
Gallbladder Stones in Pediatric Age: An Emerging Problem: The Risk of Difficult Cholecystectomy and the Importance of a Preoperative Evaluation
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Balaguer, E.J.; Price, M.R.; Burd, R.S. National trends in the utilization of cholecystectomy in children. J. Surg. Res. 2006, 134, 68–73. [Google Scholar] [CrossRef]
- Greer, D.; Heywood, S.; Croaker, D.; Gananadha, S. Is 14 the new 40: Trends in gallstone disease and cholecystectomy in Australian children. Pediatr. Surg. Int. 2018, 34, 845–849. [Google Scholar] [CrossRef]
- Mehta, S.; Lopez, M.E.; Chumpitazi, B.P.; Mazziotti, M.V.; Brandt, M.L.; Fishman, D.S. Clinical Characteristics and Risk Factors for Symptomatic Pediatric Gallbladder Disease. Pediatrics 2012, 129, e82–e88. [Google Scholar] [CrossRef]
- Frybova, B.; Drabek, J.; Lochmannova, J.; Douda, L.; Hlava, S.; Zemkova, D.; Mixa, V.; Kyncl, M.; Zeman, L.; Rygl, M.; et al. Cholelithiasis and choledocholithiasis in children; risk factors for development. PLoS ONE 2018, 13, e0196475. [Google Scholar] [CrossRef]
- Zdanowicz, K.; Daniluk, J.; Lebensztejn, D.M.; Daniluk, U. The Etiology of Cholelithiasis in Children and Adolescents—A Literature Review. Int. J. Mol. Sci. 2022, 23, 13376. [Google Scholar] [CrossRef]
- Khoo, A.K.; Cartwright, R.; Berry, S. Davenport M Cholecystectomy in English children: Evidence of an epidemic (1997–2012). J. Pediatr. Surg. 2014, 49, 284–288. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Aralica, M.; Jukić, M.; Žitko, V.; Despot, R.; Jurić, I. Gallbladder Disease in Children: A 20-year Single-center Experience. Indian Pediatr. 2019, 56, 384–386. [Google Scholar] [CrossRef]
- Santos, B.F.; Brunt, L.M.; Pucci, M.J. The Difficult Gallbladder: A Safe Approach to a Dangerous Problem. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 571–578. [Google Scholar] [CrossRef]
- Kala Sanjay, M.S.; Verma Satyajeet, M.S.; Dutta Gautam, M.S. Difficult Situations in Laparoscopic Cholecystectomy: A Multicentric Retrospective Study. Surg. Laparosc. Endosc. Percutaneous Tech. 2014, 24, 484–487. [Google Scholar] [CrossRef]
- Walker, S.K.; Maki, A.C.; Cannon, R.M.; Foley, D.S.; Wilson, K.M.; Galganski, L.A.; Wiesenauer, C.A.; Bond, S.J. Etiology and incidence of pediatric gallbladder disease. Surgery 2013, 154, 927–931. [Google Scholar] [CrossRef]
- Fradin, K.; Racine, A.D.; Belamarich, P.F. Obesity and symptomatic cholelithiasis in childhood: Epidemiologic and case-control evidence for a strong relation. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Koebnick, C.; Smith, N.; Black, M.H.; Porter, A.H.; Richie, B.A.; Hudson, S.; Gililland, D.; Jacobsen, S.J.; Longstreth, G.F. Pediatric obesity and gallstone disease: Results from a cross-sectional study of over 510,000 youth. J. Pediatr. Gastroenterol. Nutr. 2012, 5, 328. [Google Scholar] [CrossRef] [PubMed]
- Palasciano, G.; Portincasa, P.; Vinciguerra, V.; Velardi, A.; Tardi, S.; Baldassarre, G.; Albano, O. Gallstone prevalence and gallbladder volume in children an adolescents: An epidemiological ultrasonographic survey and relationship to body mass index. Am. J. Gastroenterol. 1989, 84, 1378–1382. [Google Scholar] [PubMed]
- Noviello, C.; Papparella, A.; Romano, M.; Cobellis, G. Risk Factors of Cholelithiasis Unrelated to Hematological Disorders in Pediatric Patients Undergoing Cholecystectomy. Gastroenterol. Res. 2018, 11, 346–348. [Google Scholar] [CrossRef] [PubMed]
- Bailey, P.V.; Connors, R.H.; Tracy, T.F., Jr.; Sotelo-Avila, C.; Lewis, J.E.; Weber, T.R. Changing spectrum of cholelithiasis and cholecystitis in infants and children. Am. J. Surg. 1989, 158, 585–588. [Google Scholar] [CrossRef]
- Serdaroglu, F.; Koca, Y.S.; Saltik, F.; Koca, T.; Dereci, S.; Akcam, M.; Akcam, F.Z. Gallstones in childhood: Etiology, clinical features, and prognosis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1468–1472. [Google Scholar] [CrossRef]
- Vazquez, M.C.; Rigotti, A.; Zanlungo, S. Molecular mecha- nisms underlying the link between nuclear receptor function and cholesterol gallstone formation. J. Lipids 2012, 2012, 547643. [Google Scholar] [CrossRef]
- Nassar, A.H.M.; Ashkar, K.A.; Mohamed, A.Y.; Hafiz, A.A. Is laparoscopic cholecystectomy possible without video technology? Minim. Invasive Ther. Allied Technol. 1995, 4, 63–65. [Google Scholar] [CrossRef]
- Strasberg, S.M.; Hertl, M.; Soper, N.J. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J. Am. Coll. Surg. 1995, 180, 101–125. [Google Scholar]
- Pesce, A.; Piccolo, G.; La Greca, G.; Puleo, S. Utility of fluorescent cholangiography during laparoscopic cholecystectomy: A systematic review. World J. Gastroenterol. 2015, 21, 7877–7883. [Google Scholar] [CrossRef]
- Esposito, C.; Corcione, F.; Settimi, A.; Farina, A.; Centonze, A.; Esposito, G.; Spagnuolo, M.I.; Escolino, M. Twenty-Five Year Experience with Laparoscopic Cholecystectomy in the Pediatric Population-From 10 mm Clips to Indocyanine Green Fluorescence Technology: Long-Term Results and Technical Considerations. J. Laparoendosc. Adv. Surg. Tech. Part A 2019, 29, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Purzner, R.H.; Ho, K.B.; Al-Sukhni, E.; Jayaraman, S. Safe laparoscopic subtotal cholecystectomy in the face of severe inflammation in the cystohepatic triangle: A retrospective review and proposed management strategy for the difficult gallbladder. Can. J. Surg. 2019, 62, 402–411. [Google Scholar] [CrossRef] [PubMed]
- Elshaer, M.; Gravante, G.; Thomas, K.; Sorge, R.; Al-Hamali, S.; Ebdewi, H. Subtotal cholecystectomy for “difficult gallbladders”: Systematic review and meta-analysis. JAMA Surg. 2015, 150, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Kharytaniuk, N.; Bass, G.A.; Dumbrava, B.D.; Healy, P.P.; Viani-Walsh, D.; Tiwary, T.N.; Abassi, T.; Murphy, M.P.; Griffin, E.; Walsh, T.N. The impossible gallbladder: Aspiration as an alternative to conversion. Surg. Endosc. 2020, 34, 1868–1875. [Google Scholar] [CrossRef]
- Romagnuolo, J.; Bardou, M.; Rahme, E.; Joseph, L.; Reinhold, C.; Barkun, A.N. Magnetic resonance cholangiopancreatography: A meta-analysis of test performance in suspected biliary disease. Ann. Intern. Med. 2003, 139, 547–557. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 |
|---|---|---|---|---|---|
| Gender | F | M | M | F | F |
| Age (years) | 15 | 8 | 15 | 17 | 18 |
| BMI (kg/m3) | 29.6 | 28.3 | 29.4 | 19 | 28.4 |
| Associated anomalies | / | / | / | Rett Syndrome | Rett Syndrome |
| History | Recurrent abdominal pain | Recurrent abdominal pain | / | Chronic diffuse abdominal pain | Chronic non specific abdominal pain |
| Symptoms | Acute localized abdominal pain, fever | Acute localized abdominal pain | Acute localized abdominal pain | Acute non specific abdominal pain | Acute diffuse abdominal pain |
| Abdominal US | Acute cholecystits, gallstones, dilatation of biliary tree | Acute cholecystits, gallstones | Gallbladder stones with dilatation of biliary tree | Numerous gall stones without biliary tract dilatation | Numerous gallbladder stones without biliary tract dilatation |
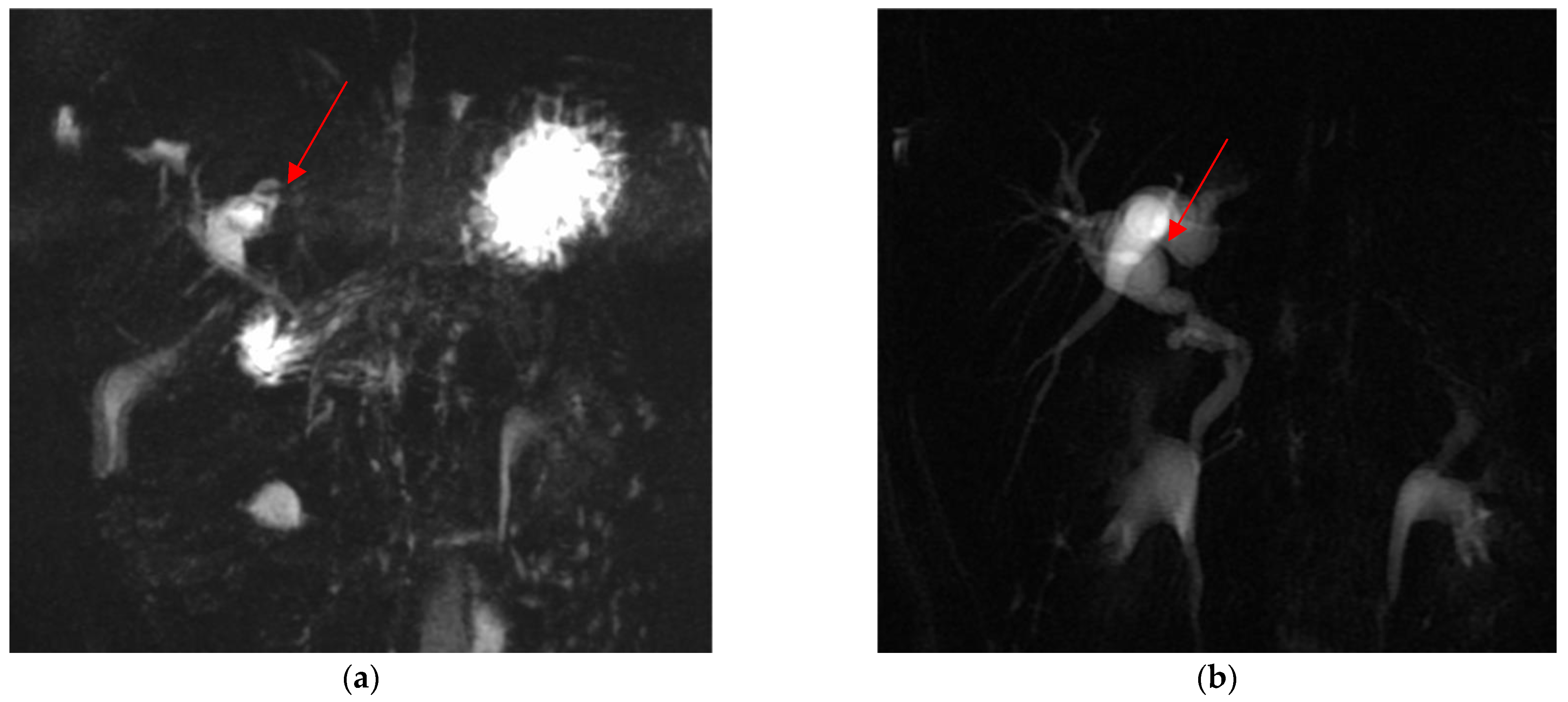
| Cholangio-MRI | Dysmorphic inflamed gallbladder with tiny infundibulum and convoluted cystic duct | Presence of gallstones | Anomaly in the biliary tract anatomy: cystic duct projected into an aberrant right anterior hepatic duct | Presence of gallstones | Presence of gallstones |
| ERCP | Removing of two small stoned | Not performed | Removing of numerous small stones in the two hepatic ducts | Not performed | Not performed |
| VLS cholecystectomy | Subtotal | Total | Subtotal | Total | Total |
| Post operative US | No biliary dilatation | Persistence of dilated biliary tree | No biliary dilatation | No biliary dilatation | No biliary dilatation |
| Post operative c-MRI | Persistence of dilated portion of the infundibulum and cystic duct | Not performed | Not performed | Not performed | Not performed |
| Last follow up (months) | 12 | 10 | 12 | 12 | 12 |
| Problems Encountered | N Patients Treated | Conversion Rate | PO Complication Rate |
|---|---|---|---|
| Acute inflammation of the gallbladder | 1 | 0% | 0% |
| Chronic inflammation | 1 | 0% | 0% |
| Difficult trocar placement and reduced camera | 2 | 0% | 0% |
| Anatomical anomalies | 1 | 0% | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Todesco, C.; Molinaro, F.; Nascimben, F.; Gentilucci, G.; Messina, M.; Cortese, A.; Briganti, V.; Tursini, S. Gallbladder Stones in Pediatric Age: An Emerging Problem: The Risk of Difficult Cholecystectomy and the Importance of a Preoperative Evaluation. Children 2023, 10, 1544. https://doi.org/10.3390/children10091544
Todesco C, Molinaro F, Nascimben F, Gentilucci G, Messina M, Cortese A, Briganti V, Tursini S. Gallbladder Stones in Pediatric Age: An Emerging Problem: The Risk of Difficult Cholecystectomy and the Importance of a Preoperative Evaluation. Children. 2023; 10(9):1544. https://doi.org/10.3390/children10091544
Chicago/Turabian StyleTodesco, Camilla, Francesco Molinaro, Francesca Nascimben, Gianluca Gentilucci, Mario Messina, Andrea Cortese, Vito Briganti, and Stefano Tursini. 2023. "Gallbladder Stones in Pediatric Age: An Emerging Problem: The Risk of Difficult Cholecystectomy and the Importance of a Preoperative Evaluation" Children 10, no. 9: 1544. https://doi.org/10.3390/children10091544
APA StyleTodesco, C., Molinaro, F., Nascimben, F., Gentilucci, G., Messina, M., Cortese, A., Briganti, V., & Tursini, S. (2023). Gallbladder Stones in Pediatric Age: An Emerging Problem: The Risk of Difficult Cholecystectomy and the Importance of a Preoperative Evaluation. Children, 10(9), 1544. https://doi.org/10.3390/children10091544