham, K.; Chan, J.; Stephenson, K.G.; Albright, C.; Scherr, J.; et al. Parent Training for Dental Care in Underserved Children with Autism: A Randomized Controlled Trial. Pediatrics 2022, 149, e2021050691. [Google Scholar] [CrossRef]
- Kazdin, A.E. Behavior Modification in Applied Settings, 7th ed.; Waveland Press: Long Grove, IL, USA, 2012; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=6dEYAAAAQBAJ&oi=fnd&pg=PR1&dq=Behavior+modification+in+applied+setting+&ots=5J8UT4s2u7&sig=jLJjKcduyEaHBnm8D8v_da-hMJg#v=onepage&q=Behavior%20modification%20in%20applied%20setting&f=false (accessed on 24 January 2024).
- Loffi, R.G. Exoesqueleto Flexível Baseado nas Linhas Miofasciais e Padrões Geométricos Gerais. Depositante: TREINI Biotecnologia LTDA. Patente brasileira nº BR102018009935-3 A2, 2019. [Google Scholar]
- Stecco, A.; Giordani, F.; Fede, C.; Pirri, C.; De Caro, R.; Stecco, C. From Muscle to the Myofascial Unit: Current Evidence and Future Perspectives. Int. J. Mol. Sci. 2023, 24, 4527. [Google Scholar] [CrossRef] [PubMed]
- Hadad, B.-S.; Schwartz, S. Perception in autism does not adhere to Weber’s law. eLife 2019, 8, e42223. [Google Scholar] [CrossRef] [PubMed]
- Williams, Z.J.; He, J.L.; Cascio, C.J.; Woynaroski, T.G. A review of decreased sound tolerance in autism: Definitions, phenomenology, and potential mechanisms. Neurosci. Biobehav. Rev. 2021, 121, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Damiano, D.L.; Forssberg, H. International initiatives to improve the lives of children with developmental disabilities. Dev. Med. Child Neurol. 2019, 61, 1121. [Google Scholar] [CrossRef]
- Fivush, R. The Development of Autobiographical Memory. Annu. Rev. Psychol. 2011, 62, 559–582. [Google Scholar] [CrossRef]
- Nelson, K.; Fivush, R. The Emergence of Autobiographical Memory: A Social Cultural Developmental Theory. Psychol. Rev. 2004, 111, 486–511. [Google Scholar] [CrossRef]
- Kendall, P.C.; Braswell, L. Cognitive-Behavioral Therapy for Impulsive Children; Guilford Press: New York, NY, USA, 1993; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=McRPHK-c7CoC&oi=fnd&pg=PA11&dq=+Cognitive-behavioral+therapy+for+impulsive+children.+Guilford+Press.&ots=2_0Ln5awcg&sig=gsRsCSrw-lCQEeYzGtb7_eIkE5Q#v=onepage&q=Cognitive-behavioral%20therapy%20for%20impulsive%20children.%20Guilford%20Press.&f=false (accessed on 24 January 2024).
- Nezu, A.M.; Nezu, C. Entrenamiento en solución de problemas. In Manual de Técnicas de Terapia y Modificación de Conducta; Caballo, V.E., Ed.; Siglo Veintinuno: Madrid, Spain, 2020; pp. 527–554. [Google Scholar]
- Santacreu, J. El entrenamiento en autoinstrucciones. In Manual de Técnicas de Terapia y Modificación de Conducta; Caballo, V.E., Ed.; Siglo Veintinuno: Madrid, Spain, 2020; pp. 607–626. [Google Scholar]
- Crick, N.R.; Dodge, K.A. A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychol. Bull. 1994, 151, 74. [Google Scholar] [CrossRef]
- Dodge, K.A. Social-Cognitive Mechanisms in the Development of Conduct Disorder and Depression. Annu. Rev. Psychol. 1993, 44, 559–584. [Google Scholar] [CrossRef] [PubMed]
- Fritz, A.; Ehlert, A.; Balzer, L. Development of mathematical concepts as basis for an elaborated mathematical understanding. S. Afr. J. Child. Educ. 2013, 3, 38–67. [Google Scholar]
- Freitas, F.R.; Herzog, M.; Haase, V.G.; Fritz, A. Compreensão conceitual do número no diagnóstico e intervenção para as dificuldades de aprendizagem na aritmética. In Diferenças Individuais, Família, Currículo e Intervenções; Chapter Pedagogia do Sucesso; Ampla: Belo Horizonte, Brazil, 2022. [Google Scholar]
- Ziv, Y.; Hadad, B.S.; Khateeb, Y. Social Information Processing in Preschool Children Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2013, 44, 846–859. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A.W.; Franklin, S.; Crerar, A. Neuropsychology and the remediation of disorders of spoken language. Hove (UK): Erl-baumn. In Cognitive Neuropsychology and Cognitive Rehabilitation; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 1994; pp. 287–315. [Google Scholar]
- Friedmann, N.; Coltheart, M. Types of Development Dyslexia; Bar-On, A., Ravid, D., Dattner, E., Eds.; Macquarie University: Berlin, Germany; De Gruyter: Boston, MA, USA, 2018; pp. 721–752. Available online: https://researchers.mq.edu.au/en/publications/types-of-development-dyslexia (accessed on 24 January 2024).
- Moura, R.; Haase, V.G.; Lopes-Silva, J.B.; Batista, L.T.; de Freitas, F.R.; Bahnmuller, J.; Moeller, K. Reading and Writing Words and Numbers: Similarities, Differences, and Implications. Loughborough University. 2021. Available online: https://www.degruyter.com/document/doi/10.1515/9783110661941-015/html (accessed on 24 January 2024).
- Temple, C. Developmental Cognitive Neuropsychology; Psychology Press: Hove, UK, 1997. [Google Scholar]
- Dawes, E.; Leitão, S.; Claessen, M.; Kane, R. A randomized controlled trial of an oral inferential comprehension intervention for young children with developmental language disorder. Child Lang. Teach. Ther. 2018, 35, 39–54. [Google Scholar] [CrossRef]
- Hessling, A.; Schuele, C.M. Individualized Narrative Intervention for School-Age Children with Specific Language Impairment. Lang. Speech, Hearth Serv. Sch. 2020, 51, 687–705. [Google Scholar] [CrossRef] [PubMed]
- Saywitz, K.J.; Snyder, L. Narrative elaboration: Test of a new procedure for interviewing children. J. Consult. Clin. Psychol. 1996, 64, 1347–1357. [Google Scholar] [CrossRef] [PubMed]
- Spencer, T.D.; Kajian, M.; Petersen, D.B.; Bilyk, N. Effects of an Individualized Narrative Intervention on Children’s Storytelling and Comprehension Skills. J. Early Interv. 2013, 35, 243–269. [Google Scholar] [CrossRef]
- Trojano, L.; Grossi, D. ‘Pure’ Constructional Apraxia—A Cognitive Analysis of a Single Case. Behav. Neurol. 1998, 11, 43–49. [Google Scholar] [CrossRef]
- Roncato, S.; Sartori, G.; Masterson, J.; Rumiati, R. Constructional apraxia: An information processing analysis. Cogn. Neuropsychol. 1987, 4, 113–129. [Google Scholar] [CrossRef]
- Van Sommers, P. Drawing and Cognition: Descriptive and Experimental Studies of Graphic Production Processes; Cambridge University Press: Cambridge, UK, 1984. [Google Scholar]
- Van Sommers, P.V. A system for drawing and drawing-related neuropsychology. Cogn. Neuropsychol. 1989, 6, 117–164. [Google Scholar] [CrossRef]
- Vincent, L.B.; Openden, D.; Gentry, J.A.; Long, L.A.; Matthews, N.L. Promoting Social Learning at Recess for Children with ASD and Related Social Challenges. Behav. Anal. Pract. 2017, 11, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Ketcheson, L.; Hauck, J.; Ulrich, D. The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: A pilot study. Autism 2017, 21, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Ke, F.; Moon, J. Virtual collaborative gaming as social skills training for high-functioning autistic children. Br. J. Educ. Technol. 2018, 49, 728–741. [Google Scholar] [CrossRef]
- Prince, J. Implementation of the Power Card Strategy to Increase Appropriate Social Commenting of Children with autism Spectrum Disorder during Game Play. Master Dissertation, Temple University, Philadelphia, PA, USA, 2018. [Google Scholar]
- Tsai, W.-T.; Lee, I.-J.; Chen, C.-H. Inclusion of third-person perspective in CAVE-like immersive 3D virtual reality role-playing games for social reciprocity training of children with an autism spectrum disorder. Univers. Access Inf. Soc. 2020, 20, 375–389. [Google Scholar] [CrossRef]
- Willingham, D. Why Don’t Students Like School? A Cognitive Scientist Answers Questions about How the Mind Works and What It Means for the Classroom; Wiley: New York, NY, USA, 2021. [Google Scholar]
- Barrouillet, P.; Camos, V.; Perruchet, P.; Seron, X. ADAPT: A Developmental, Asemantic, and Procedural Model for Transcoding from Verbal to Arabic Numerals. Psychol. Rev. 2004, 111, 368–394. [Google Scholar] [CrossRef]
- Rosenthal, M.; Wallace, G.L.; Lawson, R.; Wills, M.C.; Dixon, E.; Yerys, B.E.; Kenworthy, L. Impairments in real-world executive function increase from childhood to adolescence in autism spectrum disorders. Neuropsychology 2013, 27, 13–18. [Google Scholar] [CrossRef]
- Debodinance, E.; Maljaars, J.; Noens, I.; Noortgate, W.V.D. Interventions for toddlers with autism spectrum disorder: A meta-analysis of single-subject experimental studies. Res. Autism Spectr. Disord. 2017, 36, 79–92. [Google Scholar] [CrossRef]
- Franz, L.; Goodwin, C.D.; Rieder, A.; Matheis, M.; Damiano, D.L. Early intervention for very young children with or at high likelihood for autism spectrum disorder: An overview of reviews. Dev. Med. Child Neurol. 2022, 64, 1063–1076. [Google Scholar] [CrossRef]
- Morris, E.K. A case study in the misrepresentation of applied behavior analysis in autism: The gernsbacher lectures. Behav. Anal. 2009, 32, 205–240. [Google Scholar] [CrossRef]
- Paynter, J.; Sulek, R.; Westerveld, M. The Importance of Evidence Based Practices and Autism. In Handbook of Autism and Pervasive Developmental Disorder; Springer: Berlin/Heidelberg, Germany, 2022; pp. 579–598. [Google Scholar]
- Lovaas, O.I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J. Consult. Clin. Psychol. 1987, 55, 3–9. [Google Scholar] [CrossRef]
- Lovaas, O.I.; Koegel, R.; Simmons, J.Q.; Long, J.S. Some generalization and follow-up measures on autistic children in behavior therapy1. J. Appl. Behav. Anal. 1973, 6, 131–165. [Google Scholar] [CrossRef] [PubMed]
- Baum, W.M. Compreender o Behaviorismo—3.ed.: Comportamento, Cultura e Evolução; Artmed Editora: Belo Horizonte, Brazil, 2018; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=dIxyDwAAQBAJ&oi=fnd&pg=PT6&dq=Compreender+o+Behaviorismo:+Com (accessed on 24 January 2024).
- Cannon, J.; O’Brien, A.M.; Bungert, L.; Sinha, P. Prediction in Autism Spectrum Disorder: A Systematic Review of Empirical Evidence. Autism Res. 2021, 14, 604–630. [Google Scholar] [CrossRef] [PubMed]
- Eigsti, I.-M. A Review of Embodiment in Autism Spectrum Disorders. Front. Psychol. 2013, 4, 224. [Google Scholar] [CrossRef] [PubMed]
- Hellendoorn, A.; Wijnroks, L.; Leseman, P.P.M. Unraveling the nature of autism: Finding order amid change. Front. Psychol. 2015, 6, 359. [Google Scholar] [CrossRef] [PubMed]
- Friston, K.; Kiebel, S.; Friston, K.; Kiebel, S. Predictive coding under the free-energy principle. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- McCarty, M.J.; Brumback, A.C. Rethinking Stereotypies in Autism. Semin. Pediatr. Neurol. 2021, 38, 100897. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, P.; Giallongo, L.; Milintenda, G.; Cannarozzo, M. Autism, autistic traits and creativity: A systematic review and meta-analysis. Cogn. Process. 2021, 22, 1–36, Erratum in Cogn. Process. 2021, 22, 733.. [Google Scholar] [CrossRef]
- Wu, X.; Deng, H.; Jian, S.; Chen, H.; Li, Q.; Gong, R.; Wu, J. Global trends and hotspots in the digital therapeutics of autism spectrum disorders: A bibliometric analysis from 2002 to 2022. Front. Psychiatry 2023, 14, 1126404. [Google Scholar] [CrossRef]
- Annelise, A.J.; Costa, A.J.; Silva, J.B.L.; Chagas, P.P.; Krinzinger, H.; Lonneman, J.; Willmes, K.; Wood, G.; Haase, V.G. A hand full of numbers: A role for offloading in arithmetics learning? Front. Psychol. 2011, 2, 368. [Google Scholar] [CrossRef] [PubMed]
- Batstra, L.; Neeleman, J.; Hadders-Algra, M. The neurology of learning and behavioural problems in pre-adolescent children. Acta Psychiatr. Scand. 2003, 108, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Mundy, P. A review of joint attention and social-cognitive brain systems in typical development and autism spectrum disorder. Eur. J. Neurosci. 2018, 47, 497–514. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Toth, K.; Abbott, R.; Osterling, J.; Munson, J.; Estes, A.; Liaw, J. Early Social Attention Impairments in Autism: Social Orienting, Joint Attention, and Attention to Distress. Dev. Psychol. 2004, 40, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Dawson, G.; Munson, J.; Estes, A.; Osterling, J.; McPartland, J.; Toth, K.; Carver, L.; Abbott, R. Neurocognitive Function and Joint Attention Ability in Young Children with Autism Spectrum Disorder Versus Developmental Delay. Child Dev. 2002, 73, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Özçalışkan, S.; Goldin-Meadow, S. Gesture is at the cutting edge of early language development. Cognition 2005, 96, B101–B113. [Google Scholar] [CrossRef] [PubMed]
- Uzgiris, I.C. Two Functions of Imitation During Infancy. Int. J. Behav. Dev. 1981, 4, 1–12. [Google Scholar] [CrossRef]
- Bailes, A.F.; Greve, K.; Schmitt, L.C. Changes in Two Children with Cerebral Palsy After Intensive Suit Therapy: A Case Report. Pediatr. Phys. Ther. 2010, 22, 76–85. [Google Scholar] [CrossRef]
- Purnamasari, N.; Bachtiar, F.; Puspitha, R.A. The effectiveness of motor-cognitive dual-task training in reducing risk falls on elderly. Enfermería Clínica 2020, 30, 317–321. [Google Scholar] [CrossRef]
- Ko, M.-S.; Lee, J.-A.; Kang, S.-Y.; Jeon, H.-S. Effect of Adeli suit treatment on gait in a child with cerebral palsy: A single-subject report. Physiother. Theory Pract. 2014, 31, 275–282. [Google Scholar] [CrossRef]
- Matthews, M.J.; Watson, M.; Richardson, B. Effects of Dynamic Elastomeric Fabric Orthoses on Children with Cerebral Palsy. Prosthetics Orthot. Int. 2009, 33, 339–347. [Google Scholar] [CrossRef]
- Bar-Haim, S.; Harries, N.; Belokopytov, M.; Frank, A.; Copeliovitch, L.; Kaplanski, J.; Lahat, E. Comparison of efficacy of Adeli suit and neurodevelopmental treatments in children with cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Almeida, K.M.; Fonseca, S.T.; Figueiredo, P.R.; Aquino, A.A.; Mancini, M.C. Effects of interventions with therapeutic suits (clothing) on impairments and functional limitations of children with cerebral palsy: A systematic review. Braz. J. Phys. Ther. 2017, 21, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Levin, S.M. The tensegrity-truss as a model for spine mechanics: Biotensegrity. J. Mech. Med. Biol. 2002, 02, 375–388. [Google Scholar] [CrossRef]
- Ingber, D.E. Tensegrity and mechanotransduction. J. Bodyw. Mov. Ther. 2008, 12, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Turvey, M.T.; Fonseca, S.T. The Medium of Haptic Perception: A Tensegrity Hypothesis. J. Mot. Behav. 2014, 46, 143–187. [Google Scholar] [CrossRef] [PubMed]
- Busquet-Vanderheyden, M. As Cadeias Fisiológicas—A Cadeia Visceral: Tórax, Garganta e Boca: Descrição e Tratamento; Método Busquet: Curitiba, Brazil, 2020; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=nsjgDwAAQBAJ&oi=fnd&pg=PT4&dq=as+cadeias+fisiol (accessed on 24 January 2024).
- Myers, T.W. Anatomy Trains; Churchill Livingstone: Oxford, UK, 2001; 332p. [Google Scholar]
- Stecco, C.; Porzionato, A.; Macchi, V.; Tiengo, C.; Parenti, A.; Aldegheri, R.; Delmas, V.; De Caro, R. Histological characteristics of the deep fascia of the upper limb. Italy J. Anat. Embryol. 2006, 111, 105–110. [Google Scholar]
- Stecco, A.; Macchi, V.; Stecco, C.; Porzionato, A.; Day, J.A.; Delmas, V.; De Caro, R. Anatomical study of myofascial continuity in the anterior region of the upper limb. J. Bodyw. Mov. Ther. 2009, 13, 53–62. [Google Scholar] [CrossRef]
- Schleip, R.; Müller, D.G. Training principles for fascial connective tissues: Scientific foundation and suggested practical applications. J. Bodyw. Mov. Ther. 2013, 17, 103–115. [Google Scholar] [CrossRef]
- Schleip, R.; Bayer, J. Fascial Fitness: How to Be Vital, Elastic and Dynamic in Everyday Life and Sport; Lotus Pub: Lotus, CA, USA, 2017; 224p. [Google Scholar]
- Fede, C.; Petrelli, L.; Guidolin, D.; Porzionato, A.; Pirri, C.; Fan, C.; De Caro, R.; Stecco, C. Evidence of a new hidden neural network into deep fasciae. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Stecco, C. Functional Atlas of the Human Fascial System; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014; Available online: https://books.google.com.br/books?hl=pt-BR&lr=&id=8eDTBQAAQBAJ&oi=fnd&pg=PP1&dq=+Functional+atlas+of+the+human+fascial+system.&ots=HEfpTwL99-&sig=6-uLwccpXaN-sFouHVsFqigku_U#v=onepage&q=Functional%20atlas%20of%20the%20human%20fasc (accessed on 24 January 2024).
- Fede, C.; Petrelli, L.; Pirri, C.; Neuhuber, W.; Tiengo, C.; Biz, C.; De Caro, R.; Schleip, R.; Stecco, C. Innervation of human superficial fascia. Front. Neuroanat. 2022, 16, 981426. [Google Scholar] [CrossRef]
- Stecco, C.; Sfriso, M.M.; Porzionato, A.; Rambaldo, A.; Albertin, G.; Macchi, V.; De Caro, R. Microscopic anatomy of the visceral fasciae. J. Anat. 2017, 231, 121–128. [Google Scholar] [CrossRef]
- Mosconi, M.W.; Mohanty, S.; Greene, R.K.; Cook, E.H.; Vaillancourt, D.E.; Sweeney, J.A. Feedforward and Feedback Motor Control Abnormalities Implicate Cerebellar Dysfunctions in Autism Spectrum Disorder. J. Neurosci. 2015, 35, 2015–2025. [Google Scholar] [CrossRef] [PubMed]
- Serdarevic, F.; Ghassabian, A.; van Batenburg-Eddes, T.; White, T.; Blanken, L.M.E.; Jaddoe, V.W.V.; Verhulst, F.C.; Tiemeier, H. Infant muscle tone and childhood autistic traits: A longitudinal study in the general population. Autism Res. 2017, 10, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.A.H.; Józsa, L.; Kannus, P.; Järvinen, T.L.N.; Järvinen, M. Organization and distribution of intramuscular connective tissue in normal and immobilized skeletal muscles. An immunohistochemical, polarization and scanning electron microscopic study. J. Muscle Res. Cell Motil. 2002, 23, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.D.; Narici, M.V.; Maganaris, C.N. Myotendinous plasticity to ageing and resistance exercise in humans. Exp. Physiol. 2006, 91, 483–498. [Google Scholar] [CrossRef] [PubMed]
- Proske, U.; Gandevia, S.C. The kinaesthetic senses. J. Physiol. 2009, 587, 4139–4146. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, A.; Slack, H.G.B. The metabolism of collagen from liver, bone, skin and tendon in the normal rat. Biochem. J. 1953, 53, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Lei nº9.656, de 3 de Junho de 1998. Dispõe Sobre osPlanos e Seguros Privados de Assistência à Saúde. Diário Oficial da União. 4 June 1998. Available online: https://www.planalto.gov.br/ccivil_03/leis/l9656.htm (accessed on 29 January 2024).
- Law, M.; Baptiste, S.; Carswell, A.; McColl, M.A.; Polatajko, H.; Pollock, N. Canadian Occupational Performance Measure, 4th ed.; CAOT Publications ACE: Ottowa, ON, Canada, 2005. [Google Scholar]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale: SRS-2; Pearson: Sydney, Australia, 2012. [Google Scholar]
- Borges, L.; Hauck-Filho, N. Escala de Responsividade Social (SRS-2); Pearson: Sydney, Australia, 2020. [Google Scholar]
- Di Rezze, B.; Rosenbaum, P.; Zwaigenbaum, L.; Hidecker, M.J.C.; Stratford, P.; Cousins, M.; Camden, C.; Law, M. Developing a classification system of social communication functioning of preschool children with autism spectrum disorder. Dev. Med. Child Neurol. 2016, 58, 942–948. [Google Scholar] [CrossRef]
- Angelini, A.L.; Alves, I.C.B.; Custdio, E.M.; Duarte, W.F.; Duarte, J.L.M. Manual: Matrizes Progressivas Coloridas de Raven; Centro Editor de Testes e Pesquisas em Psicologia: São Paulo, Brazil, 1999. [Google Scholar]
- Raven, J.; Raven, J.C.; Court, J.H. Matrizes Progressivas Coloridas de Raven: CPM; Pearson: São Paulo, Brazil, 2018; 142p. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Fleitlich, B.; Cortázar, P.G.; Goodman, R. Questionário de Capacidades e Dificuldades (SDQ). Infanto Rev. Neuropsiquiatr. Infanc. Adolesc 2000, 44–50. [Google Scholar]
- Haley, S.M.; Coster, W.J.; Dumas, H.M.; Fragala-Pinkham, M.A.; Moed, R. PEDI-CAT: Development, Standardization and Administration Manual; Boston University: Boston, MA, USA, 2012. [Google Scholar]
- Franjoine, M.R.; Gunther, J.S.; Taylor, M.J. Pediatric balance scale: A modified version of the berg balance scale for the school-age child with mild to moderate motor impairment. Pediatr. Phys. Ther. Off. Publ. Sect. Pediatr. Am. Phys. Ther. Assoc. 2003, 15, 114–128. [Google Scholar] [CrossRef]
- Paillard, T.; Noé, F. Techniques and Methods for Testing the Postural Function in Healthy and Pathological Subjects. BioMed Res. Int. 2015, 2015, 891390. [Google Scholar] [CrossRef]
- Martín-Díaz, P.; Carratalá-Tejada, M.; Molina-Rueda, F.; Cuesta-Gómez, A. Reliability and agreement of the timed up and go test in children and teenagers with autism spectrum disorder. Eur. J. Pediatr. 2023, 182, 3577–3585. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Soppelsa, R.; Albaret, J.M. Test of Gross Motor Development Examiner’s Manual; Pro-Ed, Inc.: Austin, TX, USA, 2000. [Google Scholar]
- Poole, J.L.; Burtner, P.A.; Torres, T.A.; McMullen, C.K.; Markham, A.; Marcum, M.L.; Anderson, J.B.; Qualls, C. Measuring Dexterity in Children Using the Nine-hole Peg Test. J. Hand Ther. 2005, 18, 348–351. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).